

Is a Higher Amniotic Fluid Viral Load Associated with a Greater Risk of Fetal Injury in Congenital Cytomegalovirus Infection—A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
3. Inclusion and Exclusion Criteria
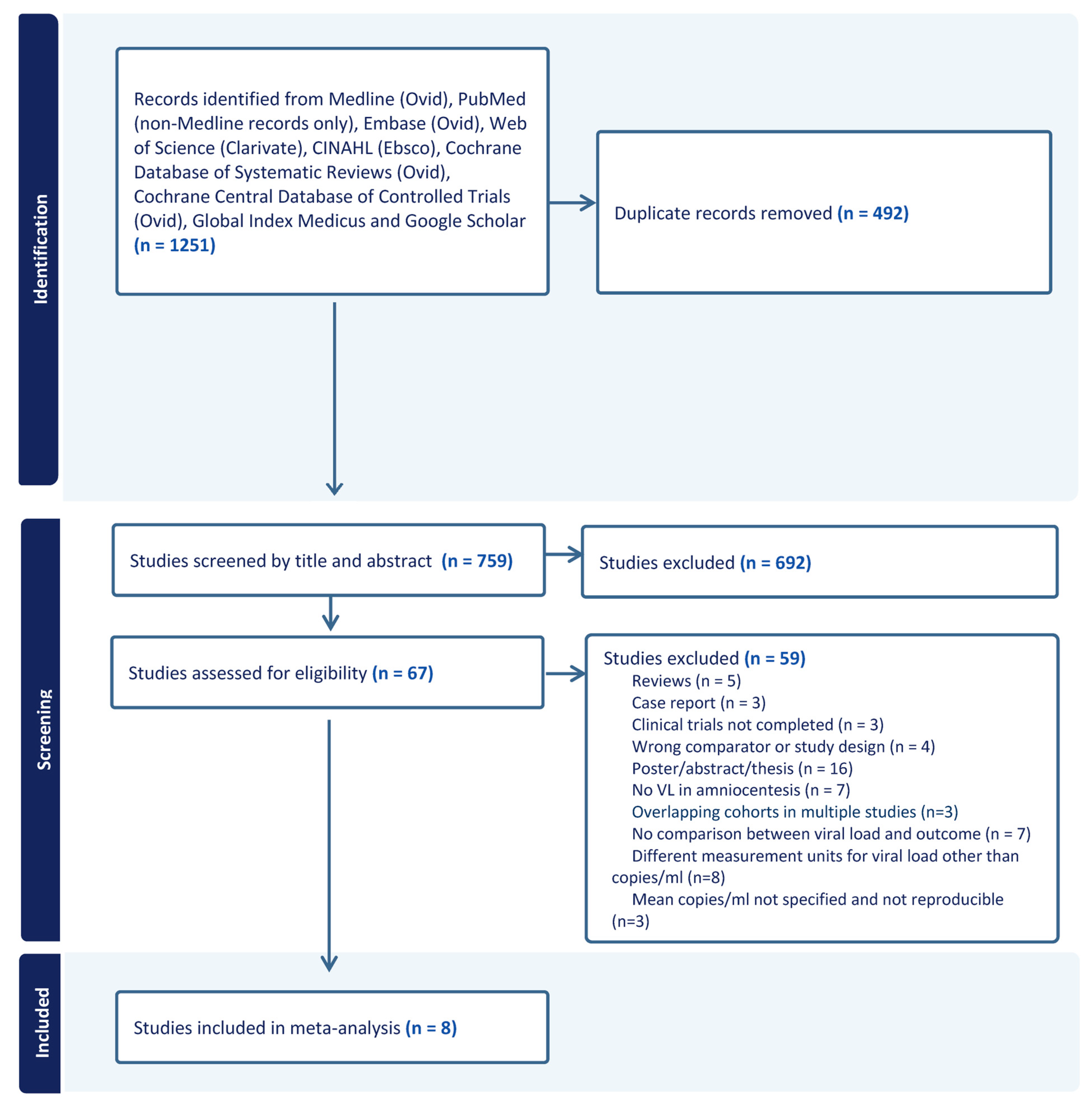
4. Search Strategy
5. Quality Analysis
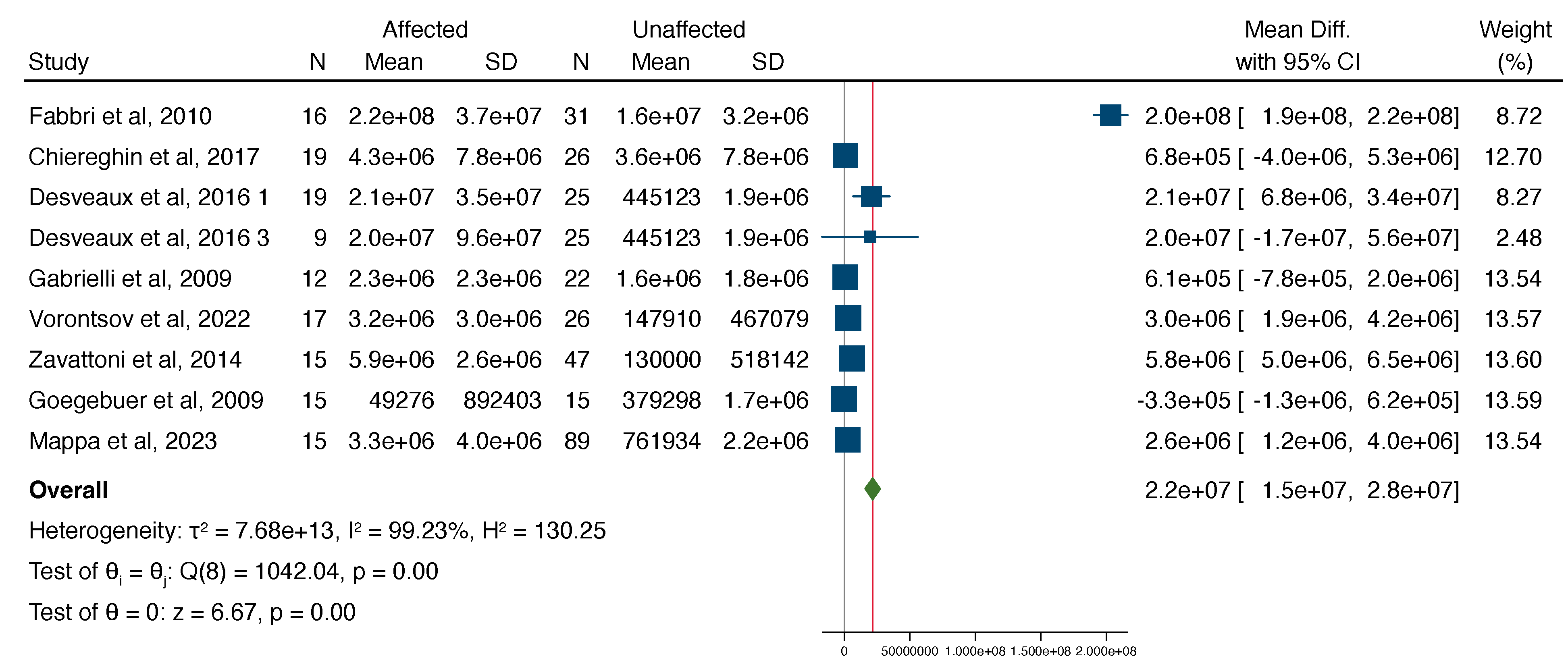
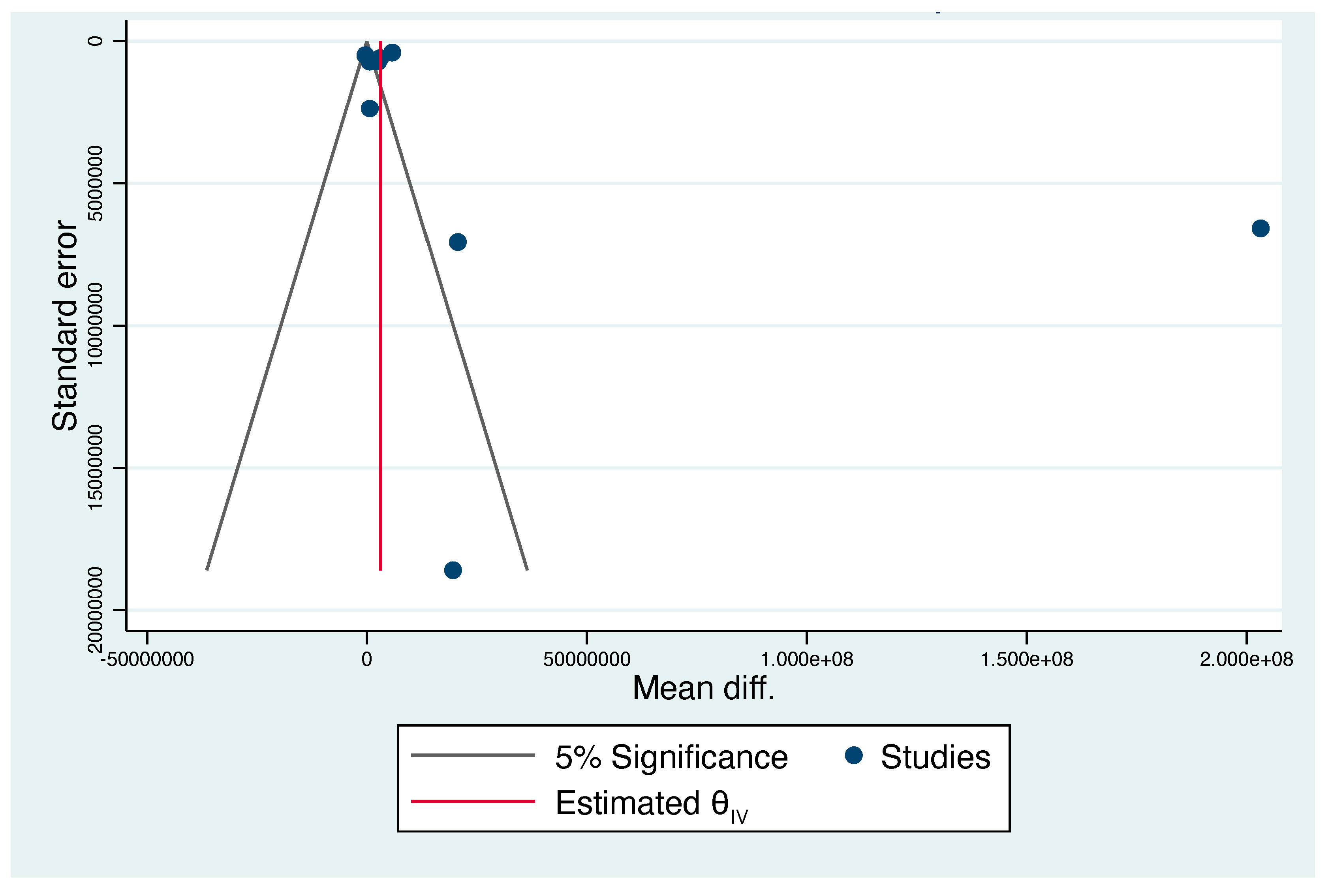
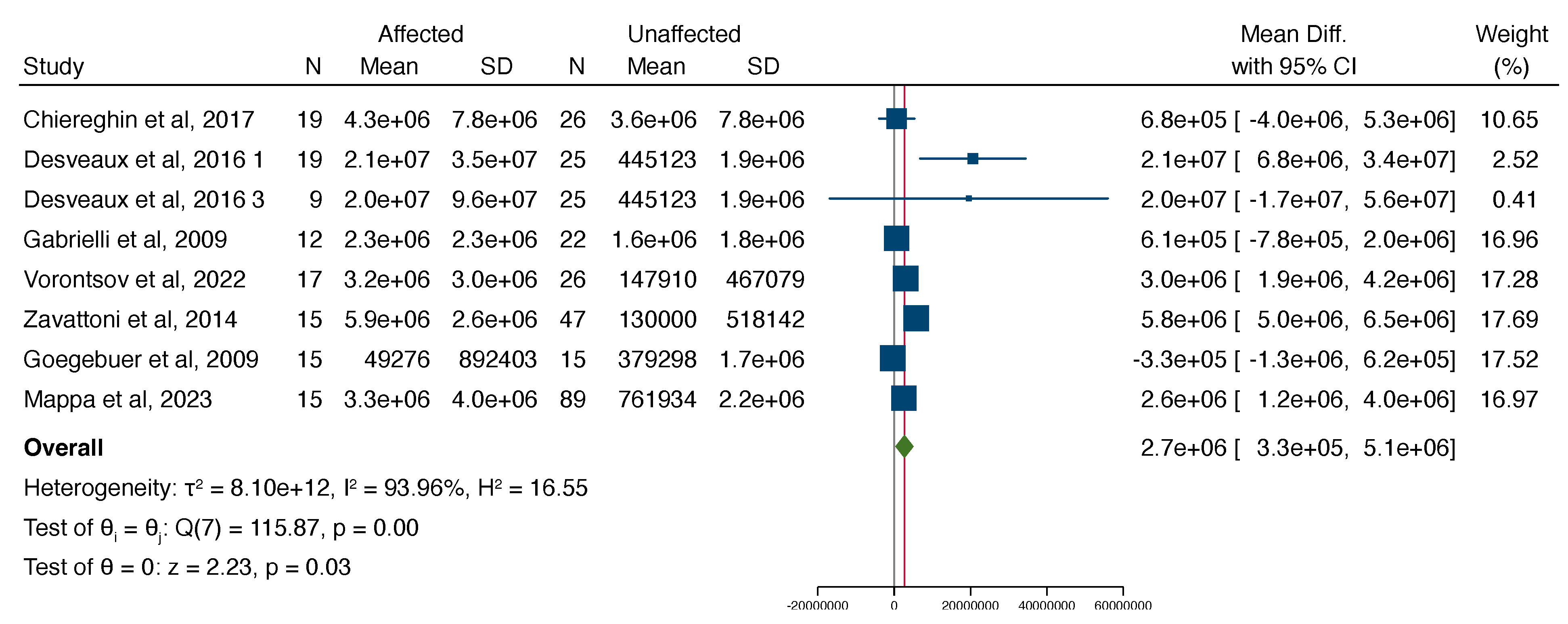
6. Statistical Analysis
7. Results
8. Outcome Definitions
9. Risk of Adverse Perinatal Outcome
10. Discussion
10.1. Main Findings
10.2. Strengths and Limitations
10.3. Implications of Findings
11. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- CDC. Available online: https://www.cdc.gov/cmv/clinical/congenital-cmv (accessed on 1 January 2023).
- Nigro, G. Maternal–fetal cytomegalovirus infection: From diagnosis to therapy. J. Matern.-Fetal Neonatal Med. 2009, 22, 169–174. [Google Scholar] [CrossRef]
- Chatzakis, C.; Ville, Y.; Makrydimas, G.; Dinas, K.; Zavlanos, A.; Sotiriadis, A. Timing of primary maternal cytomegalovirus infection and rates of vertical transmission and fetal consequences. Am. J. Obstet. Gynecol. 2020, 223, 870–883.e11. [Google Scholar] [CrossRef]
- Buca, D.; Di Mascio, D.; Rizzo, G.; Giancotti, A.; D’Amico, A.; Leombroni, M.; Makatsarya, A.; Familiari, A.; Liberati, M.; Nappi, L.; et al. Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 551–559. [Google Scholar] [CrossRef]
- Bale, J.F., Jr.; Murph, J.R.; Demmler, G.J.; Dawson, J.; Miller, J.E.; Petheram, S.J. Intrauterine Cytomegalovirus Infection and Glycoprotein B Genotypes. J. Infect. Dis. 2000, 182, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Barbi, M.; Binda, S.; Caroppo, S.; Primache, V.; Didò, P.; Guidotti, P.; Corbetta, C.; Melotti, D. CMV gB genotypes and outcome of vertical transmission: Study on dried blood spots of congenitally infected babies. J. Clin. Virol. 2001, 21, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Picone, O.; Costa, J.M.; Leruez-Ville, M.; Ernault, P.; Olivi, M.; Ville, Y. Cytomegalovirus (CMV) glycoprotein B genotype and CMV DNA load in the amniotic fluid of infected fetuses. Prenat Diagn. 2004, 24, 1001–1006. [Google Scholar] [CrossRef]
- Benoist, G.; Salomon, L.; Jacquemard, F.; Daffos, F.; Ville, Y. The prognostic value of ultrasound abnormalities and biological parameters in blood of fetuses infected with cytomegalovirus. BJOG 2008, 115, 823–829. [Google Scholar] [CrossRef]
- Hawkins-Villarreal, A.; Moreno-Espinosa, A.L.; Eixarch, E.; Marcos, M.A.; Martinez-Portilla, R.J.; Salazar, L.; Garcia-Otero, L.; Lopez, M.; Borrell, A.; Figueras, F.; et al. Blood parameters in fetuses infected with cytomegalovirus according to the severity of brain damage and trimester of pregnancy at cordocentesis. J. Clin. Virol. 2019, 119, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.Y.; Xu, F.; Chen, D.Z.; Meng, X.N.; Xu, T.S.; Lu, M.D.; Zhuge, H.-X. A Multifactorial Analysis of the Pregnancy Outcomes in Cytomegalovirus-Infected Women. Gynecol. Obstet. Invest. 2015, 80, 106–112. [Google Scholar] [CrossRef]
- Vorontsov, O.; Levitt, L.; Lilleri, D.; Vainer, G.W.; Kaplan, O.; Schreiber, L.; Arossa, A.; Spinillo, A.; Furione, M.; Alfi, O.; et al. Amniotic fluid biomarkers predict the severity of congenital cytomegalovirus infection. J. Clin. Investig. 2022, 132, e157415. [Google Scholar] [CrossRef]
- Desveaux, C.; Klein, J.; Leruez-Ville, M.; Ramirez-Torres, A.; Lacroix, C.; Breuil, B.; Froment, C.; Bascands, J.-L.; Schanstra, J.P.; Ville, Y. Identification of Symptomatic Fetuses Infected with Cytomegalovirus Using Amniotic Fluid Peptide Biomarkers. PLoS Pathog. 2016, 12, e1005395. [Google Scholar] [CrossRef]
- Gouarin, S.; Gault, E.; Vabret, A.; Cointe, D.; Rozenberg, F.; Grangeot-Keros, L.; Barjot, P.; Garbarg-Chenon, A.; Lebon, P.; Freymuth, F. Real-Time PCR Quantification of Human Cytomegalovirus DNA in Amniotic Fluid Samples from Mothers with Primary Infection. J. Clin. Microbiol. 2002, 40, 1767–1772. [Google Scholar] [CrossRef]
- Guerra, B.; Lazzarotto, T.; Quarta, S.; Lanari, M.; Bovicelli, L.; Nicolosi, A.; Landini, M.P. Prenatal diagnosis of symptomatic congenital cytomegalovirus infection. Am. J. Obstet. Gynecol. 2000, 183, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Lazzarotto, T.; Varani, S.; Guerra, B.; Nicolosi, A.; Lanari, M.; Landini, M.P. Prenatal indicators of congenital cytomegalovirus infection. J. Pediatr. 2000, 137, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Revello, M.G.; Gerna, G. Diagnosis and Management of Human Cytomegalovirus Infection in the Mother, Fetus, and Newborn Infant. Clin. Microbiol. Rev. 2002, 15, 680–715. [Google Scholar] [CrossRef]
- Goegebuer, T.; Van Meensel, B.; Beuselinck, K.; Cossey, V.; Van Ranst, M.; Hanssens, M.; Lagrou, K. Clinical Predictive Value of Real-Time PCR Quantification of Human Cytomegalovirus DNA in Amniotic Fluid Samples. J. Clin. Microbiol. 2009, 47, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Revello, M.G.; Zavattoni, M.; Furione, M.; Baldanti, F.; Gerna, G. Quantification of Human Cytomegalovirus DNA in Amniotic Fluid of Mothers of Congenitally Infected Fetuses. J. Clin. Microbiol. 1999, 37, 3350–3352. [Google Scholar] [CrossRef]
- Fabbri, E.; Revello, M.; Furione, M.; Zavattoni, M.; Lilleri, D.; Tassis, B.; Quarenghi, A.; Rustico, M.; Nicolini, U.; Ferrazzi, E.; et al. Prognostic markers of symptomatic congenital human cytomegalovirus infection in fetal blood. BJOG 2011, 118, 448–456. [Google Scholar] [CrossRef]
- Gabrielli, L.; Bonasoni, M.P.; Lazzarotto, T.; Lega, S.; Santini, D.; Foschini, M.P.; Guerra, B.; Baccolini, F.; Piccirilli, G.; Chiereghin, A.; et al. Histological findings in foetuses congenitally infected by cytomegalovirus. J. Clin. Virol. 2009, 46, S16–S21. [Google Scholar] [CrossRef]
- Mappa, I.; D’Antonio, F.; Khalil, A.; De Vito, M.; Alameddine, S.; Capannolo, G.; di Mascio, D.; Rizzo, G.; on behalf of ENSO group. Prognostic Value of Amniotic Fluid Viral Load to Predict Adverse Outcome in Pregnancies Complicated by Congenital Cytomegalovirus Infection: A Multicenter Study. Fetal. Diagn. Ther. 2023, 50, 1–7. [Google Scholar] [CrossRef]
- Chiereghin, A.; Pavia, C.; Gabrielli, L.; Piccirilli, G.; Squarzoni, D.; Turello, G.; Gibertoni, D.; Simonazzi, G.; Capretti, M.G.; Lanari, M.; et al. Clinical evaluation of the new Roche platform of serological and molecular cytomegalovirus-specific assays in the diagnosis and prognosis of congenital cytomegalovirus infection. J. Virol. Methods 2017, 248, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Zavattoni, M.; Lombardi, G.; Rognoni, V.; Furione, M.; Klersy, C.; Stronati, M.; Baldanti, F. Maternal, fetal, and neonatal parameters for prognosis and counseling of HCMV congenital infection. J. Med. Virol. 2014, 86, 2163–2170. [Google Scholar] [CrossRef] [PubMed]
- NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 June 2023).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Pass, R.F.; Fowler, K.B.; Boppana, S.B.; Britt, W.J.; Stagno, S. Congenital cytomegalovirus infection following first trimester maternal infection: Symptoms at birth and outcome. J. Clin. Virol. 2006, 35, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus infection during pregnancy: State of the science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef] [PubMed]
- Goderis, J.; De Leenheer, E.; Smets, K.; Van Hoecke, H.; Keymeulen, A.; Dhooge, I. Hearing Loss and Congenital CMV Infection: A Systematic Review. Pediatrics 2014, 134, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Guerra, B.; Simonazzi, G.; Puccetti, C.; Lanari, M.; Farina, A.; Lazzarotto, T.; Rizzo, N. Ultrasound prediction of symptomatic congenital cytomegalovirus infection. Am. J. Obstet. Gynecol. 2008, 198, 380.e1–380.e7. [Google Scholar] [CrossRef] [PubMed]
- Hui, L.; Wood, G. Perinatal outcome after maternal primary cytomegalovirus infection in the first trimester: A practical update and counseling aid. Prenat Diagn. 2015, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Grosse, S.D.; Ross, D.S. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev. Med. Virol. 2007, 17, 355–363. [Google Scholar] [CrossRef]
- de Romanelli, R.M.C.; Magny, J.F.; Jacquemard, F. Prognostic markers of symptomatic congenital cytomegalovirus infection. Braz. J. Infect. Dis. 2008, 12, 38–43. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Ghout, I.; Bussières, L.; Stirnemann, J.; Magny, J.F.; Couderc, S.; Salomon, L.J.; Guilleminot, T.; Aegerter, P.; Benoist, G.; et al. In utero treatment of congenital cytomegalovirus infection with valacyclovir in a multicenter, open-label, phase II study. Am. J. Obstet. Gynecol. 2016, 215, 462.e1–462.e10. [Google Scholar] [CrossRef] [PubMed]
- Jacquemard, F.; Yamamoto, M.; Costa, J.M.; Romand, S.; Jaqz-Aigrain, E.; Dejean, A.; Daffos, F.; Ville, Y. Maternal administration of valaciclovir in symptomatic intrauterine cytomegalovirus infection. BJOG 2007, 114, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, F.; Marinceu, D.; Prasad, S.; Khalil, A. Effectiveness and safety of prenatal valacyclovir for congenital cytomegalovirus infection: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2023, 61, 436–444. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Studies Included in the Meta-Analysis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study and First Author | Country of Origin | Years | Study Design | Total (n) | Sym (n) | Mean VL in Sym c/mL | Asym (n) | Mean VL in Asym c/mL | Timing of Amniocentesis (wks) | CNS Findings | Extra CNS Findings | Diagnostic Tool | Neonatal Outcome and Length of Follow Up |
| Studies reporting fetal outcomes only | |||||||||||||
| Fabri 2010 [19] | Italy | 1995–2009 | RS | 47 | 16 | 2.2e+08 | 31 | 1.6e+07 | NOS | VM, microcephaly, MRI alteration | echogenic bowel, Ascites, hyperechogenic liver, pelvic effusion, enlarged placenta | US and MRI | N/A |
| Gabrielli 2009 [20] | Italy | NOS | RS | 34 | 12 | 2.3e+06 | 22 | 1.6e+06 | 20–21 | VM, periventricular heterogenicity, hydrocephalus | FGR, echogenic bowel, hepatomegaly | US | N/A |
| Vorontsov 2022 [11] | Israel | NOS | RS | 43 | 17 | 3.2e+06 | 26 | 147,910 | 20–23 (and at least 6 wks after the assumed time of infection | US—temporal cysts, hyperechogenic ventricular wall, cortical and thalamic calcifications, VM > 15 mm, ACC, polymicrogyria, head circumference < 2 SD, white matter cystic lesions, periventricular hyper echogenicity and cysts, small cerebellum, intracerebral calcifications, porencephalic cyst in the occipital lobe; periventricular calcifications, intraventricular adhesions, temporal cysts, mild VM, hypoplasia of corpus callosum, enlarged cisterna magna. MRI—temporal cysts, polymicrogyria, occipital and temporal cysts | hydrops (ascites, pericardial effusion, cardiomegaly) echogenic bowel, liver calcifications, placentomegaly, | US and MRI | N/A |
| Mappa 2023 [21] | Italy | 2012–2021 | RS | 104 | 15 | 3.3e+06 | 89 | 761,934 | Symptomatic—20.6 ± 1.18 Asymptomatic 20.5 ± 1.39 (p = 0.81) | microcephaly, periventricular pseudo cyst, VM with intracranial calcifications, malformations of cortical development, destructive encephalopathy, intracranial calcifications in basal ganglia or germinal matrix | NOS | US and MRI | N/A |
| Studies reporting fetal and neonatal outcomes | |||||||||||||
| Chiereghin 2017 [22] | Italy | NOS | RS | 45 | 19 | 4.3e+06 | 26 | 3.6e+06 | 20–21 (and at least 6–8 wks after maternal infection) | NOS | NOS | NOS | NOS |
| Desveaux 2016 1 [12] | France | NOS | RS Fetal comparison | 44 | 19 | 2.1e+07 | 25 | 445,123 | Symptomatic—mean 23 (17–29) Asymptomatic—mean 22 (range 17–29) (p = 0.4) | lissencephaly, diffuse white matter lesions, intraventricular adhesions, microcephaly, intra-cerebral clastic lesions, multiple intracerebral calcifications, hypoplasia of the corpus callosum, VM, PVL, lateral ventricle partitioning, periventricular necrosis. | hepatomegaly, ascites, echogenic bowel, liver calcifications, FGR, pericardial effusion, placentomegaly | US and MRI | N/A |
| Desveaux 2016 2 [12] | RS Neonatal comparison | 34 | 9 | 2.0e+07 | 25 | 445,123 | N/A | N/A | US and MRI | Severe psychomotor delay, epilepsy, bilateral hearing loss. 36 m follow-up | |||
| Studies reporting neonatal outcomes only | |||||||||||||
| Zavattoni 2014 [23] | Italy | 1995–2009 | RS | 62 | 15 | 5.9e+06 | 47 | 130,000 | Median 21 (range 18–35) with a time interval of 13 weeks (range 2–14) between maternal infection and amniocentesis | N/A | US and MRI | chorioretinitis, hearing loss, petechiae, hepatomegaly, hepatitis, thrombocytopenia, prematurity, anemia, SGA, hypotonia. 6y follow-up | |
| Goegebuer 2009 [17] | Belgium | 2002–2006 | RS | 30 | 15 | 49,276 | 15 | 379,298 | 15.5−32.1 | N/A | N/A | US | preterm birth, SGA, petechiae or purpura, hepatosplenomegaly, CNS abnormalities, elevated liver enzymes, thrombocytopenia or conjugated hyperbilirubinemia, neurologic disturbances, delays in psychomotor and/or mental developmental status, and CMV-related audiological or visual problem. Up to 3 yrs of follow-up |
| Total (n) | 443 | 137 | 306 | ||||||||||
| Study | Population Selection | Exposure | Overall | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Was the research question or objective in this paper clearly stated and appropriate? | Was the study population clearly specified and defined? | Did the authors include a sample size justification? | Were controls selected or recruited from the same or similar population that gave rise to the cases (including the same timeframe)? | Were the definitions, inclusion and exclusion criteria, algorithms or processes used to identify or select cases and controls valid, reliable, and implemented consistently across all study participants? | Were the cases clearly defined and differentiated from controls? | If less than 100 percent of eligible cases and/or controls were selected for the study, were the cases and/or controls randomly selected from those eligible? | Was there use of concurrent controls? | Were the investigators able to confirm that the exposure/risk occurred prior to the development of the condition or event that defined a participant as a case? | Were the measures of exposure/risk clearly defined, valid, reliable, and implemented consistently (including the same time period) across all study participants? | Were the assessors of exposure/risk blinded to the case or control status of participants? | Were key potential confounding variables measured and adjusted statistically in the analyses? If matching was used, did the investigators account for matching during study analysis? | ||
| Fabri [19] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Fair |
| Chiereghin [22] | 3 | 3 | 2 | 3 | 3 | 2 | 1 | 2 | 3 | 3 | 2 | 2 | Good |
| Desveaux [12] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Good |
| Gabrielli [20] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Fair |
| Vorontsov [11] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Good |
| Zavatoni [23] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Fair |
| Goegebuer [17] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Fair |
| Mappa [21] | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 2 | 2 | Good |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilad, N.; Agrawal, S.; Philippopoulos, E.; Murphy, K.E.; Shinar, S. Is a Higher Amniotic Fluid Viral Load Associated with a Greater Risk of Fetal Injury in Congenital Cytomegalovirus Infection—A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 2136. https://doi.org/10.3390/jcm13072136
Gilad N, Agrawal S, Philippopoulos E, Murphy KE, Shinar S. Is a Higher Amniotic Fluid Viral Load Associated with a Greater Risk of Fetal Injury in Congenital Cytomegalovirus Infection—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(7):2136. https://doi.org/10.3390/jcm13072136
Chicago/Turabian StyleGilad, Noa, Swati Agrawal, Eleni Philippopoulos, Kellie E. Murphy, and Shiri Shinar. 2024. "Is a Higher Amniotic Fluid Viral Load Associated with a Greater Risk of Fetal Injury in Congenital Cytomegalovirus Infection—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 7: 2136. https://doi.org/10.3390/jcm13072136
APA StyleGilad, N., Agrawal, S., Philippopoulos, E., Murphy, K. E., & Shinar, S. (2024). Is a Higher Amniotic Fluid Viral Load Associated with a Greater Risk of Fetal Injury in Congenital Cytomegalovirus Infection—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(7), 2136. https://doi.org/10.3390/jcm13072136