
Trifecta Outcomes of Robot-Assisted Partial Nephrectomy Using the New Hugo™ RAS System Versus Laparoscopic Partial Nephrectomy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Endpoints, Outcome, and Statistical Analysis
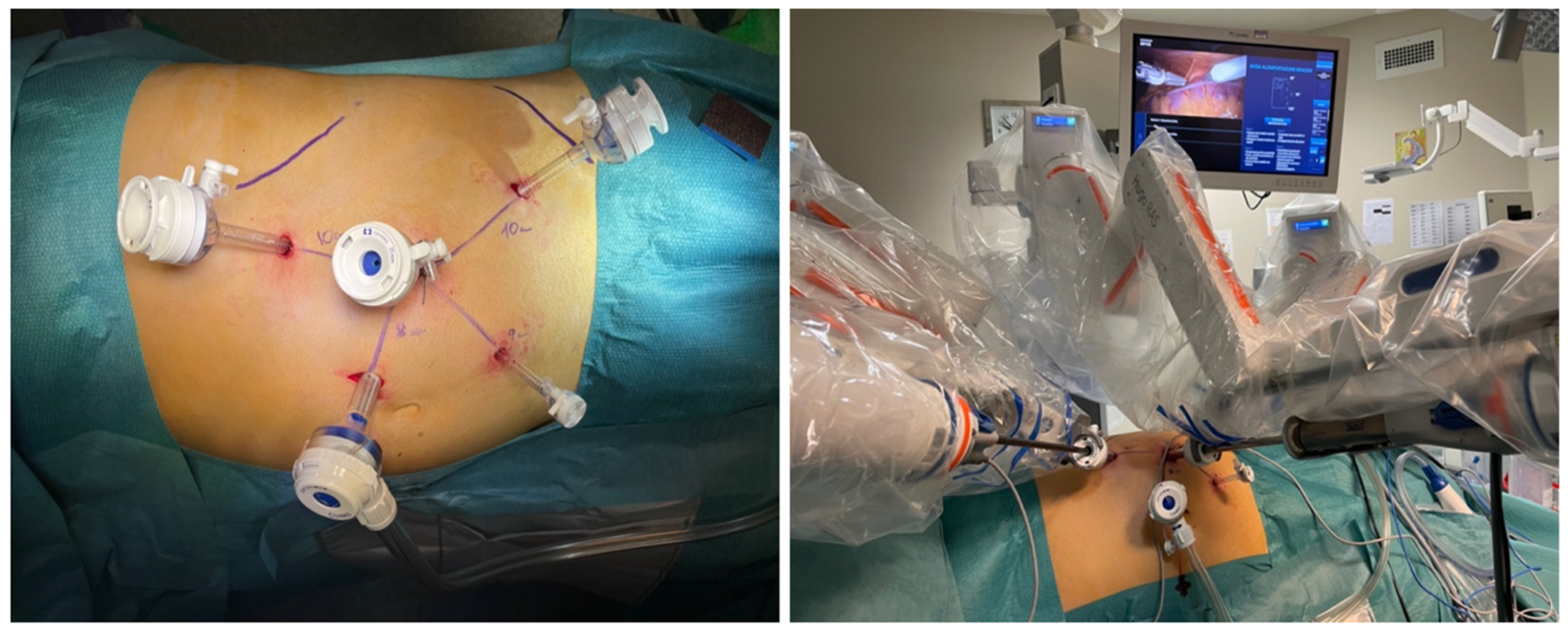
2.3. Trocar Configuration and Surgical Procedure
2.4. Post-Operative Management and Follow-Up
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bukavina, L.; Bensalah, K.; Bray, F.; Carlo, M.; Challacombe, B.; Karam, J.A.; Kassouf, W.; Mitchell, T.; Montironi, R.; O’Brien, T.; et al. Epidemiology of Renal Cell Carcinoma: 2022 Update. Eur. Urol. 2022, 82, 529–542. [Google Scholar] [CrossRef]
- Campi, R.; Sessa, F.; Corti, F.; Carrion, D.M.; Mari, A.; Amparore, D.; Mir, M.C.; Fiori, C.; Papalia, R.; Kutikov, A.; et al. Triggers for delayed intervention in patients with small renal masses undergoing active surveillance: A systematic review. Minerva Urol. Nefrol. 2020, 72, 389–407. [Google Scholar] [CrossRef]
- Napolitano, L.; Orecchia, L.; Giulioni, C.; Carbonara, U.; Tavella, G.; Lizzio, L.; Fimognari, D.; De Palma, A.; Gheza, A.; Grosso, A.A.; et al. The Role of miRNA in the Management of Localized and Advanced Renal Masses, a Narrative Review of the Literature. Appl. Sci. 2023, 13, 275. [Google Scholar] [CrossRef]
- Marchioni, M.; Rivas, J.G.; Autran, A.; Socarras, M.; Albisinni, S.; Ferro, M.; Schips, L.; Scarpa, R.M.; Papalia, R.; Esperto, F. Biomarkers for Renal Cell Carcinoma Recurrence: State of the Art. Curr. Urol. Rep. 2021, 22, 31. [Google Scholar] [CrossRef]
- Petrozza, V.; Pastore, A.L.; Palleschi, G.; Tito, C.; Porta, N.; Ricci, S.; Marigliano, C.; Costantini, M.; Simone, G.; Di Carlo, A.; et al. Secreted miR-210-3p as non-invasive biomarker in clear cell renal cell carcinoma. Oncotarget 2017, 8, 69551–69558. [Google Scholar] [CrossRef]
- Rouprêt, M.; Seisen, T.; Birtle, A.J.; Capoun, O.; Compérat, E.M.; Dominguez-Escrig, J.L.; Gürses Andersson, I.; Liedberg, F.; Mariappan, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur. Urol. 2023, 84, 49–64. [Google Scholar] [CrossRef]
- Tuderti, G.; Mastroianni, R.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Ferriero, M.; Misuraca, L.; Guaglianone, S.; Costantini, M.; Torregiani, G.; et al. Assessing the Trade-off Between the Safety and Effectiveness of Off-clamp Robotic Partial Nephrectomy for Renal Masses with a High RENAL Score: A Propensity Score-matched Comparison of Perioperative and Functional Outcomes in a Multicenter Analysis. Eur. Urol. Focus. 2023, 9, 1037–1043. [Google Scholar] [CrossRef]
- Bradshaw, A.W.; Autorino, R.; Simone, G.; Yang, B.; Uzzo, R.G.; Porpiglia, F.; Capitanio, U.; Porter, J.; Bertolo, R.; Minervini, A.; et al. Robotic partial nephrectomy vs minimally invasive radical nephrectomy for clinical T2a renal mass: A propensity score-matched comparison from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. BJU Int. 2020, 126, 114–123. [Google Scholar] [CrossRef]
- Papalia, R.; Simone, G.; Ferriero, M.; Guaglianone, S.; Costantini, M.; Giannarelli, D.; Maini, C.L.; Forastiere, E.; Gallucci, M. Laparoscopic and robotic partial nephrectomy without renal ischaemia for tumours larger than 4 cm: Perioperative and functional outcomes. World J. Urol. 2012, 30, 671–676. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Guaglianone, S.; Forestiere, E.; Gallucci, M. Preoperative superselective transarterial embolization in laparoscopic partial nephrectomy: Technique, oncologic, and functional outcomes. J. Endourol. 2009, 23, 1473–1478. [Google Scholar] [CrossRef]
- Brassetti, A.; Anceschi, U.; Bove, A.M.; Prata, F.; Costantini, M.; Ferriero, M.; Mastroianni, R.; Misuraca, L.; Tuderti, G.; Torregiani, G.; et al. Purely Off-Clamp Laparoscopic Partial Nephrectomy Stands the Test of Time: 15 Years Functional and Oncologic Outcomes from a Single Center Experience. Curr. Oncol. 2023, 30, 1196–1205. [Google Scholar] [CrossRef]
- Takagi, T.; Yoshida, K.; Kondo, T.; Kobayashi, H.; Iizuka, J.; Okumi, M.; Ishida, H.; Nagashima, Y.; Tanabe, K. Peritumoral pseudocapsule status according to pathological characteristics from robot-assisted laparoscopic partial nephrectomy for localized renal cell carcinoma. Int. J. Urol. 2019, 26, 446–450. [Google Scholar] [CrossRef]
- Prata, F.; Ragusa, A.; Anceschi, U.; Civitella, A.; Tuzzolo, P.; Tedesco, F.; Cacciatore, L.; Iannuzzi, A.; Callè, P.; Raso, G.; et al. Hugo RAS Robot-Assisted Partial Nephrectomy for High-Nephrometry Score Complex Renal Mass: Case Report and Surgical Technique. Videourology 2023, 37. Available online: https://home.liebertpub.com/vid (accessed on 16 March 2024). [CrossRef]
- Prata, F.; Ragusa, A.; Anceschi, U.; Iannuzzi, A.; Tedesco, F.; Cacciatore, L.; Civitella, A.; Tuzzolo, P.; Cirillo, R.; Callè, P.; et al. Three-arms off-clamp robot-assisted partial nephrectomy with the new Hugo robot-assisted surgery system. BJU Int. 2024, 133, 48–52. [Google Scholar] [CrossRef]
- Simone, G.; Ferriero, M.; Papalia, R.; Costantini, M.; Guaglianone, S.; Gallucci, M. Zero-ischemia minimally invasive partial nephrectomy. Curr. Urol. Rep. 2013, 14, 465–470. [Google Scholar] [CrossRef]
- Simone, G.; Tuderti, G.; Anceschi, U.; Papalia, R.; Ferriero, M.; Misuraca, L.; Minisola, F.; Mastroianni, R.; Costantini, M.; Guaglianone, S.; et al. Oncological outcomes of minimally invasive partial versus minimally invasive radical nephrectomy for cT1-2/N0/M0 clear cell renal cell carcinoma: A propensity score-matched analysis. World J. Urol. 2017, 35, 789–794. [Google Scholar] [CrossRef]
- Carbonara, U.; Simone, G.; Capitanio, U.; Minervini, A.; Fiori, C.; Larcher, A.; Checcucci, E.; Amparore, D.; Crocerossa, F.; Veccia, A.; et al. Robot-assisted partial nephrectomy: 7-Year outcomes. Minerva Urol. Nephrol. 2021, 73, 540–543. [Google Scholar] [CrossRef]
- Brassetti, A.; Ragusa, A.; Tedesco, F.; Prata, F.; Cacciatore, L.; Iannuzzi, A.; Bove, A.M.; Anceschi, U.; Proietti, F.; D’annunzio, S.; et al. Robotic Surgery in Urology: History from PROBOT® to, H.U.G.O.T.M. Sensors 2023, 23, 7104. [Google Scholar] [CrossRef]
- Prata, F.; Ragusa, A.; Tempesta, C.; Iannuzzi, A.; Tedesco, F.; Cacciatore, L.; Raso, G.; Civitella, A.; Tuzzolo, P.; Callè, P.; et al. State of the Art in Robotic Surgery with Hugo RAS System: Feasibility, Safety and Clinical Applications. J. Pers. Med. 2023, 13, 1233. [Google Scholar] [CrossRef]
- Anceschi, U.; Ferriero, M.C.; Tuderti, G.; Brassetti, A.; Bertolo, R.; Capitanio, U.; Larcher, A.; Garisto, J.; Antonelli, A.; Mottrie, A.; et al. Head to Head Impact of Margin, Ischemia, Complications, Score Versus a Novel Trifecta Score on Oncologic and Functional Outcomes After Robotic-assisted Partial Nephrectomy: Results of a Multicenter Series. Eur. Urol. Focus 2021, 7, 1391–1399. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Prata, F.; Ragusa, A.; Civitella, A.; Tuzzolo, P.; Tedesco, F.; Cacciatore, L.; Iannuzzi, A.; Callè, P.; Raso, G.; Fantozzi, M.; et al. Robot-assisted partial nephrectomy using the novel HugoTM RAS system: Feasibility, setting and perioperative outcomes of the first off-clamp series. Urologia 2024. [Google Scholar] [CrossRef]
- Huang, W.C.; Levey, A.S.; Serio, A.M.; Snyder, M.; Vickers, A.J.; Raj, G.V.; Scardino, P.T.; Russo, P. Chronic kidney disease after nephrectomy in patients with renal cortical tumours: A retrospective cohort study. Lancet Oncol. 2006, 7, 735–740. [Google Scholar] [CrossRef]
- MacLennan, S.; Imamura, M.; Lapitan, M.C.; Omar, M.I.; Lam, T.B.; Hilvano-Cabungcal, A.M.; Royle, P.; Stewart, F.; MacLennan, G.; MacLennan, S.J.; et al. Systematic review of perioperative and quality-of-life outcomes following surgical management of localised renal cancer. Eur. Urol. 2012, 62, 1097–1117. [Google Scholar] [CrossRef]
- Thompson, R.H.; Boorjian, S.A.; Lohse, C.M.; Leibovich, B.C.; Kwon, E.D.; Cheville, J.C.; Blute, M.L. Radical nephrectomy for pT1a renal masses may be associated with decreased overall survival compared with partial nephrectomy. J. Urol. 2008, 179, 468–473. [Google Scholar] [CrossRef]
- Capitanio, U.; Terrone, C.; Antonelli, A.; Minervini, A.; Volpe, A.; Furlan, M.; Matloob, R.; Regis, F.; Fiori, C.; Porpiglia, F.; et al. Nephron-sparing techniques independently decrease the risk of cardiovascular events relative to radical nephrectomy in patients with a T1a-T1b renal mass and normal preoperative renal function. Eur. Urol. 2015, 67, 683–689. [Google Scholar] [CrossRef]
- Simone, G.; De Nunzio, C.; Ferriero, M.; Cindolo, L.; Brookman-May, S.; Papalia, R.; Sperduti, I.; Collura, D.; Leonardo, C.; Anceschi, U.; et al. Trends in the use of partial nephrectomy for cT1 renal tumors: Analysis of a 10-yr European multicenter dataset. Eur. J. Surg. Oncol. 2016, 42, 1729–1735. [Google Scholar] [CrossRef]
- Papalia, R.; De Castro Abreu, A.L.; Panebianco, V.; Duddalwar, V.; Simone, G.; Leslie, S.; Guaglianone, S.; Tejura, T.; Ferriero, M.; Costantini, M.; et al. Novel kidney segmentation system to describe tumour location for nephron-sparing surgery. World J. Urol. 2015, 33, 865–871. [Google Scholar] [CrossRef]
- Simone, G.; Capitanio, U.; Tuderti, G.; Presicce, F.; Leonardo, C.; Ferriero, M.; Misuraca, L.; Costantini, M.; Larcher, A.; Minisola, F.; et al. On-clamp versus off-clamp partial nephrectomy: Propensity score-matched comparison of long-term functional outcomes. Int. J. Urol. 2019, 26, 985–991. [Google Scholar] [CrossRef]
- Bertolo, R.; Simone, G.; Garisto, J.; Nakhoul, G.; Armanyous, S.; Agudelo, J.; Costantini, M.; Tuderti, G.; Gallucci, M.; Kaouk, J. Off-clamp vs on-clamp robotic partial nephrectomy: Perioperative, functional and oncological outcomes from a propensity-score matching between two high-volume centers. Eur. J. Surg. Oncol. 2019, 45, 1232–1237. [Google Scholar] [CrossRef]
- Chang, K.D.; Abdel Raheem, A.; Kim, K.H.; Oh, C.K.; Park, S.Y.; Kim, Y.S.; Ham, W.S.; Han, W.K.; Choi, Y.D.; Chung, B.H.; et al. Functional and oncological outcomes of open, laparoscopic and robot-assisted partial nephrectomy: A multicentre comparative matched-pair analyses with a median of 5 years’ follow-up. BJU Int. 2018, 122, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Alimi, Q.; Peyronnet, B.; Sebe, P.; Cote, J.-F.; Kammerer-Jacquet, S.-F.; Khene, Z.-E.; Pradere, B.; Mathieu, R.; Verhoest, G.; Guillonneau, B.; et al. Comparison of Short-Term Functional, Oncological, and Perioperative Outcomes Between Laparoscopic and Robotic Partial Nephrectomy Beyond the Learning Curve. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.E.; You, J.H.; Kim, D.K.; Rha, K.H.; Lee, S.H. Comparison of perioperative outcomes between robotic and laparoscopic partial nephrectomy: A systematic review and meta-analysis. Eur. Urol. 2015, 67, 891–901. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Overall (n = 89) | RAPN (n = 27) Group A | Laparoscopic PN (n = 62) Group B | p-Value |
|---|---|---|---|---|
| Age (n, median, IQR) | 66 (55–72) | 68 (57–73) | 65.5 (54–72) | 0.55 |
| Gender (n, %) | ||||
|
|
|
| 0.04 |
| BMI (kg/m2, median, IQR) | 27 (24.3–30.1) | 27.4 (25.9–31.2) | 26.3 (24–30.1) | 0.19 |
| ASA score (n, %) | ||||
|
|
|
| 0.06 |
| Charlson Comorbidity Index (median, IQR) | 4 (4–5) | 4 (3–5) | 4 (4–5) | 0.81 |
| Diabetes (n, %) | 12 (13.5%) | 2 (7.4%) | 10 (16.1%) | 0.26 |
| Hypertension (n, %) | 48 (53.9%) | 14 (51.8%) | 34 (54.8%) | 0.79 |
| Preoperative Hemoglobin (g/dL, median, IQR) | 14.7 (13.3–15.4) | 14.7 (12.3–15.4) | 14.6 (13.2–15.4) | 0.77 |
| Preoperative Creatinine (mg/dL, median, IQR) | 0.91 (0.76–1.02) | 0.93 (0.81–1.09) | 0.90 (0.73–1.00) | 0.17 |
| Preoperative eGFR (mL/min/1.73 m2, median, IQR) | 84.6 (69.8–26.5) | 77.5 (64.2–92.3) | 85.6 (70.3–99.8) | 0.08 |
| Clinical Tumor Size (mm, median, IQR) | 31 (20–44) | 34 (26–45) | 29 (19–44) | 0.14 |
| cT (n, %) | ||||
|
|
|
| 0.22 |
| Side (n, %) | ||||
|
|
|
| |
| 0.51 | ||||
| R.E.N.A.L. score (median, IQR) | 6 (5–7) | 7 (5–8) | 6 (5–7) | 0.11 |
| Variable | Overall (n = 89) | RAPN (n = 27) Group A | Laparoscopic PN (n = 62) Group B | p-Value |
|---|---|---|---|---|
| Operative Time (min, median, IQR) | 135 (75–197) | 91 (50–149) | 149.5 (83–203) | 0.005 |
| Estimated blood loss (mL, median, IQR) | 100 (50–300) | 150 (50–450) | 100 (50–200) | 0.20 |
| Perioperative complications (n, %) | 9 (10.1%) | 3 (11.1%) | 6 (9.7%) | 0.07 |
| Length of Stay (days, median, IQR) | 4 (3–5) | 3 (3–4) | 5 (4–5) | 0.002 |
| Hemoglobin at discharge (g/dL, median, IQR) | 11.6 (10.4–12.5) | 11.2 (9.1–12.3) | 11.8 (10.5–12.7) | 0.09 |
| Creatinine at discharge (mg/dL, median, IQR) | 0.93 (0.77–1.1) | 0.93 (0.82–1.13) | 0.92 (0.75–1.1) | 0.67 |
| eGFR at discharge (mL/min/1.73 m2, median, IQR) | 79.5 (63–92.1) | 74.9 (63–92.1) | 80.1 (63–92.1) | 0.85 |
| Readmission (n, %) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Pathological Size (mm, median, IQR) | 30 (14–40) | 30 (20–43) | 30 (13–40) | 0.23 |
| Pathology (n, %) | ||||
|
|
|
| |
| 0.07 | ||||
| Histology_subtype (n, %) | ||||
|
|
|
| 0.27 |
| Positive Margins (n, %) | 4 (4.5%) | 1 (3.7%) | 3 (4.8%) | 0.82 |
| pT Stage (n, %) | ||||
|
|
|
| 0.11 |
| Last follow-up (months, median, IQR) | 5 (1–9) | 2 (1–5) | 5 (1–9) | |
| Creatinine at last follow-up (mg/dL, median, IQR) | 0.98 (0.85–1.13) | 0.99 (0.85–1–14) | 0.97 (0.79–1.08) | 0.53 |
| eGFR at last follow-up (mL/min/1.73 m2, median, IQR) | 79.3 (58.7–88.7) | 79.3 (58.3–87.8) | 78 (60.6–90) | 0.97 |
| Trifecta achievement rate (%) | 71 (85.4%) | 25 (92.6%) | 51 (82.3%) | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prata, F.; Ragusa, A.; Tedesco, F.; Pira, M.; Iannuzzi, A.; Fantozzi, M.; Civitella, A.; Scarpa, R.M.; Papalia, R. Trifecta Outcomes of Robot-Assisted Partial Nephrectomy Using the New Hugo™ RAS System Versus Laparoscopic Partial Nephrectomy. J. Clin. Med. 2024, 13, 2138. https://doi.org/10.3390/jcm13072138
Prata F, Ragusa A, Tedesco F, Pira M, Iannuzzi A, Fantozzi M, Civitella A, Scarpa RM, Papalia R. Trifecta Outcomes of Robot-Assisted Partial Nephrectomy Using the New Hugo™ RAS System Versus Laparoscopic Partial Nephrectomy. Journal of Clinical Medicine. 2024; 13(7):2138. https://doi.org/10.3390/jcm13072138
Chicago/Turabian StylePrata, Francesco, Alberto Ragusa, Francesco Tedesco, Matteo Pira, Andrea Iannuzzi, Marco Fantozzi, Angelo Civitella, Roberto Mario Scarpa, and Rocco Papalia. 2024. "Trifecta Outcomes of Robot-Assisted Partial Nephrectomy Using the New Hugo™ RAS System Versus Laparoscopic Partial Nephrectomy" Journal of Clinical Medicine 13, no. 7: 2138. https://doi.org/10.3390/jcm13072138