
Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review


Abstract
:1. Introduction
2. Methods
3. Epidemiology
4. Pathophysiology and Clinic
4.1. Skeletal Problems
4.2. Neuropsychiatric Disturbances
4.3. Immunodeficiency
4.4. Diagnosis of PAD
- Inspection of the legs and feet;
- Bilateral palpation of the femoral, popliteal, ankle, and foot pulses;
- Doppler sonographic measurement of the ankle–brachial index (ABI) or toe–brachial index (TBI);
- Duplex sonography of the pelvic and leg arteries;
- Digital diagnostic/therapeutic subtraction angiography (DSA);
- MRA and CTA.
5. Classifications
6. Therapy
7. Revascularization
8. Recurrence and Follow-Up
9. Conclusions for Practice
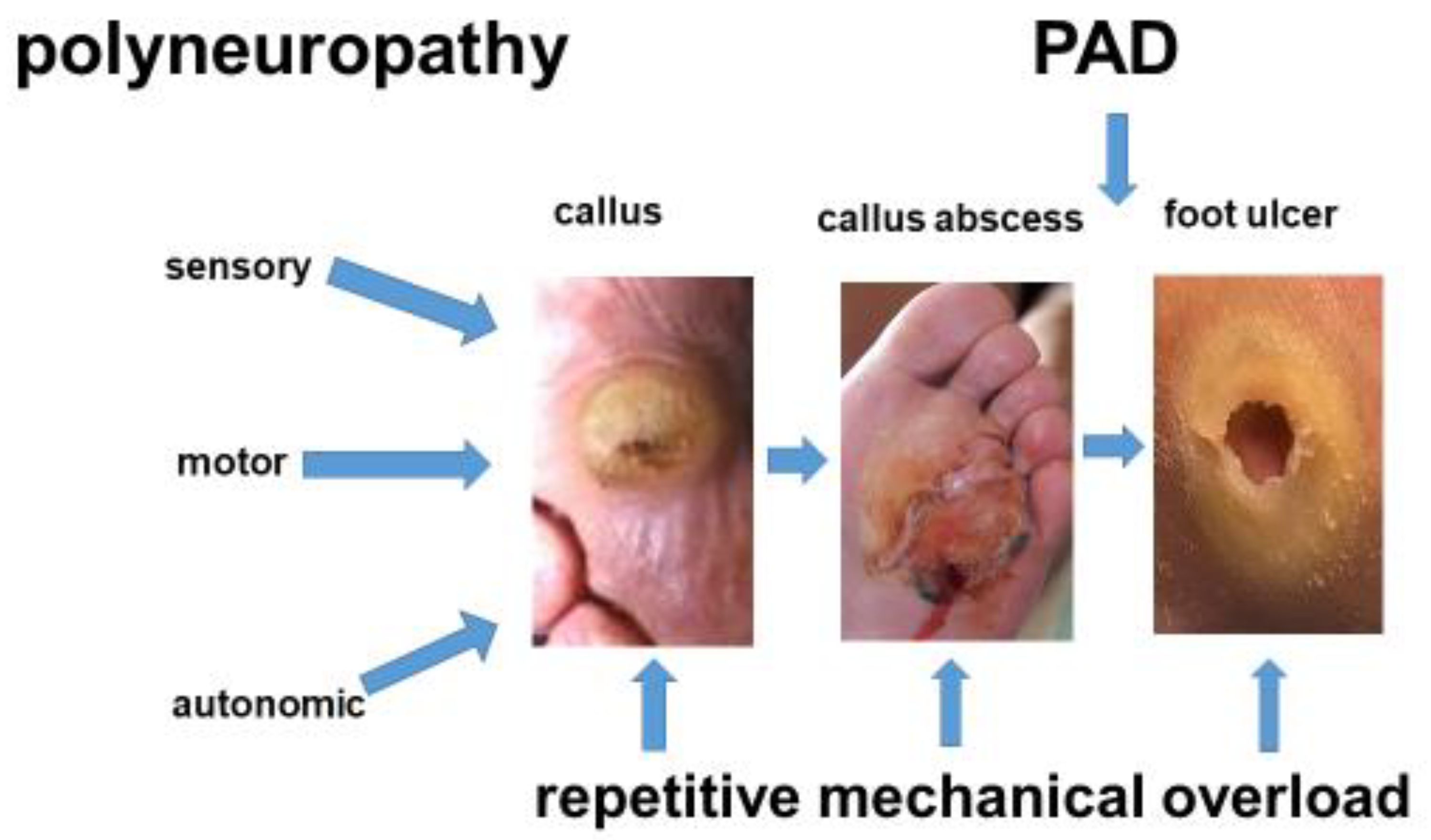
- Mechanical overload in PAD patients is painful. In DFS patients, it leads to painless foot ulcers;
- In PAD, the degree of ischemia is reflected by the ankle–brachial index (ABI). In DFS, the ABI is misleading, owing to PNP-driven mediasclerosis of the infrapopliteal arteries;
- Tissue loss in PAD reflects CLTI, while foot lesions in DFS primarily indicate PNP. Since PNP may mask CLTI, assessment of the arterial perfusion of the legs is mandatory for both patient groups;
- In PAD, occlusive processes are localized more proximally (pelvic, femoral arteries) than in neuroischemic DFS (crural–pedal arteries). PNP-related vascular pathologies (media sclerosis, chronic capillary ischemia) additionally reduce the blood flow to the feet in DFS patients;
- PAD and DFS represent fundamentally different pathophysiological entities. Hence, therapeutic concepts differ substantially between the two patient populations;
- Revascularization is crucial in PAD patients. In DFS patients, offloading and stage-appropriate wound care predominate the interdisciplinary treatment concept. Revascularization is mandatory if coexisting PAD prevents the healing of foot lesions;
- Classifying DFS patients according to the degree of ischemia (Fontaine, Rutherford) may be misleading since ABI measurement is not reliable, and the criterion “pain” is missing.
Funding
Conflicts of Interest
References
- Fowkes, F.G.R.; Aboyans, V.; Fowkes, F.J.; McDermott, M.M.; Sampson, U.K.; Criqui, M.H. Peripheral arterial disease: Epidemiology and global perspectives. Nature reviews. Cardiology 2017, 14, 156–170. [Google Scholar] [PubMed]
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef] [PubMed]
- IDF Diabetes Atlas, 10th ed.; International Diabetes Federation, 2022; Available online: https://www.diabetesatlas.org (accessed on 23 February 2024).
- Chantelau, E.A. Nociception at the diabetic foot, an uncharted territory. World J. Diabetes 2015, 6, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Hochlenert, D.; Engels, G.; Morbach, S.; Schliwa, S.; Game, F.L. (Eds.) Das Diabetische Fußsyndrom—Über die Entität zur Therapie, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2022; ISBN 978-3-662-64971-8. [Google Scholar] [CrossRef]
- Prompers, L.; Schaper, N.; Apelqvist, J.; Edmonds, M.; Jude, E.; Mauricio, D.; Uccioli, L.; Urbancic, V.; Bakker, K.; Holstein, P.; et al. Prediction of outcome in individuals with diabetic foot ulcers: Focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia 2008, 51, 747–754. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Reiber, G.E.; Vileikyte, L.; Boyko, E.J.; Del Aguila, M.; Smith, D.G.; Lavery, L.A.; Boulton, A.J.M. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999, 22, 157–162. [Google Scholar] [CrossRef]
- Pecoraro, R.E.; Reiber, G.E.; Burgess, E.M. Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care 1990, 13, 513–521. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; for the Joint, G.W.G. Global vascular guidelines on the management of chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 3S–125S. [Google Scholar] [CrossRef] [PubMed]
- Lawall, H.; Huppert, P.; Espinola-Klein, C.; Rümenapf, G. The diagnosis and treatment of peripheral arterial vascular disease. Dtsch. Ärzteblatt Int. 2016, 113, 729–736. [Google Scholar] [CrossRef]
- Diehm, C.; Schuster, A.; Allenberg, J.R.; Darius, H.; Haberl, R.; Lange, S.; Pittrow, D.; von Stritzky, B.; Tepohl, G.; Trampisch, H.J. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: Cross-sectional study. Atherosclerosis 2004, 172, 95–105. [Google Scholar] [CrossRef]
- Hockley, T. Executive Summary: Peripheral Patients? Peripheral Arterial Disease: A Health Policy Review; LSE London School of Economics and Political Science: London, UK, 2016; Atlas ID: (2016)1,014,968.011. [Google Scholar]
- Martelli, E.; Enea, I.; Zamboni, M.; Federici, M.; Bracale, U.M.; Sangiorgi, G.; Martelli, A.R.; Messina, T.; Settembrini, A.M. Focus on the Most Common Paucisymptomatic Vasculopathic Population, from Diagnosis to Secondary Prevention of Complications. Diagnostics 2023, 13, 2356. [Google Scholar] [CrossRef] [PubMed]
- Tönnies, T.; Röckl, A.; Hoyer, A.; Heidemann, C.; Baumert, J.; Du, Y.; Scheidt-Nave, C.; Brinks, R. Projected number of people with diabetes in Germany in 2040. Diabetes Med. 2019, 36, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Tönnies, T.; Brinks, R.; Kuss, O.; Hering, R.; Schulz, M. Spatio-temporal trends in the incidence of type 2 diabetes in Germany—Analysis of the claims data of 63 million persons with statutory health insurance from 2014 to 2019. Dtsch. Ärzteblatt Int. 2022, 119, 173–179. [Google Scholar] [CrossRef]
- Magliano, D.J.; Islam, R.M.; Barr, E.L.M.; Gregg, E.W.; E Pavkov, M.; Harding, J.L.; Tabesh, M.; Koye, D.N.; E Shaw, J. Trends in incidence of total or type 2 diabetes: Systematic review. BMJ 2019, 366, 15003. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J.M.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apequist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Swerdlow, M.A.; Armstrong, A.A.; Conte, M.S.; Padula, W.V.; Bus, S.A. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J. Foot Ankle Res. 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Zaharia, O.P.; Strassburger, K.; Strom, A.; Bönhof, G.J.; Karusheva, Y.; Antoniou, S.; Bódis, K.; Markgraf, D.F.; Burkart, V.; Müssig, K.; et al. German Diabetes Study Group. Risk of diabetes-associated diseases in subgroups of patients with recent-onset diabetes: A 5-year follow-up study. Lancet Diabetes Endocrinol. 2019, 7, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diabetes Rep. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 diabetes and ist impact on the immune system. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef]
- Sämann, A.; Tajiyeva, O.; Müller, N.; Tschauner, T.; Hoyer, H.; Wolf, G.; Müller, U.A. Prevalence of the diabetic foot syndrome at the primary care level in Germany. A cross-sectional study. Diabetes Med. 2008, 25, 557–563. [Google Scholar] [CrossRef]
- Kröger, K.; Berg, C.; Santosa, F.; Malyar, N.; Reinecke, H. Lower limb amputation in Germany—An analysis of data from the German Federal Statistical Office between 2005 and 2014. Dtsch. Ärzteblatt Int. 2017, 114, 130–136. [Google Scholar]
- Narres, M.; Kvitkina, T.; Claessen, H.; Droste, S.; Schuster, B.; Morbach, S.; Rümenapf, G.; Van Acker, K.; Icks, A. Incidence of lower extremity amputations in the diabetic compared with the non-diabetic population: A systematic review. PLoS ONE 2017, 12, e0182081. [Google Scholar] [CrossRef] [PubMed]
- Claessen, H.; Narres, M.; Haastert, B.; Arend, W.; Hoffmann, F.; Morbach, S.; Rümenapf, G.; Kvitkina, T.; Friedel, H.; Günster, C.; et al. Lower-extremity amputations in people with and without diabetes in Germany, 2008–2012—An analysis of more than 30 million inhabitants. Clin. Epidemiol. 2018, 10, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R. Intersociety consensus fort he management of peripheral arterial disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 2007, 33, S1–S75. [Google Scholar] [CrossRef]
- IWGDF. 2019 IWGDF Guidelines on the Prevention and Management of Diabetic Foot Disease. 2019. Available online: www.iwgdfguidelines.org (accessed on 10 December 2022).
- Morbach, S.; Müller, E.; Reike, H.; Risse, A.; Rümenapf, G.; Spraul, M. Diabetisches Fußsyndrom. Diabetol. Stoffwechs. 2017, 12, 181–189. [Google Scholar] [CrossRef]
- Faglia, E.; Favales, F.; Quarantiello, A. Angiographic evaluation of peripheral arterial occlusive disease and its role as a prognostic determinant for major amputation in diabetic subjects with foot ulcer. Diabetes Care 1998, 4, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Veith, F.J.; Gupta, S.K.; Wengerter, K.R.; Goldsmith, J.; Rivers, S.P.; Bakal, C.W.; Dietzek, A.M.; Cynamon, J.; Sprayregen, S.; Gliedmann, M. Changing arteriosclerotic disease patterns and management strategies in lower-limb-threatening ischemia. Ann. Surg. 1990, 212, 402–412. [Google Scholar] [CrossRef]
- Chabbert-Buffet, N.; LeDevehat, C.; Khodabandhelou, T.; Allaire, E.; Gaitz, J.P.; Tribout, L.; Abdoucheli-Baudot, N.; Vayssairat, M. Evidence for associated cutaneous microangiopathy in diabetic patients with neuropathic foot ulceration. Diabetes Care 2003, 26, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Maegawa, H.; Watada, H.; Yabe, D.; Node, K.; Murohara, T.; Wada, J. Interconnection between cardiovascular, renal and metabolic disorders: A narrative review with a focus on Japan. Diab. Obes. Metabol. 2022, 24, 2283–2296. [Google Scholar] [CrossRef]
- Feldman, E.L.; Nave, K.A.; Jensen, T.S.; Bennett, D.L.H. New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain. Neuron 2017, 93, 1296–1313. [Google Scholar] [CrossRef]
- Jörneskog, G. Why critical limb ischemia criteria are not applicable to diabetic foot and what the consequences are. Scand. J. Surg. 2012, 101, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Forst, T.; Pfützner, A.; Kann, P.; Lobmann, R.; Schäfer, H.; Beyer, J. Association between diabetic autonomic C-fibre neuropathy and medial wall calcification and the significance in the outcome of trophic foot lesions. Exp. Clin. Endocrinol. Diabetes 1995, 103, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Holtz-Neiderer, K.; Wendel, C.; Mohler, M.J.; Kimbriel, H.R.; Lavery, L.A. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am. J. Med. 2007, 120, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Ming, A.; Alhajjar, A.; Walter, I.; Piehler, C.; Hoetzsch, J.; Leuckert, M.; Clemens, V.; Petrow, A.; Siddiquee, I.M.; Scurt, F.G.; et al. Telemedical monitoring of plantar temperature in diabetic patients at risk of foot ulcers—The Randomized Smart Prevent Diabetic Feet Trial. Dtsch. Ärzteblatt Int. 2024, 121, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; Andros, G.; Apelqvist, J.; Bakker, K.; Lammer, J.; Lepäntalo, M.; Mills, J.L.; Reekers, J.; Shearman, C.P.; Zierler, R.E.; et al. Diagnosis and treatment of peripheral arterial disease in diabetic patients with a foot ulcer. A progress report of the International Working Group on the Diabetic Foot. Diabetes Metab. Res. Rev. 2012, 28 (Suppl. 1), 218–224. [Google Scholar] [CrossRef] [PubMed]
- Hinchliffe, R.J.; Forsythe, R.A.; Apelqvist, J.; Boyko, E.J.; Fitrige, R.; Pio Hong, J.; Katsanos, K.; Mills, J.L.; Nikols, S.; Reekers, J.; et al. Guidelines on diagnosis, prognosis, and management of peripheral artery disease in patients with foot ulcers and diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3276. [Google Scholar] [CrossRef]
- Ince, P.; Zulfiquarali, G.A.; Lutale, J.K.; Basit, A.; Mansour Ali, S.; Chonan, F.; Morbach, S.; Möllenberg, J.; Game, F.L.; Jeffcoate, W.J. Use of the SINBAD classification system and score in compaing outcome of foot ulcer management on three continents. Diabetes Care 2008, 31, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Monteiro-Soares, M.; Russell, D.; Boyko, E.J.; Jeffcoate, W.; Mills, J.L.; Morbach, S.; Game, F. Guidelines on the classification of diabetic foot ulcers (IWGDF 2019). Diabetes. Metab. Res. Rev. 2020, 36, e3227. [Google Scholar] [CrossRef]
- Mills, J.L.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. The Society for Vascular Lower Extremity Threatened Limb Classicifation System: Risk Stratifcation based on Wound, Ischemia, and foot infection (WIFI). J. Vasc. Surg. 2014, 59, 220–234. [Google Scholar] [CrossRef]
- Rümenapf, G.; Morbach, S.; Schmidt, A.; Sigl, M. Intermittent claudication and asymptomatic peripheral arterial disease—Conservative treatment versus revascularization. Dtsch. Ärzteblatt Int. 2020, 117, 188–193. [Google Scholar] [CrossRef]
- Hageman, D.; Fokkenrood, H.J.; Gommans, L.N.; van den Houten, M.M.; Teijink, J.A. Supervised exercise therapy versus home-based exercise therapy versus walking advice for intermittent claudication. Cochrane Database Syst. Rev. 2018, 2018, CD005263. [Google Scholar] [CrossRef] [PubMed]
- Musuuza, J.; Sutherland, B.L.; Kurter, S.; Balasubramanian, P.; Bartels, C.M.; Brennan, M.B. A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. J. Vasc. Surg. 2020, 71, 1433–1446. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef]
- Ogurtsova, K.; Morbach, S.; Haastert, B.; Dubský, M.; Rümenapf, G.; Ziegler, D.; Jirkovska, A.; Icks, A. Cumulative long-term recurrence of diabetic foot ulcers in two cohorts from cetres in Germany and the Czech Republic. Diab. Res. Clin. Pract. 2021, 172, 108621. [Google Scholar] [CrossRef]
- Aagaard, T.V.; Moeini, S.; Skou, S.T.; Madsen, U.R.; Brorson, S. Benefits and harms of exercise therapy for patients with diabetic foot ulcers: A systematic review. Int. J. Low. Extrem. Wounds 2022, 21, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.; van Netten, J.J.; on behalf of the International Working Group on the Diabetic Foot. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3369. [Google Scholar]
- Farber, A.; Menard, M.T.; Conte, M.S.; Kaufman, J.A.; Powell, R.J.; Choudhry, N.K.; Hamza, T.H.; Assmann, S.F.; Creager, M.A.; Cziraky, M.J.; et al. Surgery or endovascular therapy for chronic limb-threatening ischemia. N. Engl. J. Med. 2022, 387, 2305–2316. [Google Scholar] [CrossRef]
- Almasri, J.; Adusumalli, J.; Asi, N.; Lakis, S.; Alsawas, M.; Prokop, L.J.; Bradbury, A.; Honours, C.B.; Kolh, P.; Conte, M.S.; et al. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatenig ischemia. J.Vasc. Surg. 2019, 69, 26S–36S. [Google Scholar] [CrossRef] [PubMed]
- Zenunaj, G.; Acciarri, P.; Baldazzi, G.; Cosacco, A.M.; Gasbarro, V.; Traina, L. Endovascular revascularization versus open surgery with prosthetic bypass to femoro-popliteal lesions in patients with peripheral arterial disease. J. Clin. Med. 2023, 12, 5978. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Apelqvist, J.; Boyko, E.J.; Fitridge, R.; Hong, J.P.; Katsanos, K.; Mills, J.L.; Nikol, S.; Reekers, J.; Venermo, M.; et al. Effectiveness of revascularisation of the ulcerated foot in patients with diabetes and peripheral artery disease: A systematic review. Diabetes Metab. Res. Rev. 2020, 36, e3279. [Google Scholar] [CrossRef]
- Paraskevas, K.I.; Baker, D.M.; Pompella, A.; Mikhailidis, D.P. Does diabetes mellitus play a role in restenosis and patency rates following lower extremity peripheral arterial revascularisation? A critical overview. Ann. Vasc. Surg. 2008, 22, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Wallaert, J.B.; Nolan, B.W.; Adams, J.; Stanley, A.C.; Eldrup-Jorgensen, J.; Cronenwett, J.L.; Goodney, P.P. The impact of diabetes on postoperative outcomes following lower-extremity bypass surgery. J. Vasc. Surg. 2012, 56, 1317–1323. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Fontaine | Rutherford | |||
|---|---|---|---|---|
| stage | symptoms | grade | category | symptoms |
| I | asymptomatic | 0 | 0 | asymptomatic |
| II a | walking distance > 200 m | I | 1 | marginal |
| II b | walking distance < 200 m | I | 2 | significant |
| I | 3 | serious claudication | ||
| III | ischemic rest pain | II | 4 | ischemic rest pain |
| IV | tissue loss | III III | 5 6 | small area necrosis extensive necrosis |
| PAD without Neuropathy | PAD with Neuropathy (Mostly DFS) | |
|---|---|---|
| wound pain | high | low |
| CLTI-related pain level | high | low |
| loss of protective sensation (LOPS) | rare (alcohol abuse) | standard |
| activity level | reduced (pain) | inadequately high |
| motor neuropathy | none | frequent |
| ischemic neuropathy | rarely | none |
| autosympathectomy | no | frequent |
| clinical sing of overload | pain | foot ulcer |
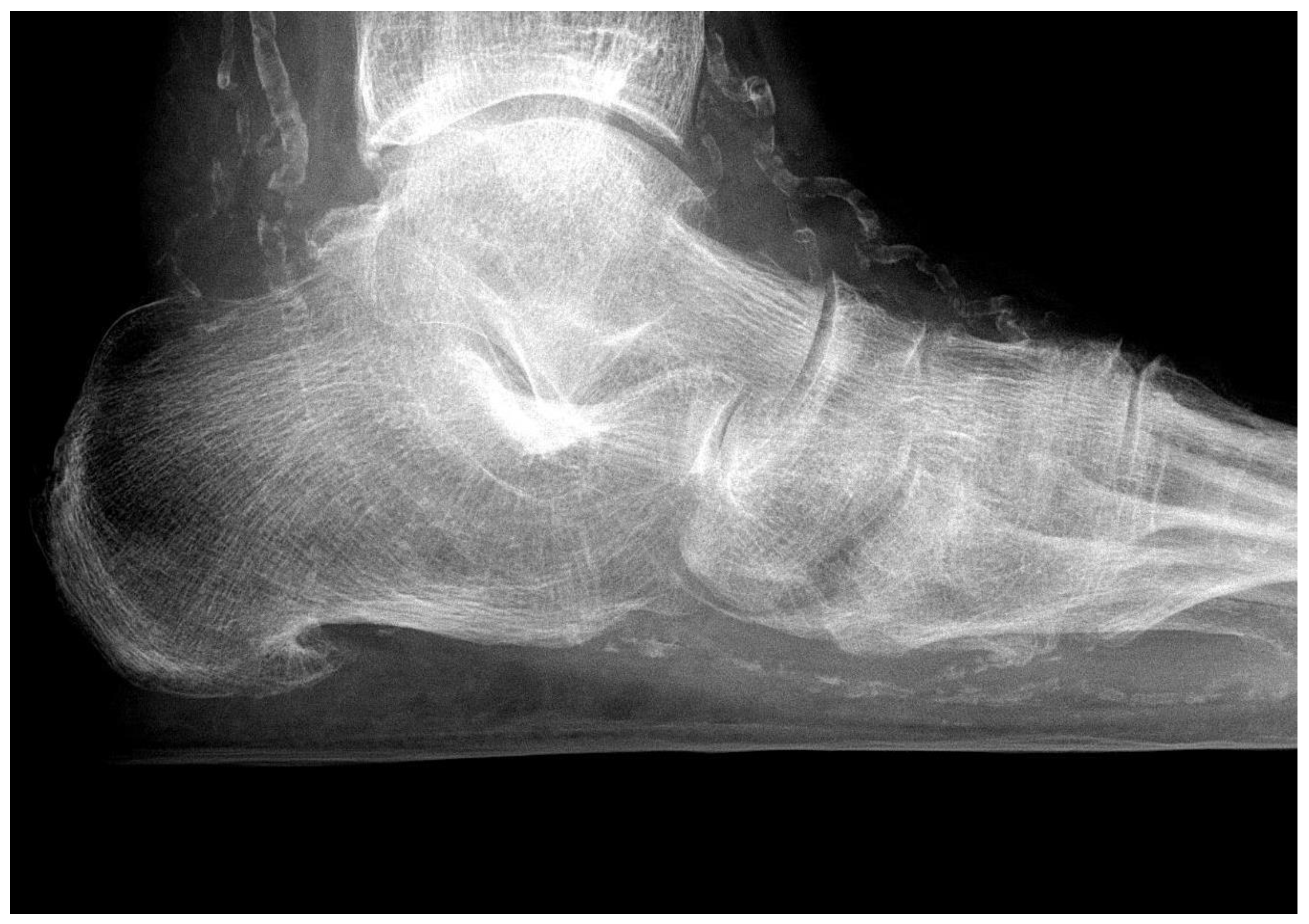
| skeletal changes | rare | frequent (Charcot foot) |
| main cause of foot lesions | CLTI | neuropathy pressure overload foot/toe deformities |
| neuropsychiatric problems | dementia (age-dependent) alcohol abuse (frequently) | depression, neglect, loss of body perception (asomatognosia) |
| Immunodeficiency | rare | frequent |
| PAD without Neuropathy | PAD with Neuropathy (Mostly DFS) | |
|---|---|---|
| soft tissue edema | rare (heart failure) | common |
| toenails | - | frequently mycotic |
| skin of the foot | atrophic, thin, cold, paling when elevated | dry, warm, rosy, filling of veins even when elevated |
| skin of the foot sole | atrophy without hyperkeratosis | hyperkeratosis, calluses, fissures, pressure ulcers |
| pedal muscles | - | commonly atrophic |
| plantar fat pad | - | atrophic |
| foot position | normal | ball foot, pointed foot (shortening of calf muscles) |
| toes | no hair, livid acral lesions | claws/hammer toes, corns |
| localization of foot lesions | indicates areas without sufficient residual blood flow | reveals pathobiomechanics |
| neurological deficits | rare (ischemic neuropathy) | common (pain, temperature, vibration, painful painless foot etc.) |
| infrared thermography | low skin temperature | high skin temperature may favor overestimation of arterial perfusion |
| PAD without Neuropathy | PAD with Neuropathy (Mostly DFS) | |
|---|---|---|
| affected vessels | macroangiopathy | microangiopathy, macroangiopathy |
| microagiopathy-related impaired oxygen diffusion | no | common |
| chronic capillary ischemia | no | common |
| media sclerosis | no | yes |
| distribution of PAD | Iliaco-femoral | infrapopliteal or pedal |
| multilevel disease | common | common |
| popliteal pulse | frequently lost | often palpable |
| pain | strong | weak or missing |
| ankle–brachial index (ABI) | useful | useless (falsely high) |
| toe–brachial index (TBI) | unnecessary | useful |
| staging according to Fontaine or Rutherford | useful | questionable |
| classification (e.g., SINBAD) | useless | useful |
| WIfI classification | useful | useful |
| PAD without Neuropathy | PAD with Neuropathy (Mostly DFS) | |
|---|---|---|
| treatment concept | vascular | multidisciplinary |
| timely treatment of CLTI | common | usually too late |
| supervised walking exercise training (SET) | IC: useful CLTI: dangerous | dangerous |
| revascularization solves the problem | mostly | rarely alone |
| offloading performed by the patient | mostly (pain) | rarely (neuropathy) |
| recurrence rate of ulcers/necroses | low | high |
| ultrasound bypass control | yes | yes |
| ultrasound control of endovascular reconstructions | no | regularly |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rümenapf, G.; Abilmona, N.; Morbach, S.; Sigl, M. Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review. J. Clin. Med. 2024, 13, 2141. https://doi.org/10.3390/jcm13072141
Rümenapf G, Abilmona N, Morbach S, Sigl M. Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review. Journal of Clinical Medicine. 2024; 13(7):2141. https://doi.org/10.3390/jcm13072141
Chicago/Turabian StyleRümenapf, Gerhard, Nour Abilmona, Stephan Morbach, and Martin Sigl. 2024. "Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review" Journal of Clinical Medicine 13, no. 7: 2141. https://doi.org/10.3390/jcm13072141
APA StyleRümenapf, G., Abilmona, N., Morbach, S., & Sigl, M. (2024). Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review. Journal of Clinical Medicine, 13(7), 2141. https://doi.org/10.3390/jcm13072141