


Associations between Sleep Disturbances, Personality Traits and Self-Regulation in a Sample of Healthy Adults

 , ,
, ,  , , and
, , and 
Abstract
1. Introduction
1.1. Insomnia and Personality Traits
1.2. The Present Study
2. Method
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Sociodemographic Information
2.3.2. Sleep Quality
2.3.3. Self-Regulation
2.3.4. Personality Profiles
2.3.5. Data Analysis
3. Results
3.1. General Sociodemographic Information
3.2. Frequencies of Good and Poor Sleepers, Based on the Cut-Off Values of the Pittsburgh Sleep Quality Index (PSQI)
3.3. Correlations between Sleep, Self-Regulation and Personality Traits
3.4. Predicting Sleep Disturbances
3.5. Categories of Self-Regulation on Sleep Disturbances and Personality Traits
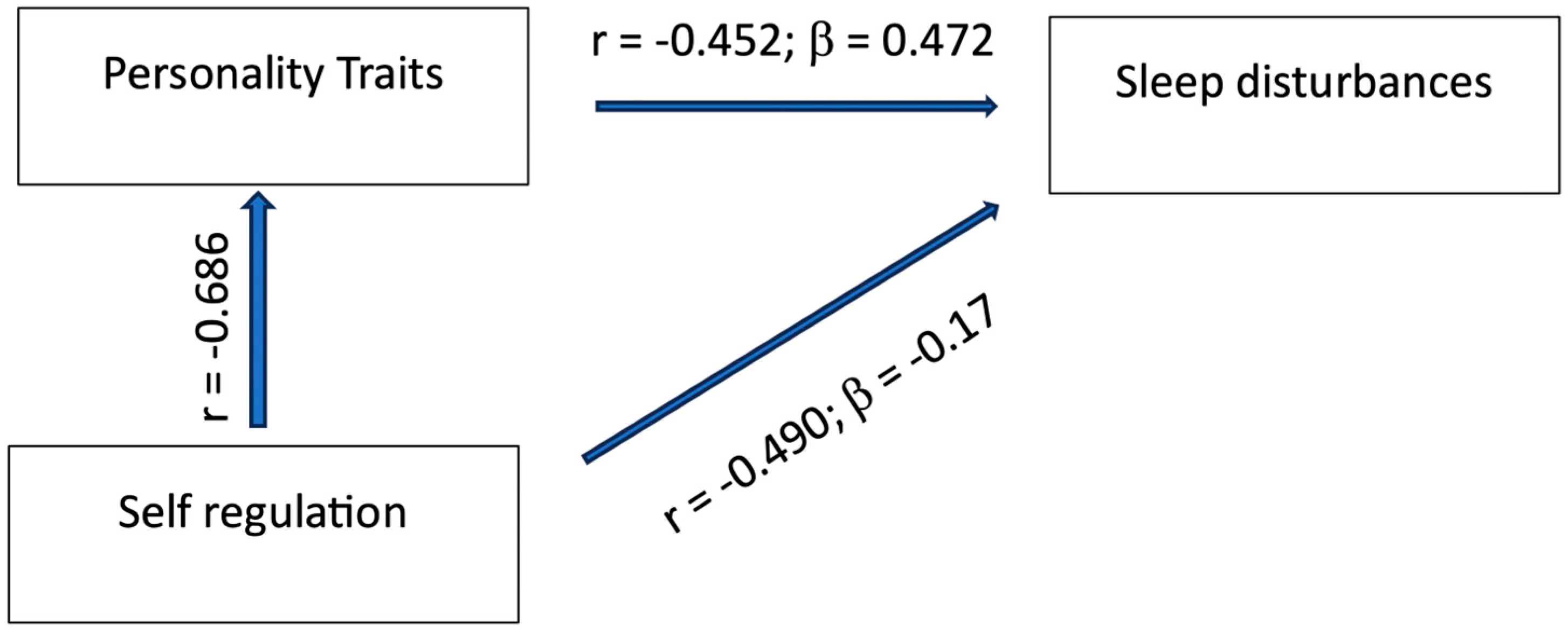
3.6. Direct and Indirect Effects of Self-Regulation on Sleep Disturbances
4. Discussion
4.1. State Self-Regulation and Sleep
4.2. Personality Traits and Sleep
4.3. State–Trait Dimensions, and Direct and Indirect Effects on Sleep
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Cao, D.; Huang, Y.; Chen, Z.; Wang, R.; Dong, Q.; Wei, Q.; Liu, L. Sleep duration and health outcomes: An umbrella review. Sleep Breath 2022, 26, 1479–1501. [Google Scholar] [CrossRef] [PubMed]
- Acheson, A.; Richards, J.B.; de Wit, H. Effects of sleep deprivation on impulsive behaviors in men and women. Physiol. Behav. 2007, 91, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Lowe, C.J.; Safati, A.; Hall, P.A. The neurocognitive consequences of sleep restriction: A meta-analytic review. Neurosci. Biobehav. Rev. 2017, 80, 586–604. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, R.C.; Barnes, J.C.; Hay, C. Sleep deprivation, low self-control, and delinquency: A test of the strength model of self-control. J. Youth Adolesc. 2015, 44, 465–477. [Google Scholar] [CrossRef]
- Baiden, P.; Tadeo, S.K.; Tonui, B.C.; Seastrunk, J.D.; Boateng, G.O. Association between insufficient sleep and suicidal ideation among adolescents. Psychiatry Res. 2020, 287, 112579. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Dvorsky, M.R.; Holdaway, A.S.; Luebbe, A.M. Sleep problems and suicidal behaviors in college students. J. Psychiatr. Res. 2018, 99, 122–128. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Lee, H.C.; Chen, P.Y.; Lai, Y.F.; Tu, Y.K. Associations between sleep duration and suicidality in adolescents: A systematic review and dose-response meta-analysis. Sleep Med. Rev. 2018, 42, 119–126. [Google Scholar] [CrossRef]
- Dong, M.; Lu, L.; Sha, S.; Zhang, L.; Zhang, Q.; Ungvari, G.S.; Balbuena, L.; Xiang, Y.T. Sleep Disturbances and the Risk of Incident Suicidality: A Systematic Review and Meta-Analysis of Cohort Studies. Psychosom. Med. 2021, 83, 739–745. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Babiss, L.A.; Malaspina, D.; Turner, J.B.; Zammit, G.K.; Posner, K. Earlier parental set bedtimes as a protective factor against depression and suicidal ideation. Sleep 2010, 33, 97–106. [Google Scholar] [CrossRef]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. In StatPearls; StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kang, G.E.; Patriquin, M.A.; Nguyen, H.; Oh, H.; Rufino, K.A.; Storch, E.A.; Schanzer, B.; Mathew, S.J.; Salas, R.; Najafi, B. Objective measurement of sleep, heart rate, heart rate variability, and physical activity in suicidality: A systematic review. J. Affect. Disord. 2020, 273, 318–327. [Google Scholar] [CrossRef]
- Liu, J.W.; Tu, Y.K.; Lai, Y.F.; Lee, H.C.; Tsai, P.S.; Chen, T.J.; Huang, H.C.; Chen, Y.T.; Chiu, H.Y. Associations between sleep disturbances and suicidal ideation, plans, and attempts in adolescents: A systematic review and meta-analysis. Sleep 2019, 42, zsz054. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Innamorati, M.; Forte, A.; Longo, L.; Mazzetta, C.; Erbuto, D.; Ricci, F.; Palermo, M.; Stefani, H.; Seretti, M.E.; et al. Insomnia as a predictor of high-lethality suicide attempts. Int. J. Clin. Pract. 2013, 67, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Allan, S.; Beattie, L.; Bohan, J.; MacMahon, K.; Rasmussen, S. Sleep problem, suicide and self-harm in university students: A systematic review. Sleep Med. Rev. 2019, 44, 58–69. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, S.; Xu, H. Systematic review and meta-analysis of the relationship between sleep disorders and suicidal behaviour in patients with depression. BMC Psychiatry 2019, 19, 303. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.M.; Brower, K.J.; Zucker, R.A. Sleep problems, suicidal ideation, and self-harm behaviors in adolescence. J. Psychiatr. Res. 2011, 45, 505–511. [Google Scholar] [CrossRef]
- Rusnac, N.; Spitzenstetter, F.; Tassi, P. Chronic sleep loss and risk-taking behavior: Does the origin of sleep loss matter? Behav. Sleep Med. 2018, 17, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Short, M.A.; Weber, N. Sleep duration and risk-taking in adolescents: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 41, 185–196. [Google Scholar] [CrossRef]
- Telzer, E.H.; Fuligni, A.J.; Lieberman, M.D.; Galvan, A. The effects of poor quality sleep on brain function and risk taking in adolescence. NeuroImage 2013, 71, 275–283. [Google Scholar] [CrossRef]
- Baglioni, C.; Spiegelhalder, K.; Lombardo, C.; Riemann, D. Sleep and emotions: A focus on insomnia. Sleep Med. Rev. 2010, 14, 227–238. [Google Scholar] [CrossRef]
- Asarnow, L.D.; McGlinchey, E.; Harvey, A.G. The effects of bedtime and sleep duration on academic and emotional outcomes in a nationally representative sample of adolescents. J. Adolesc. Health 2014, 54, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Bouwmans, M.E.J.; Bos, E.H.; Hoenders, H.J.R.; Oldehinkel, A.J.; de Jonge, P. Sleep quality predicts positive and negative affect but not vice versa. An electronic diary study in depressed and healthy individuals. J. Affect. Disord. 2017, 207, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Brand, S.; Kirov, R.; Kalak, N.; Gerber, M.; Puhse, U.; Lemola, S.; Correll, C.U.; Cortese, S.; Meyer, T.; Holsboer-Trachsler, E. Perfectionism related to self-reported insomnia severity, but not when controlled for stress and emotion regulation. Neuropsychiatr. Dis. Treat. 2015, 11, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.; McNeill, K.; Ireland, J.L.; Qurashi, I. Facial emotion recognition and sleep in mentally disordered patients: A natural experiment in a high security hospital. Psychiatry Res. 2015, 230, 725–727. [Google Scholar] [CrossRef] [PubMed]
- de Almondes, K.M.; Júnior, F.W.N.H.; Alves, N.T. Sleep deprivation and implications for recognition and perception of facial emotions. Sleep Biol. Rhythm. 2016, 14, 13–22. [Google Scholar] [CrossRef]
- Goldstein, A.N.; Walker, M.P. The role of sleep in emotional brain function. Annu. Rev. Clin. Psychol. 2014, 10, 679–708. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.; Kahn-Greene, E.T.; Lipizzi, E.L.; Newman, R.A.; Kamimori, G.H.; Balkin, T.J. Sleep deprivation reduces perceived emotional intelligence and constructive thinking skills. Sleep Med. 2008, 9, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Kyle, S.D.; Beattie, L.; Spiegelhalder, K.; Rogers, Z.; Espie, C.A. Altered emotion perception in insomnia disorder. Sleep 2014, 37, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Maccari, L.; Martella, D.; Marotta, A.; Sebastiani, M.; Banaj, N.; Fuentes, L.J.; Casagrande, M. Effects of sleep loss on emotion recognition: A dissociation between face and word stimuli. Exp. Brain Res. 2014, 232, 3147–3157. [Google Scholar] [CrossRef]
- Palmer, C.A.; Alfano, C.A. Sleep and emotion regulation: An organizing, integrative review. Sleep Med. Rev. 2017, 31, 6–16. [Google Scholar] [CrossRef]
- Shimizu, M.; Gillis, B.T.; Buckhalt, J.A.; El-Sheikh, M. Linear and Nonlinear Associations between Sleep and Adjustment in Adolescence. Behav. Sleep Med. 2020, 18, 690–704. [Google Scholar] [CrossRef] [PubMed]
- Talbot, L.S.; McGlinchey, E.L.; Kaplan, K.A.; Dahl, R.E.; Harvey, A.G. Sleep deprivation in adolescents and adults: Changes in affect. Emotion 2010, 10, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Tempesta, D.; Socci, V.; De Gennaro, L.; Ferrara, M. Sleep and emotional processing. Sleep Med. Rev. 2018, 40, 183–195. [Google Scholar] [CrossRef] [PubMed]
- van der Helm, E.; Gujar, N.; Walker, M.P. Sleep deprivation impairs the accurate recognition of human emotions. Sleep 2010, 33, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, M.; Cluydts, R. The emotional brain and sleep: An intimate relationship. Sleep Med. Rev. 2010, 14, 219–226. [Google Scholar] [CrossRef]
- Yoo, S.S.; Gujar, N.; Hu, P.; Jolesz, F.A.; Walker, M.P. The human emotional brain without sleep—A prefrontal amygdala disconnect. Curr. Biol. 2007, 17, R877–R878. [Google Scholar] [CrossRef] [PubMed]
- Gardani, M.; Bradford, D.R.R.; Russell, K.; Allan, S.; Beattie, L.; Ellis, J.G.; Akram, U. A systematic review and meta-analysis of poor sleep, insomnia symptoms and stress in undergraduate students. Sleep Med. Rev. 2022, 61, 101565. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Mendoza, J.; Li, Y.; Vgontzas, A.N.; Fang, J.; Gaines, J.; Calhoun, S.L.; Liao, D.; Bixler, E.O. Insomnia is Associated with Cortical Hyperarousal as Early as Adolescence. Sleep 2016, 39, 1029–1036. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Vela-Bueno, A.; Vgontzas, A.N.; Ramos-Platon, M.J.; Olavarrieta-Bernardino, S.; Bixler, E.O.; De la Cruz-Troca, J.J. Cognitive-emotional hyperarousal as a premorbid characteristic of individuals vulnerable to insomnia. Psychosom. Med. 2010, 72, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef]
- Harvey, A.G. Pre-sleep cognitive activity: A comparison of sleep-onset insomniacs and good sleepers. Br. J. Clin. Psychol. 2000, 39 Pt 3, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G. A transdiagnostic approach to treating sleep disturbance in psychiatric disorders. Cogn. Behav. Ther. 2009, 38 (Suppl. 1), 35–42. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G.; Tang, N.K.; Browning, L. Cognitive approaches to insomnia. Clin. Psychol. Rev. 2005, 25, 593–611. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Drake, C.L.; Harvey, A.G.; Krystal, A.D.; Manber, R.; Riemann, D.; Spiegelhalder, K. Insomnia disorder. Nat. Rev. Dis. Primers 2015, 1, 15026. [Google Scholar] [CrossRef] [PubMed]
- Norell-Clarke, A.; Jansson-Frojmark, M.; Tillfors, M.; Harvey, A.G.; Linton, S.J. Cognitive processes and their association with persistence and remission of insomnia: Findings from a longitudinal study in the general population. Behav. Res. Ther. 2014, 54, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Mendoza, J.; Baker, J.H.; Vgontzas, A.N.; Gaines, J.; Liao, D.; Bixler, E.O. Insomnia symptoms with objective short sleep duration are associated with systemic inflammation in adolescents. Brain Behav. Immun. 2017, 61, 110–116. [Google Scholar] [CrossRef]
- Zhao, L.; Wang, E.; Zhang, X.; Karama, S.; Khundrakpam, B.; Zhang, H.; Guan, M.; Wang, M.; Cheng, J.; Shi, D.; et al. Cortical Structural Connectivity Alterations in Primary Insomnia: Insights from MRI-Based Morphometric Correlation Analysis. Biomed. Res. Int. 2015, 2015, 817595. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.P.; Harvey, A.G. Obligate symbiosis: Sleep and affect. Sleep Med. Rev. 2010, 14, 215–217. [Google Scholar] [CrossRef]
- Prather, A.A. Sleep and Affect: Introduction to the Special Issue. Affect. Sci. 2022, 3, 291–294. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Frojmark, M.; Palagini, L.; Rucker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 43, 96–105. [Google Scholar] [CrossRef]
- Hertenstein, E.; Benz, F.; Schneider, C.L.; Baglioni, C. Insomnia—A risk factor for mental disorders. J. Sleep Res. 2023, 32, e13930. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Hertenstein, E.; Riemann, D.; Nissen, C. Sleep, insomnia and mental health. J. Sleep Res. 2022, 31, e13628. [Google Scholar] [CrossRef]
- Boland, E.M.; Goldschmied, J.R.; Gehrman, P.R. Does insomnia treatment prevent depression? Sleep 2023, 46, zsad104. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, M.; Wang, Y.L. Emotion, emotion regulation and sleep: An intimate relationship. AIMS Neurosci. 2018, 5, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Bahmani, D.; Esmaeili, L.; Mokhtari, F.; Sadeghi, L.; Afsharzadeh, M.; Shaygannejad, V.; Mirmosayyeb, O.; Goldstein-Piekarski, A.N.; Gross, J.J. Effects of Acceptance and Commitment Therapy (ACT) and Mindfulness-Based Stress Reduction (MBSR) on Symptoms and Emotional Competencies in Individuals with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 2022, 104029. [Google Scholar] [CrossRef]
- Hertenstein, E.; Trinca, E.; Wunderlin, M.; Schneider, C.L.; Züst, M.A.; Fehér, K.D.; Su, T.; Straten, A.V.; Berger, T.; Baglioni, C.; et al. Cognitive behavioral therapy for insomnia in patients with mental disorders and comorbid insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 62, 101597. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Bahmani, D.; Motl, R.W.; Sadeghi Bahmani, L.; Mirmosayyeb, O.; Shaygannejad, V.; Mokhtari, F.; Gross, J.J. Emotional competencies in multiple sclerosis. Mult. Scler. Relat. Disord. 2023, 78, 104896. [Google Scholar] [CrossRef]
- Sadeghi Bahmani, D.; Razazian, N.; Farnia, V.; Alikhani, M.; Tatari, F.; Brand, S. Compared to an active control condition, in persons with multiple sclerosis two different types of exercise training improved sleep and depression, but not fatigue, paresthesia, and intolerance of uncertainty. Mult. Scler. Relat. Disord. 2019, 36, 101356. [Google Scholar] [CrossRef]
- Sellbom, M.; Carragher, N.; Sunderland, M.; Calear, A.L.; Batterham, P.J. The role of maladaptive personality domains across multiple levels of the HiTOP structure. Personal. Ment. Health 2020, 14, 30–50. [Google Scholar] [CrossRef]
- Johann, A.F.; Feige, B.; Hertenstein, E.; Nissen, C.; Benz, F.; Steinmetz, L.; Baglioni, C.; Riemann, D.; Spiegelhalder, K.; Akram, U. The Effects of Cognitive Behavioral Therapy for Insomnia on Multidimensional Perfectionism. Behav. Ther. 2023, 54, 386–399. [Google Scholar] [CrossRef]
- Ellis, J.G.; Perlis, M.L.; Espie, C.A.; Grandner, M.A.; Bastien, C.H.; Barclay, N.L.; Altena, E.; Gardani, M. The natural history of insomnia: Predisposing, precipitating, coping, and perpetuating factors over the early developmental course of insomnia. Sleep 2021, 44, zsab095. [Google Scholar] [CrossRef]
- Larsgård, B.; Saksvik-Lehouillier, I. The predictive power of personality traits on insomnia symptoms: A longitudinal study of shift workers. Personal. Individ. Differ. 2017, 115, 35–42. [Google Scholar] [CrossRef]
- Akram, U.; Ellis, J.G.; Barclay, N.L. Anxiety Mediates the Relationship between Perfectionism and Insomnia Symptoms: A Longitudinal Study. PLoS ONE 2015, 10, e0138865. [Google Scholar] [CrossRef] [PubMed]
- Jansson-Fröjmark, M.; Linton, S.J. Is perfectionism related to pre-existing and future insomnia? A prospective study. Br. J. Clin. Psychol. 2007, 46, 119–124. [Google Scholar] [CrossRef]
- van de Laar, M.; Verbeek, I.; Pevernagie, D.; Aldenkamp, A.; Overeem, S. The role of personality traits in insomnia. Sleep Med. Rev. 2010, 14, 61–68. [Google Scholar] [CrossRef]
- Akram, U.; Stevenson, J.C.; Gardani, M.; Allen, S.; Johann, A.F. Personality and insomnia: A systematic review and narrative synthesis. J. Sleep Res. 2023, 32, e14031. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Chehri, A.; Nourozi, M.; Eskandari, S.; Khazaie, H.; Hemati, N.; Jalali, A. Validation of the Persian version of the Pittsburgh Sleep Quality Index in elderly population. Sleep Sci. 2020, 13, 119–124. [Google Scholar] [CrossRef]
- Farrahi, J.; Nakhaee, N.; Sheibani, V.; Garrusi, B.; Amirkafi, A. Psychometric properties of the Persian version of the Pittsburgh Sleep Quality Index addendum for PTSD (PSQI-A). Sleep Breath 2009, 13, 259–262. [Google Scholar] [CrossRef]
- Farrahi Moghaddam, J.; Nakhaee, N.; Sheibani, V.; Garrusi, B.; Amirkafi, A. Reliability and validity of the Persian version of the Pittsburgh Sleep Quality Index (PSQI-P). Sleep Breath 2012, 16, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Nazifi, M.; Mokarami, H.; Akbaritabar, A.; Kalte, O.; Rahi, A. Psychometric Properties of the Persian Translation of Pittsburgh Sleep Quality Index. Health Scope 2014, 3, e15547. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Zakiei, A.; Khazaie, H.; Alimoradi, M.; Kadivarian, A.; Rajabi-Gilan, N.; Komasi, S. A Causal Model for the Control of Risk Factors for Cardiovascular Diseases Using a new Temperamental Personality Theory in the General Population of Western Iran: The Mediating Role of Self-Regulation. J. Pract. Cardiovasc. Sci. 2021, 7, 190–197. [Google Scholar] [CrossRef]
- Carey, K.B.; Neal, D.J.; Collins, S.E. A psychometric analysis of the self-regulation questionnaire. Addict. Behav. 2004, 29, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Lara, D.R.; Bisol, L.W.; Brunstein, M.G.; Reppold, C.T.; de Carvalho, H.W.; Ottoni, G.L. The Affective and Emotional Composite Temperament (AFECT) model and scale: A system-based integrative approach. J. Affect. Disord. 2012, 140, 14–37. [Google Scholar] [CrossRef]
- Hair Jr, J.F.; Black, C.W.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Andover, UK, 2019. [Google Scholar]
- Rudolf, M.; Müller, J. Multivariate Analyses; Hogrefe: Goettingen, Germay, 2004. [Google Scholar]
- Brosius, F. SPSS. In Umfassendes Handbuch zu Statistik und Datenanalyse—Comprehensive Textbook for Statistics and Data Analysis; mitp Verlags GmBH & Co.: Frechen, Germany, 2018. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Prerna Tigga, N.; Garg, S. Prediction of Global Psychological Stress and Coping Induced by the COVID-19 Outbreak: A Machine Learning Study. Alpha Psychiatry 2022, 23, 193–202. [Google Scholar] [CrossRef]
- Benz, F.; Meneo, D.; Baglioni, C.; Hertenstein, E. Insomnia symptoms as risk factor for somatic disorders: An umbrella review of systematic reviews and meta-analyses. J. Sleep Res. 2023, 32, e13984. [Google Scholar] [CrossRef] [PubMed]
- Quach, J.L.; Nguyen, C.D.; Williams, K.E.; Sciberras, E. Bidirectional Associations Between Child Sleep Problems and Internalizing and Externalizing Difficulties From Preschool to Early Adolescence. JAMA Pediatr. 2018, 172, e174363. [Google Scholar] [CrossRef]
- Quach, J.; Hiscock, H.; Canterford, L.; Wake, M. Outcomes of child sleep problems over the school-transition period: Australian population longitudinal study. Pediatrics 2009, 123, 1287–1292. [Google Scholar] [CrossRef]
- Miller, K.E.; Gehrman, P.R. REM Sleep: What Is It Good for? Curr. Biol. 2019, 29, R806–R807. [Google Scholar] [CrossRef]
- Morse, A.M.; Kothare, S.V. Sleep disorders and concussion. Handb. Clin. Neurol. 2018, 158, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, M.C.; Baylan, S.; Gardani, M. Prevalence of insomnia and insomnia symptoms following mild-traumatic brain injury: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 61, 101563. [Google Scholar] [CrossRef] [PubMed]
- Primavera, D.; Aviles Gonzalez, C.I.; Romano, F.; Kalcev, G.; Pinna, S.; Minerba, L.; Scano, A.; Orrù, G.; Cossu, G. Does the Response to a Stressful Condition in Older Adults with Life Rhythm Dysregulations Provide Evidence of the Existence of the “Dysregulation of Mood, Energy, and Social Rhythms Syndrome”? Healthcare 2023, 12, 87. [Google Scholar] [CrossRef] [PubMed]
- Zakiei, A.; Khazaie, H.; Rostampour, M.; Lemola, S.; Esmaeili, M.; Dürsteler, K.; Brühl, A.B.; Sadeghi-Bahmani, D.; Brand, S. Acceptance and Commitment Therapy (ACT) Improves Sleep Quality, Experiential Avoidance, and Emotion Regulation in Individuals with Insomnia-Results from a Randomized Interventional Study. Life 2021, 11, 133. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | N (%) | Statistics | |
|---|---|---|---|
| Sex | Male | 180 (21.3) | X2 = 279.191, p < 0.001 |
| Female | 666 (78.7) | ||
| Education | Under diploma | 157 (18.6) | X2 = 37.697; p < 0.001 |
| Diploma | 246 (29.1) | ||
| Bachelor | 264 (31.2) | ||
| Master and higher | 179 (21.2) | ||
| Marital status | Single | 206 (24.3) | X2 = 598.730; p < 0.001 |
| Married | 603 (71.3) | ||
| Other | 37 (4.4) | ||
| Occupation | Unemployment | 432 (51.1) | X2 = 196.390; p < 0.001 |
| Student | 103 (12.2) | ||
| Employment | 311 (36.8) | ||
| Age (Years) | 18–25 | 102 (12.1) | X2 = 505.404, p < 0.001 |
| 25–35 | 444 (52.5) | ||
| 35–50 | 279 (33) | ||
| 50–65 | 21 (2.5) | ||
| PSQI Total Score | Self-Regulation | Internalization | Externalization | Stability | Instability | Total Personality Score | |
|---|---|---|---|---|---|---|---|
| PSQI total score | - | −0.49 *** | 0.406 *** | 0.401 *** | −0.219 *** | 0.240 *** | 0.452 *** |
| Self-regulation | - | - | −0.517 *** | −0.565 *** | 0.516 *** | −0.346 *** | −0.686 *** |
| Internalization | - | - | 0.566 *** | −0.206 *** | 0.520 *** | 0.845 *** | |
| Externalization | - | - | - | - | −0.287 *** | 0.275 *** | 0.752 *** |
| Stability | - | - | - | - | - | −0.025 | −0.500 *** |
| Instability | - | - | - | - | - | - | 0.678 *** |
| Personality total score | - | ||||||
| M | 5.63 | 117.08 | 8.01 | 6.44 | 10.04 | 7.08 | 29.46 |
| SD | 3.66 | 16.17 | 3.01 | 2.45 | 2.32 | 2.73 | 7.42 |
| Variables | Coefficients | Standard Error | β | t | p | R | R2 | Durbin–Watson | VIF |
|---|---|---|---|---|---|---|---|---|---|
| Intercept | 2.64 | 1.83 | 1.47 | 0.148 | 0.481 | 0.232 | 2.009 | ||
| Self-regulation | −0.039 | 0.010 | −0.171 | −3.89 | <0.001 | 1.605 | |||
| Externalization | 0.265 | 0.059 | 0.178 | 4.54 | <0.001 | 1.728 | |||
| Internalization | 0.233 | 0.051 | 0.192 | 4.53 | <0.001 | 1.609 | |||
| Excluded variables: Stability; instability; personality total score: p < 0.35 | |||||||||
| Variables | Very Low | Low | Medium | High | Very High | F | p | ηp2 |
|---|---|---|---|---|---|---|---|---|
| n = 169 | n = 179 | n = 164 | n = 156 | n = 178 | ||||
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | ||||
| PSQI total | 7.97 (4.25) | 5.95 (3.25) | 5.56 (3.25) | 4.81 (3.21) | 3.83 (2.82) | 35.13 | <0.001 | 0.144 |
| Externalization | 8.63 (2.51) | 6.95 (2.16) | 6.28 (1.82) | 5.65 (1.88) | 4.70 (1.88) | 86.38 | <0.001 | 0.292 |
| Internalization | 10.50 (2.79) | 8.54 (2.39) | 7.91 (2.66) | 6.88 (2.57) | 6.16 (2.69) | 68.68 | <0.001 | 0.247 |
| Stability | 8.32 (2.24) | 9.54 (1.87) | 10.11 (1.99) | 10.64 (2.13) | 11.59 (2.01) | 60.24 | <0.001 | 0.224 |
| Instability | 8.61 (2.92) | 7.27 (2.42) | 7.27 (2.61) | 6.23 (2.24) | 6.01 (2.60) | 26.84 | <0.001 | 0.114 |
| Personality total score | 37.40 (6.35) | 31.23 (4.68) | 29.35 (5.60) | 26.12 (5.59) | 23.29 (5.92) | 153.23 | <0.001 | 0.423 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakiei, A.; Sadeghi-Bahmani, D.; Khazaie, H.; Lorestani, Z.; Sadeghi, M.; Korani, D.; Sahraei, Z.; Komasi, S.; Stanga, Z.; Brühl, A.B.; et al. Associations between Sleep Disturbances, Personality Traits and Self-Regulation in a Sample of Healthy Adults. J. Clin. Med. 2024, 13, 2143. https://doi.org/10.3390/jcm13072143
Zakiei A, Sadeghi-Bahmani D, Khazaie H, Lorestani Z, Sadeghi M, Korani D, Sahraei Z, Komasi S, Stanga Z, Brühl AB, et al. Associations between Sleep Disturbances, Personality Traits and Self-Regulation in a Sample of Healthy Adults. Journal of Clinical Medicine. 2024; 13(7):2143. https://doi.org/10.3390/jcm13072143
Chicago/Turabian StyleZakiei, Ali, Dena Sadeghi-Bahmani, Habibolah Khazaie, Zeinab Lorestani, Mohammad Sadeghi, Dariuosh Korani, Zeinab Sahraei, Saeid Komasi, Zeno Stanga, Annette B. Brühl, and et al. 2024. "Associations between Sleep Disturbances, Personality Traits and Self-Regulation in a Sample of Healthy Adults" Journal of Clinical Medicine 13, no. 7: 2143. https://doi.org/10.3390/jcm13072143
APA StyleZakiei, A., Sadeghi-Bahmani, D., Khazaie, H., Lorestani, Z., Sadeghi, M., Korani, D., Sahraei, Z., Komasi, S., Stanga, Z., Brühl, A. B., & Brand, S. (2024). Associations between Sleep Disturbances, Personality Traits and Self-Regulation in a Sample of Healthy Adults. Journal of Clinical Medicine, 13(7), 2143. https://doi.org/10.3390/jcm13072143