
Review of Temperature Management in Traumatic Brain Injuries

Abstract
1. Introduction
2. Materials and Methods
3. Historical Background
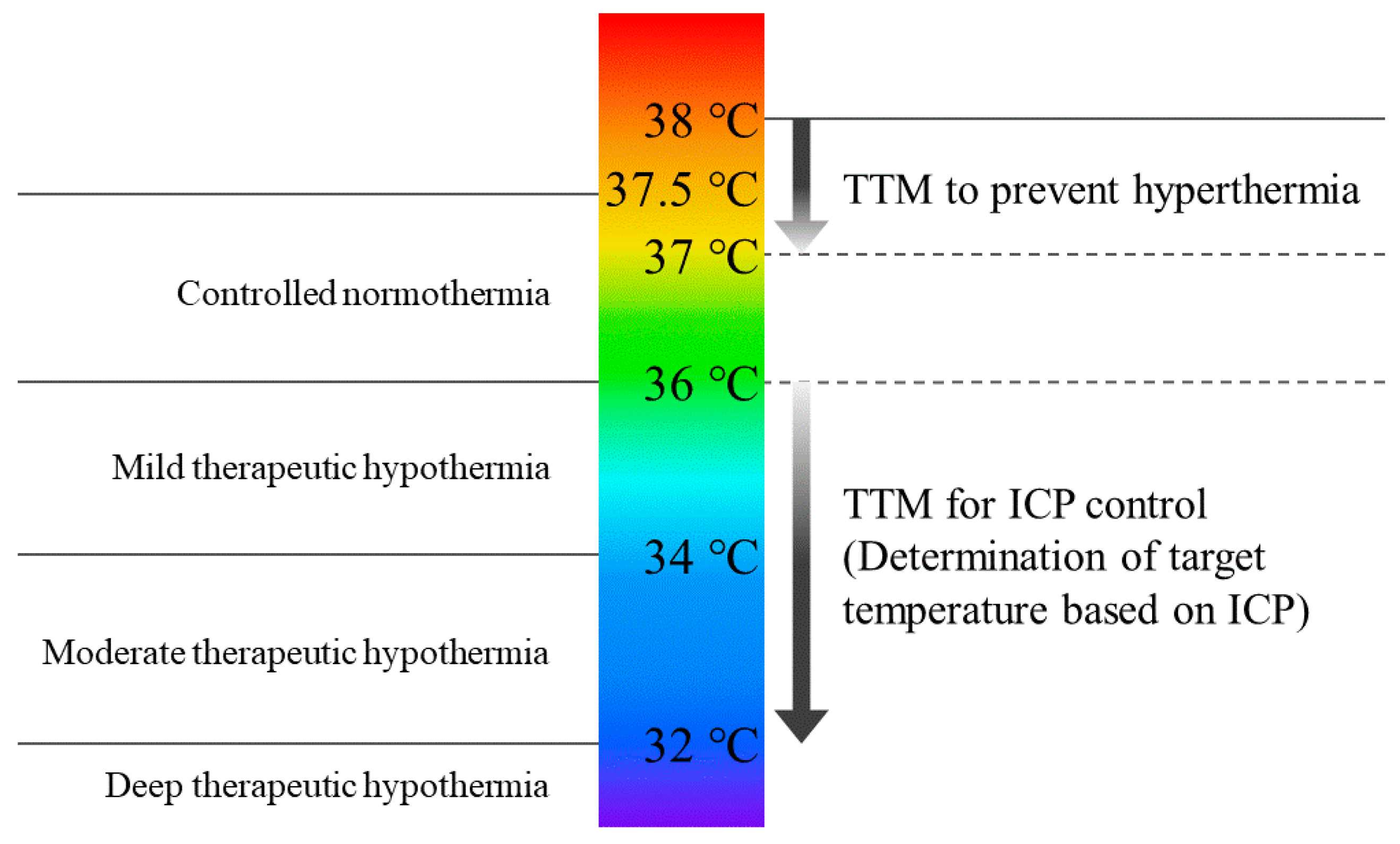
4. Terminology of Body Temperature Management
5. TTM for ICP Control
6. TTM to Prevent Hyperthermia
7. Prevention of Shivering during TTM
8. Limitations
9. Conclusions
10. Future Directions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shiozaki, T.; Hayakata, T.; Taneda, M.; Nakajima, Y. A Multicenter Prospective Randomized Controlled Trial of the Efficacy of Mild Hypothermia for Severely Head Injured Patients with Low Intracranial Pressure. J. Neurosurg. 2001, 94, 50–54. [Google Scholar] [CrossRef]
- Jiang, J.; Yu, M.; Zhu, C. Effect of Long-Term Mild Hypothermia Therapy in Patients with Severe Traumatic Brain Injury: 1-Year Follow-up Review of 87 Cases. J. Neurosurg. 2000, 93, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Marion, D.W.; Penrod, L.E.; Kelsey, S.F.; Obrist, W.D. Treatment of Traumatic Brain Injury with Moderate Hypothermia. N. Engl. J. Med. 1997, 336, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Clifton, G.L.; Allen, S.; Barrodale, P.; Plenger, P. A Phase II Study of Moderate Hypothermia in Severe Brain Injury. J. Neurotrauma 1993, 10, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Clifton, G.L.; Miller, E.R.; Sung, C.C.; Levin, H.S. Lack of Effect of Induction of Hypothermia after Acute Brain Injury. N. Engl. J. Med. 2001, 344, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, T.; Yamashita, S.; Nagao, S.; Hayashi, N.; Ohashi, Y.; Aibiki, M.; Aruga, T.; Asai, Y.; Dohi, K.; Eguchi, Y.; et al. Prolonged Mild Therapeutic Hypothermia versus Fever Control with Tight Hemodynamic Monitoring and Slow Rewarming in Patients with Severe Traumatic Brain Injury: A Randomized Controlled Trial. J. Neurotrauma 2015, 32, 3197. [Google Scholar] [CrossRef] [PubMed]
- Clifton, G.L.; Valadka, A.; Zygun, D.; Coffey, C.S. Very Early Hypothermia Induction in Patients with Severe Brain Injury (the National Acute Brain Injury Study: Hypothermia II): A Randomised Trial. Lancet Neurol. 2011, 10, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Dasic, D.; Morgan, L.; Panezai, A.; Syrmos, N.; Ligarotti, G.K.I.; Zaed, I.; Chibbaro, S.; Khan, T.; Prisco, L.; Ganau, M. A Scoping Review on the Challenges, Improvement Programs, and Relevant Output Metrics for Neurotrauma Services in Major Trauma Centers. Surg. Neurol. Int. 2022, 13, 171. [Google Scholar] [CrossRef]
- Hergenroeder, G.W.; Yokobori, S.; Choi, H.A.; Schmitt, K.; Detry, M.A.; Schmitt, L.H.; McGlothlin, A.; Puccio, A.M.; Jagid, J.; Kuroda, Y.; et al. Hypothermia for Patients Requiring Evacuation of Subdural Hematoma: A Multicenter Randomized Clinical Trial. Neurocrit. Care 2022, 36, 560–572. [Google Scholar] [CrossRef]
- Clifton, G.L.; Coffey, C.S.; Fourwinds, S.; Zygun, D.; Valadka, A.; Smith, K.R.; Frisby, M.L.; Bucholz, R.D.; Wilde, E.A.; Levin, H.S.; et al. Early Induction of Hypothermia for Evacuated Intracranial Hematomas: A Post Hoc Analysis of Two Clinical Trials. J. Neurosurg. 2012, 117, 714–720. [Google Scholar] [CrossRef]
- Chen, H.; Wu, F.; Yang, P.; Shao, J.; Chen, Q.; Zheng, R. A Meta-Analysis of the Effects of Therapeutic Hypothermia in Adult Patients with Traumatic Brain Injury. Crit. Care 2019, 23, 396. [Google Scholar] [CrossRef] [PubMed]
- Watson, H.I.; Shepherd, A.A.; Rhodes, J.K.J.; Andrews, P.J.D. Revisited: A Systematic Review of Therapeutic Hypothermia for Adult Patients Following Traumatic Brain Injury. Crit. Care Med. 2018, 46, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Crompton, E.M.; Lubomirova, I.; Cotlarciuc, I.; Han, T.S.; Sharma, S.D.; Sharma, P. Meta-Analysis of Therapeutic Hypothermia for Traumatic Brain Injury in Adult and Pediatric Patients. Crit. Care Med. 2017, 45, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, E.; Koizumi, H.; Kunitsugu, I.; Fujisawa, H.; Suzuki, M. Survey of Brain Temperature Management in Patients with Traumatic Brain Injury in the Japan Neurotrauma Data Bank. J. Neurotrauma 2014, 31, 315–320. [Google Scholar] [CrossRef] [PubMed]
- England, T.N. Mild Therapeutic Hypothermia to Improve the Neurologic Outcome after Cardiac Arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of Comatose Survivors of Out-of-Hospital Cardiac Arrest with Induced Hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef]
- Peberdy, M.A.; Callaway, C.W.; Neumar, R.W.; Geocadin, R.G.; Zimmerman, J.L.; Donnino, M.; Gabrielli, A.; Silvers, S.M.; Zaritsky, A.L.; Merchant, R.; et al. Part 9: Post-Cardiac Arrest Care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, 768–786. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted Temperature Management at 33 °C versus 36 °C after Cardiac Arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef]
- Dankiewicz, J.; Cronberg, T.; Lilja, G.; Jakobsen, J.C.; Levin, H.; Ullén, S.; Rylander, C.; Wise, M.P.; Oddo, M.; Cariou, A.; et al. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2021, 384, 2283–2294. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Greif, R.; Morley, P.T.; Ng, K.C.; Olasveengen, T.M.; Singletary, E.M.; Soar, J.; Cheng, A.; Drennan, I.R.; Liley, H.G.; et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations: Summary from the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation 2022, 146, e483–e557. [Google Scholar]
- Chen, C.; Ma, T.Z.; Wang, L.N.; Wang, J.J.; Tu, Y.; Zhao, M.L.; Zhang, S.; Sun, H.T.; Li, X.H. Mild Hypothermia Facilitates the Long-Term Survival of Newborn Cells in the Dentate Gyrus after Traumatic Brain Injury by Diminishing a pro-Apoptotic Microenvironment. Neuroscience 2016, 335, 114–121. [Google Scholar] [CrossRef]
- Wang, C.F.; Zhao, C.C.; He, Y.; Li, Z.Y.; Liu, W.L.; Huang, X.J.; Deng, Y.F.; Li, W.P. Mild Hypothermia Reduces Endoplasmic Reticulum Stress-Induced Apoptosis and Improves Neuronal Functions after Severe Traumatic Brain Injury. Brain Behav. 2019, 9, e01248. [Google Scholar] [CrossRef]
- Smith, S.L.; Hall, E.D. Mild Pre- and Posttraumatic Hypothermia Attenuates Blood-Brain Barrier Damage Following Controlled Cortical Impact Injury in the Rat. J. Neurotrauma 1996, 13, 1–9. [Google Scholar] [CrossRef]
- Polderman, K.H. Mechanisms of Action, Physiological Effects, and Complications of Hypothermia. Crit. Care Med. 2009, 37, S186–S202. [Google Scholar] [CrossRef]
- Vassilieff, N.; Rosencher, N.; Sessler, D.I.; Conseiller, C. Shivering Threshold during Spinal Anesthesia Is Reduced in Elderly Patients. Anesthesiology 1995, 83, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Perman, S.M.; Bartos, J.A.; Del Rios, M.; Donnino, M.W.; Hirsch, K.G.; Jentzer, J.C.; Kudenchuk, P.J.; Kurz, M.C.; Maciel, C.B.; Menon, V.; et al. Temperature Management for Comatose Adult Survivors of Cardiac Arrest: A Science Advisory from the American Heart Association. Circulation 2023, 148, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Flynn, L.M.C.C.; Rhodes, J.; Andrews, P.J.D.D.; Al, F.E.T. Therapeutic Hypothermia Reduces Intracranial Pressure and Partial Brain Oxygen Tension in Patients with Severe Traumatic Brain Injury: Preliminary Data from the Eurotherm3235 Trial. Ther. Hypothermia Temp. Manag. 2015, 5, 143–151. [Google Scholar] [CrossRef]
- Sahuquillo, J.; Pérez-Bárcena, J.; Biestro, A.; Zavala, E.; Merino, M.A.; Vilalta, A.; Poca, M.A.; Garnacho, A.; Adalia, R.; Homar, J.; et al. Intravascular Cooling for Rapid Induction of Moderate Hypothermia in Severely Head-Injured Patients: Results of a Multicenter Study (IntraCool). Intensive Care Med. 2009, 35, 890–898. [Google Scholar] [CrossRef]
- Qiu, W.; Zhang, Y.; Sheng, H.; Zhang, J.; Wang, W.; Liu, W.; Chen, K.; Zhou, J.; Xu, Z. Effects of Therapeutic Mild Hypothermia on Patients with Severe Traumatic Brain Injury after Craniotomy. J. Crit. Care 2007, 22, 229–235. [Google Scholar] [CrossRef]
- Zhi, D.; Zhang, S.; Lin, X. Study on Therapeutic Mechanism and Clinical Effect of Mild Hypothermia in Patients with Severe Head Injury. Surg. Neurol. 2003, 59, 381–385. [Google Scholar] [CrossRef]
- Milde, L.N. Clinical Use of Mild Hypothermia for Brain Protection: A Dream Revisited. J. Neurosurg. Anesthesiol. 1992, 4, 211–215. [Google Scholar] [CrossRef]
- Hawryluk, G.W.J.; Aguilera, S.; Buki, A.; Bulger, E.; Citerio, G.; Cooper, D.J.; Arrastia, R.D.; Diringer, M.; Figaji, A.; Gao, G.; et al. A Management Algorithm for Patients with Intracranial Pressure Monitoring: The Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2019, 45, 1783–1794. [Google Scholar] [CrossRef] [PubMed]
- Hui, J.; Feng, J.; Tu, Y.; Zhang, W.; Zhong, C.; Liu, M.; Wang, Y.; Long, L.; Chen, L.; Liu, J.; et al. Safety and Efficacy of Long-Term Mild Hypothermia for Severe Traumatic Brain Injury with Refractory Intracranial Hypertension (LTH-1): A Multicenter Randomized Controlled Trial. EClinicalMedicine 2021, 32, 100732. [Google Scholar] [CrossRef]
- Léger, M.; Frasca, D.; Roquilly, A.; Seguin, P.; Cinotti, R.; Dahyot-Fizelier, C.; Asehnoune, K.; Le Borgne, F.; Gaillard, T.; Foucher, Y.; et al. Early Use of Barbiturates Is Associated with Increased Mortality in Traumatic Brain Injury Patients from a Propensity Score-Based Analysis of a Prospective Cohort. PLoS ONE 2022, 17, e0268013. [Google Scholar] [CrossRef]
- Kajiwara, S.; Hasegawa, Y.; Negoto, T.; Orito, K.; Kawano, T.; Yoshitomi, M.; Sakata, K.; Takeshige, N.; Yamakawa, Y.; Jono, H.; et al. Efficacy of a Novel Prophylactic Barbiturate Therapy for Severe Traumatic Brain Injuries: Step-down Infusion of a Barbiturate with Normothermia. Neurol. Med. Chir. 2021, 61, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Chen, D.; Ding, L.; Ling, W.; Xu, F. Fever Burden Is an Independent Predictor for Prognosis of Traumatic Brain Injury. PLoS ONE 2014, 9, e90956. [Google Scholar] [CrossRef] [PubMed]
- Rosengart, A.J.; Schultheiss, K.E.; Tolentino, J.; Macdonald, R.L. Prognostic Factors for Outcome in Patients with Aneurysmal Subarachnoid Hemorrhage. Stroke 2007, 38, 2315–2321. [Google Scholar] [CrossRef]
- Bray, J.E.; Stub, D.; Bloom, J.E.; Segan, L.; Mitra, B.; Smith, K.; Finn, J.; Bernard, S. Changing Target Temperature from 33 °C to 36 °C in the ICU Management of Out-of-Hospital Cardiac Arrest: A before and after Study. Resuscitation 2017, 113, 39–43. [Google Scholar] [CrossRef]
- Greer, D.M.; Funk, S.E.; Reaven, N.L.; Ouzounelli, M.; Uman, G.C. Impact of Fever on Outcome in Patients with Stroke and Neurologic Injury: A Comprehensive Meta-Analysis. Stroke 2008, 39, 3029–3035. [Google Scholar] [CrossRef]
- Kinoshita, K.; Chatzipanteli, K.; Alonso, O.F.; Howard, M.; Dietrich, W.D. The Effect of Brain Temperature on Hemoglobin Extravasation after Traumatic Brain Injury. J. Neurosurg. 2002, 97, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, E.; Fujisawa, H.; Ito, H.; Ishikawa, T.; Maekawa, T. Brain Temperature Modifies Glutamate Neurotoxicity In Vivo. J. Neurotrauma 2009, 16, 285–297. [Google Scholar] [CrossRef]
- Ginsberg, M.D.; Sternau, L.L.; Globus, M.Y.; Dietrich, W.D.; Busto, R. Therapeutic Modulation of Brain Temperature: Relevance to Ischemic Brain Injury. Cerebrovasc. Brain Metab. Rev. 1992, 4, 189–225. [Google Scholar] [PubMed]
- Jiang, J.Y.; Lyeth, B.G.; Kapasi, M.Z.; Jenkins, L.W.; Povlishock, J.T. Moderate Hypothermia Reduces Blood-Brain Barrier Disruption Following Traumatic Brain Injury in the Rat. Acta Neuropathol. 1992, 84, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Young, A.B.; Ott, L.G.; Beard, D.; Dempsey, R.J.; Tibbs, P.A.; McClain, C.J. The Acute-Phase Response of the Brain-Injured Patient. J. Neurosurg. 1988, 69, 375–380. [Google Scholar] [CrossRef]
- Picetti, E.; Oddo, M.; Prisco, L.; Helbok, R.; Taccone, F.S. A Survey on Fever Monitoring and Management in Patients With Acute Brain Injury: The SUMMA Study. J. Neurosurg. Anesthesiol. 2019, 31, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.J.D.; Sinclair, H.L.; Rodriguez, A.; Harris, B.A.; Battison, C.G.; Rhodes, J.K.J.; Murray, G.D.; Eurotherm3235 Trial Collaborators. Hypothermia for Intracranial Hypertension after Traumatic Brain Injury. N. Engl. J. Med. 2015, 373, 2403–2412. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.J.; Nichol, A.D.; Bailey, M.; Bernard, S.; Cameron, P.A.; Pili-Floury, S.; Forbes, A.; Gantner, D.; Higgins, A.M.; Huet, O.; et al. Effect of Early Sustained Prophylactic Hypothermia on Neurologic Outcomes among Patients with Severe Traumatic Brain Injury. JAMA-J. Am. Med. Assoc. 2018, 320, 2211–2220. [Google Scholar] [CrossRef]
- Zhao, Q.J.; Zhang, X.G.; Wang, L.X. Mild Hypothermia Therapy Reduces Blood Glucose and Lactate and Improves Neurologic Outcomes in Patients with Severe Traumatic Brain Injury. J. Crit. Care 2011, 26, 311–315. [Google Scholar] [CrossRef]
- Badjatia, N.; Strongilis, E.; Gordon, E.; Prescutti, M.; Fernandez, L.; Fernandez, A.; Buitrago, M.; Schmidt, J.M.; Ostapkovich, N.D.; Mayer, S.A. Metabolic Impact of Shivering during Therapeutic Temperature Modulation: The Bedside Shivering Assessment Scale. Stroke 2008, 39, 3242–3247. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, Y. Neurocritical Care Update. J. Intensive Care 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Norisue, Y.; Fujimoto, Y.; Nakagawa, K. Preliminary Guideline- and Pathophysiology-Based Protocols for Neurocritical Care. J. Intensive Care 2018, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Maegele, M.; Schöchl, H.; Menovsky, T.; Maréchal, H.; Marklund, N.; Buki, A.; Stanworth, S. Coagulopathy and Haemorrhagic Progression in Traumatic Brain Injury: Advances in Mechanisms, Diagnosis, and Management. Lancet Neurol. 2017, 16, 630–647. [Google Scholar] [CrossRef] [PubMed]
- Hifumi, T.; Kuroda, Y.; Kawakita, K.; Yamashita, S.; Oda, Y.; Dohi, K.; Maekawa, T. Therapeutic Hypothermia in Patients with Coagulopathy Following Severe Traumatic Brain Injury. Scand. J. Trauma. Resusc. Emerg. Med. 2017, 25, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Quine, E.J.; Murray, L.; Trapani, T.; Cooper, D.J. Thromboelastography to Assess Coagulopathy in Traumatic Brain Injury Patients Undergoing Therapeutic Hypothermia. Ther. Hypothermia Temp. Manag. 2021, 11, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Graziano, F.; Rebora, P.; Elli, F.; Giussani, C.; Oddo, M.; Meyfroidt, G.; Helbok, R.; Taccone, F.S.; Prisco, L.; et al. Intracranial Pressure Monitoring in Patients with Acute Brain Injury in the Intensive Care Unit (SYNAPSE-ICU): An International, Prospective Observational Cohort Study. Lancet Neurol. 2021, 20, 548–558. [Google Scholar] [CrossRef]
- Forcione, M.; Yakoub, K.M.; Chiarelli, A.M.; Perpetuini, D.; Merla, A.; Sun, R.; Sawosz, P.; Belli, A.; Davies, D.J. Dynamic Contrast-Enhanced near-Infrared Spectroscopy Using Indocyanine Green on Moderate and Severe Traumatic Brain Injury: A Prospective Observational Study. Quant. Imaging Med. Surg. 2020, 10, 2085–2097. [Google Scholar] [CrossRef]


{kind=link}
| Purpose | ICP Control | Prevention of Fever | Prevention of Secondary Brain Damage in PCAS | Reducing Fever in Heat Patients with Stroke |
|---|---|---|---|---|
| Subject | Severe TBI and stroke | Severe TBI and stroke | PCAS | Severe heat stroke |
| Target temperature | 33–36 °C | 37–38 °C | 32–36 °C | 38 °C |
| Device | Intravascular catheters Surface cooling | Intravascular catheters * | Intravascular catheters Surface cooling | Intravascular catheters |
| Medication | Analgosedative drugs, muscle relaxants, and antipyretic drugs | Antipyretic drugs and analgosedative drugs | Analgosedative drugs, muscle relaxants, and antipyretic drugs | Analgosedative drugs and muscle relaxants |
| Respirator | with | with or without | with | with |
| Duration | 1–2 weeks | 1–2 weeks | ~1 week | 1–2 days |
| Study | Participants (Hypothermia/Control) | Target Temperature (°C) (Hypothermia/Control) | Mean Temperature (°C) of the Control Group | Temperature Management Device (Hypothermia/Control) | Cooling Methods of the Hypothermia Group | Poor Outcome (Hypothermia/Control), p-Value |
|---|---|---|---|---|---|---|
| Shiozaki 2001 [1] | 45/46 | 33.5–34.5/36.5–37.5 | n.a. | Cooling blankets/surface cooling | Cooling blankets, gastric lavage with cold fluid | 53%/41%, p = 0.251 |
| Clifton 2001 NABIS: H [5] | 190/178 | 32.5–34.0/37.0 | 37.2 ± 0.8 | Temperature control pads/n.a. | Gastric lavage with cold fluid and room temperature ventilated air | 57%/57%, p = 0.99 |
| Clifton 2011 NABIS: H2 [7] | 52/45 | 33.0/37.0 | 37.2 ± 0.4 | Surface cooling (Arctic Sun®)/cooling blankets | Intravenous cold fluid, gastric lavage with cold fluid, surface cooling, room temperature of ventilated air | 60%/56%, p = 0.67 |
| Maekawa 2015 BHYPO [6] | 95/45 | 32.0–34.0/35.5–37.0 | 35.7 ± 1.0 (Day 1) | Cooling blankets/cooling blankets | Surface cooling, gastric lavage with cold fluid and intravenous cold fluid | 53%/48%, p = 0.597 |
| Andrews 2015 Eurotherm3235 [48] | 195/192 | 32.0–35.0/n. a. | 37.0 | Usual cooling technique/n.a. | Intravenous cold fluid | 74.3%/63.5%, p = 0.03 |
| Cooper 2018 POLAR [49] | 256/239 | 32.5–33.5/36.5–37.5 | 37.0 | Surface cooling/surface cooling | Intravenous cold fluid and surface cooling | 51.2%/49.1%, p = 0.94 |
| Hui 2021 LTH-1 [35] | 156/146 | 34.0–35.0/37.0 | 37.08 | Cooling blankets/surface cooling | Cooling blankets | 41.3%/51.9%, p = 0.105 |
| Hergenroeder 2022 HOPES [9] | 16/16 | 33.0/37.0 | 36.0–37.0 | Intravascular catheters (Thermogard System®)/intravascular catheters (Thermogard System®) | Intravascular cooling | 62%/75%, p = 0.35 |
| Study | Participants (Hypothermia/Control) | Target Temperature (°C) (Hypothermia/Control) | Mean Temperature (°C) of the Control Group | Temperature Management Device (Hypothermia/Control) | Cooling Methods of the Hypothermia Group | Poor Outcome (Hypothermia/Control), p-Value |
|---|---|---|---|---|---|---|
| Jiang 2000 [2] | 43/44 | 33–35/37–38 | n.a. | Cooling blankets/n.a. | Cooling blankets | 53.5%/72.7%, p < 0.05 |
| Qiu 2007 [31] | 40/40 | 34.5–36.0/37.5–38.0 | n.a. | Cooling blankets, cooling caps/none | Cooling blankets, cooling caps, surface cooling, intravenous cold fluid | 30.0%/52.5%, p = 0.041 |
| Zhi 2003 [32] | 198/198 | 32.0–35.0/36.5–37.0 | n.a. | Cooling blankets/n.a. | Cooling blankets | 38.3%/62.1%, p: n.a. |
| Zhao 2011 [50] | 40/41 | 32.5–33.0/37.0 | n.a. | Cooling blankets/n.a. | Cooling blankets | 25.0%/48.8%, p = 0.038 |
| STEP 1 (Go to next step if BSAS > 0) | Acetaminophen 650–1000 mg IV/PO q 4–6 h Skin counter-warming Magnesium sulfate 20 mEq/20 mg IV (if with hypomagnesemia) |
| STEP 2 (Go to next step if BSAS > 0) | Meperidine 35–50 mg IV q 3–4 h and/or Dexmedetomidine IV infusion 0.2 mcg/kg/h and/or Fentanyl IV infusion 25 mcg/h |
| STEP 3 (Go to next step if BSAS > 0) | Intubation if not already undertaken Propofol 20–40 mg IV bolus followed by 0.5–3 mg/kg/h or Midazolam 3–5 mg IV bolus followed by 0.06–0.18 mg/kg/h |
| STEP 4 | Rocuronium 50 mg IV bolus followed by 10–20 mg/h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawakita, K.; Shishido, H.; Kuroda, Y. Review of Temperature Management in Traumatic Brain Injuries. J. Clin. Med. 2024, 13, 2144. https://doi.org/10.3390/jcm13072144
Kawakita K, Shishido H, Kuroda Y. Review of Temperature Management in Traumatic Brain Injuries. Journal of Clinical Medicine. 2024; 13(7):2144. https://doi.org/10.3390/jcm13072144
Chicago/Turabian StyleKawakita, Kenya, Hajime Shishido, and Yasuhiro Kuroda. 2024. "Review of Temperature Management in Traumatic Brain Injuries" Journal of Clinical Medicine 13, no. 7: 2144. https://doi.org/10.3390/jcm13072144
APA StyleKawakita, K., Shishido, H., & Kuroda, Y. (2024). Review of Temperature Management in Traumatic Brain Injuries. Journal of Clinical Medicine, 13(7), 2144. https://doi.org/10.3390/jcm13072144