
Immunomodulation Driven by Theranova Filter during a Single HD Session


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Sample Collection and Laboratory Parameters
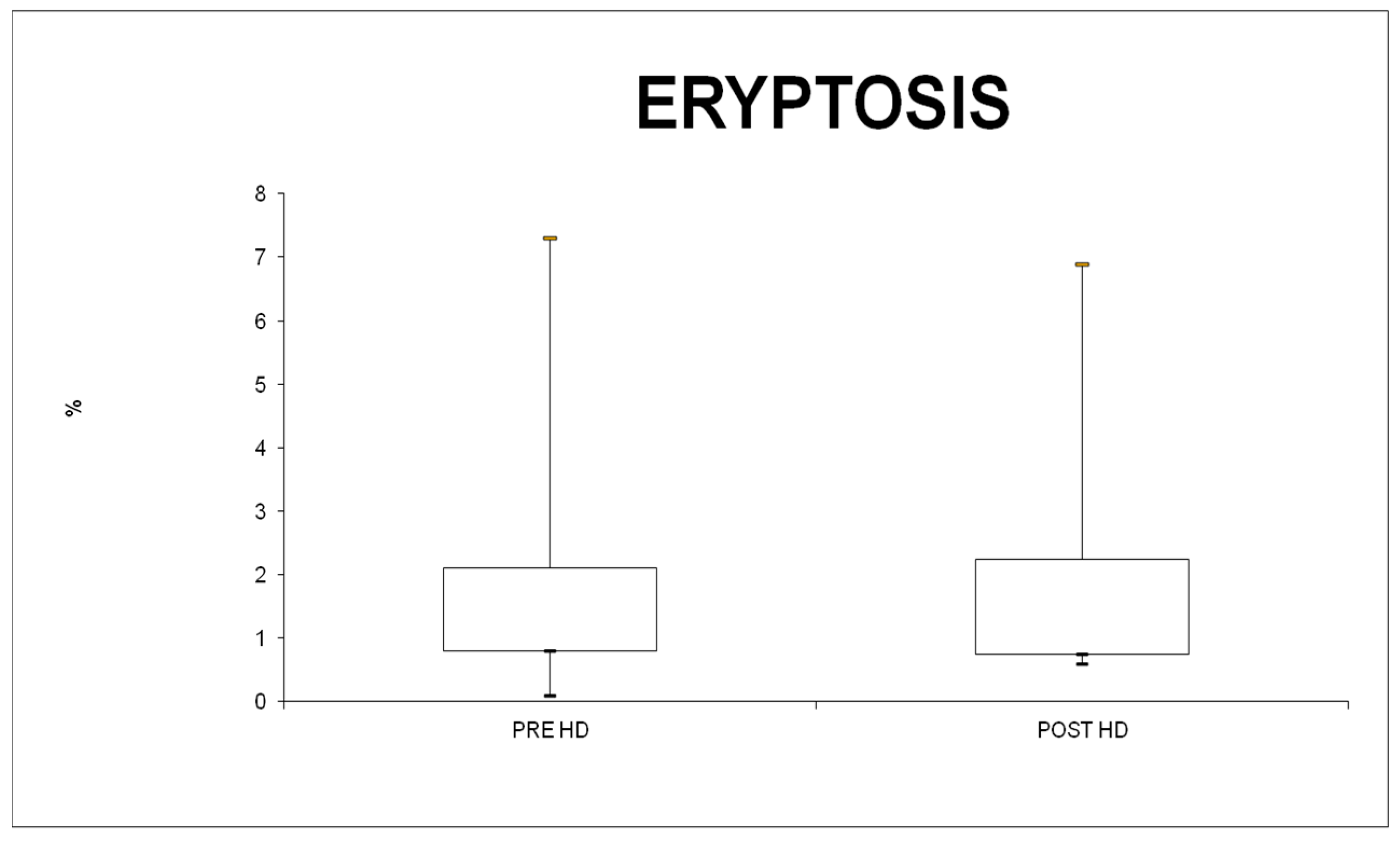
2.3. Eryptosis Evaluation
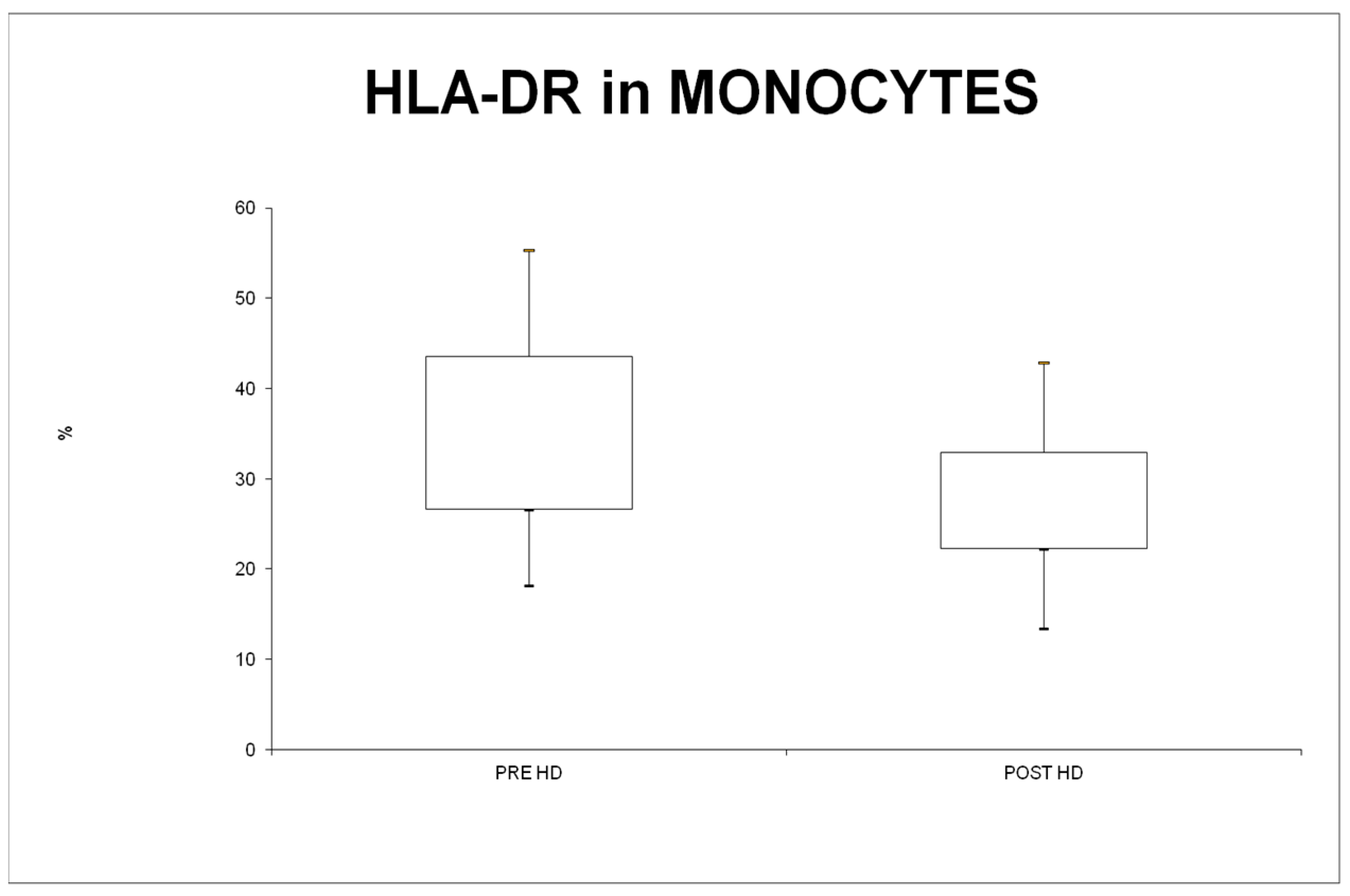
2.4. HLA-DR Expression
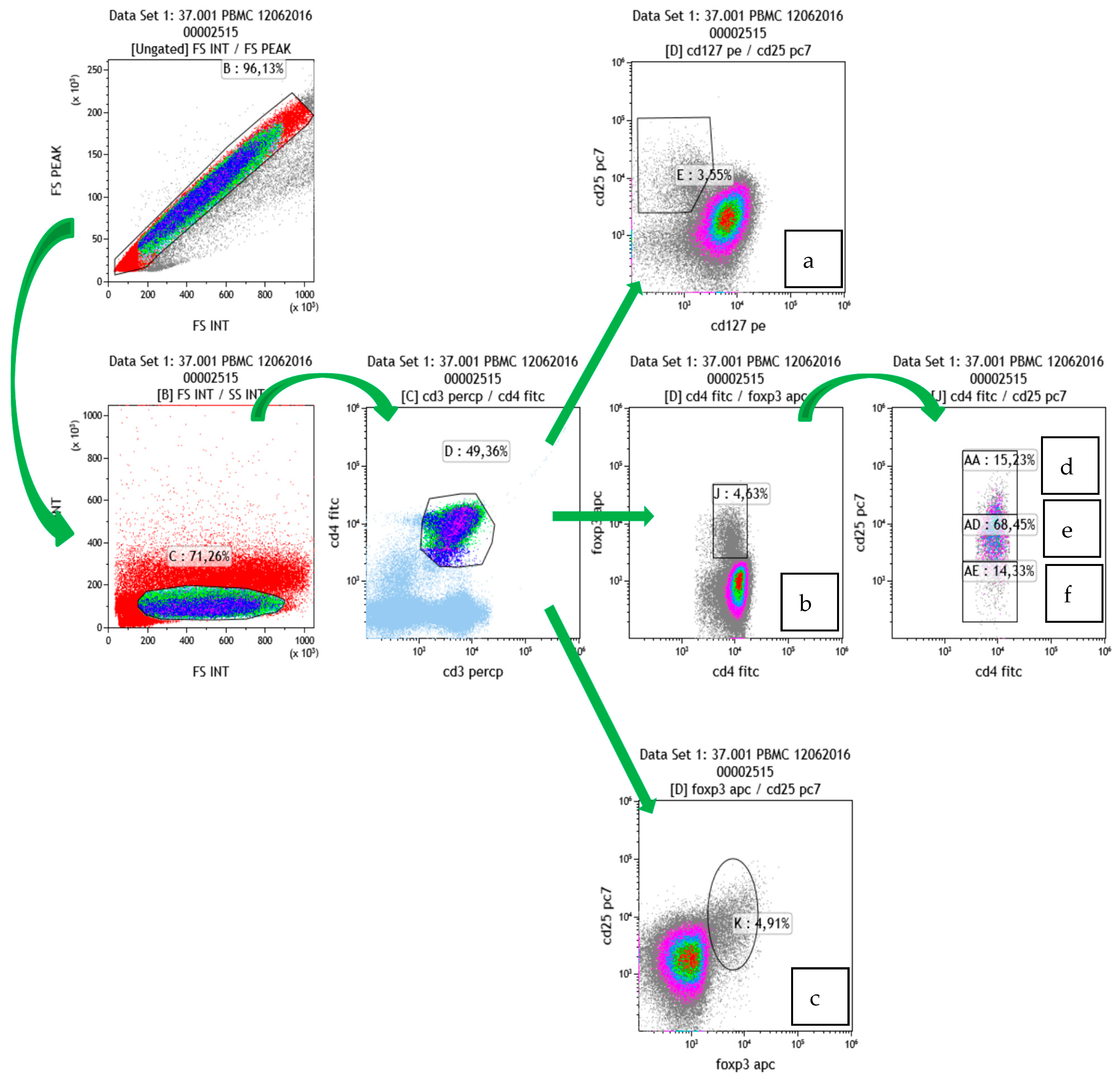
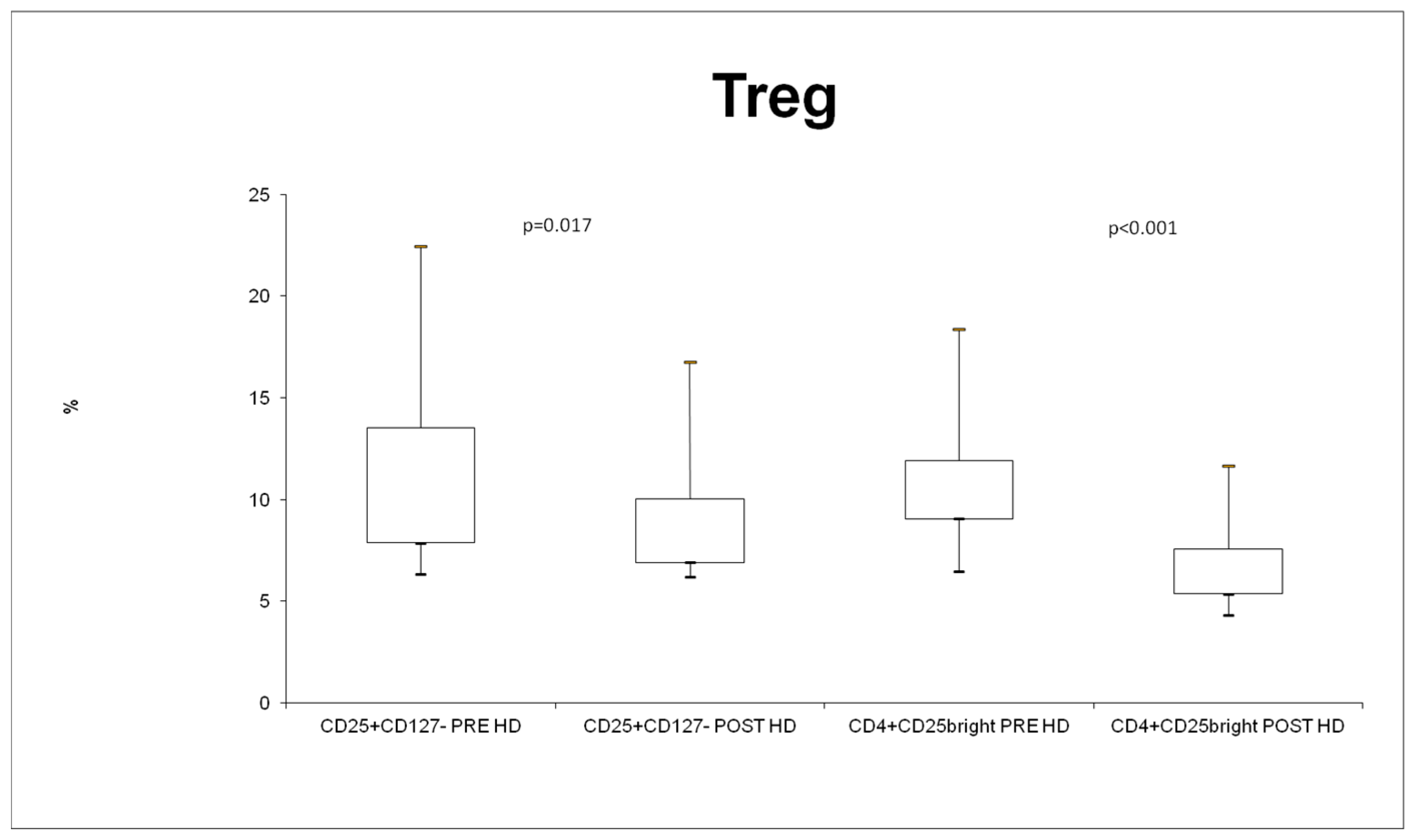
2.5. Treg Cells Detection
2.6. Statistical Analysis
3. Results
3.1. Subjects
3.2. RBC Analysis and Eryptosis
3.3. WBC Counts and Differentiation
3.4. Expression of Monocyte Cell Surface Marker (HLA-DR)
3.5. Treg
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Girndt, M.; Sester, U.; Sester, M.; Kaul, H.; Kohler, H. Impaired cellular immune function in patients with end-stage renal failure. Nephrol. Dial. Transplant. 1999, 14, 2807–2810. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Van Loo, A.; Dhondt, A.M.; De Smet, R.; Ringoir, S. Influence of uraemia and haemodialysis on host defence and infection. Nephrol. Dial. Transplant. 1996, 11, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Stefoni, S.; DeSanctis, L.B.; Nanni-Costa, A.; Iannelli, S.; Borgnino, L.C.; Buscaroli, A.; Buttazzi, R.; La Manna, G.; Todeschini, P.; Giudicissi, G.; et al. Dialysis and the Immune system. Contrib. Nephrol. 1995, 113, 80–91. [Google Scholar] [PubMed]
- Descamps-Latscha, B.; Herbelin, A.; Nguyen, A.T.; Roux-Lombard, P.; Zingraff, J.; Moynot, A.; Verger, C.; Dahmane, D.; de Groote, D.; Jungers, P.; et al. Balance between il-1 beta, tnf-alpha, and their specific inhibitors in chronic renal failure and maintenance dialysis. Relationships with activation markers of t cells, b cells, and monocytes. J. Immunol. 1995, 154, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Schiller, B.; Ziegler-Heitbrock, H.W.; Meyer, N.; Schmidt, B.; Blumenstein, M. Monocyte phenotype and interleukin-1 production in patients undergoing haemodialysis. Nephron 1991, 59, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Von Appen, K.; Goolsby, C.; Mehl, P.; Goewert, R.; Ivanovich, P. Leukocyte adhesion molecules as biocompatibility markers for hemodialysis membranes. ASAIO J. 1994, 40, M609–M615. [Google Scholar] [CrossRef]
- Ruiz, P.; Gomez, F.; Schreiber, A.D. Impaired function of macrophage fc gamma receptors in end-stage renal disease. N. Engl. J. Med. 1990, 322, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Roccatello, D.; Mazzucco, G.; Coppo, R.; Piccoli, G.; Rollino, C.; Scalzo, B.; Guerra, M.G.; Cavalli, G.; Giachino, O.; Amore, A.; et al. Functional changes of monocytes due to dialysis membranes. Kidney Int. 1989, 35, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Grooteman, M.P.; Nube, M.J.; van Houte, A.J.; Schoorl, M.; van Limbeek, J. Granulocyte sequestration in dialysers: A comparative elution study of three different membranes. Nephrol. Dial. Transplant. 1995, 10, 1859–1864. [Google Scholar]
- Grooteman, M.P.; Nube, M.J.; van Limbeek, J.; Schoorl, M.; van Houte, A.J. Lymphocyte subsets in dialyser eluates: A new parameter of bioincompatibility? Nephrol. Dial. Transplant. 1996, 11, 1073–1078. [Google Scholar] [CrossRef]
- Schouten, W.E.; Grooteman, M.P.; Schoorl, M.; van Houte, A.J.; Nube, M.J. Monocyte activation in peripheral blood and dialyser eluates: Phenotypic profile and cytokine release. Nephron 2002, 91, 646–653. [Google Scholar] [CrossRef]
- Lang, F.; Bissinger, R.; Abed, M.; Artunc, F. Eryptosis—the neglected cause of anemia in end stage renal disease. Kidney Blood Press. Res. 2017, 42, 749–760. [Google Scholar] [CrossRef] [PubMed]
- Hendrikx, T.K.; van Gurp, E.A.; Mol, W.M.; Schoordijk, W.; Sewgobind, V.D.; Ijzermans, J.N.; Weimar, W.; Baan, C.C. End-stage renal failure and regulatory activities of cd4+ cd25bright+ foxp3+ T-cells. Nephrol. Dial. Transplant. 2009, 24, 1969–1978. [Google Scholar] [CrossRef] [PubMed]
- De Cal, M.; Cruz, D.N.; Corradi, V.; Nalesso, F.; Polanco, N.; Lentini, P.; Brendolan, A.; Tetta, C.; Ronco, C. Hla-dr expression and apoptosis: A cross-sectional controlled study in hemodialysis and peritoneal dialysis patients. Blood Purif. 2008, 26, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Kaminska, D.; Koscielska-Kasprzak, K.; Chudoba, P.; Mazanowska, O.; Banasik, M.; Zabinska, M.; Boratynska, M.; Lepiesza, A.; Korta, K.; Gomolkiewicz, A.; et al. Type of renal replacement therapy (hemodialysis versus peritoneal dialysis) does not affect cytokine gene expression or clinical parameters of renal transplant candidates. BioMed Res. Int. 2015, 2015, 797490. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Schaier, M.; Leick, A.; Uhlmann, L.; Kalble, F.; Eckstein, V.; Ho, A.; Meuer, S.; Mahnke, K.; Sommerer, C.; Zeier, M.; et al. The role of age-related t-cell differentiation in patients with renal replacement therapy. Immunol. Cell Biol. 2017, 95, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Rimmele, T.; Payen, D.; Cantaluppi, V.; Marshall, J.; Gomez, H.; Gomez, A.; Murray, P.; Kellum, J.A. Immune cell phenotype and function in sepsis. Shock 2016, 45, 282–291. [Google Scholar] [CrossRef]
- Almeida, A.; Lourenco, O.; Fonseca, A.M. Haemodialysis in diabetic patients modulates inflammatory cytokine profile and t cell activation status. Scand. J. Immunol. 2015, 82, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Crowley, L.C.; Marfell, B.J.; Scott, A.P.; Waterhouse, N.J. Quantitation of apoptosis and necrosis by annexin v binding, propidium iodide uptake, and flow cytometry. Cold Spring Harb. Protoc. 2016, 2016, pdb-prot087288. [Google Scholar] [CrossRef]
- Lang, E.; Lang, F. Triggers, inhibitors, mechanisms, and significance of eryptosis: The suicidal erythrocyte death. Biomed. Res. Int. 2015, 2015, 513518. [Google Scholar] [CrossRef]
- Fazekas de St Groth, B.; Zhu, E.; Asad, S.; Lee, L. Flow cytometric detection of human regulatory t cells. Methods Mol. Biol. 2011, 707, 263–279. [Google Scholar] [PubMed]
- Steinborn, A.; Schmitt, E.; Kisielewicz, A.; Rechenberg, S.; Seissler, N.; Mahnke, K.; Schaier, M.; Zeier, M.; Sohn, C. Pregnancy-associated diseases are characterized by the composition of the systemic regulatory t cell (treg) pool with distinct subsets of tregs. Clin. Exp. Immunol. 2012, 167, 84–98. [Google Scholar] [CrossRef] [PubMed]
- Alikhan, M.A.; Huynh, M.; Kitching, A.R.; Ooi, J.D. Regulatory t cells in renal disease. Clin. Transl. Immunol. 2018, 7, e1004. [Google Scholar] [CrossRef] [PubMed]
- Safinia, N.; Vaikunthanathan, T.; Fraser, H.; Thirkell, S.; Lowe, K.; Blackmore, L.; Whitehouse, G.; Martinez-Llordella, M.; Jassem, W.; Sanchez-Fueyo, A.; et al. Successful expansion of functional and stable regulatory t cells for immunotherapy in liver transplantation. Oncotarget 2016, 7, 7563–7577. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Salazar, E.K.; Cortes-Hernandez, A.; Aleman-Muench, G.R.; Alberu, J.; Rodriguez-Aguilera, J.R.; Recillas-Targa, F.; Chagoya de Sanchez, V.; Cuevas, E.; Mancilla-Urrea, E.; Perez Garcia, M.; et al. Methylation of foxp3 tsdr underlies the impaired suppressive function of tregs from long-term belatacept-treated kidney transplant patients. Front. Immunol. 2017, 8, 219. [Google Scholar] [CrossRef]
- Sharma, R.; Kinsey, G.R. Regulatory t cells in acute and chronic kidney diseases. Am. J. Physiol. Renal Physiol. 2018, 314, F679–F698. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Treatment | ||||||
|---|---|---|---|---|---|---|---|
| Age (at Treatment) 2017 | Gender (F/M) | DM (Yes/No) | Kt/V | Qb | UreaPRE | Duration | |
| 1 | 70 | M | yes | 1.06 | 248.3 | 95 | 4 |
| 2 | 67 | M | yes | 0.95 | 210 | 189.5 | 4 |
| 3 | 65 | M | yes | 1.28 | 350 | 160 | 4.5 |
| 4 | 64 | M | no | 1 | 213 | 156.3 | 4 |
| 5 | 70 | M | yes | 0.9 | 200 | 125 | 3.5 |
| 6 | 63 | F | yes | 1.2 | 300 | 162 | 3.5 |
| 7 | 81 | M | no | 1.25 | 310 | 153 | 4 |
| 8 | 86 | M | no | 1.3 | 300 | 95 | 3.5 |
| 9 | 84 | M | yes | 1.2 | 300 | 123 | 3.5 |
| 10 | 71 | F | no | 1.3 | 320 | 159 | 4 |
| 11 | 79 | F | no | 0.9 | 250 | 121 | 3.5 |
| MedianPRE | MedianPOST | p Value | |
|---|---|---|---|
| Lymphocytes | 51.76; IQR 42.93–60.15 | 47.7; IQR 41.37–60.81 | 0.54 |
| T Lymphocytes | 18.79; IQR 13.15–23.61 | 16.95; IQR 8.65–21.81 | 0.42 |
| Monocytes | 18.4; IQR 13.45–31.55 | 17.1; IQR 11.6–22.85 | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caprara, C.; Virzì, G.M.; Chieregato, K.; Marchionna, N.; Corradi, V.; Brendolan, A.; Ronco, C.; Zanella, M. Immunomodulation Driven by Theranova Filter during a Single HD Session. J. Clin. Med. 2024, 13, 2147. https://doi.org/10.3390/jcm13072147
Caprara C, Virzì GM, Chieregato K, Marchionna N, Corradi V, Brendolan A, Ronco C, Zanella M. Immunomodulation Driven by Theranova Filter during a Single HD Session. Journal of Clinical Medicine. 2024; 13(7):2147. https://doi.org/10.3390/jcm13072147
Chicago/Turabian StyleCaprara, Carlotta, Grazia Maria Virzì, Katia Chieregato, Nicola Marchionna, Valentina Corradi, Alessandra Brendolan, Claudio Ronco, and Monica Zanella. 2024. "Immunomodulation Driven by Theranova Filter during a Single HD Session" Journal of Clinical Medicine 13, no. 7: 2147. https://doi.org/10.3390/jcm13072147
APA StyleCaprara, C., Virzì, G. M., Chieregato, K., Marchionna, N., Corradi, V., Brendolan, A., Ronco, C., & Zanella, M. (2024). Immunomodulation Driven by Theranova Filter during a Single HD Session. Journal of Clinical Medicine, 13(7), 2147. https://doi.org/10.3390/jcm13072147