
Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Subjects
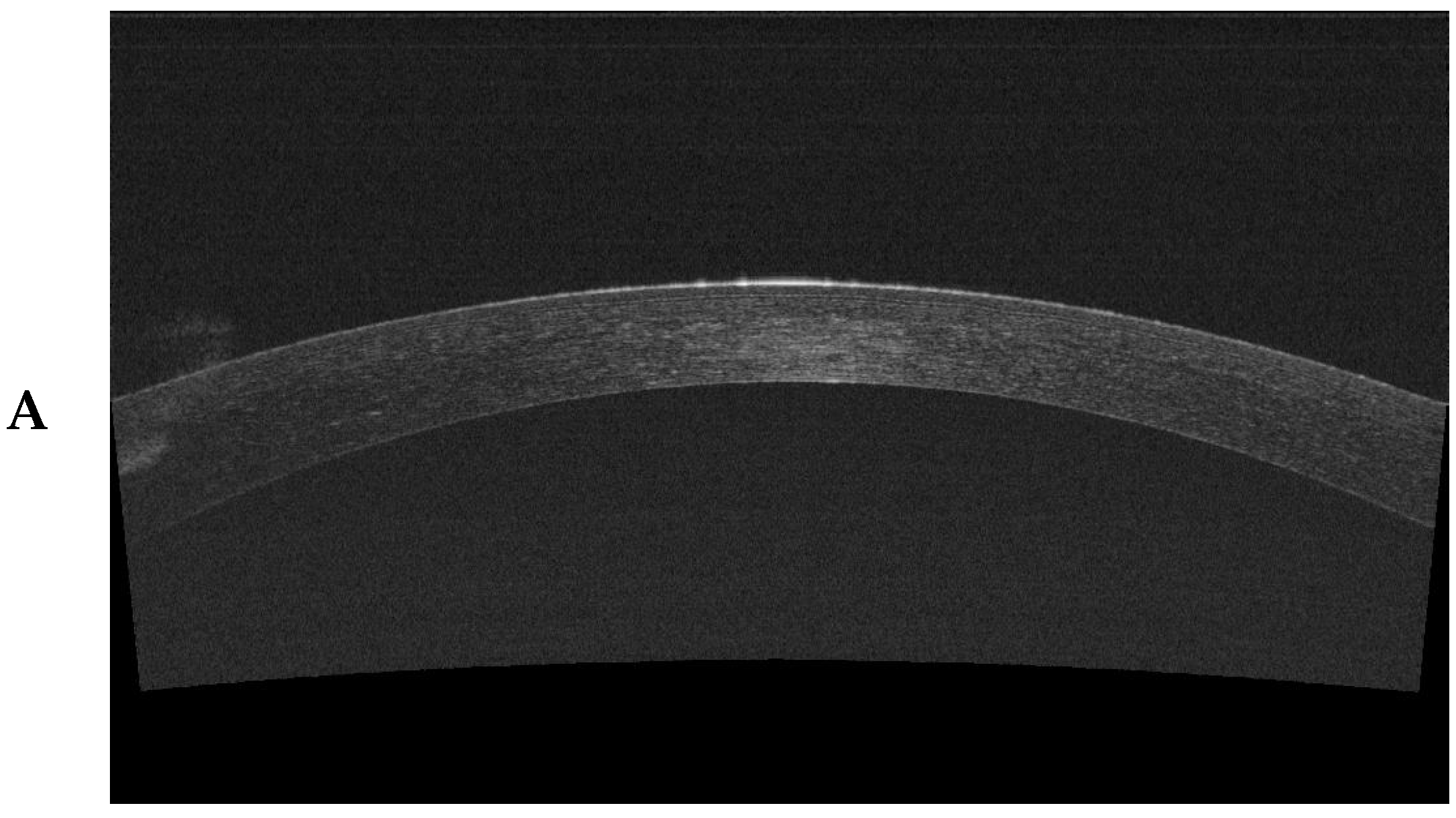
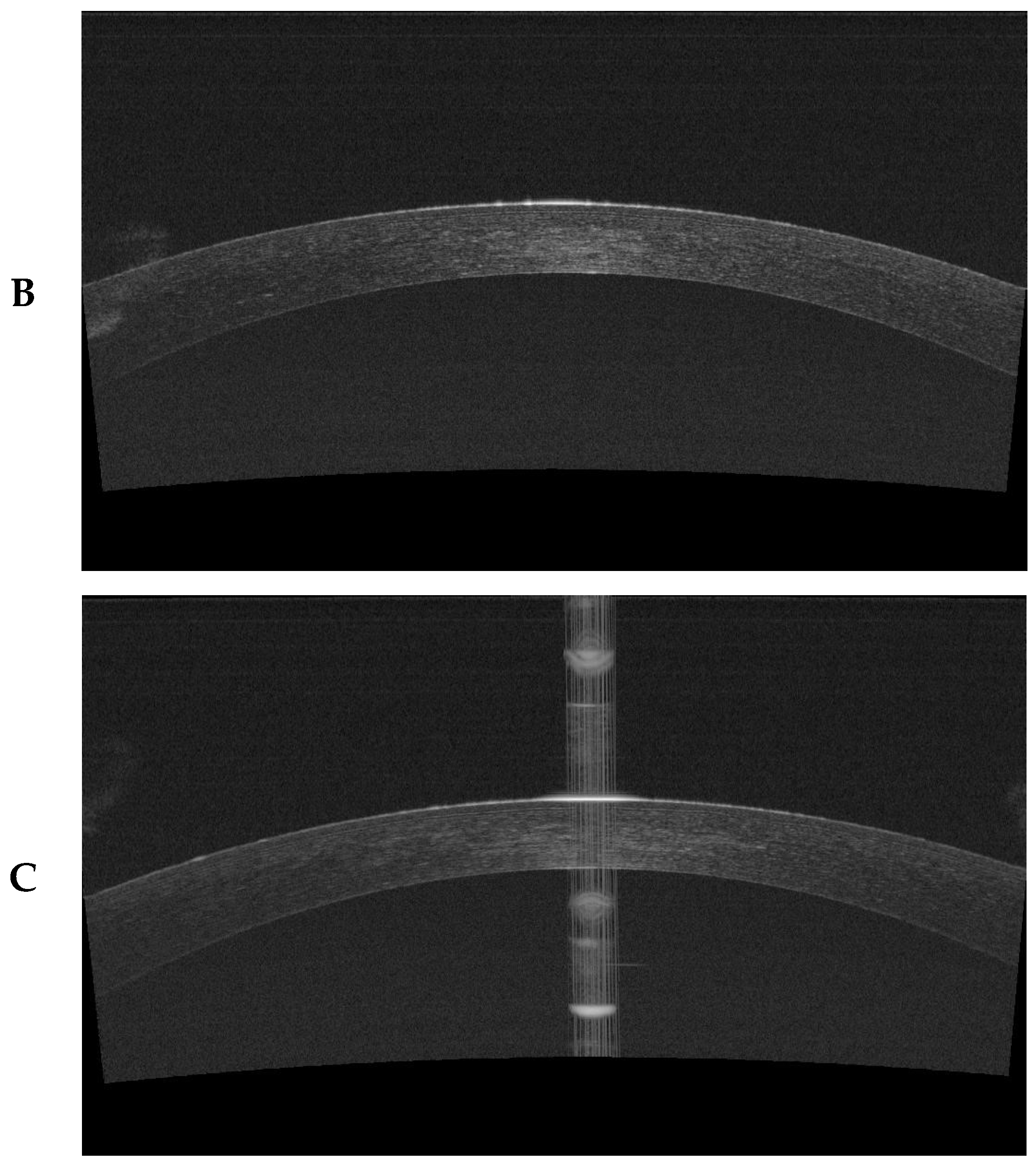
2.3. Anterior Segment Optical Coherence Tomography
2.4. Surgical Intervention—The ReLEx SMILE Procedure
- cutting posterior lamellar plane—refractive
- cutting lenticule side
- cutting anterior lamellar plane—neutral
- cap side cut—port—position 115°
2.5. Statistical Analysis
3. Results
3.1. Analysis of Qualitative Changes That Characterized the Study Group
3.2. Changes in Cap Thickness during the Observation
3.3. Changes in the RST during the Observation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernández-Barrientos, Y.; Ramos-Suárez, A.; Fernández-Sánchez, F.; Tirado-Carmona, A. Post-Laser in Situ Keratomileusis Interface Arthrographis kalrae Keratitis. Arq. Bras. Oftalmol. 2019, 83, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, F.; Shrestha, G.S.; Vijay, A.K.; Carnt, N. Epidemiology, Microbiology, and Genetics of Contact Lens–Related and Non–Contact Lens-Related Infectious Keratitis. Eye Contact Lens 2022, 48, 127–133. [Google Scholar] [CrossRef]
- Konda, N.; Garg, P.; Sharma, S.; Willcox, M.D. Risk Factors for Contact Lens–Related Microbial Keratitis and Associated Vision Loss in a South Indian Population. Eye Contact Lens 2021, 47, 118–126. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Tanya, S.M.; Costello, F.; Kherani, F.; Shamie, N.; Zhu, D. Navigating Personal and Professional Development Through Social Media in Ophthalmology. Clin. Ophthalmol. 2022, 16, 2263. [Google Scholar] [CrossRef] [PubMed]
- Joffe, S.N. The 25th Anniversary of Laser Vision Correction in the United States. Clin. Ophthalmol. 2021, 15, 1163. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, A.H.; Grauslund, J.; Ivarsen, A.R.; Hjortdal, J.Ø. Efficacy, Safety, Predictability, Contrast Sensitivity, and Aberrations after Femtosecond Laser Lenticule Extraction. J. Cataract. Refract. Surg. 2014, 40, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Blum, M.; Täubig, K.; Gruhn, C.; Sekundo, W.; Kunert, K.S. Five-Year Results of Small Incision Lenticule Extraction (ReLEx SMILE). Br. J. Ophthalmol. 2016, 100, 1192–1195. [Google Scholar] [CrossRef] [PubMed]
- Vatsa, S.; Dhawan, P.; Sood, S. A to Z of ReLeX SMILE: ALL You Need to Know. Delhi J. Ophthalmol. 2021, 32, 25–31. [Google Scholar] [CrossRef]
- Klokova, O.A.; Sakhnov, S.N.; Geydenrikh, M.S.; Damashauskas, R.O. Quality of Life after Refractive Surgery: ReLEx SMILE vs Femto-LASIK. Clin. Ophthalmol. 2019, 13, 561–570. [Google Scholar] [CrossRef]
- Pavkova, Z.; Kacerovska, J.; Kacerovsky, M. Comparison of the Efficiency of femtoLASIK and ReLEx SMILE in Terms of Dioptric Error Reduction. Biomed. Pap. Med. Fac. Palacky Univ. Olomouc 2018, 162, 329–334. [Google Scholar] [CrossRef]
- Wolniewińska, M.; Czarnota-Nowakowska, B.; Wolniewińska, J.; Wierzbowska, J.; Kocięcki, J. SMILE—Charakterystyka zabiegu i jakość życia pacjentów. Ophthatherapy 2021, 8, 133–141. [Google Scholar] [CrossRef]
- Chiche, A.; Trinh, L.; Baudouin, C.; Denoyer, A. SMILE (Small Incision Lenticule Extraction) among the Corneal Refractive Surgeries in 2018. J. Fr. D’ophtalmol. 2018, 41, e245–e252. [Google Scholar] [CrossRef] [PubMed]
- Bower, K.S.; Woreta, F. Update on Contraindications for Laser-Assisted in Situ Keratomileusis and Photorefractive Keratectomy. Curr. Opin. Ophthalmol. 2014, 25, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T.K.; Ryu, I.H.; Lee, G.; Kim, Y.; Kim, J.K.; Lee, I.S.; Kim, J.S.; Rim, T.H. Adopting Machine Learning to Automatically Identify Candidate Patients for Corneal Refractive Surgery. NPJ Digit. Med. 2019, 2, 59. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Luo, Y.; Ye, Y.; Chen, P.; Liu, C.; Lei, L.; Zhuang, J.; Yu, K. A Comparative and Prospective Study of Corneal Biomechanics after SMILE and FS-LASIK Performed on the Contralateral Eyes of High Myopia Patients. Ann. Transl. Med. 2022, 10, 730. [Google Scholar] [CrossRef] [PubMed]
- Nanavaty, M.A.; Naveed, H.; Ashena, Z.; Mukhija, R. Ex-Vivo Study on the Surface Quality of Corneal Lenticule and Stroma after Low Energy Femtosecond Laser Lenticule Extraction. Sci. Rep. 2022, 12, 10034. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Archer, T.J.; Randleman, J.B. Mathematical Model to Compare the Relative Tensile Strength of the Cornea after PRK, LASIK, and Small Incision Lenticule Extraction. J. Refract. Surg. 2013, 29, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Horodyńska, D. ReLEx SMILE–Najnowsza Metoda Laserowej Korekcji Wad Wzroku–Bez Płatka, Bez Ekscimera, Tylko Laser Femtosekundowy. Ophtha Ther. Ther. Ophthalmol. 2015, 2, 187–196. [Google Scholar]
- Salaroli, C.H.R.; Li, Y.; Zhang, X.; Tang, M.; Ramos, J.L.B.; Allemann, N.; Huang, D. Repeatability of Laser in Situ Keratomileusis Flap Thickness Measurement by Fourier-Domain Optical Coherence Tomography. J. Cataract. Refract. Surg. 2011, 37, 649–654. [Google Scholar] [CrossRef][Green Version]
- Garcia, P.N.; Chamon, W.; Allemann, N. Comparability of Corneal Thickness and Opacity Depth Assessed by OCT and UBM. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 1915–1923. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M.; Johnson, N. Accuracy and Reproducibility of Artemis Central Flap Thickness and Visual Outcomes of LASIK with the Carl Zeiss Meditec VisuMax Femtosecond Laser and MEL 80 Excimer Laser Platforms. J. Refract. Surg. 2010, 26, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Brar, S.; Rathod, D.P.; Roopashree, C.R.; Ganesh, S. One-Year Visual and Refractive Outcomes Following LASIK for Myopia and Myopic Astigmatism with MEL 90 versus Schwind Amaris 750S Excimer Laser: A Comparative Study. J. Ophthalmol. 2021, 2021, 9929181. [Google Scholar] [CrossRef] [PubMed]
- Tay, E.; Li, X.; Chan, C.; Tan, D.T.; Mehta, J.S. Refractive Lenticule Extraction Flap and Stromal Bed Morphology Assessment with Anterior Segment Optical Coherence Tomography. J. Cataract. Refract. Surg. 2012, 38, 1544–1551. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Wang, L.; Zhou, X.-T.; Yu, Z.-Q. Cap Morphology after Small-Incision Lenticule Extraction and Its Effects on Intraocular Scattering. Int. J. Ophthalmol. 2018, 11, 456. [Google Scholar] [PubMed]
- Zhao, J.; Yao, P.; Li, M.; Chen, Z.; Shen, Y.; Zhao, Z.; Zhou, Z.; Zhou, X. The Morphology of Corneal Cap and Its Relation to Refractive Outcomes in Femtosecond Laser Small Incision Lenticule Extraction (SMILE) with Anterior Segment Optical Coherence Tomography Observation. PLoS ONE 2013, 8, e70208. [Google Scholar] [CrossRef][Green Version]
- Smorawski, M.; Nawrot, G.; Wierzbowska, J. Chirurgia Refrakcyjna Rogówki–Przegląd Technologii Laserowych i Metod. OphthaTher. Ther. Ophthalmol. 2016, 3, 38–44. [Google Scholar]
- Wierzbowska, J.; Smorawski, M.; Uram, D. Indywidualizacja Wyboru Metody Korekcji Wady Wzroku. OphthaTher. Ther. Ophthalmol. 2021, 8, 58–64. [Google Scholar] [CrossRef]
- Tataru, C.P. The Current State of Refractive Surgery. Rom. J. Ophthalmol. 2017, 61, 237. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Carp, G.I.; Archer, T.J.; Buick, T.; Gobbe, M.; Rowe, E.L.; Jukic, M.; Brandon, E.; Moore, J.; Moore, T. LASIK for the Correction of High Hyperopic Astigmatism with Epithelial Thickness Monitoring. J. Refract. Surg. 2017, 33, 314–321. [Google Scholar] [CrossRef]
- Riau, A.K.; Angunawela, R.I.; Chaurasia, S.S.; Lee, W.S.; Tan, D.T.; Mehta, J.S. Early Corneal Wound Healing and Inflammatory Responses after Refractive Lenticule Extraction (ReLEx). Investig. Ophthalmol. Vis. Sci. 2011, 52, 6213–6221. [Google Scholar] [CrossRef]
- Blum, M.; Lauer, A.S.; Kunert, K.S.; Sekundo, W. 10-Year Results of Small Incision Lenticule Extraction. J. Refract. Surg. 2019, 35, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Latz, C.; Asshauer, T.; Rathjen, C.; Mirshahi, A. Femtosecond-Laser Assisted Surgery of the Eye: Overview and Impact of the Low-Energy Concept. Micromachines 2021, 12, 122. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, M.J.; Ruiz-Oblitas, L.; Munuera, J.M.; Aliseda, D.; García-Layana, A.; Moreno-Montañés, J. Optical Coherence Tomography Evaluation of the Corneal Cap and Stromal Bed Features after Laser in Situ Keratomileusis for High Myopia and Astigmatism. Ophthalmology 2000, 107, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Netto, M.V.; Shekhar, R.; Krueger, R.R.; Huang, D. A Longitudinal Study of LASIK Flap and Stromal Thickness with High-Speed Optical Coherence Tomography. Ophthalmology 2007, 114, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Thomas, J.; Cox, I.; Rollins, A. Noncontact Measurements of Central Corneal Epithelial and Flap Thickness after Laser in Situ Keratomileusis. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1812–1816. [Google Scholar] [CrossRef]
- Bohac, M.; Koncarevic, M.; Dukic, A.; Biscevic, A.; Cerovic, V.; Merlak, M.; Gabric, N.; Patel, S. Unwanted Astigmatism and High-order Aberrations One Year after Excimer and Femtosecond Corneal Surgery. Optom. Vis. Sci. 2018, 95, 1064–1076. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Expressing informed consent to participate in this study | Lack of informed consent to participate in this study |
| Age over 18 years | Younger than 18 years of age |
| Stable refraction in the year preceding this study | Opaque optical media |
| Myopia ≤ −3.0 DS | Current or past inflammation of the vascular membrane |
| Astigmatism ≤ 3.0 Dcyl | Eye defects |
| CDVA ≥ 0.5 on the Snellen chart | Undergone laser corneal treatment |
| CT ≥ 490 µm | Undergone surgical treatment of the eyes |
| RST ≥ 250 µm | Autoimmune diseases |
| Normal corneal topography | Diabetes |
| Pregnancy and breastfeeding |
| Division | Gender | Total | Chi Test Result2, p-Value | ||
|---|---|---|---|---|---|
| Female (n = 37) | Male (n = 13) | ||||
| Eye | Right | 18 (49.30%) | 7 (52.00%) | 25 (50.00%) | Chi2 = 0.104 p = 0.748 |
| Left | 19 (50.70%) | 6 (48.00%) | 25 (50.00%) | ||
| Myopic astigmatism | No | 18 (47.90%) | 7 (56.00%) | 25 (50.00%) | Chi2 = 0.104 p = 0.748 |
| Yes | 19 (52.10%) | 6 (44.00%) | 25 (50.00%) | ||
| Visual impairment | No | 29 (79.50%) | 12 (92.00%) | 41 (82.00%) | Chi2 = 1.260 p = 0.261 |
| Yes | 8 (20.50%) | 1 (8.00%) | 9 (18.00%) | ||
| 1 Day | 7 Days | 60 Days | 180 Days | p-Value | |
|---|---|---|---|---|---|
| Cap center (µm) | 144.27 ± 15.85 | 141.20 ± 13.89 | 136.56 ± 12.03 | 135.05 ± 11.22 | 0.014 1 <0.001 2 0.224 3 |
| Cap position 12 (µm) | 138.14 ± 11.46 | 138.68 ± 12.73 | 134.19 ± 10.21 | 132.52 ± 8.75 | 0.598 1 <0.001 2 0.102 3 |
| Cap position 6 (µm) | 143.18 ± 13.31 | 142.00 ± 12.80 | 137.54 ± 11.40 | 132.79 ± 10.58 | 0.301 1 <0.001 2 <0.001 3 |
| Cap position 3 (µm) | 143.57 ± 11.63 | 142.51 ± 12.70 | 137.68 ± 10.63 | 133.81 ± 10.25 | 0.337 1 <0.001 2 <0.001 3 |
| Cap position 9 (µm) | 137.32 ± 12.10 | 134.96 ± 10.85 | 132.67 ± 10.55 | 130.50 ± 8.84 | 0.024 1 0.028 2 0.038 3 |
| 1 Day | 7 Days | 60 Days | 180 Days | p-Value | |
|---|---|---|---|---|---|
| RST center (µm) | 295.38 ± 41.95 | 291.80 ± 41.56 | 294.86 ± 40.2 | 291.64 ± 40.36 | 0.012 1 0.032 2 0.224 3 |
| RST position 12 (µm) | 334.86 ± 37.75 | 325.33 ± 39.20 | 326.99 ± 39.32 | 323.99 ± 39.32 | <0.001 1 0.283 2 0.052 3 |
| RST position 6 (µm) | 335.17 ± 37.55 | 328.24 ± 39.01 | 330.05 ± 38.28 | 329.45 ± 38.67 | <0.001 1 0.184 2 0.660 3 |
| RST position 3 (µm) | 320.80 ± 40.21 | 315.42 ± 39.05 | 319.13 ± 38.06 | 318.80 ± 39.85 | <0.0011 <0.01 2 <0.816 3 |
| RST position 9 (µm) | 334.44 ± 38.02 | 330.99 ± 39.72 | 330.29 ± 39.75 | 327.82 ± 40.54 | 0.001 1 0.607 2 0.072 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janiszewska-Bil, D.; Czarnota-Nowakowska, B.; Kuciel-Polczak, I.; Dobrowolski, D.; Grabarek, B.O.; Lyssek-Boroń, A.; Wylęgała, E.; Wierzbowska, J. Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction. J. Clin. Med. 2024, 13, 2148. https://doi.org/10.3390/jcm13072148
Janiszewska-Bil D, Czarnota-Nowakowska B, Kuciel-Polczak I, Dobrowolski D, Grabarek BO, Lyssek-Boroń A, Wylęgała E, Wierzbowska J. Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction. Journal of Clinical Medicine. 2024; 13(7):2148. https://doi.org/10.3390/jcm13072148
Chicago/Turabian StyleJaniszewska-Bil, Dominika, Barbara Czarnota-Nowakowska, Izabela Kuciel-Polczak, Dariusz Dobrowolski, Beniamin Oskar Grabarek, Anita Lyssek-Boroń, Edward Wylęgała, and Joanna Wierzbowska. 2024. "Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction" Journal of Clinical Medicine 13, no. 7: 2148. https://doi.org/10.3390/jcm13072148
APA StyleJaniszewska-Bil, D., Czarnota-Nowakowska, B., Kuciel-Polczak, I., Dobrowolski, D., Grabarek, B. O., Lyssek-Boroń, A., Wylęgała, E., & Wierzbowska, J. (2024). Assessment of Changes in Cap and Residual Stromal Thickness Values during a 6-Month Observation after Refractive Lenticule Extraction Small Incision Lenticule Extraction. Journal of Clinical Medicine, 13(7), 2148. https://doi.org/10.3390/jcm13072148