

Efficacy of Trimetazidine in the Prevention of Contrast-Induced Nephropathy in Patients Undergoing Contrast Coronary Intervention: A Systematic Review and Meta-Analysis (PRISMA)



Abstract
1. Introduction
2. Materials and Methods
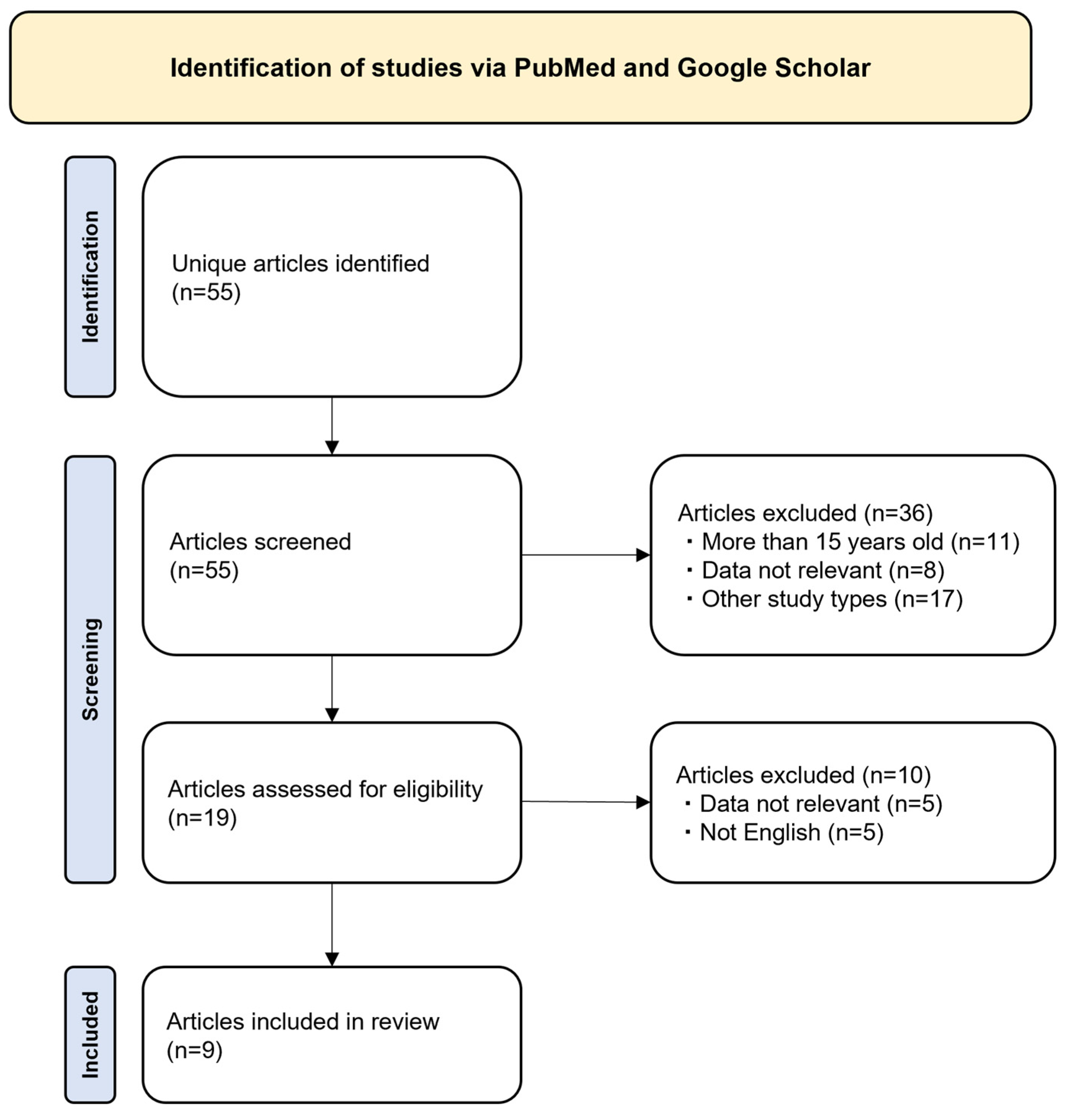
2.1. Search Strategy
- Patient (P)—Patients undergoing Cardiac Intervention (CAG, PCI, or coronary artery bypass graft [CABG]);
- Interventions (I)—Administration of trimetazidine; peri-procedure;
- Comparator (C)—Not restrictive; included placebo, only hydration, or active comparator;
- Outcomes (O)—Incidence of CIN (an increase in SCr of ≥25% or ≥44 μmol/L within 3 days after administration of contrast media, in the absence of an alternative etiology [5];
- Time Frame (T)—15 years;
- and Study type (S)—Only clinical trials.
- The literature search was performed in March 2023 and updated on 7 December 2023.
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Patient Characteristics
3.4. Efficacy Results
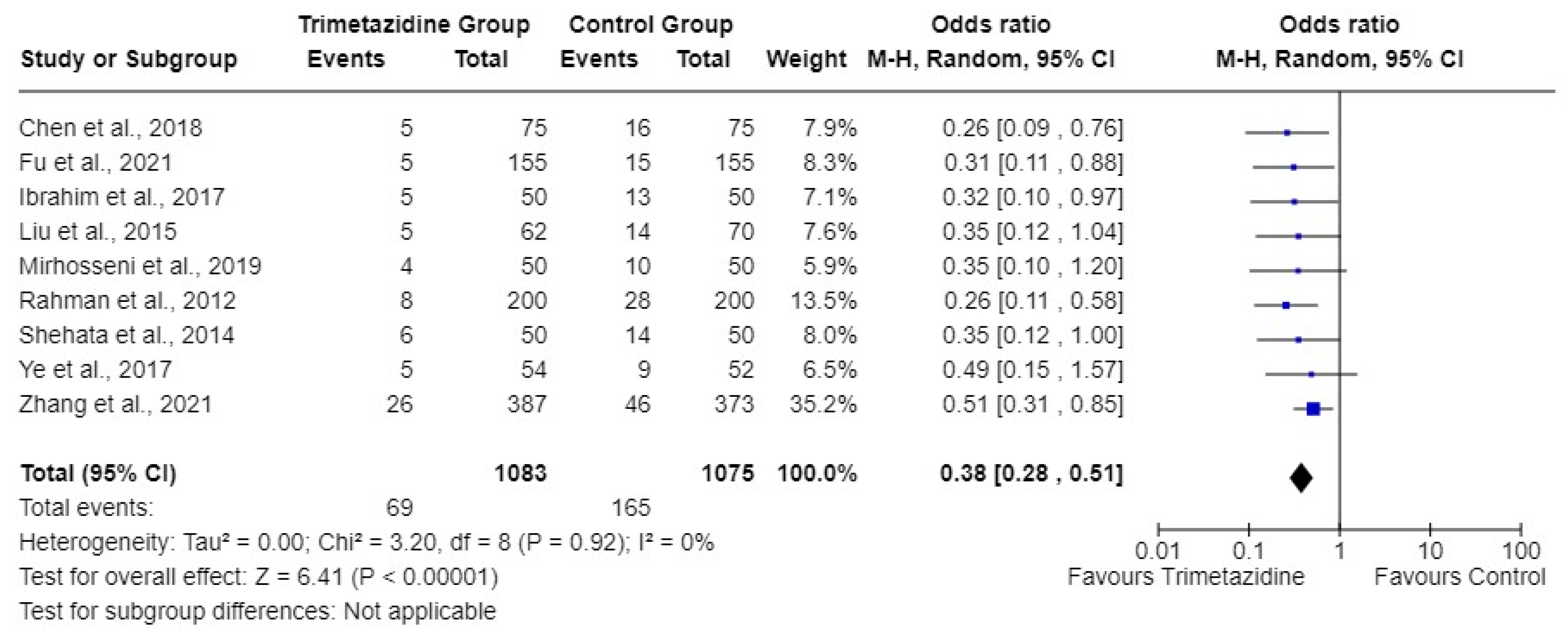
3.4.1. Overall Efficacy
3.4.2. Subgroup Analyses
3.5. Safety Results
3.6. Assessment of Included Articles
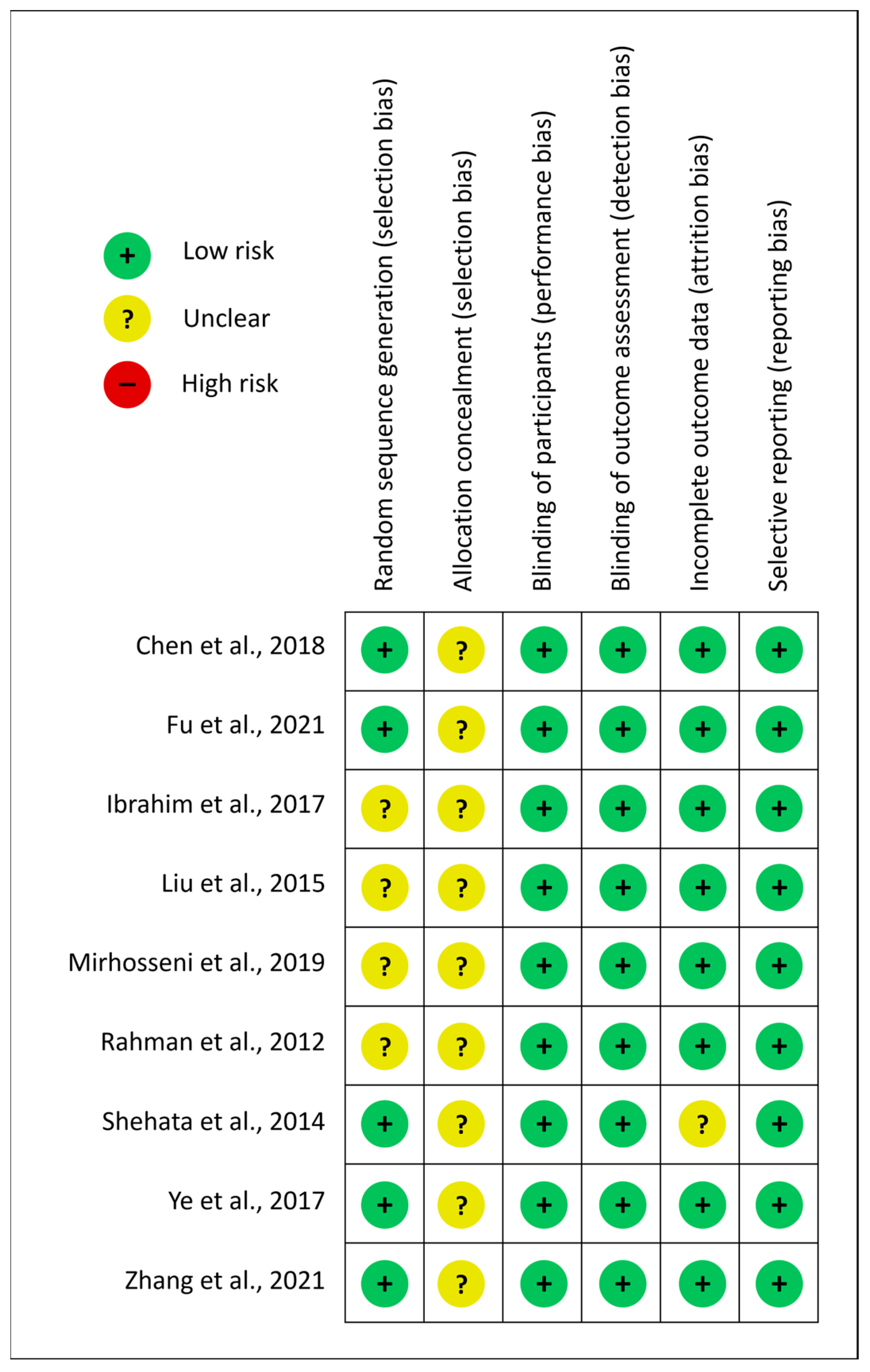
3.6.1. Risk of Bias
3.6.2. Heterogeneity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, M.Y.; Lo, W.C.; Wu, Y.C.; Lin, T.C.; Lin, C.H.; Wu, M.S.; Tu, Y.K. The Incidence of Contrast-Induced Nephropathy and the Need of Dialysis in Patients Receiving Angiography: A Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 862534. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, H.A.; Amoozgar, B.; Jain, S.; Velasco, N.; Zahid, U.; Abbasi, H.; Alasadi, L.; Prince, M.R. Trimetazidine reduces contrast-induced nephropathy in patients with renal insufficiency undergoing coronary angiography and angioplasty: A systematic review and meta-analysis (PRISMA). Medicine 2021, 100, e24603. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Chen, X.R.; Chen, Y.Q.; Niu, T.S.; Liao, Y.M. Prevalence and Predictors of Contrast-Induced Nephropathy (CIN) in Patients with ST-Segment Elevation Myocardial Infarction (STEMI) Undergoing Percutaneous Coronary Intervention (PCI): A Meta-Analysis. J. Interv. Cardiol. 2019, 2019, 2750173. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, P.; Yang, S.; Li, W.; Men, X.; Fu, N. Preventive effect of trimetazidine on contrast-induced nephropathy undergoing percutaneous coronary intervention in elderly moderate and high-risk diabetics stratified by mehran score. Perfusion 2021, 36, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Stacul, F.; Van der Molen, A.; Reimer, P.; Webb, J.A.W.; Thomsen, H.S.; Morcos, S.K.; Lmen, T.; Aspelin, P.; Bellin, M.F.; Clement, O.; et al. Contrast induced nephropathy: Updated ESUR contrast media safety committee guidelines. Eur. Radiol. 2011, 21, 2527–2541. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Liu, F.; Lu, J.; Yang, X.; Xiao, B.; Jin, Y.; Zhang, J. Coenzyme Q10 combined with trimetazidine in the prevention of contrast-induced nephropathy in patients with coronary heart disease complicated with renal dysfunction undergoing elective cardiac catheterization: A randomized control study and in vivo study. Eur. J. Med. Res. 2018, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.; Ricottini, E.; Nusca, A.; Colonna, G.; Pasceri, V.; D’Ambrosio, A.; Montinaro, A.; Di Sciascio, G. Short-term, high-dose Atorvastatin pretreatment to prevent contrast-induced nephropathy in patients with acute coronary syndromes undergoing percutaneous coronary intervention (from the ARMYDA-CIN [atorvastatin for reduction of myocardial damage during angioplasty--contrast-induced nephropathy] trial. Am. J. Cardiol. 2011, 108, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Marzilli, M.; Vinereanu, D.; Lopaschuk, G.; Chen, Y.; Dalal, J.J.; Danchin, N.; Etriby, E.; Ferrari, R.; Gowdak, L.H.; Lopatin, Y.; et al. Trimetazidine in cardiovascular medicine. Int. J. Cardiol. 2019, 293, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Zhang, J.; Zhang, H.; Zhang, P.; Fu, X.; Zeng, Z.; Zhang, X.; Li, W.; Yang, S.; Liu, X.; et al. Trimetazidine can prevent the occurrence of contrast-induced nephropathy after percutaneous coronary intervention in elderly patients with renal insufficiency. Perfusion 2021, 36, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Haque, S.S.; Rokeya, B.; Siddique, M.A.; Banerjee, S.K.; Ahsan, S.A.; Rahman, F.; Mahmood, M.; Ahmed, K.; Bhuiyan, M.M.; et al. Trimetazidine in the prevention of contrast induced nephropathy after coronary angiogram. Mymensingh Med. J. 2012, 21, 292–299. [Google Scholar] [PubMed]
- Liu, W.; Ming, Q.; Shen, J.; Wei, Y.; Li, W.; Chen, W.; Xu, Y. Trimetazidine Prevention of Contrast-Induced Nephropathy in Coronary Angiography. Am. J. Med. Sci. 2015, 350, 398–402. [Google Scholar] [CrossRef]
- Mirhosseni, A.; Farahani, B.; Gandomi-Mohammadabadi, A.; Keyvani, H.; Biglari-Abhari, M.; Davari, A.; Vazirizade-Mahabadi, M.H.; Savaj, S. Preventive Effect of Trimetazidine on Contrast-Induced Acute Kidney Injury in CKD Patients Based on Urinary Neutrophil Gelatinase-associated Lipocalin (uNGAL): A randomized Clinical Trial. Iran J. Kidney Dis. 2019, 13, 191–197. [Google Scholar] [PubMed]
- Shehata, M. Impact of trimetazidine on incidence of myocardial injury and contrast-induced nephropathy in diabetic patients with renal dysfunction undergoing elective percutaneous coronary intervention. Am. J. Cardiol. 2014, 114, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, T.A.; El-Mawardy, R.H.; El-Serafy, A.S.; El-Fekky, E.M. Trimetazidine in the prevention of contrast-induced nephropathy in chronic kidney disease. Cardiovasc. Revasc. Med. 2017, 18, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Lu, H.; Su, Q.; Xian, X.; Li, L. Effect of trimetazidine on preventing contrast-induced nephropathy in diabetic patients with renal insufficiency. Oncotarget 2017, 8, 102521–102530. [Google Scholar] [CrossRef] [PubMed]
- Geenen, R.W.F.; Kingma, H.J.; van der Molen, A.J. Contrast-induced nephropathy: Pharmacology, pathophysiology and prevention. Insights Imaging 2013, 4, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Onbasili, A.O.; Yeniceriglu, Y.; Agaoglu, P.; Karul, A.; Tekten, T.; Akar, H.; Discigil, G. Trimetazidine in the prevention of contrast-induced nephropathy after coronary procedures. Heart 2007, 93, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.; Pande, A.; Chakraborty, S.; Dutta, R.; Tarafdar, A. Trimetazidine in the prevention of contrast induced nephropathy following coronary angiography/angioplasty. Indian Heart J. 2015, 67, s49–s71. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sr No | Author | Study Design | Geography | Trimetazidine Dose | Population Characteristics, Specific Inclusion Criteria | Procedure Performed | Type of Contrast | Sample Size | |
|---|---|---|---|---|---|---|---|---|---|
| Control | Trimetazidine | ||||||||
| 1 | Chen et al., 2018 [6] | RCT, Double Blind paralleled | China | 20 mg, TDS for 48 h pre and 72 h post-procedure | Renal Insufficiency | CAG/PCI | Iopromide | 75 | 75 |
| 2 | Fu et al., 2021 [9] | RCT | China | 20 mg, TDS for 24 h pre and 72 h post procedure | Renal Insufficiency | PCI | Iopromide /Iodixanol | 155 | 155 |
| 3 | Ibrahim et al., 2017 [14] | RCT | Egypt | 35 mg, BD for 48 h pre and 24 h post procedure | Renal Insufficiency | CAG | NA | 50 | 50 |
| 4 | Liu et al., 2015 [11] | RCT | China | 20 mg, TDS for 48 h pre and 24 h post procedure | Renal Insufficiency | CAG/PCI | Iodixanol | 70 | 62 |
| 5 | Mirhosseni et al., 2019 [12] | RCT | Iran | 35 mg, BD for 48 h pre and 24 h post procedure | Renal Insufficiency | CAG | NA | 50 | 50 |
| 6 | Rahman et al., 2012 [10] | RCT | Bangladesh | 35 mg, BD for 96 h starting at a 48 h pre procedure | General | CAG | Iopamidol | 200 | 200 |
| 7 | Shehata et al., 2014 [13] | RCT, Double blind | Egypt | 35 mg, BD for 72 h starting at a 48 h pre procedure | Mild CKD + Diabetes | PCI | Iopromide | 50 | 50 |
| 8 | Ye et al., 2017 [15] | RCT | China | 20 mg, TDS for 48 h pre and 24 h post procedure | Diabetes + Renal insufficiency | CAG/PCI | Iodixanol | 52 | 54 |
| 9 | Zhang et al., 2021 [4] | RCT | China | 35 mg, BD for 24 h pre and 72 h post procedure | Diabetes | PCI | Iodixanol | 373 | 387 |
| Sr No | Author | Sample Size, N | Mean Age, Years | Male,
n (%) | Mean LVEF, % | Mean Serum Creatinine (Trimetazidine vs. Control), μmol/L | Diabetes,
n (%) | Hypertension,
n (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | Chen et al., 2018 [6] | 150 | 62 | 83 (55) | 55 | NA | 65 (43) | 67 (45) |
| 2 | Fu et al., 2021 [9] | 310 | 77 | 152 (49) | NA | 101.27 vs. 100.94 | 141 (45) | 177 (57) |
| 3 | Ibrahim et al., 2017 [14] | 100 | 64 | 57 (57) | 52 | 137.94 vs. 138.82 | 57 (57) | 64 (64) |
| 4 | Liu et al., 2015 [11] | 132 | 59 | 75 (57) | NA | 107.74 vs. 103.38 | 80 (61) | 72 (55) |
| 5 | Mirhosseni et al., 2019 [12] | 100 | 66 | 44 (44) | 51 | 112.27 vs. 114.04 | 62 (62) | 63 (63) |
| 6 | Rahman et al., 2012 [10] | 400 | 56 | 336 (84) | NA | 122.88 vs. 123.76 | NA | 316 (79) |
| 7 | Shehata et al., 2014 [13] | 100 | 59 | 68 (68) | 54 | 176.80 vs. 176.80 | 100 (100) | 48 (48) |
| 8 | Ye et al., 2017 [15] | 106 | 64 | 63 (59) | NA | NA | 106 (100) | 75 (71) |
| 9 | Zhang et al., 2021 [4] | 760 | 66 | 527 (69) | 60 | † | 760 (100) | 300 (39) |
| Overall | 2158 | - | 1405 (65) | - | - | 1371 (64) | 1182 (55) |
| Sr No | Author | Trimetazidine Group | Control Group | Bivariate OR (Calculated) | Multivariate OR (From Publication) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | N | % Incidence | Yes | No | N | % Incidence | Bivariate OR (95% CI) | p-Value | Bivariate OR (95% CI) | p-Value | ||
| 1 | Chen et al., 2018 [6] | 5 | 70 | 75 | 6.7 | 16 | 59 | 75 | 21.3 | 0.2634 (0.091–0.762) | 0.017 | 0.252 (0.082–0.774) | 0.016 |
| 2 | Fu et al., 2021 [9] | 5 | 150 | 155 | 3.2 | 15 | 140 | 155 | 9.7 | 0.3111 (0.1102–0.8785) | 0.035 | 0.274 (0.089–0.847) | 0.025 |
| 3 | Ibrahim et al., 2017 [14] | 5 | 45 | 50 | 10 | 13 | 37 | 50 | 26 | 0.3162 (0.1032–0.9686) | 0.0373 | NA | NA |
| 4 | Liu et al., 2015 [11] | 5 | 57 | 62 | 8.1 | 14 | 56 | 70 | 20 | 0.3509 (0.1185–1.0391) | 0.080 | NA | NA |
| 5 | Mirhosseni et al., 2019 [12] | 4 | 46 | 50 | 8.0 | 10 | 40 | 50 | 20 | 0.3478 (0.1012–1.1954) | 0.148 | NA | NA |
| 6 | Rahman et al., 2012 [10] | 8 | 192 | 200 | 4.0 | 28 | 172 | 200 | 14 | 0.256 (0.1136–0.5767) | 0.0007 | NA | NA |
| 7 | Shehata et al., 2014 [13] | 6 | 44 | 50 | 12.0 | 14 | 36 | 50 | 28 | 0.3506 (0.1223–1.005) | 0.078 | NA | NA |
| 8 | Ye et al., 2017 [15] | 5 | 49 | 54 | 9.3 | 9 | 43 | 52 | 16.7 | 0.4875 (0.1517–1.5668) | 0.2608 | NA | NA |
| 9 | Zhang et al., 2021 [4] | 26 | 361 | 387 | 6.7 | 46 | 327 | 373 | 12.3 | 0.512 (0.3094–0.8472) | 0.009 | 0.294 (0.094–0.920) | 0.035 |
| Overall | 69 | 1014 | 1083 | 6.4 | 165 | 910 | 1075 | 15.4 | 0.3753 (0.2794–0.504) | <0.0001 | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nair, T.; Ray, S.; George, J.; Pande, A. Efficacy of Trimetazidine in the Prevention of Contrast-Induced Nephropathy in Patients Undergoing Contrast Coronary Intervention: A Systematic Review and Meta-Analysis (PRISMA). J. Clin. Med. 2024, 13, 2151. https://doi.org/10.3390/jcm13072151
Nair T, Ray S, George J, Pande A. Efficacy of Trimetazidine in the Prevention of Contrast-Induced Nephropathy in Patients Undergoing Contrast Coronary Intervention: A Systematic Review and Meta-Analysis (PRISMA). Journal of Clinical Medicine. 2024; 13(7):2151. https://doi.org/10.3390/jcm13072151
Chicago/Turabian StyleNair, Tiny, Saumitra Ray, Jacob George, and Arindam Pande. 2024. "Efficacy of Trimetazidine in the Prevention of Contrast-Induced Nephropathy in Patients Undergoing Contrast Coronary Intervention: A Systematic Review and Meta-Analysis (PRISMA)" Journal of Clinical Medicine 13, no. 7: 2151. https://doi.org/10.3390/jcm13072151
APA StyleNair, T., Ray, S., George, J., & Pande, A. (2024). Efficacy of Trimetazidine in the Prevention of Contrast-Induced Nephropathy in Patients Undergoing Contrast Coronary Intervention: A Systematic Review and Meta-Analysis (PRISMA). Journal of Clinical Medicine, 13(7), 2151. https://doi.org/10.3390/jcm13072151