
Oncologic Outcomes of Salvage Abdominoperineal Resection for Anal Squamous Cell Carcinoma Initially Managed with Chemoradiation
 , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. Treatment
2.3. Statistical Analysis
3. Results
3.1. Patients and Tumor Characteristics
3.2. Surgical Technique and Complications
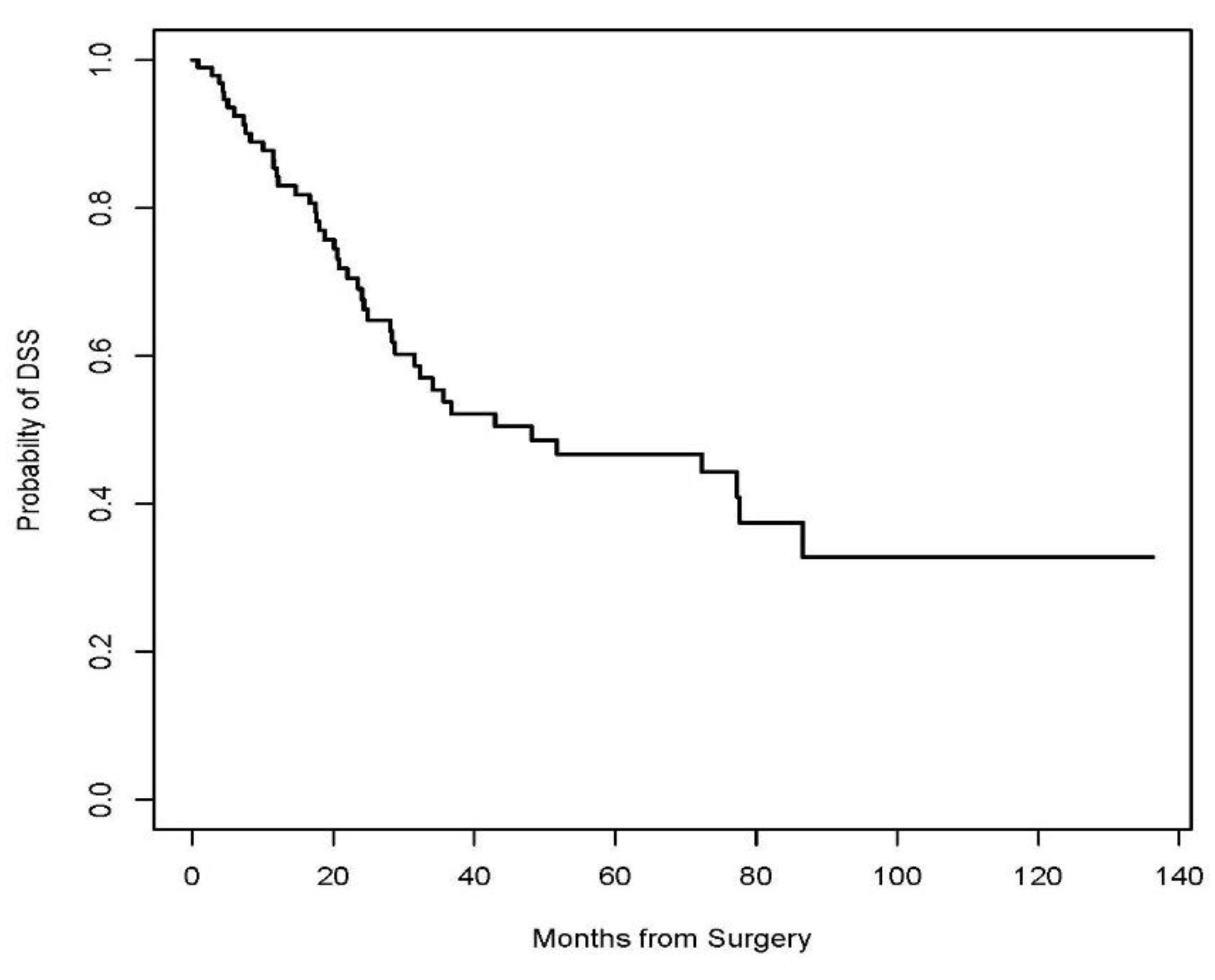
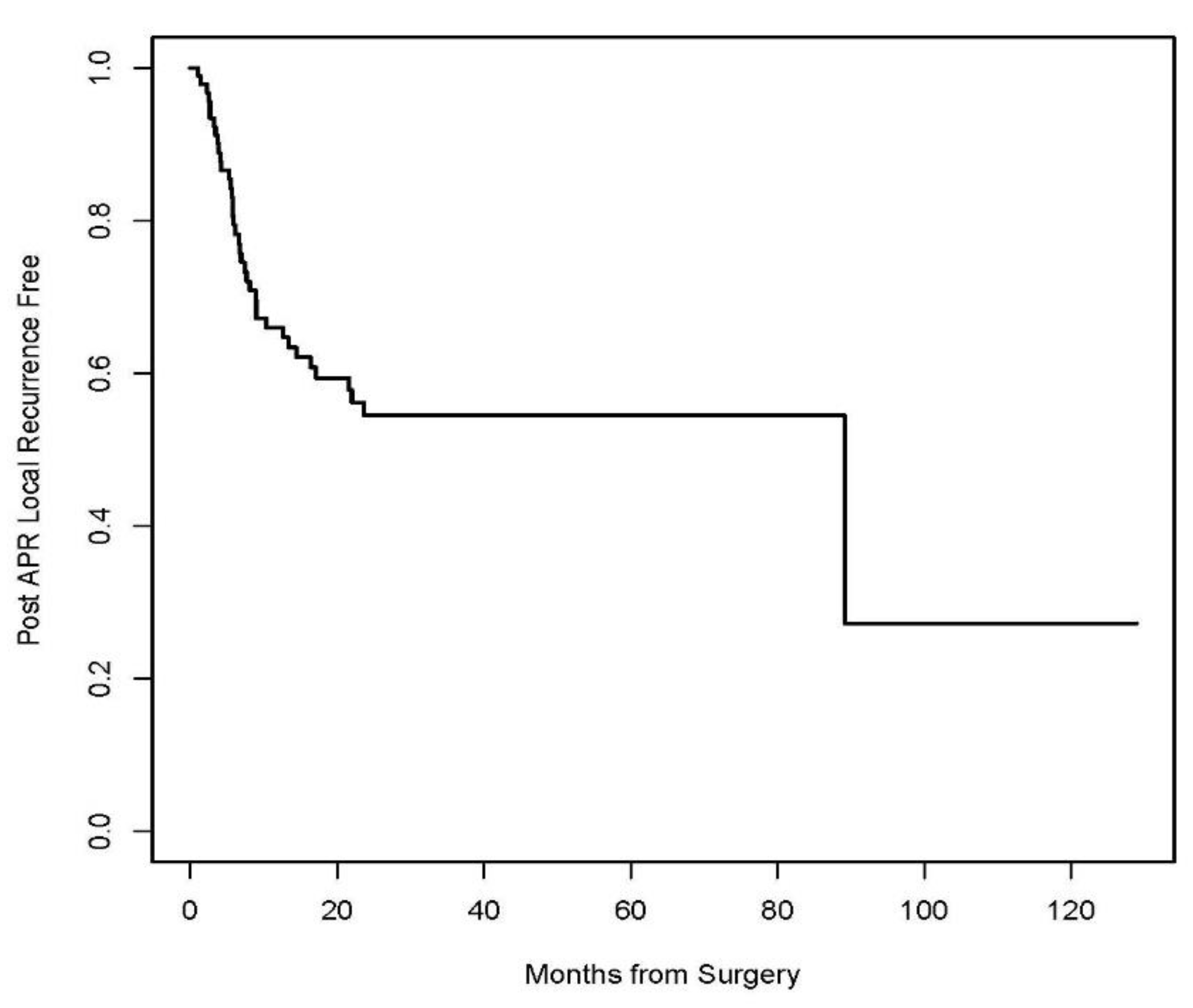
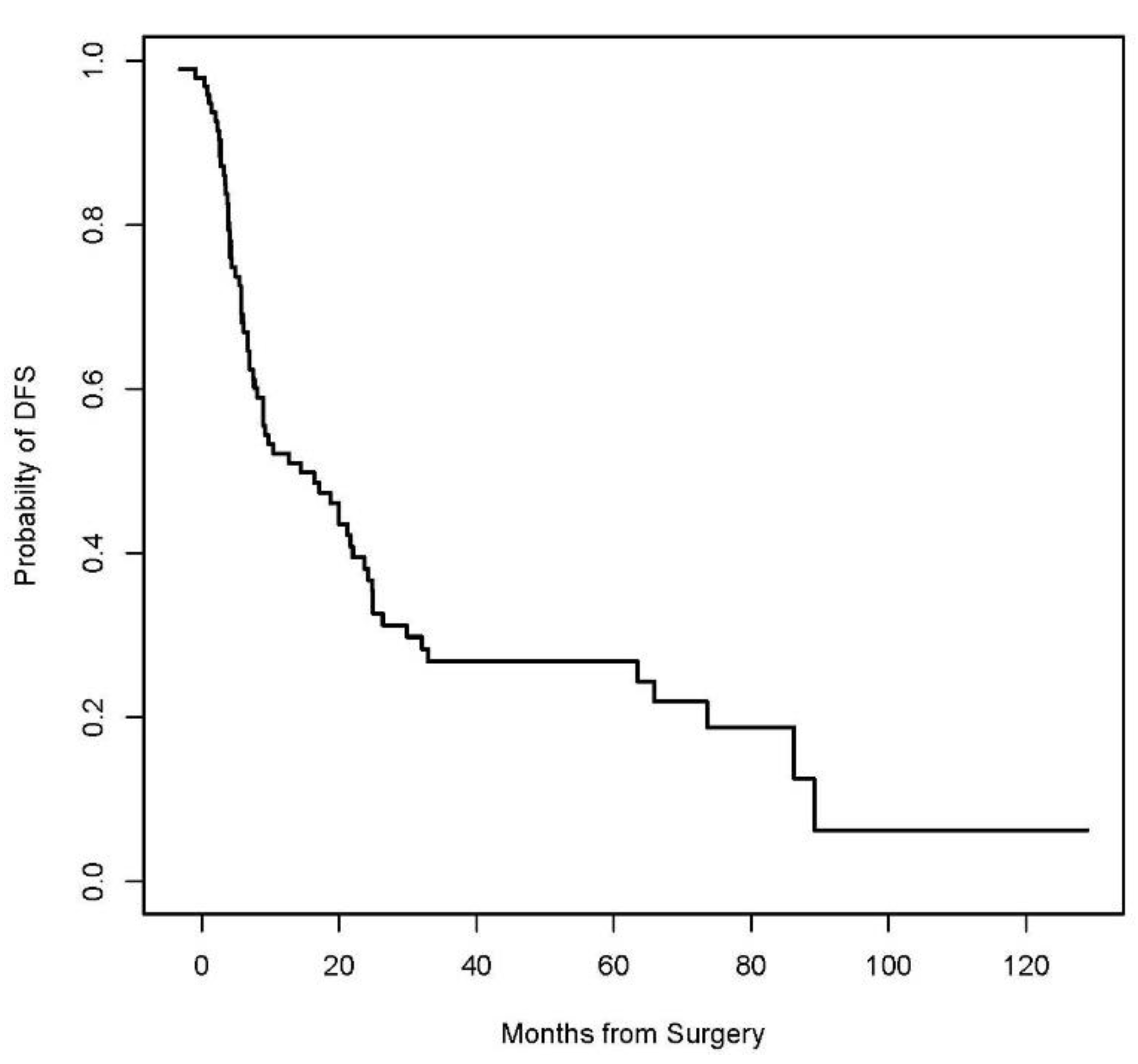
3.3. Disease-Specific, Recurrence-Free, and Disease-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- UKCCCR Anal Cancer Trial Working Party. Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 1996, 348, 1049–1054. [Google Scholar] [CrossRef]
- Bartelink, H.; Roelofsen, F.; Eschwege, F.; Rougier, P.; Bosset, J.F.; Gonzalez, D.G.; Peiffert, D.; van Glabbeke, M.; Pierart, M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1997, 15, 2040–2049. [Google Scholar] [CrossRef]
- Flam, M.; John, M.; Pajak, T.F.; Petrelli, N.; Myerson, R.; Doggett, S.; Quivey, J.; Rotman, M.; Kerman, H.; Coia, L.; et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: Results of a phase III randomized intergroup study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1996, 14, 2527–2539. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, L.L.; Winter, K.A.; Ajani, J.A.; Pedersen, J.E.; Moughan, J.; Benson, A.B., 3rd; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 4344–4351. [Google Scholar] [CrossRef] [PubMed]
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.; Sarkaria, A.; Merchant, S.J.; Booth, C.M.; Patel, S.V. A systematic review of outcomes after salvage abdominoperineal resection for persistent or recurrent anal squamous cell cancer. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2019, 21, 632–650. [Google Scholar] [CrossRef]
- Park, I.J.; Chang, G. Survival and Operative Outcomes After Salvage Surgery for Recurrent or Persistent Anal Cancer. Ann. Coloproctol. 2020, 36, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001–2015. J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Northover, J.M.; Cervantes, A.; ESMO Guidelines Working Group. Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2010, 21 (Suppl. 5), v87–v92. [Google Scholar] [CrossRef]
- van der Wal, B.C.; Cleffken, B.I.; Gulec, B.; Kaufman, H.S.; Choti, M.A. Results of salvage abdominoperineal resection for recurrent anal carcinoma following combined chemoradiation therapy. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2001, 5, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Papaconstantinou, H.T.; Bullard, K.M.; Rothenberger, D.A.; Madoff, R.D. Salvage abdominoperineal resection after failed Nigro protocol: Modest success, major morbidity. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2006, 8, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Hagemans, J.A.W.; Blinde, S.E.; Nuyttens, J.J.; Morshuis, W.G.; Mureau, M.A.M.; Rothbarth, J.; Verhoef, C.; Burger, J.W.A. Salvage Abdominoperineal Resection for Squamous Cell Anal Cancer: A 30-Year Single-Institution Experience. Ann. Surg. Oncol. 2018, 25, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.V.; Ko, G.; Raphael, M.J.; Booth, C.M.; Brogly, S.B.; Kalyvas, M.; Li, W.; Hanna, T. Salvage Abdominoperineal Resection for Anal Squamous Cell Carcinoma: Use, Risk Factors, and Outcomes in a Canadian Population. Dis. Colon Rectum 2020, 63, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; Whelan, P.; Cummings, B.J.; Stern, H.S. Management of persistent or locally recurrent epidermoid cancer of the anal canal with abdominoperineal resection. Acta Oncol. 2001, 40, 34–36. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Alamri, Y.; Buchwald, P.; Dixon, L.; Dobbs, B.; Eglinton, T.; McCormick, J.; Wakeman, C.; Frizelle, F.A. Salvage surgery in patients with recurrent or residual squamous cell carcinoma of the anus. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2016, 42, 1687–1692. [Google Scholar] [CrossRef] [PubMed]
- Allal, A.S.; Laurencet, F.M.; Reymond, M.A.; Kurtz, J.M.; Marti, M.C. Effectiveness of surgical salvage therapy for patients with locally uncontrolled anal carcinoma after sphincter-conserving treatment. Cancer 1999, 86, 405–409. [Google Scholar] [CrossRef]
- Brown, K.G.M.; Solomon, M.J.; Steffens, D.; Ng, K.S.; Byrne, C.M.; Austin, K.K.S.; Lee, P.J. Pelvic Exenteration for Squamous Cell Carcinoma of the Anus: Oncological, Morbidity, and Quality-of-Life Outcomes. Dis. Colon Rectum 2023, 66, 1427–1434. [Google Scholar] [CrossRef]
- Ferenschild, F.T.; Vermaas, M.; Hofer, S.O.; Verhoef, C.; Eggermont, A.M.; de Wilt, J.H. Salvage abdominoperineal resection and perineal wound healing in local recurrent or persistent anal cancer. World J. Surg. 2005, 29, 1452–1457. [Google Scholar] [CrossRef]
- Guerra, G.R.; Kong, J.C.; Bernardi, M.P.; Ramsay, R.G.; Phillips, W.A.; Warrier, S.K.; Lynch, A.C.; Ngan, S.Y.; Heriot, A.G. Salvage Surgery for Locoregional Failure in Anal Squamous Cell Carcinoma. Dis. Colon Rectum 2018, 61, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lefèvre, J.H.; Corte, H.; Tiret, E.; Boccara, D.; Chaouat, M.; Touboul, E.; Svrcek, M.; Lefrancois, M.; Shields, C.; Parc, Y. Abdominoperineal resection for squamous cell anal carcinoma: Survival and risk factors for recurrence. Ann. Surg. Oncol. 2012, 19, 4186–4192. [Google Scholar] [CrossRef] [PubMed]
- Mullen, J.T.; Rodriguez-Bigas, M.A.; Chang, G.J.; Barcenas, C.H.; Crane, C.H.; Skibber, J.M.; Feig, B.W. Results of surgical salvage after failed chemoradiation therapy for epidermoid carcinoma of the anal canal. Ann. Surg. Oncol. 2007, 14, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Schiller, D.E.; Cummings, B.J.; Rai, S.; Le, L.W.; Last, L.; Davey, P.; Easson, A.; Smith, A.J.; Swallow, C.J. Outcomes of salvage surgery for squamous cell carcinoma of the anal canal. Ann. Surg. Oncol. 2007, 14, 2780–2789. [Google Scholar] [CrossRef] [PubMed]
- Ellenhorn, J.D.; Enker, W.E.; Quan, S.H. Salvage abdominoperineal resection following combined chemotherapy and radiotherapy for epidermoid carcinoma of the anus. Ann. Surg. Oncol. 1994, 1, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Beal, K.P.; Wong, D.; Guillem, J.G.; Paty, P.B.; Saltz, L.L.; Wagman, R.; Minsky, B.D. Primary adenocarcinoma of the anus treated with combined modality therapy. Dis. Colon Rectum 2003, 46, 1320–1324. [Google Scholar] [CrossRef]
- Wright, J.L.; Gollub, M.J.; Weiser, M.R.; Saltz, L.B.; Wong, W.D.; Paty, P.B.; Temple, L.K.; Guillem, J.G.; Minsky, B.D.; Goodman, K.A. Surgery and high-dose-rate intraoperative radiation therapy for recurrent squamous-cell carcinoma of the anal canal. Dis. Colon Rectum 2011, 54, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Chessin, D.B.; Hartley, J.; Cohen, A.M.; Mazumdar, M.; Cordeiro, P.; Disa, J.; Mehrara, B.; Minsky, B.D.; Paty, P.; Weiser, M.; et al. Rectus flap reconstruction decreases perineal wound complications after pelvic chemoradiation and surgery: A cohort study. Ann. Surg. Oncol. 2005, 12, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Kitaguchi, D.; Tsukada, Y.; Ito, M.; Horasawa, S.; Bando, H.; Yoshino, T.; Yamada, K.; Ajioka, Y.; Sugihara, K. Survival outcomes following salvage abdominoperineal resection for recurrent and persistent anal squamous cell carcinoma. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2023, 49, 106929. [Google Scholar] [CrossRef]
- Severino, N.P.; Chadi, S.A.; Rosen, L.; Coiro, S.; Choman, E.; Berho, M.; Wexner, S.D. Survival following salvage abdominoperineal resection for persistent and recurrent squamous cell carcinoma of the anus: Do these disease categories affect survival? Color. Dis. 2016, 18, 959–966. [Google Scholar] [CrossRef]
- Fields, A.C.; Melnitchouk, N.; Senturk, J.; Irani, J.; Bleday, R.; Goldberg, J. Early versus late salvage abdominoperineal resection for anal squamous cell carcinoma: Is there a difference in survival? J. Surg. Oncol. 2019, 120, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Correa, J.H.; Castro, L.S.; Kesley, R.; Dias, J.A.; Jesus, J.P.; Olivatto, L.O.; Martins, I.O.; Lopasso, F.P. Salvage abdominoperineal resection for anal cancer following chemoradiation: A proposed scoring system for predicting postoperative survival. J. Surg. Oncol. 2013, 107, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Winter, K.A.; Gunderson, L.L.; Pedersen, J.; Benson, A.B., 3rd; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; Willett, C. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: A randomized controlled trial. JAMA 2008, 299, 1914–1921. [Google Scholar] [CrossRef] [PubMed]
- John, M.; Pajak, T.; Flam, M.; Hoffman, J.; Markoe, A.; Wolkov, H.; Paris, K. Dose escalation in chemoradiation for anal cancer: Preliminary results of RTOG 92-08. Cancer J. Sci. Am. 1996, 2, 205–211. [Google Scholar]
- Konski, A.; Garcia, M., Jr.; John, M.; Krieg, R.; Pinover, W.; Myerson, R.; Willett, C. Evaluation of planned treatment breaks during radiation therapy for anal cancer: Update of RTOG 92-08. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Peiffert, D.; Tournier-Rangeard, L.; Gérard, J.P.; Lemanski, C.; François, E.; Giovannini, M.; Cvitkovic, F.; Mirabel, X.; Bouché, O.; Luporsi, E.; et al. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: Final analysis of the randomized UNICANCER ACCORD 03 trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1941–1948. [Google Scholar] [CrossRef]
- Hallemeier, C.L.; You, Y.N.; Larson, D.W.; Dozois, E.J.; Nelson, H.; Klein, K.A.; Miller, R.C.; Haddock, M.G. Multimodality therapy including salvage surgical resection and intraoperative radiotherapy for patients with squamous-cell carcinoma of the anus with residual or recurrent disease after primary chemoradiotherapy. Dis. Colon Rectum 2014, 57, 442–448. [Google Scholar] [CrossRef]
- Osborne, M.C.; Maykel, J.; Johnson, E.K.; Steele, S.R. Anal squamous cell carcinoma: An evolution in disease and management. World J. Gastroenterol. 2014, 20, 13052–13059. [Google Scholar] [CrossRef]
- Carr, R.M.; Jin, Z.; Hubbard, J. Research on Anal Squamous Cell Carcinoma: Systemic Therapy Strategies for Anal Cancer. Cancers 2021, 13, 2180. [Google Scholar] [CrossRef]
- Cacheux, W.; Rouleau, E.; Briaux, A.; Tsantoulis, P.; Mariani, P.; Richard-Molard, M.; Buecher, B.; Dangles-Marie, V.; Richon, S.; Lazartigues, J.; et al. Mutational analysis of anal cancers demonstrates frequent PIK3CA mutations associated with poor outcome after salvage abdominoperineal resection. Br. J. Cancer 2016, 114, 1387–1394. [Google Scholar] [CrossRef]
- Cacheux, W.; Dangles-Marie, V.; Rouleau, E.; Lazartigues, J.; Girard, E.; Briaux, A.; Mariani, P.; Richon, S.; Vacher, S.; Buecher, B.; et al. Exome sequencing reveals aberrant signalling pathways as hallmark of treatment-naive anal squamous cell carcinoma. Oncotarget 2018, 9, 464–476. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 96 (%) |
|---|---|
| Median age in years (range) | 63 (33.87) |
| No. (%) male | 39 (40.6) |
| No. (%) HIV a (+) | 17 (17.7) |
| Primary tumor treatment regimen, n (%) | |
| 5-FU/capecitabine + MMC b/cisplatin+ RT | 86 (89.6) |
| 5-FU + RT | 6 (6.2) |
| RT alone | 4 (4.2) |
| Indication for surgery | |
| Persistent | 39 (40.6) |
| Recurrent | 57 (59.4) |
| AJCC c pathological stage, n (%) | |
| 0 | 7 (7.3) |
| is | 1 (1.0) |
| I | 7 (7.7) |
| II | 32 (33.3) |
| III | 49 (51.0) |
| Pathological T classification, n (%) | |
| pT0/Tis | 9 (9.4) |
| pT1 | 7 (7.3) |
| pT2 | 31 (32.3) |
| pT3 | 18 (18.7) |
| pT4 | 31 (32.3) |
| Pathological N classification, n (%) | |
| pN− | 77 (80.2) |
| pN+ | 19 (19.8) |
| Characteristics | N = 96 (%) |
|---|---|
| No. (%) type surgical approach | |
| APR | 43 (44.8) |
| Extended APR a | 44 (45.8) |
| Pelvic Exenteration, posterior b | 5 (5.2) |
| Pelvic Exenteration, Total | 4 (4.2) |
| No. (%) type perineal wound closure | |
| Primary | 15 (15.6) |
| Gluteal Flap | 8 (8.3) |
| Gracilis Flap | 4 (4.2) |
| VRAM | 69 (71.9) |
| No. (%) surgical complications by Clavien–Dindo grade | |
| 1–2 | 8 (8.3) |
| 3–5 | 19 (19.8) |
| No. (%) positive margin resection | 20 (20.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosen, R.; Quezada-Diaz, F.F.; Gönen, M.; Karagkounis, G.; Widmar, M.; Wei, I.H.; Smith, J.J.; Nash, G.M.; Weiser, M.R.; Paty, P.B.; et al. Oncologic Outcomes of Salvage Abdominoperineal Resection for Anal Squamous Cell Carcinoma Initially Managed with Chemoradiation. J. Clin. Med. 2024, 13, 2156. https://doi.org/10.3390/jcm13082156
Rosen R, Quezada-Diaz FF, Gönen M, Karagkounis G, Widmar M, Wei IH, Smith JJ, Nash GM, Weiser MR, Paty PB, et al. Oncologic Outcomes of Salvage Abdominoperineal Resection for Anal Squamous Cell Carcinoma Initially Managed with Chemoradiation. Journal of Clinical Medicine. 2024; 13(8):2156. https://doi.org/10.3390/jcm13082156
Chicago/Turabian StyleRosen, Roni, Felipe F. Quezada-Diaz, Mithat Gönen, Georgios Karagkounis, Maria Widmar, Iris H. Wei, J. Joshua Smith, Garrett M. Nash, Martin R. Weiser, Philip B. Paty, and et al. 2024. "Oncologic Outcomes of Salvage Abdominoperineal Resection for Anal Squamous Cell Carcinoma Initially Managed with Chemoradiation" Journal of Clinical Medicine 13, no. 8: 2156. https://doi.org/10.3390/jcm13082156