
Long-Term Mortality after Transcatheter Edge-to-Edge Mitral Valve Repair Significantly Decreased over the Last Decade: Comparison between Initial and Current Experience from the MiTra Ulm Registry
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcomes and Definitions
2.3. Statistics
3. Results
3.1. Baseline Characteristics
3.2. Echocardiographic and Invasive Hemodynamic Assessment
3.3. Short-Term Outcomes
3.4. Functional Outcomes in the First vs. Current M-TEER Experience
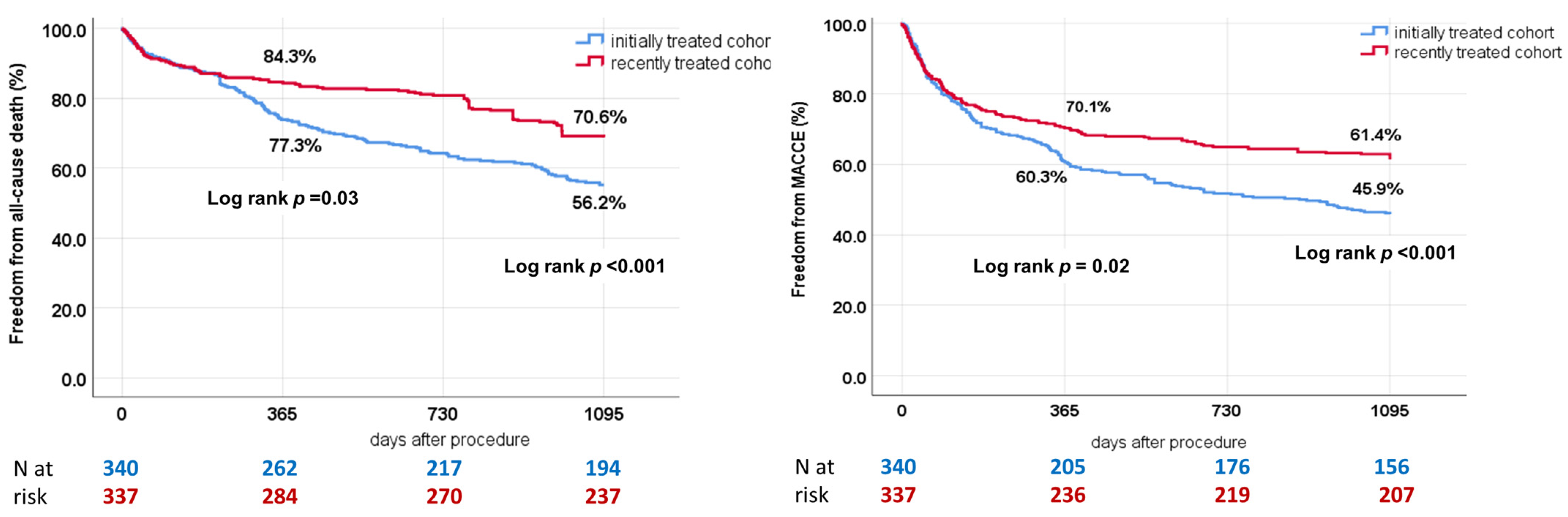
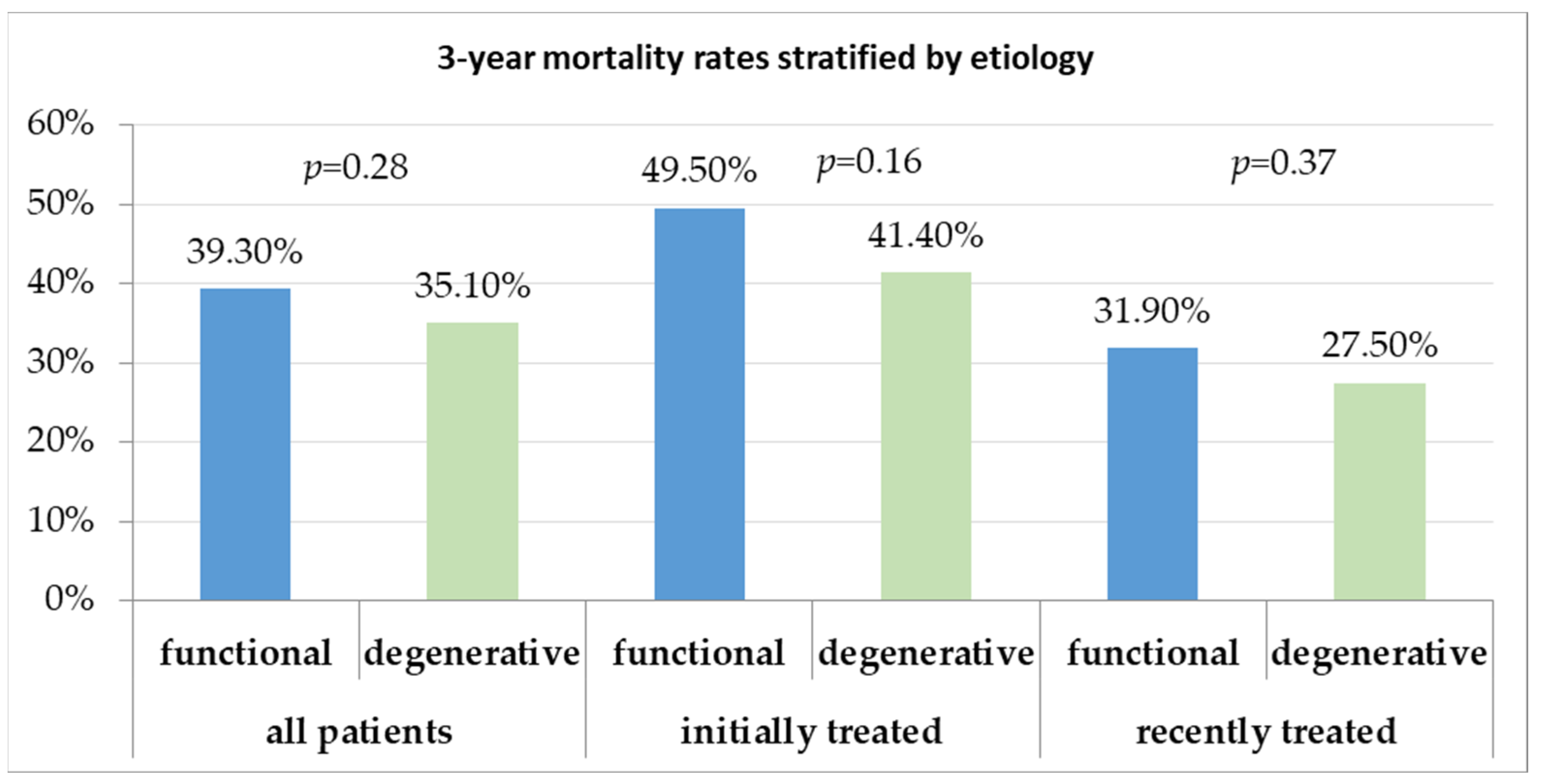
3.5. Trends in Long-Term Follow-Up over the Last Decade
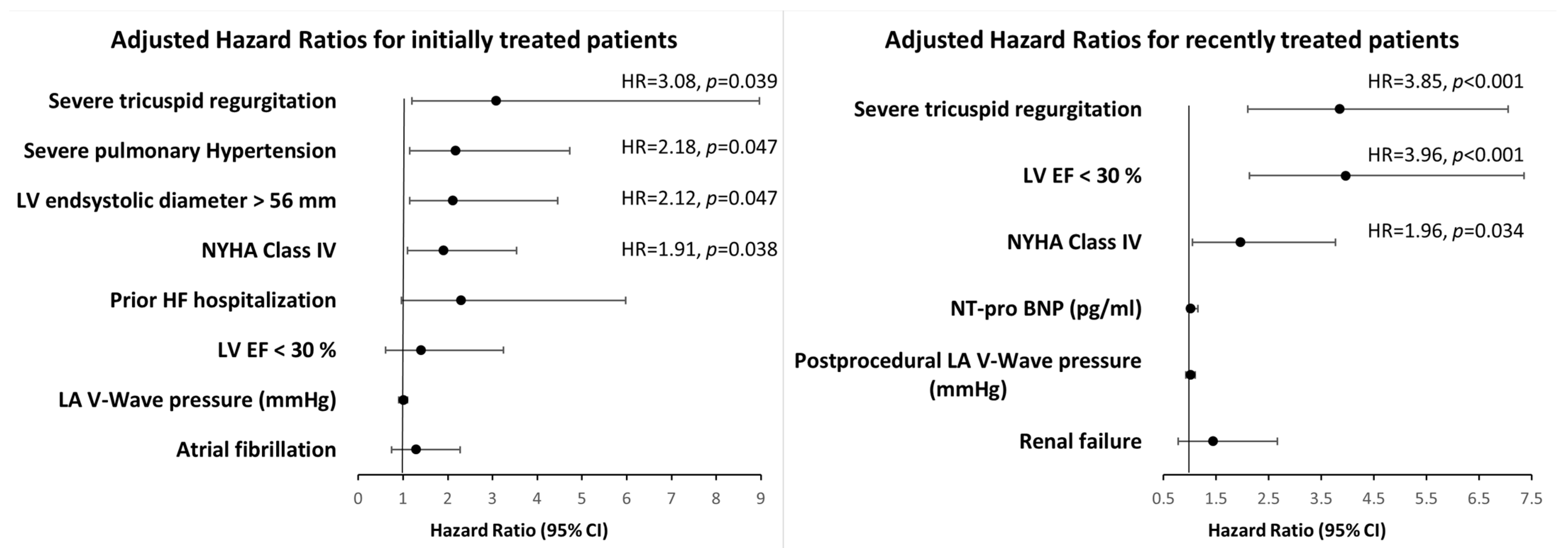
3.6. Predictors of Long-Term Mortality over the Last Decade
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous Repair or Surgery for Mitral Regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Puls, M.; Lubos, E.; Boekstegers, P.; von Bardeleben, R.S.; Ouarrak, T.; Butter, C.; Zuern, C.S.; Bekeredjian, R.; Sievert, H.; Nickenig, G.; et al. One-Year Outcomes and Predictors of Mortality after MitraClip Therapy in Contemporary Clinical Practice: Results from the German Transcatheter Mitral Valve Interventions Registry. Eur. Heart J. 2016, 37, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Baldus, S.; Schillinger, W.; Franzen, O.; Bekeredjian, R.; Sievert, H.; Schofer, J.; Kuck, K.-H.; Konorza, T.; Möllmann, H.; Hehrlein, C.; et al. MitraClip Therapy in Daily Clinical Practice: Initial Results from the German Transcatheter Mitral Valve Interventions (TRAMI) Registry. Eur. J. Heart Fail. 2012, 14, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. EuroIntervention 2022, 17, e1126–e1196. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [PubMed]
- Kalbacher, D.; Schäfer, U.; Bardeleben, R.S.v.; Eggebrecht, H.; Sievert, H.; Nickenig, G.; Butter, C.; May, A.E.; Bekeredjian, R.; Ouarrak, T.; et al. Long-Term Outcome, Survival and Predictors of Mortality after MitraClip Therapy: Results from the German Transcatheter Mitral Valve Interventions (TRAMI) Registry. Int. J. Cardiol. 2019, 277, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.-F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Armoiry, X.; Vahanian, A.; Boutitie, F.; Mewton, N.; Trochu, J.; Lefèvre, T.; Messika-Zeitoun, D.; Guerin, P.; Cormier, B.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation: Outcomes at 2 Years. Eur. J. Heart Fail. 2019, 21, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.K.; Grayburn, P.A.; Rinaldi, M.J.; Kapadia, S.R.; et al. 3-Year Outcomes of Transcatheter Mitral Valve Repair in Patients with Heart Failure. J. Am. Coll. Cardiol. 2021, 77, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Nita, N.; Schneider, L.; Dahme, T.; Markovic, S.; Keßler, M.; Rottbauer, W.; Tadic, M. Trends in Transcatheter Edge-to-Edge Mitral Valve Repair Over a Decade: Data From the MiTra ULM Registry. Front. Cardiovasc. Med. 2022, 9, 850356. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev. Española De Cardiol. (Engl. Ed.) 2018, 71, 110. [Google Scholar] [CrossRef]
- Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 2: Endpoint Definitions: A Consensus Document from the Mitral Valve Academic Research Consortium–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26184623/ (accessed on 22 April 2022).
- Kar, S.; Feldman, T.; Qasim, A.; Trento, A.; Kapadia, S.; Pedersen, W.; Lim, D.S.; Kipperman, R.; Smalling, R.W.; Bajwa, T.; et al. Five-Year Outcomes of Transcatheter Reduction of Significant Mitral Regurgitation in High-Surgical-Risk Patients. Heart 2019, 105, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Orban, M.; Karam, N.; Lubos, E.; Kalbacher, D.; Braun, D.; Deseive, S.; Neuss, M.; Butter, C.; Praz, F.; Kassar, M.; et al. Impact of Proportionality of Secondary Mitral Regurgitation on Outcome After Transcatheter Mitral Valve Repair. JACC Cardiovasc. Imaging 2021, 14, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Maor, E.; Raphael, C.E.; Panaich, S.S.; Reeder, G.S.; Nishimura, R.A.; Nkomo, V.T.; Rihal, C.S.; Eleid, M.F. Acute Changes in Left Atrial Pressure after MitraClip Are Associated with Improvement in 6-Minute Walk Distance. Circ Cardiovasc. Interv. 2017, 10, e004856. [Google Scholar] [CrossRef] [PubMed]
- Predictors of Left Ventricular Reverse Remodeling after Percutaneous Therapy for Mitral Regurgitation with the MitraClip System–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/32104977/ (accessed on 22 April 2022).
- Grayburn, P.A.; Foster, E.; Sangli, C.; Weissman, N.J.; Massaro, J.; Glower, D.G.; Feldman, T.; Mauri, L. Relationship between the Magnitude of Reduction in Mitral Regurgitation Severity and Left Ventricular and Left Atrial Reverse Remodeling after MitraClip Therapy. Circulation 2013, 128, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Grasso, C.; Popolo Rubbio, A.; Capodanno, D.; Buccheri, S.; Di Salvo, M.E.; Cannata, S.; Scandura, S.; Mangiafico, S.; Farruggio, S.; Salerno, T.; et al. Incidence, Timing, Causes and Predictors of Early and Late Re-Hospitalization in Patients Who Underwent Percutaneous Mitral Valve Repair with the MitraClip System. Am. J. Cardiol. 2018, 121, 1253–1259. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 677) | Initially Treated (n = 340) | Recently Treated (n = 337) | p-Value | |
|---|---|---|---|---|
| Age (years) | 76 ± 8 | 76 ± 8 | 76 ± 9 | 0.683 |
| Male (%) | 402 (59.4) | 208 (61.1) | 194 (57.6) | 0.342 |
| Functional MR (%) | 429 (63.3) | 233 (68.4) | 196 (58.2) | 0.004 |
| NYHA class | ||||
| I–II (%) | 99 (14.7) | 47 (13.8) | 52 (15.4) | 0.626 |
| III (%) | 332 (49.0) | 136 (40.0) | 196 (58.2) | <0.001 |
| IV (%) | 246 (36.3) | 157(46.2) | 89 (26.4) | <0.001 |
| Prior heart failure hospitalization | 338 (49.9) | 200 (58.8) | 138 (40.9) | <0.001 |
| Interventions and surgeries | ||||
| PCI (%) | 308 (45.5) | 143(42.1) | 165 (48.9) | 0.060 |
| CABG (%) | 108 (16) | 60 (17.7) | 48 (14.2) | 0.273 |
| Valve surgery (%) | 40 (5.9) | 22 (6.4) | 18 (5.3) | 0.566 |
| Comorbidities | ||||
| Previous MI (%) | 159 (23.5) | 70 (20.6) | 89 (26.4) | 0.103 |
| CAD (%) | 469 (69.3) | 246 (72.5) | 223 (66.1) | 0.064 |
| DCM (%) | 123 (18.2) | 59(17.4) | 64(18.9) | 0.605 |
| Hypertension (%) | 544 (80.4) | 280 (82.3) | 264 (78.3) | 0.185 |
| Diabetes (%) | 192 (28.3) | 112 (33) | 80 (23.7) | 0.177 |
| Atrial fibrillation (%) | 441 (65.1) | 228 (67.1) | 213 (63.2) | 0.273 |
| Peripheral artery disease (%) | 60 (8.9) | 31 (9.4) | 29 (8.6) | 0.676 |
| COPD (%) | 84 (12.4) | 47 (13.7) | 37 (10.9) | 0.299 |
| Chronic renal failure (%) | 365 (53.9) | 190 (56) | 175 (52) | 0.252 |
| Previous cancer (%) | 116 (17.2) | 61 (18) | 55 (16.3) | 0.203 |
| Antiarrhythmia devices | ||||
| CRT (%) | 66 (9.8) | 36 (10.7) | 30 (8.9) | 0.369 |
| ICD (%) | 97 (14.3) | 68 (20) | 29 (8.6) | 0.022 |
| Pacemaker (%) | 62 (9.2) | 36 (9.9) | 26 (8.7) | 0.505 |
| Euro Score II | 8.4 ± 8.2 | 9.6 ± 8.1 | 7.8 ± 8.2 | <0.001 |
| Therapy | ||||
| Loop diuretics (%) | 523 (77.3) | 264 (77.7) | 259 (76.8) | 0.757 |
| ACEI (%) | 319 (47.1) | 173 (51) | 146 (43) | 0.034 |
| ARB (%) | 185 (27.3) | 82 (24.1) | 103 (31) | 0.037 |
| ARNI (%) | 78(11.5) | 8(2.3) | 70 (20.7) | 0.001 |
| Beta-blockers (%) | 586 (86.6) | 292 (86) | 294 (87.2) | 0.501 |
| Aldosterone antagonists (%) | 304 (44.9) | 121 (41) | 183 (54) | 0.032 |
| Laboratory | ||||
| GFR (mL/min/1.73 m2) | 47 ± 19 | 46 ± 18 | 49 ± 20 | 0.137 |
| Troponin T (ng/L) | 87 ± 144 | 139 ± 211 | 43 ± 98 | 0.021 |
| NT-pro-BNP (pg/mL) | 6601 ± 7238 | 7264 ± 7011 | 5995 ± 7398 | 0.001 |
| All (n = 677) | Initially Treated (n = 340) | Recently Treated (n = 337) | p-Value | |
|---|---|---|---|---|
| Echocardiography | ||||
| LVEF (%) | 44 ± 17 | 43 ± 17 | 44 ± 17 | 0.434 |
| LVEDD (mm) | 60 ± 11 | 62 ± 12 | 58 ± 10 | 0.017 |
| LVESD (mm) | 47 ± 15 | 49 ± 16 | 43 ± 13 | 0.007 |
| Interventricular septum thickness (mm) | 11 ± 4.8 | 10.5 ± 2.4 | 11.3 ± 6 | 0.039 |
| LA (mm) | 57 ± 10 | 58 ± 12 | 55 ± 8 | 0.045 |
| sPAP | 59 ± 17 | 62 ± 20 | 57 ± 15 | 0.047 |
| EROA | 0.43 ± 0.35 | 0.48 ± 0.4 | 0.4 ± 0.31 | 0.003 |
| Carpentier Type I | 205(30.1) | 111(32.7) | 94(27.6) | 0.139 |
| Carpentier Type II | 141(20.9) | 67(19.7) | 74(21.7) | 0.553 |
| Carpentier Type IIIa | 109(16.3) | 42(12.3) | 67(20.4) | 0.002 |
| Carpentier Type IIIb | 222(32.7) | 120(35.3) | 102(30.3) | 0.147 |
| Severe TR (grade III/IV) | 253(37.3) | 161(47.3) | 92 (27.3) | <0.001 |
| Catheterization | ||||
| Heart rate (beat/min) | 72 ± 15 | 72 ± 14 | 71 ± 17 | 0.241 |
| Mean RA pressure (mmHg) | 11 ± 7 | 11 ± 6 | 10 ± 7 | 0.102 |
| Mean RV pressure (mmHg) | 26 ± 28 | 32 ± 32 | 13 ± 8 | <0.001 |
| Systolic PA pressure (mmHg) | 55 ± 19 | 57 ± 21 | 50 ± 15 | 0.011 |
| Diastolic PA pressure (mmHg) | 23 ± 14 | 25 ± 15 | 19 ± 8 | 0.041 |
| Mean PA pressure (mmHg) | 34 ± 14 | 35 ± 15 | 32 ± 11 | 0.015 |
| Mean LA pressure (mmHg) | 27± 18 | 28 ± 18 | 22 ± 18 | 0.016 |
| V wave LA pressure | 32± 16 | 37 ± 18 | 30 ± 15 | 0.003 |
| SVR (dynes/seconds/cm−5) | 2019 ± 2201 | 2812 ± 529 | 1996 ± 2227 | 0.009 |
| Cardiac index (L/min/m2) | 2.08 ± 0.55 | 2.06 ± 0.57 | 2.13 ± 0.50 | 0.143 |
| All (n = 677) | Initially Treated (n = 340) | Recently Treated (n = 337) | p-Value | |
|---|---|---|---|---|
| Time after procedure (days) | 6.7 ± 5.6 | 7.69 ± 5.6 | 5.7 ± 5.3 | <0.001 |
| ICU length (days) | 1.0 ± 3.9 | 1.05 ± 3.9 | 0.94 ± 3.9 | <0.001 |
| Fluoroscopy time (min) | 29 ± 17 | 30 ± 17 | 27 ± 17 | <0.001 |
| Number of clips implanted | 1.3 ±0.7 | 1.3 ±0.5 | 1.41 ±0.9 | 0.281 |
| MVARC device success | 635 (93.8) | 317 (93.3) | 318 (94.3) | 0.660 |
| Post-procedural mean LA pressure (mmHg) | 15 ± 6 | 16 ± 6 | 12 ± 4 | <0.001 |
| Post-procedural v wave LA pressure | 22 ± 11 | 24 ± 9 | 19 ± 11 | <0.001 |
| Grade of MR after procedure | 1.5 ± 0.7 | 1.6 ± 0.7 | 1.5 ± 0.6 | 0.093 |
| Transmitral mean gradient after procedure | 3.4 ± 1.90 | 3.4 ± 2.2 | 3.5 ± 1.7 | 0.224 |
| Periprocedural mortality | 21 (3.1) | 10 (2.9) | 11 (3.2) | 0.848 |
| 30-day rehospitalization | 26 (3.9) | 13 (3.8) | 13 (3.9) | 0.920 |
| 30-day all-cause mortality | 27 (4) | 12 (3.5) | 15 (4.5) | 0.470 |
| 30-day MACCE | 51 (7.6) | 27 (8) | 24 (7.1) | 0.703 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nita, N.; Tadic, M.; Mörike, J.; Paukovitsch, M.; Felbel, D.; Keßler, M.; Gröger, M.; Schneider, L.-M.; Rottbauer, W. Long-Term Mortality after Transcatheter Edge-to-Edge Mitral Valve Repair Significantly Decreased over the Last Decade: Comparison between Initial and Current Experience from the MiTra Ulm Registry. J. Clin. Med. 2024, 13, 2172. https://doi.org/10.3390/jcm13082172
Nita N, Tadic M, Mörike J, Paukovitsch M, Felbel D, Keßler M, Gröger M, Schneider L-M, Rottbauer W. Long-Term Mortality after Transcatheter Edge-to-Edge Mitral Valve Repair Significantly Decreased over the Last Decade: Comparison between Initial and Current Experience from the MiTra Ulm Registry. Journal of Clinical Medicine. 2024; 13(8):2172. https://doi.org/10.3390/jcm13082172
Chicago/Turabian StyleNita, Nicoleta, Marijana Tadic, Johannes Mörike, Michael Paukovitsch, Dominik Felbel, Mirjam Keßler, Matthias Gröger, Leonhard-Moritz Schneider, and Wolfgang Rottbauer. 2024. "Long-Term Mortality after Transcatheter Edge-to-Edge Mitral Valve Repair Significantly Decreased over the Last Decade: Comparison between Initial and Current Experience from the MiTra Ulm Registry" Journal of Clinical Medicine 13, no. 8: 2172. https://doi.org/10.3390/jcm13082172