
Possible Mechanisms for Adverse Cardiac Events Caused by Exercise-Induced Hypertension in Long-Distance Middle-Aged Runners: A Review

Abstract
1. Key Points
2. Introduction
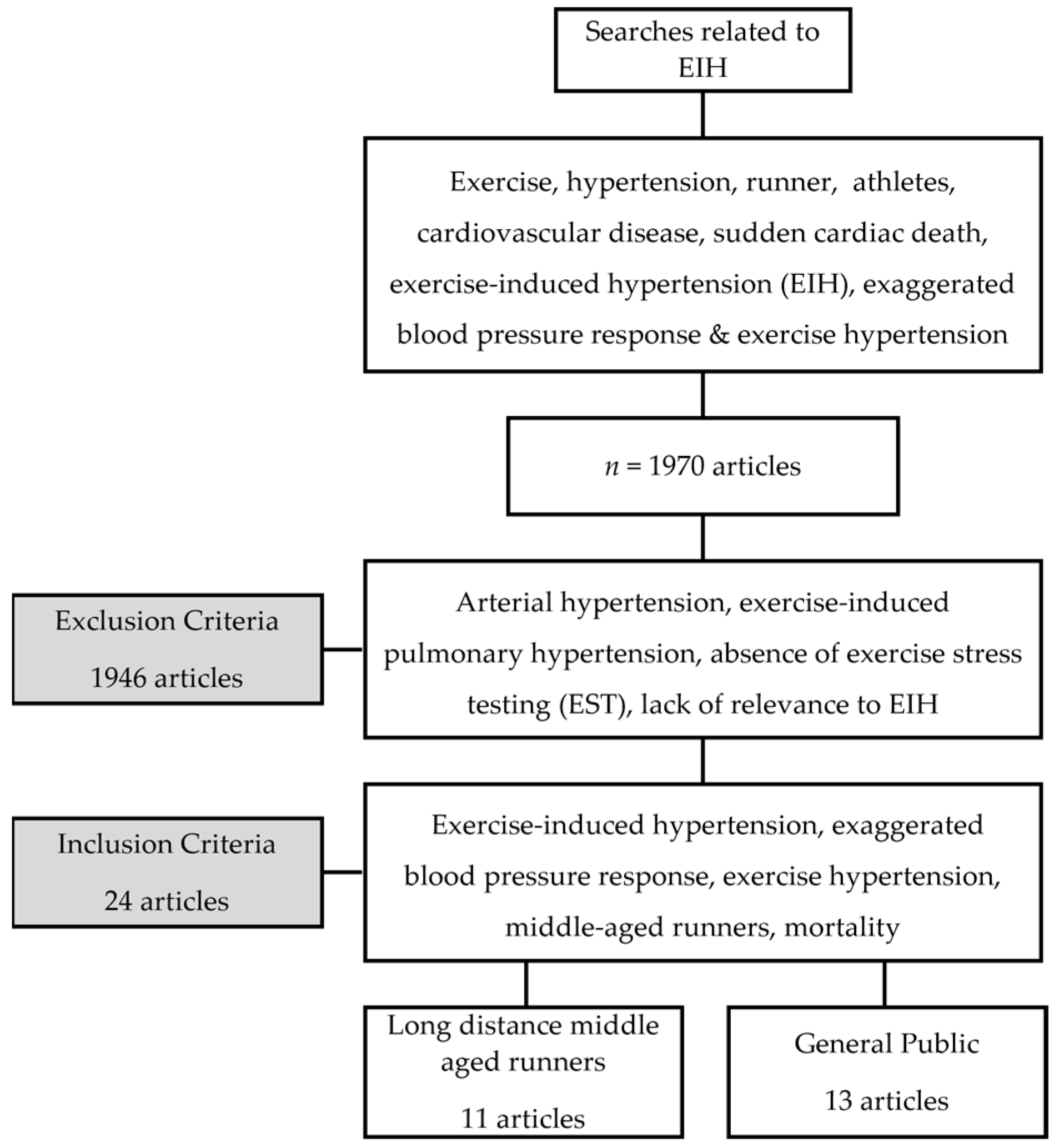
3. Methods
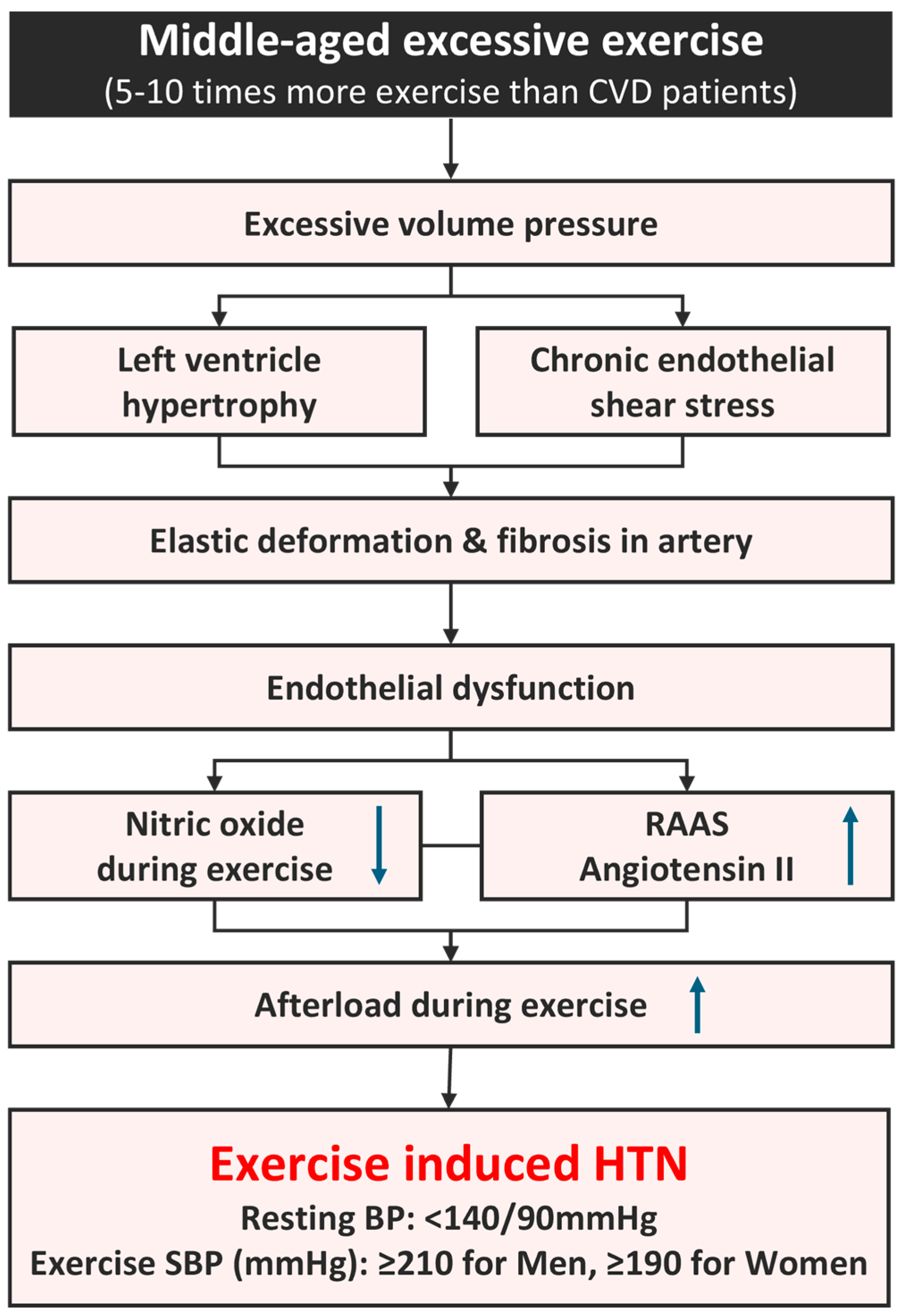
3.1. Mechanism of EIH in Long-Distance Runners (Figure 2)

3.2. Atherosclerotic Plaque Development in EIH
3.3. CAD in Long-Distance Runners
3.4. RPP and Oxidative Stress at High Exercise Intensity
3.5. CAD, Angiotensin II, and Myocardial Ischemia in EIH Runners
3.6. Cardiac/Inflammatory Markers and Long-Distance Runners with EIH (Table 1)
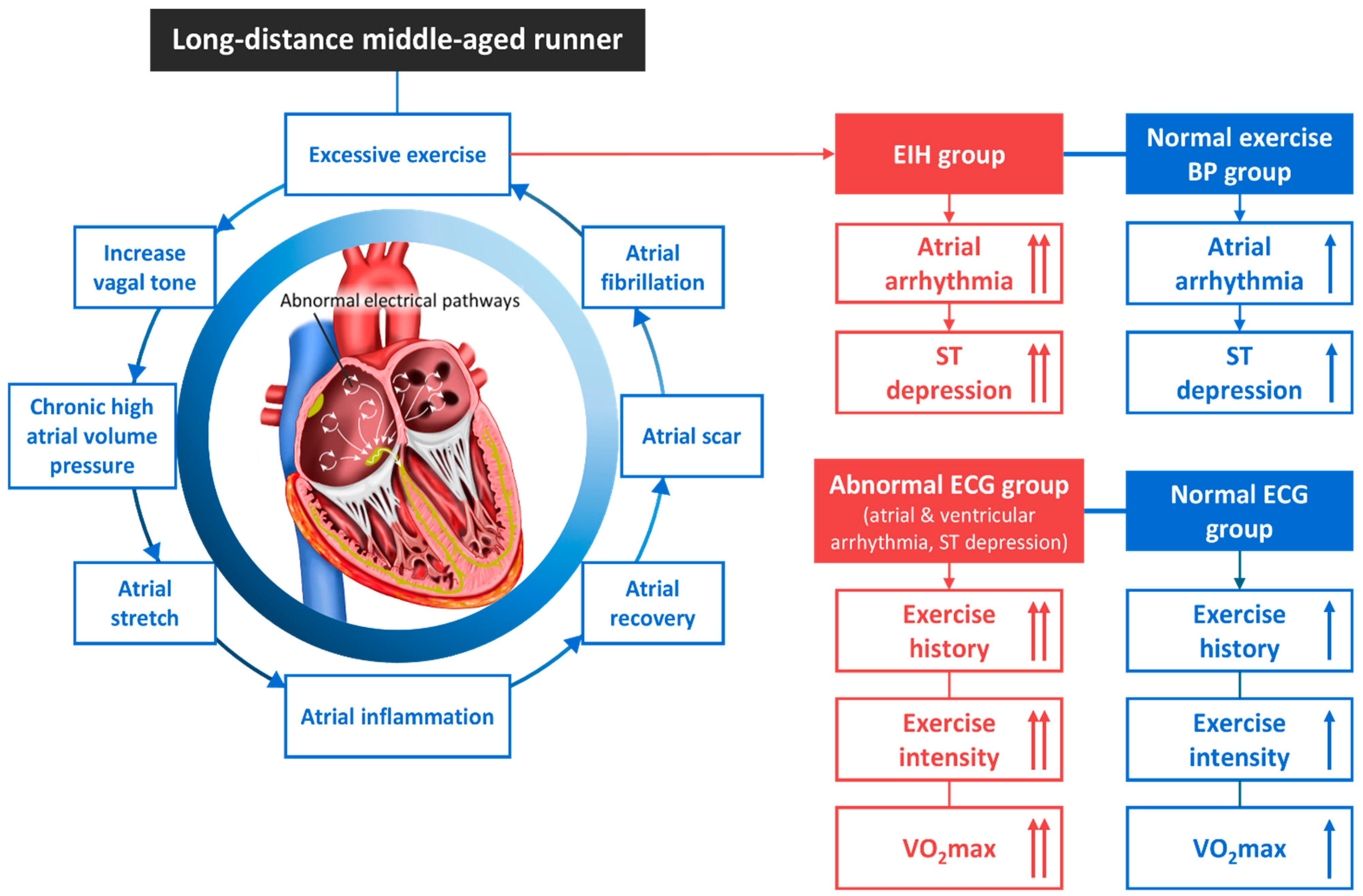
3.7. Arrhythmogenic Mechanism in Long-Distance Runners with EIH (Figure 3)
3.7.1. Exercise Type and Myocardial Remodeling

3.7.2. Chronic Excessive Exercise and AF
3.7.3. AF in Middle-Aged Runners with EIH
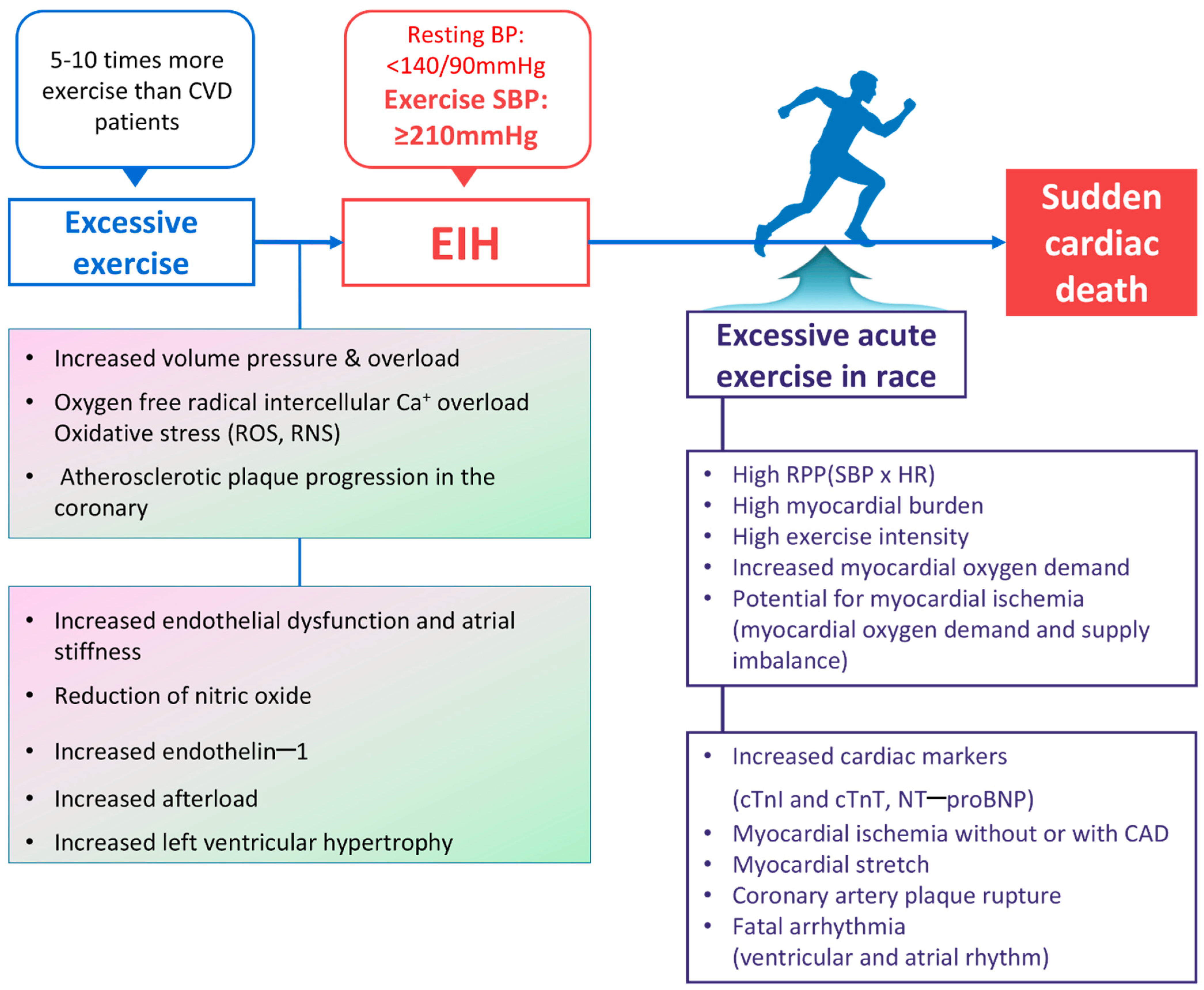
3.8. SCD Hypothesis in Middle-Aged Runners with EIH (Figure 4)

3.9. Can EIH Be Improved by Exercise?
3.10. Interventions for Prevention of SCD in Runners with EIH
3.11. Research Limitations and Future Research Directions
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACEi | angiotensin-converting enzyme inhibitors |
| AERg | abnormal ECG response group |
| AF | atrial fibrillation |
| AIX | augmentation index |
| ARBs | angiotensin II receptor blockers |
| ARG | arrhythmia runners’ group |
| BBs | beta blockers |
| CAC | coronary artery calcium |
| CCBs | calcium-channel blockers |
| cCT | cardiac computed tomography |
| CCVD | cardio-cerebro-vascular disease |
| CK | creatinine kinase |
| CHD | coronary heart disease |
| CON | control |
| cTnI | cardiac troponin I |
| CVD | cardiovascular disease |
| ECGs | electrocardiograms |
| CHG | complex hypertension group |
| EIH | exercise-induced hypertension |
| ET-1 | endothelin-1 |
| GXT | graded exercise test |
| HBPG | high-blood-pressure group |
| hCMP | hypertrophic cardiomyopathy |
| hsCRP | high-sensitivity C-reactive protein |
| IL-10 | interleukin-10 |
| LDL | low-density lipoprotein |
| LVH | left ventricular hypertrophy |
| MDCT | multi-detector computed tomography |
| MSBP | maximal systolic blood pressure |
| NCG | normal control group |
| NBPG | normal blood pressure group |
| NEBPR | normal-exercise blood pressure response |
| NO | nitric oxide |
| NOR | normal |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| NRG | normal runners’ group |
| PWV | pulse wave velocity |
| RAAS | renin–angiotensin–aldosterone system |
| ROS | reactive oxygen species |
| RPP | rate pressure product |
| SBP | systolic blood pressure |
| SCD | sudden cardiac death |
| sE-selectin | soluble E-selectin |
| sVCAM | soluble vascular cell adhesion molecule |
References
- Eckart, R.E.; Shry, E.A.; Burke, A.P.; McNear, J.A.; Appel, D.A.; Castillo-Rojas, L.M.; Avedissian, L.; Pearse, L.A.; Potter, R.N.; Tremaine, L.; et al. Sudden Death in Young Adults: An Autopsy-Based Series of a Population Undergoing Active Surveillance. J. Am. Coll. Cardiol. 2011, 58, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Arija, V.; Villalobos, F.; Pedret, R.; Vinuesa, A.; Jovani, D.; Pascual, G.; Basora, J. Physical activity, cardiovascular health, quality of life and blood pressure control in hypertensive subjects: Randomized clinical trial. Health Qual. Life Outcomes 2018, 16, 184. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; La Gerche, A.; Coombes, J.S. Exercise and cardiovascular risk in patients with hypertension. Am. J. Hypertens. 2014, 28, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Ried-Larsen, M.; Rasmussen, M.G.; Blond, K.; Overvad, T.F.; Overvad, K.; Steindorf, K.; Katzke, V.; Andersen, J.L.M.; Petersen, K.E.N.; Aune, D.; et al. Association of Cycling with All-Cause and Cardiovascular Disease Mortality Among Persons with Diabetes. JAMA Intern. Med. 2021, 181, 1196–1205. [Google Scholar] [CrossRef] [PubMed]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q.; et al. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Whellan, D.J.; Duncan, P.; Pastva, A.M.; Mentz, R.J.; Reeves, G.R.; Nelson, M.B.; Chen, H.; Upadhya, B.; Reed, S.D.; et al. Physical Rehabilitation for Older Patients Hospitalized for Heart Failure. N. Engl. J. Med. 2021, 385, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S.; Hyde, R.T.; Wing, A.L.; Lee, I.-M.; Jung, D.L.; Kampert, J.B. The Association of Changes in Physical-Activity Level and Other Lifestyle Characteristics with Mortality among Men. New Engl. J. Med. 1993, 328, 538–545. [Google Scholar] [CrossRef]
- Noakes, T.D. Heart disease in marathon runners: A review. Med. Sci. Sports Exerc. 1987, 19, 187–194. [Google Scholar] [CrossRef]
- Zilinski, J.L.; Contursi, M.E.; Isaacs, S.K.; Deluca, J.R.; Lewis, G.D.; Weiner, R.B.; Hutter, A.M., Jr.; D’Hemecourt, P.A.; Troyanos, C.; Dyer, K.S.; et al. Myocardial Adaptations to Recreational Marathon Training Among Middle-Aged Men. Circ. Cardiovasc. Imaging 2015, 8, e002487. [Google Scholar] [CrossRef]
- Burke, A.P.; Farb, A.; Malcom, G.T.; Liang, Y.-H.; Smialek, J.E.; Virmani, R. Plaque rupture and sudden death related to exertion in men with coronary artery disease. JAMA 1999, 281, 921–926. [Google Scholar] [CrossRef]
- Maron, B.J.; Poliac, L.C.; Roberts, W.O. Risk for sudden cardiac death associated with marathon running. J. Am. Coll. Cardiol. 1996, 28, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Ratliff, N.B.; Harris, K.M.; Smith, A.S.; Tankh-Johnson, M.; Gornick, C.C.; Maron, B.J. Cardiac arrest in a young marathon runner. Lancet 2002, 360, 542. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.J. Relative risk of sudden cardiac death during marathon running. Arch. Intern. Med. 1997, 157, 1269–1270. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Levine, B.D. Protecting athletes from sudden cardiac death. JAMA 2006, 296, 1648–1650. [Google Scholar] [CrossRef]
- Thompson, D.; Williams, C.; Kingsley, M.; Nicholas, C.W.; Lakomy, H.K.; McArdle, F.; Jackson, M.J. Muscle Soreness and Damage Parameters after Prolonged Intermittent Shuttle-Running Following Acute Vitamin C Supplementation. Int. J. Sports Med. 2001, 22, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Chandra, N.; Bastiaenen, R.; Papadakis, M.; Sharma, S. Sudden Cardiac Death in Young Athletes: Practical Challenges and Diagnostic Dilemmas. J. Am. Coll. Cardiol. 2013, 61, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Drezner, J.A.; Maleszewski, J.J.; Lopez-Anderson, M.; Owens, D.S.; Prutkin, J.M.; Asif, I.M.; Klossner, D.; Ackerman, M.J.; M, A.; et al. Pathogeneses of Sudden Cardiac Death in National Collegiate Athletic Association Athletes. Circ. Arrhythmia Electrophysiol. 2014, 7, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden Deaths in Young Competitive Athletes: Analysis of 1866 Deaths in the United States, 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Muller, J.E.; Abela, G.S.; Nesto, R.W.; Tofler, G.H. Triggers, acute risk factors and vulnerable plaques: The lexicon of a new frontier. J. Am. Coll. Cardiol. 1994, 23, 809–813. [Google Scholar] [CrossRef]
- Van Rosendael, A.R.; De Graaf, M.A.; Scholte, A.J. Cardiac arrest during vigorous exercise: Coronary plaque rupture or myocardial ischaemia? Neth. Heart J. 2015, 23, 130–132. [Google Scholar] [CrossRef][Green Version]
- Giri, S.; Thompson, P.D.; Kiernan, F.J.; Clive, J.; Fram, D.B.; Mitchel, J.F.; Hirst, J.A.; McKay, R.G.; Waters, D.D. Clinical and Angiographic Characteristics of Exertion-Related Acute Myocardial Infarction. JAMA 1999, 282, 1731–1736. [Google Scholar] [CrossRef]
- Thompson, P.D. Exercise prescription and proscription for patients with coronary artery disease. Circulation 2005, 112, 2354–2363. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Malhotra, R.; Chiampas, G.; D’Hemecourt, P.; Troyanos, C.; Cianca, J.; Smith, R.N.; Wang, T.J.; Roberts, W.O.; Thompson, P.D.; et al. Cardiac Arrest during Long-Distance Running Races. N. Engl. J. Med. 2012, 366, 130–140. [Google Scholar] [CrossRef]
- Gobel, F.L.; Norstrom, A.L.; Nelson, R.R.; Jorgensen, C.R.; Wang, Y. The rate-pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation 1978, 57, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Allison, T.G.; Cordeiro, M.A.; Miller, T.D.; Daida, H.; Squires, R.W.; Gau, G.T. Prognostic significance of exercise-induced systemic hypertension in healthy subjects. Am. J. Cardiol. 1999, 83, 371–375. [Google Scholar] [CrossRef]
- Lauer, M.S.; Pashkow, F.J.; Harvey, S.A.; Marwick, T.H.; Thomas, J.D. Angiographic and prognostic implications of an exaggerated exercise systolic blood pressure response and rest systolic blood pressure in adults undergoing evaluation for suspected coronary artery disease. J. Am. Coll. Cardiol. 1995, 26, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.P.; Larson, M.G.; Manolio, T.A.; O’donnell, C.J.; Lauer, M.; Evans, J.C.; Levy, D. Blood Pressure Response During Treadmill Testing as a Risk Factor for New-Onset Hypertension. Circulation 1999, 99, 1831–1836. [Google Scholar] [CrossRef]
- Kurl, S.; Laukkanen, J.; Rauramaa, R.; Lakka, T.; Sivenius, J.; Salonen, J. Systolic Blood Pressure Response to Exercise Stress Test and Risk of Stroke. Stroke 2001, 32, 2036–2041. [Google Scholar] [CrossRef]
- Mundal, R.; Kjeldsen, S.E.; Sandvik, L.; Erikssen, G.; Thaulow, E.; Erikssen, J. Exercise blood pressure predicts mortality from myocardial infarction. Hypertension 1996, 27, 324–329. [Google Scholar] [CrossRef]
- Goel, R.; Majeed, F.; Vogel, R.; Corretti, M.C.; Weir, M.; Mangano, C.; White, C.; Plotnick, G.D.; Miller, M. Exercise-Induced Hypertension, Endothelial Dysfunction, and Coronary Artery Disease in a Marathon Runner. Am. J. Cardiol. 2007, 99, 743–744. [Google Scholar] [CrossRef]
- Kim, C.-H.; Park, Y.; Chun, M.Y.; Kim, Y.-J. Exercise-induced hypertension can increase the prevalence of coronary artery plaque among middle-aged male marathon runners. Medicine 2020, 99, e19911. [Google Scholar] [CrossRef]
- Kim, C.-H.; Park, Y.; Chun, M.Y.; Kim, Y.-J. Exercise-induced hypertension is associated with angiotensin II activity and total nitric oxide. Medicine 2020, 99, e20943. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Goh, C.W.; Byun, Y.S.; Lee, Y.H.; Lee, J.B.; Shin, Y.O. Left ventricular hypertrophy, diastolic dysfunction, pulse pressure, and plasma ET-1 in marathon runners with exaggerated blood pressure response. Int. Heart J. 2013, 54, 82–87. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Kim, C.-H.; Shin, K.-A.; Kim, A.-C.; Lee, Y.-H.; Goh, C.-W.; Oh, J.-K.; Nam, H.-S.; Park, Y. Cardiac Markers of EIH Athletes in Ultramarathon. Int. J. Sports Med. 2012, 33, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, S.; Park, K. Exercise characteristics and incidence of abnormal electrocardiogram response in long-distance runners with exercise-induced hypertension. J. Clin. Hypertens. 2021, 23, 1915–1921. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Kim, C.-H.; Park, K.-M. Excessive exercise habits of runners as new signs of hypertension and arrhythmia. Int. J. Cardiol. 2016, 217, 80–84. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Park, Y.; Kang, D.-H.; Kim, C.-H. Excessive Exercise Habits in Marathoners as Novel Indicators of Masked Hypertension. BioMed Res. Int. 2017, 2017, 1342842. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.S.; Jae, S.Y.; Kim, Y.-J. Exercise-induced hypertension, arterial stiffness, and cardiorespiratory fitness in runners. J. Sports Med. Phys. Fit. 2022, 62, 1397–1403. [Google Scholar] [CrossRef]
- Kim, Y.J.; Shin, Y.O.; Lee, Y.H.; Jee, H.M.; Shin, K.A.; Goh, C.W.; Kim, C.H.; Min, Y.K.; Yang, H.M.; Lee, J.B. Effects of Marathon Running on Cardiac Markers and Endothelin-1 in EIH Athletes. Int. J. Sports Med. 2013, 34, 777–782. [Google Scholar] [CrossRef]
- Jee, H.; Park, J.; Oh, J.-G.; Lee, Y.-H.; Shin, K.-A.; Kim, Y.-J. Effect of a Prolonged Endurance Marathon on Vascular Endothelial and Inflammation Markers in Runners with Exercise-Induced Hypertension. Am. J. Phys. Med. Rehabil. 2013, 92, 513–522. [Google Scholar] [CrossRef]
- Kim, C.-H.; Kang, D.-H.; Kim, Y.-J. Effects of Ultra-Marathon Running on Pro-inflammatory, Anti-inflammatory and Endothelial Function Factors in Athletes with Exercise-induced Hypertension. Korean J. Sports Med. 2016, 34, 169. [Google Scholar] [CrossRef]
- Park, M.-H.; Shin, K.-A.; Kim, C.-H.; Lee, Y.-H.; Park, Y.; Ahn, J.; Kim, Y.-J. Effects of Long-Distance Running on Cardiac Markers and Biomarkers in Exercise-Induced Hypertension Runners: An Observational Study. Ann. Rehabilitation Med. 2018, 42, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Le, V.-V.; Mitiku, T.; Sungar, G.; Myers, J.; Froelicher, V. The Blood Pressure Response to Dynamic Exercise Testing: A Systematic Review. Prog. Cardiovasc. Dis. 2008, 51, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Gottdiener, J.S.; Brown, J.; Zoltick, J.; Fletcher, R.D. Left Ventricular Hypertrophy in Men with Normal Blood Pressure: Relation to Exaggerated Blood Pressure Response to Exercise. Ann. Intern. Med. 1990, 112, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Jae, S.Y.; Kurl, S.; Kunutsor, S.K.; Franklin, A.B.; Laukkanen, A.J. Relation of maximal systolic blood pressure during exercise testing to the risk of sudden cardiac death in men with and without cardiovascular disease. Eur. J. Prev. Cardiol. 2019, 27, 2220–2222. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, S.E.; Mundal, R.; Sandvik, L.; Erikssen, G.; Thaulow, E.; Erikssen, J. Supine and exercise systolic blood pressure predict cardiovascular death in middle-aged men. J. Hypertens. 2001, 19, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W.I.; Nichaman, M.Z.; Frankowski, R.F.; Blair, S.N. Maximal exercise hemodynamics and risk of mortality in apparently healthy men and women. Med. Sci. Sports Exerc. 1996, 28, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Kurl, S.; Rauramaa, R.; Lakka, T.A.; Venäläinen, J.M.; Salonen, J.T. Systolic blood pressure response to exercise testing is related to the risk of acute myocardial infarction in middle-aged men. Eur. J. Prev. Cardiol. 2006, 13, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.G.; Otahal, P.; Cleland, V.J.; Blizzard, L.; Marwick, T.H.; Sharman, J.E. Exercise-Induced Hypertension, Cardiovascular Events, and Mortality in Patients Undergoing Exercise Stress Testing: A Systematic Review and Meta-Analysis. Am. J. Hypertens. 2012, 26, 357–366. [Google Scholar] [CrossRef]
- Skretteberg, P.T.; Grundvold, I.; Kjeldsen, S.E.; Engeseth, K.; Liestøl, K.; Erikssen, G.; Erikssen, J.; Gjesdal, K.; Bodegard, J. Seven-Year Increase in Exercise Systolic Blood Pressure at Moderate Workload Predicts Long-Term Risk of Coronary Heart Disease and Mortality in Healthy Middle-Aged Men. Hypertension 2013, 61, 1134–1140. [Google Scholar] [CrossRef]
- Weiss, S.A.; Blumenthal, R.S.; Sharrett, A.R.; Redberg, R.F.; Mora, S. Exercise Blood Pressure and Future Cardiovascular Death in Asymptomatic Individuals. Circulation 2010, 121, 2109–2116. [Google Scholar] [CrossRef]
- Gupta, M.P.; Polena, S.; Coplan, N.; Panagopoulos, G.; Dhingra, C.; Myers, J.; Froelicher, V. Prognostic Significance of Systolic Blood Pressure Increases in Men During Exercise Stress Testing. Am. J. Cardiol. 2007, 100, 1609–1613. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Leitão, C.B.; Canani, L.H.; Ricardo, E.D.; Pinto, L.C.; Gross, J.L. Blood pressure responses to exercise in type II diabetes mellitus patients with masked hypertension. J. Hum. Hypertens. 2009, 23, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Zaidi, A. Exercise-induced arrhythmogenic right ventricular cardiomyopathy: Fact or fallacy? Eur. Heart J. 2011, 33, 938–940. [Google Scholar] [CrossRef] [PubMed]
- Klenk, C.; Klenk, C.; Brunner, H.; Brunner, H.; Nickel, T.; Nickel, T.; Sagmeister, F.; Sagmeister, F.; Yilmaz, A.; Yilmaz, A.; et al. Cardiac structure and function in response to a multi-stage marathon over 4486 km. Eur. J. Prev. Cardiol. 2019, 28, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Whyte, G.; Sheppard, M.; George, K.; Shave, R.; Wilson, M.; Prasad, S.; O’hanlon, R.; Sharma, S. Post-mortem evidence of idiopathic left ventricular hypertrophy and idiopathic interstitial myocardial fibrosis: Is exercise the cause? Br. J. Sports Med. 2007, 42, 304–305. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Kardara, D.; Anastasakis, A.; Baou, K.; Terentes-Printzios, D.; Tousoulis, D.; Stefanadis, C. Arterial Stiffness and Wave Reflections in Marathon Runners. Am. J. Hypertens. 2010, 23, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Miyai, N.; Arita, M.; Morioka, I.; Miyashita, K.; Nishio, I.; Takeda, S. Exercise BP response in subjects with high-normal BP: Exaggerated blood pressure response to exercise and risk of future hypertension in subjects with high-normal blood pressure. J. Am. Coll. Cardiol. 2000, 36, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Stewart, K.J.; Sung, J.; Silber, H.A.; Fleg, J.L.; Kelemen, M.D.; Turner, K.L.; Bacher, A.C.; Dobrosielski, D.A.; DeRegis, J.R.; Shapiro, E.P.; et al. Exaggerated exercise blood pressure is related to impaired endothelial vasodilator function. Am. J. Hypertens. 2004, 17, 314–320. [Google Scholar] [CrossRef]
- Tzemos, N.; Lim, P.O.; MacDonald, T.M. Exercise blood pressure and endothelial dysfunction in hypertension. Int. J. Clin. Pract. 2009, 63, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Thanassoulis, G.; Lyass, A.; Benjamin, E.J.; Larson, M.G.; Vita, J.A.; Levy, D.; Hamburg, N.M.; Widlansky, M.E.; O’Donnell, C.J.; Mitchell, G.F.; et al. Relations of Exercise Blood Pressure Response to Cardiovascular Risk Factors and Vascular Function in the Framingham Heart Study. Circulation 2012, 125, 2836–2843. [Google Scholar] [CrossRef] [PubMed]
- Burr, J.F.; Drury, C.T.; Phillips, A.A.; Ivey, A.; Ku, J.; Warburton, D.E. Long-term ultra-marathon running and arterial compliance. J. Sci. Med. Sport 2014, 17, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.G.; Sharman, J.E. Exercise Hypertension. Pulse 2014, 1, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Hibino, M.; Kobeissi, E.; Aune, D. Blood pressure, hypertension and the risk of sudden cardiac death: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 2020, 35, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.D.; Gona, P.; Larson, M.G.; Plehn, J.F.; Benjamin, E.J.; O’Donnell, C.J.; Levy, D.; Vasan, R.S.; Wang, T.J. Exercise Blood Pressure and the Risk of Incident Cardiovascular Disease (from the Framingham Heart Study). Am. J. Cardiol. 2008, 101, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Tsiflikas, I.; Thomas, C.; Fallmann, C.; Schabel, C.; Mangold, S.; Ketelsen, D.; Claussen, C.D.; Axmann, D.; Schroeder, S.; Burgstahler, C. Prevalence of Subclinical Coronary Artery Disease in Middle-Aged, Male Marathon Runners Detected by Cardiac CT. Rofo 2015, 187, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Merghani, A.; Maestrini, V.; Rosmini, S.; Cox, A.T.; Dhutia, H.; Bastiaenan, R.; David, S.; Yeo, T.J.; Narain, R.; Malhotra, A.; et al. Prevalence of Subclinical Coronary Artery Disease in Masters Endurance Athletes with a Low Atherosclerotic Risk Profile. Circulation 2017, 136, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Mason, S.A.; Trewin, A.J.; Parker, L.; Wadley, G.D. Antioxidant supplements and endurance exercise: Current evidence and mechanistic insights. Redox Biol. 2020, 35, 101471. [Google Scholar] [CrossRef]
- El Assar, M.; Angulo, J.; Rodríguez-Mañas, L. Oxidative stress and vascular inflammation in aging. Free Radic. Biol. Med. 2013, 65, 380–401. [Google Scholar] [CrossRef]
- Knez, W.L.; Coombes, J.S.; Jenkins, D.G. Ultra-Endurance Exercise and Oxidative Damage: Implications for Cardio-Vascular Health. Sports Med. 2006, 36, 429–441. [Google Scholar] [CrossRef]
- Dinh, Q.N.; Drummond, G.R.; Sobey, C.G.; Chrissobolis, S. Roles of Inflammation, Oxidative Stress, and Vascular Dysfunction in Hypertension. BioMed Res. Int. 2014, 2014, 406960. [Google Scholar] [CrossRef]
- Mastaloudis, A.; Leonard, S.W.; Traber, M.G. Oxidative stress in athletes during extreme endurance exercise. Free Radic. Biol. Med. 2001, 31, 911–922. [Google Scholar] [CrossRef]
- Sánchez-Quesada, J.; Homs-Serradesanferm, R.; Serrat-Serrat, J.; Serra-Grima, J.; González-Sastre, F.; Ordóñez-Llanos, J. Increase of LDL susceptibility to oxidation occurring after intense, long duration aerobic exercise. Atherosclerosis 1995, 118, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.J.; Bryan, D.R.; Neumeier, W.H.; Glasser, S.P.; Hunter, G.R. Serum Tumor Necrosis Factor-alpha associates with Myo-cardial Oxygen Demand and Exercise Tolerance in Postmenopausal Women. Int. J. Exerc. Sci. 2018, 11, 42–54. [Google Scholar]
- Members, T.F.; Thygesen, K.; Alpert, J.S.; White, H.D.; Jaffe, A.S.; Apple, F.S.; Galvani, M.; Katus, H.A.; Newby, L.K.; Ravkilde, J.; et al. Universal definition of myocardial infarction. Eur. Heart J. 2007, 28, 2525–2538. [Google Scholar] [CrossRef] [PubMed]
- Richards, A.M.; Nicholls, M.G.; Yandle, T.G.; Frampton, C.; Espiner, E.A.; Turner, J.G.; Buttimore, R.C.; Lainchbury, J.G.; Elliott, J.M.; Ikram, H.; et al. Plasma N-Terminal Pro–Brain Natriuretic Peptide and Adrenomedullin. Circulation 1998, 97, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- Fortescue, E.B.; Shin, A.Y.; Greenes, D.S.; Mannix, R.C.; Agarwal, S.; Feldman, B.J.; Shah, M.I.; Rifai, N.; Landzberg, M.J.; Newburger, J.W.; et al. Cardiac Troponin Increases Among Runners in the Boston Marathon. Ann. Emerg. Med. 2007, 49, 137–143.e1. [Google Scholar] [CrossRef]
- Scharhag, J.; Herrmann, M.; Urhausen, A.; Haschke, M.; Herrmann, W.; Kindermann, W. Independent elevations of N-terminal pro–brain natriuretic peptide and cardiac troponins in endurance athletes after prolonged strenuous exercise. Am. Heart J. 2005, 150, 1128–1134. [Google Scholar] [CrossRef]
- Scott, J.M.; Esch, B.T.; Shave, R.; Warburton, D.E.; Gaze, D.; George, K. Cardiovascular Consequences of Completing a 160-km Ultramarathon. Med. Sci. Sports Exerc. 2009, 41, 25–33. [Google Scholar] [CrossRef]
- Scharhag, J.; George, K.; Shave, R.; Urhausen, A.; Kindermann, W. Exercise-Associated Increases in Cardiac Biomarkers. Med. Sci. Sports Exerc. 2008, 40, 1408–1415. [Google Scholar] [CrossRef]
- Nie, J.; Close, G.; George, K.P.; Tong, T.K.; Shi, Q. Temporal association of elevations in serum cardiac troponin T and myocardial oxidative stress after prolonged exercise in rats. Eur. J. Appl. Physiol. 2010, 110, 1299–1303. [Google Scholar] [CrossRef] [PubMed]
- Hickman, P.E.; Potter, J.M.; Aroney, C.; Koerbin, G.; Southcott, E.; Wu, A.H.; Roberts, M.S. Cardiac troponin may be released by ischemia alone, without necrosis. Clin. Chim. Acta 2010, 411, 318–323. [Google Scholar] [CrossRef] [PubMed]
- McNeil, P.L.; Terasaki, M. Coping with the inevitable: How cells repair a torn surface membrane. Nature 2001, 3, E124–E129. [Google Scholar] [CrossRef]
- Kim, Y.J.; Ahn, J.K.; Shin, K.A.; Kim, C.H.; Lee, Y.H.; Park, K.M. Correlation of Cardiac Markers and Biomarkers with Blood Pressure of Middle-Aged Marathon Runners. J. Clin. Hypertens. 2015, 17, 868–873. [Google Scholar] [CrossRef]
- Vinereanu, D.; Florescu, N.; Sculthorpe, N.; Tweddel, A.C.; Stephens, M.R.; Fraser, A.G. Left ventricular long-axis diastolic function is augmented in the hearts of endurance-trained compared with strength-trained athletes. Clin. Sci. 2002, 103, 249–257. [Google Scholar] [CrossRef]
- Palatini, P.; Mos, L.; Di Marco, A.; Mormino, P.; Munari, L.; Del Torre, M.; Valle, F.; Pessina, A.C.; Dal Palu, C. Intra-arterial blood pressure recording during sports activities. J. Hypertens. 1987, 5, 479–481. [Google Scholar]
- Pluim, B.M.; Zwinderman, A.H.; van der Laarse, A.; van der Wall, E.E. The Athlete’s Heart. A meta-analysis of cardiac structure and function. Circulation 2000, 101, 336–344. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, J.D.; McKelvie, R.S.; Moroz, D.E.; Sale, D.G.; McCartney, N.; Buick, F.; Durand, M.J.; Phillips, S.A.; Widlansky, M.E.; Otterson, M.F.; et al. Factors affecting blood pressure during heavy weight lifting and static contractions. J. Appl. Physiol. 1992, 73, 1590–1597. [Google Scholar] [CrossRef]
- Mithchell, J.H.; Haskell, W.L.; Raven, P.B. Classification of sports. J. Am. Coll. Cardiol. 1994, 24, 864–866. [Google Scholar] [CrossRef]
- Foster, C.; Gaeckle, T.; Braastad, R.; Schmidt, D.H.; Port, S.C. First-pass radionuclide angiography during bicycle and treadmill exercise. J. Nucl. Cardiol. 1995, 2, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Chun, H.; Kim, C.-H. Exaggerated Response of Systolic Blood Pressure to Cycle Ergometer. Ann. Rehabil. Med. 2013, 37, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.T.; Franklin, B.A. Reduced Incidence of Cardiac Arrhythmias in Walkers and Runners. PLoS ONE 2013, 8, e65302. [Google Scholar] [CrossRef] [PubMed]
- Baldesberger, S.; Bauersfeld, U.; Candinas, R.; Seifert, B.; Zuber, M.; Ritter, M.; Jenni, R.; Oechslin, E.; Luthi, P.; Scharf, C.; et al. Sinus node disease and arrhythmias in the long-term follow-up of former professional cyclists. Eur. Heart J. 2007, 29, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M. Atrial fibrillation in endurance athletes. Eur. J. Prev. Cardiol. 2013, 21, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, J.; Nielsen, J.R. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace 2009, 11, 1156–1159. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, J.; Kujala, U.M.; Kaprio, J.; Sarna, S.; Viitasalo, M. Lone atrial fibrillation in vigorously exercising middle aged men: Case-control study. BMJ 1998, 316, 1784–1785. [Google Scholar] [CrossRef] [PubMed]
- Mont, L.; Elosua, R.; Brugada, J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace 2008, 11, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Mont, L.; Sambola, A.; Brugada, J.; Vacca, M.; Marrugat, J.; Elosua, R.; Paré, C.; Azqueta, M.; Sanz, G. Long-lasting sport practice and lone atrial fibrillation. Eur. Heart J. 2002, 23, 477–482. [Google Scholar] [CrossRef]
- Waldmann, V.; Jouven, X.; Narayanan, K.; Piot, O.; Chugh, S.S.; Albert, C.M.; Marijon, E. Association Between Atrial Fibrillation and Sudden Cardiac Death: Pathophysiological and Epidemiological Insights. Circ. Res. 2020, 127, 301–309. [Google Scholar] [CrossRef]
- Rattanawong, P.; Upala, S.; Riangwiwat, T.; Jaruvongvanich, V.; Sanguankeo, A.; Vutthikraivit, W.; Chung, E.H. Atrial fibrillation is associated with sudden cardiac death: A systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2018, 51, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Zipes, D.P.; Libby, P.; Bonow, R.O.; Mann, D.L.; Tomaselli, G.F.; Braunwald, E. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 11th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2019. [Google Scholar]
- Shenasa, M.; Shenasa, H. Hypertension, left ventricular hypertrophy, and sudden cardiac death. Int. J. Cardiol. 2017, 237, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Waks, J.W.; Sitlani, C.M.; Soliman, E.Z.; Kabir, M.; Ghafoori, E.; Biggs, M.L.; Henrikson, C.A.; Sotoodehnia, N.; Biering-Sørensen, T.; Agarwal, S.K.; et al. Global Electric Heterogeneity Risk Score for Prediction of Sudden Cardiac Death in the General Population: The Atherosclerosis Risk in Communities (ARIC) and Cardiovascular Health (CHS) Studies. Circulation 2016, 133, 2222–2234. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Rauramaa, R. Systolic blood pressure during exercise testing and the risk of sudden cardiac death. Int. J. Cardiol. 2013, 168, 3046–3047. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, L.; Kervio, G.; Doutreleau, S.; Mathieu, J.-P.; Guy, J.-M.; Mignot, A.; Corneloup, L.; Passard, F.; Laporte, T.; Girard-Girod, A.; et al. The medical value and cost-effectiveness of an exercise test for sport preparticipation evaluation in asymptomatic middle-aged white male and female athletes. Arch. Cardiovasc. Dis. 2017, 110, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Katzel, L.I.; Fleg, J.L.; Busby-Whitehead, M.J.; Sorkin, J.D.; Becker, L.C.; Lakatta, E.G.; Goldberg, A.P. Exercise-induced silent myo-cardial ischemia in master athletes. Am. J. Cardiol. 1998, 81, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Leischik, R.; Spelsberg, N.; Niggemann, H.; Dworrak, B.; Tiroch, K. Exercise-induced arterial hypertension–An independent factor for hypertrophy and a ticking clock for cardiac fatigue or atrial fibrillation in athletes? F1000Research 2014, 3, 105. [Google Scholar] [CrossRef] [PubMed]
- Bond, V.; Stephens, Q.; Adams, R.G.; Vaccaro, P.; Demeersman, R.; Williams, D.; Obisesan, T.O.; Franks, B.D.; Oke, L.M.; Coleman, B.; et al. Aerobic Exercise Attenuates an Exaggerated Exercise Blood Pressure Response in Normotensive Young Adult African-American Men. Blood Press. 2002, 11, 229–234. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Boeno, F.P.; Ramis, T.R.; Munhoz, S.V.; Farinha, J.B.; Moritz, C.E.; Leal-Menezes, R.; Ribeiro, J.L.; Christou, D.D.; Reischak-Oliveira, A. Effect of aerobic and resistance exercise training on inflammation, endothelial function and ambulatory blood pressure in middle-aged hypertensive patients. J. Hypertens. 2020, 38, 2501–2509. [Google Scholar] [CrossRef]
- Möhlenkamp, S.; Lehmann, N.; Breuckmann, F.; Bröcker-Preuss, M.; Nassenstein, K.; Halle, M.; Budde, T.; Mann, K.; Barkhausen, J.; Heusch, G.; et al. Running: The risk of coronary events: Prevalence and prognostic relevance of coronary atherosclerosis in marathon runners. Eur. Heart J. 2008, 29, 1903–1910. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Coca, A.; Kahan, T.; Boriani, G.; Manolis, A.S.; Olsen, M.H.; Oto, A.; Potpara, T.S.; Steffel, J.; Marín, F.; et al. Hypertension and Cardiac Arrhythmias: Executive Summary of a Consensus Document from the European Heart Rhythm Association (EHRA) and ESC Council on Hypertension, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and Sociedad Latinoamericana de Estimulación Cardíaca y Electrofisiología (SOLEACE). Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 235–250. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-K.; Kang, S.-H. Effects of Aerobic Exercise on Blood Pressure Response during Exercise. Iran. J. Public Health 2019, 48, 1738–1740. [Google Scholar] [CrossRef]
- Kim, Y.J.; Shin, Y.O. Effects of aerobic exercise on cardiopulmonary- related factors in exercise-induced hypertension patients. Exerc. Sci. 2007, 16, 131–140. [Google Scholar]
- Miyai, N.; Arita, M.; Miyashita, K.; Morioka, I.; Shiraishi, T.; Nishio, I.; Takeda, S. Antihypertensive Effects of Aerobic Exercise in Middle-Aged Normotensive Men with Exaggerated Blood Pressure Response to Exercise. Hypertens. Res. 2002, 25, 507–514. [Google Scholar] [CrossRef]
- Ogita, H.; Liao, J.K. Endothelial Function and Oxidative Stress. Endothelium 2004, 11, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Witztum, J. The oxidation hypothesis of atherosclerosis. Lancet 1994, 344, 793–795. [Google Scholar] [CrossRef]
- Thirupathi, A.; Pinho, R.A.; Ugbolue, U.C.; He, Y.; Meng, Y.; Gu, Y. Effect of Running Exercise on Oxidative Stress Biomarkers: A Systematic Review. Front. Physiol. 2021, 11, 610112. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Mao, Q.; Cao, J.; Wang, Y.; Zhou, X.; Fan, L. Effects of coenzyme Q10 on vascular endothelial function in humans: A meta-analysis of randomized controlled trials. Atherosclerosis 2011, 221, 311–316. [Google Scholar] [CrossRef]
- Morrison, D.; Hughes, J.; Della Gatta, P.A.; Mason, S.; Lamon, S.; Russell, A.P.; Wadley, G.D. Vitamin C and E supplementation prevents some of the cellular adaptations to endurance-training in humans. Free Radic. Biol. Med. 2015, 89, 852–862. [Google Scholar] [CrossRef]
- Paulsen, G.; Cumming, K.T.; Holden, G.; Hallén, J.; Rønnestad, B.R.; Sveen, O.; Skaug, A.; Paur, I.; Bastani, N.E.; Østgaard, H.N.; et al. Vitamin C and E supplementation hampers cellular adaptation to endurance training in humans: A double-blind, randomised, controlled trial. J. Physiol. 2014, 592, 1887–1901. [Google Scholar] [CrossRef]
- Tiano, L.; Belardinelli, R.; Carnevali, P.; Principi, F.; Seddaiu, G.; Littarru, G.P. Effect of coenzyme Q10 administration on endothelial function and extracellular superoxide dismutase in patients with ischaemic heart disease: A double-blind, randomized controlled study. Eur. Heart J. 2007, 28, 2249–2255. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, R.J.; Canale, R.E.; McCarthy, C.G.; Farney, T.M. Impact of Oral Ubiquinol on Blood Oxidative Stress and Exercise Performance. Oxidative Med. Cell Longev. 2012, 2012, 465020. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, A.; Solito, F.; Carmosino, G.; Bargossi, A.M.; Fiorella, P.L. Effect of ubidecarenone oral treatment on aerobic power in middle-aged trained subjects. J. Sports Med. Phys. Fit. 2000, 40, 51–57. [Google Scholar]
- Clifford, T.; Jeffries, O.; Stevenson, E.J.; Davies, K.A.B. The effects of vitamin C and E on exercise-induced physiological adaptations: A systematic review and Meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 3669–3679. [Google Scholar] [CrossRef]
- Mason, S.A.; Baptista, R.; Della Gatta, P.A.; Yousif, A.; Russell, A.P.; Wadley, G.D. High-dose vitamin C supplementation increases skeletal muscle vitamin C concentration and SVCT2 transporter expression but does not alter redox status in healthy males. Free Radic. Biol. Med. 2014, 77, 130–138. [Google Scholar] [CrossRef]
- Okudan, N.; Belviranli, M.; Torlak, S. Coenzyme Q10 does not prevent exercise-induced muscle damage and oxidative stress in sedentary men. J. Sports Med. Phys. Fit. 2018, 58, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Östman, B.; Sjödin, A.; Michaëlsson, K.; Byberg, L. Coenzyme Q10 supplementation and exercise-induced oxidative stress in humans. Nutrition 2012, 28, 403–417. [Google Scholar] [CrossRef]
- Franz, I.-W.; Behr, U.; Ketelhut, R. Resting and Exercise Blood Pressure with Atenolol, Enalapril and a Low-Dose Combination. J. Hypertens. 1987, 5, S37–S41. [Google Scholar] [CrossRef]
- Haasis, R.; Bethge, H. Exercise blood pressure and heart rate reduction 24 and 3 hours after drug intake in hypertensive patients follwing 4 weeks of treatment with bisoprolol and metoprolol: A randomized multicentre double-blind study (BISOMET). Eur. Heart J. 1987, 8, 103–113. [Google Scholar] [CrossRef]
- Lorimer, A.R.; Barbour, M.B.; Lawrie, T.D. An evaluation of the effect on resting and exercise blood pressure of some first line treatments in hypertension. Ann. Clin. Res. 1983, 15, 30–34. [Google Scholar]
- Kokkinos, P.; Chrysohoou, C.; Panagiotakos, D.; Narayan, P.; Greenberg, M.; Singh, S. Beta-Blockade Mitigates Exercise Blood Pressure in Hypertensive Male Patients. J. Am. Coll. Cardiol. 2006, 47, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.P.; Jacob, R.F.; Kubant, R.; Jacoby, A.; Louka, F.; Corbalan, J.J.; Malinski, T. Effects of angiotensin receptor blockers on endothelial nitric oxide release: The role of eNOS variants. Br. J. Clin. Pharmacol. 2012, 74, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Radenkovic, M.; Stojanović, M.; Nešić, I.; Prostran, M. Angiotensin receptor blockers & endothelial dysfunction: Possible correlation & therapeutic implications. Indian J. Med. Res. 2016, 144, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Ha, J.-W. Hypertensive response to exercise: Mechanisms and clinical implication. Clin. Hypertens. 2016, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Shim, C.Y.; Ha, J.-W.; Park, S.; Choi, E.-Y.; Choi, D.; Rim, S.-J.; Chung, N. Exaggerated blood pressure response to exercise is associated with augmented rise of angiotensin II during exercise. J. Am. Coll. Cardiol. 2008, 52, 287–292. [Google Scholar] [CrossRef]
- Warner, J.G.; Metzger, D.; Kitzman, D.W.; Wesley, D.J.; Little, W.C. Losartan improves exercise tolerance in patients with diastolic dysfunction and a hypertensive response to exercise. J. Am. Coll. Cardiol. 1999, 33, 1567–1572. [Google Scholar] [CrossRef]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. ACSM’s New Preparticipation Health Screening Recommendations from ACSM’s Guidelines for Exercise Testing and Prescription, Ninth Edition. Optom. Vis. Sci. 2013, 12, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Gherbesi, E.; Faggiano, A.; Sala, C.; Carugo, S.; Grassi, G.; Tadic, M. Masked Hypertension and Exaggerated Blood Pressure Response to Exercise: A Review and Meta-Analysis. Diagnostics 2023, 13, 1005. [Google Scholar] [CrossRef]
- de Gregorio, C.; Giallauria, F.; Lantone, G.; Bellomo, F.; Campisi, M.; Firetto, G.; Mazzone, P.; Testa, C.; Grimaldi, P.; Casale, M.; et al. Exaggerated blood pressure reactionreaction to exercise in subjects with and without systemic hypertension. Eur. J. Prev. Cardiol. 2021, 28, 1152–1154. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Aim | Group (n, age) | Method | Result | Conclusion |
|---|---|---|---|---|---|
| Kim et al. [31] | To investigate the prevalence of CAD in middle-aged runners with EIH. | NBPG (n = 22, 51.7 ± 4.9) EIHG (n = 28, 54.5 ± 5.0) | Comparison of CAD prevalence in EIH and non-EIH groups according to GXT results | EIHG had higher CAC scores (42.6 ± 67.8) than NBPG (2.8 ± 6.0). EIHG had a higher CAC score distribution than NBPG. EIHG had a higher prevalence of coronary artery plaque and maximum internal arterial stenosis than NBPG. | Middle-aged runners with EIH are associated with an increased prevalence of coronary artery plaques. EIH screening via GXT is recommended, followed by MDCT. |
| Kim et al. [32] | To assess the association between middle-aged runners with EIH and ATII. | NBPG (n = 21, 53.6 ± 4.9) EIHG (n = 35, 53.9 ± 4.8) CHG (n = 14, 52.1 ± 5.1) | Blood collection before and after GXT, followed by RAAS and NO tests | ATII activity and a reduction in NO were associated with endothelial dysfunction in runners with EIH. | ATII inhibitors are appropriate antihypertensive medications for runners with EIH. |
| Kim et al. [34] | To compare cardiac markers and inflammation before and after a 100 km run between EIH and NOR runners. | NOR (n = 10, 46.8 ± 1.2) EIH (n = 10, 47.5 ± 1.3) | Blood collection pre-run and at 50 and 100 km | CK: Increase in EIH with respect to NOR at 100 km NT-proBNP: Increase in EIH with respect to NOR at 50 and 100 km CRP: Increase in EIH with respect to NOR at 100 km | Runners with EIH did not show myocardial damage following the 100 km run but had myocardial stress and active muscle damage due to epithelial dysfunction. |
| Kim et al. [35] | To investigate the prevalence of abnormal ECG response and training characteristics of middle-aged runners with EIH. | NEIHg (n = 268, 48.4 ± 7.1) EIHg (n = 338, 49.9 ± 7.2) Non-AERg (n = 569) AERg (n = 37) | Comparison of abnormal responses in GXT and training characteristics | EIHG had higher frequencies of ST segment depression and atrial arrhythmias than NEIHg. AERg had longer training history and greater total training time than non-AERg | The high incidence of myocardial ischemia and atrial arrythmias among middle-aged runners with EIH is associated with excessive training. |
| Kim et al. [36] | To compare hemodynamic response and training characteristics between the abnormal response group (ARG) and the normal response group (NRG). | NRG (n = 538, 49.0 ± 7.3) ARG (n = 14, 49.2 ± 7.9) | Comparison of arrhythmias detected in GXT, hemodynamic response, and training characteristics | Both groups had prehypertension and EIH in the resting state. ARG had lower DBP and higher VO2max, a longer training history, and higher training intensity than NRG. | Middle-aged long-distance runners exhibited prehypertension and EIH. ARG has high training intensity, a long training history, and high cardiorespiratory fitness and requires regular cardiovascular tests and adequate exercise prescriptions. |
| Kim et al. [37] | To investigate excessive exercise habits, resting and exercise blood pressure, and cardiac events. | NBPG (n = 214, 49.1 ± 7.7) HBPG (n = 357, 48.8 ± 6.6) | Comparison of training characteristics and cardiac events between a resting hypertension group and a non-resting-hypertension group based on GXT results | HBPG had a shorter marathon history than NBPG but had higher training intensity, a longer daily training duration, and a higher drinking frequency. | High training intensity and long training time can be used as new indices for potential resting and exercise hypertension for middle-aged long-distance runners. |
| Yoon et al [38] | To investigate the arterial stiffness of middle-aged runners with EIH | NBPG (n = 17, 49.9 ± 5.3) EIHG (n = 39, 51.7 ± 5.0) CHG (n = 10, 50.8 ± 3.3) | Comparison of AIX, AIX@75bpm, and PWV between groups assigned based on GXT results | CHG had higher AIX and AIX@75bp than EIHG and NBPG. EIHG had higher AIX and AIX@75bp than NBPG. VO2max was inversely correlated with MSBP during exercise, PWV, AIX, and AIX75@bpm | High arterial stiffness can increase the risk of cerebrovascular diseases in runners with EIH. On the other hand, cardiopulmonary fitness is negatively correlated with exercise blood pressure and arterial stiffness. Further research on this correlation is necessary. |
| Kim et al. [39] | To compare cardiac markers and ET-1 before and after a marathon between EIH and CON runners. | CON (n = 10, 52.5 ± 7.9) EIH (n = 10, 50.6 ± 7.5) | Blood collection pre- and post-run | cTnI, NT-proBNP, ET-1: Increased in EIH with respect to CON immediately after the run | Increased vascular tone and blood pressure during a marathon increased myocardial stress and perfusion in runners with EIH. |
| Jee et al. [40] | To compare inflammatory precursors in endothelial cells per section of a 308 km run between EIH and CON runners. | CON (n = 8, 49.7 ± 5.6) EIH (n = 8, 46.7 ± 5.4) | Blood collection pre-run and at 100 and 200 km | sVCAM-1: Increased in EIH with respect to CON at 100 and 200 km sE-selectin: Increased in EIH with respect to CON at 100 km Leukocytes: Increased in EIH with respect to CON at 308 km | Vascular resistance and shear force can increase during a 308 km run, damaging endothelial cells in runners with EIH. |
| Kim et al. [41] | To compare anti-inflammatory precursors and NO before and after a 100 km run between EIH and NCG runners. | NCG (n = 8, 53.5 ± 8.8) EIHG (n = 10, 53.7 ± 4.3) | Blood collection pre-run and at 100 km | IL-10: Decreased in EIH with respect to NCG in the resting state NO: Decreased in EIH with respect to NCG at 100 km | In EIHG, excessive exercise inhibits NO release by endothelial cells, causing blood pressure to rise excessively due to vascular constriction. |
| Park et al. [42] | To compare cardiac and inflammatory markers in the recovery phase following a 100 km run between EIH and NEBPR runners. | NEBPR (n = 11, 51.7 ± 4.3) EIH (n = 11, 52.9 ± 3.8) | Pre, 100 km | CK, nTnI: Increased in EIH with respect to NEBPR at 100 km and 24 h NT-proBNP: Increased in EIH with respect to NEBPR at 100 km and 24 and 72 h hsCRP: Increased in EIH with respect to NEBPR at 24 h | Increased inflammation and cardiac markers until the recovery phase can lead to volume and pressure overloads and restricted blood flow in the heart, leading to myocardial damage in runners with EIH. |
| Ref. | Aim | Subject | Method | Result | Conclusion |
|---|---|---|---|---|---|
| Allison et al. [25] | To assess the prognosis of subjects with exercise hypertension. | A total of 150 healthy subjects | 7.7 ± 2.9-year follow-up | High risk of major cardiovascular death in the EIH group. | Healthy, asymptomatic subjects might be at a high risk of major cardiovascular events. |
| Kurl et al. [28] | To examine the association between exercise SBP and the risk of stroke. | A total of 1026 subjects without cerebrovascular disease. | 10.4-year follow-up | The risk of stroke and ischemic stroke increased with MSBP in the exercise test and blood pressure at 2 min into the recovery phase increased. | Exercise SBP tests are recommended as additional tools in predicting future strokes. |
| Mundal et al. [29] | To investigate whether casual blood pressure and exercise SBP can predict the morbidity and mortality rates of myocardial infarction in healthy men. | Healthy males (n = 1999, 40–59 years). 31,984 patients | Sixteen-year follow-up for males who were healthy from 1972 to 1975 | Blood pressure during exercise is a stronger predictor of morbidity and mortality than casual blood pressure due to myocardial infarction. | Blood pressure values measured during an exercise stress test can be used to differentiate between moderate and severe hypertension. |
| Le et al. [43] | To investigate the association between exercise blood pressure response and CVD. | 3045 men (n = 1437, 43 ± 10 years) and women (n = 1608, 43 ± 10 years) | Measure blood pressure at stage 2 of the Bruce protocol and blood pressure during the recovery phase 20-year follow-up | Increases in SBP and DBP in the exercise stress test were associated with SVD | Low-intensity exercise and DBP in the recovery phase predicted cardiovascular disease in middle-aged adults. Exercise DBP can be a better predictor of exercise SBP. |
| Gottdiener et al. [44] | To assess the correlation between excessive blood pressure response during exercise in the absence of hypertension and LVH. | Health examination subjects (n = 39, male, 44.6 ± 8.5) | SBP ≥ 210 mmHg, SBP < 210 mmHg during maximal exercise | LVH detected in 14 of 22 men with SBP ≥ 210 mmHg. LVH was mild but accompanied by an increase in left atrium size, suggestive of impaired left ventricular filling. | Excessive blood pressure responses during an exercise stress test are associated with LVH, even in non-hypertensive subjects. |
| Jae et al. [45] | To investigate the association between MSBP during an exercise stress test and the risk of SCD in men. | Health examination subjects from 1984 to 1989 (n = 2410, 42–61 years) divided into those with CVD (n = 884) and those without (n = 1526) Investigate the correlation between MSBP (≥210 mmHg) and SCD in these subjects | Within 1–24 h after the onset of SCD symptoms, analyze data about ventricular tachycardia, atrial fibrillation, and SCD. | For men without a history of CVD, the risk of SCD is high when MSBP ≥ 210 mmHg. For men with a history of CVD, the risk of SCD is high when MSBP < 210 mmHg. | For men without a history of CVD, SCD contributes to endothelial dysfunction, inflammation, atherosclerosis, and future hypertension For men with a history of CVD, SCD is associated with reduced cardiac function |
| Kjeldsen et al. [46] | To investigate SBP during a cycle ergometer test and cardiovascular mortalities. | A total of 1999 healthy subjects (40–59 years) | 21-year follow-up | An excessive increase in SBP measured during moderate-load exercise predicts CV regardless of age, office blood pressure, and other risk factors for CV | An abnormal increase in exercise SBP can warn clinicians of a possible increase in cardiovascular risk regardless of office blood pressure |
| Kohl et al. [47] | To examine the correlation between hemodynamic response to maximal exercise, CVD, and CHD mortality. | n = 20,387 (male, 42.2 years) n = 6234 (female 41.9 years) | Mean follow-up of 8.1 years | In total, 348 men and 66 women died during the follow-up period. All-cause mortalities increased as MSBP increased and maximum heart rate decreased. | Excessive SBP or reduced heart rate during maximal exercise increases mortalities. |
| Laukkanen et al. [48] | To investigate the association between the risk of AMI and exercise SBP response. | A total of 1731 middle-aged subjects without CAD | 12.7-year follow-up | Maximal SBP elevation in a cycle ergo test is associated with the risk of myocardial infarction | The speed and extent of SBP elevation in a graded exercise test are predictors of myocardial infarction. Regular blood pressure measurements through exercise tests are important |
| Schultz et al. [49] | To review the relationships between EIH and cardiovascular events and mortality prediction. | A total of 46,314 subjects without serious CAD | 15.2 ± 4.0 years of follow-up | For every 10 mmHg increase in exercise SBP, the risk of cardiovascular events and mortality increased by 4% regardless of office blood pressure, age, and risk factors of CV. | As a risk factor, EIH is independent of CV events and deaths. |
| Skretteberg et al. [50] | To investigate whether exercise SBP is associated with CHD. | Men (n = 1392, mean 49.2 years) | Monitor changes in SBP during a cycle ergo test to assess the risk of CHD and SCD over 7 years. | An increase in exercise SBP over 7 years independently predicts an increase in mortality and the risk of CV and CDH. | High exercise SBP is a strong risk factor for CV in men. The regulation of excessive exercise blood pressure is necessary. |
| Weiss et al. [51] | To investigate whether excessive blood pressure elevation during exercise increases the risk of cardiovascular death. | Follow-up of 6578 asymptomatic patients (mean age 46 years) who showed excessive blood pressure elevation in Bruce stage 2 and a normal blood pressure group. | GXT (Bruce protocol) followed by a 20-year follow-up | Maximum exercise blood pressure in Bruce stage 2 is significantly associated with death from CVD. | It is necessary to screen non-hypertensive patients with Bruce stage 2 blood pressure > 180/90 mmHg who are at high risk of death from CVD and properly manage them. |
| Gupta et al. [52] | To investigate whether an increase in SBP is associated with CV prognosis in EST. | 6145 men Comparison between a group with SBP elevation ≤ 43 mmHg (n = 3062, 61 ± 11 years, A group) and a group with SBP elevation ≥ 44 mmHg (n = 3083, 57 ± 11 years, B group) | Mean follow-up of 6.6 years for two groups | 676 patients died from cardiovascular conditions during the follow-up period. Higher cardiovascular mortality was found in Group A than in Group B (13.7% vs. 8.2%, p < 0.001). | For EST, a ≥44 mmHg increase in SBP was associated with a 23% increase in survival rate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-J.; Park, K.-M. Possible Mechanisms for Adverse Cardiac Events Caused by Exercise-Induced Hypertension in Long-Distance Middle-Aged Runners: A Review. J. Clin. Med. 2024, 13, 2184. https://doi.org/10.3390/jcm13082184
Kim Y-J, Park K-M. Possible Mechanisms for Adverse Cardiac Events Caused by Exercise-Induced Hypertension in Long-Distance Middle-Aged Runners: A Review. Journal of Clinical Medicine. 2024; 13(8):2184. https://doi.org/10.3390/jcm13082184
Chicago/Turabian StyleKim, Young-Joo, and Kyoung-Min Park. 2024. "Possible Mechanisms for Adverse Cardiac Events Caused by Exercise-Induced Hypertension in Long-Distance Middle-Aged Runners: A Review" Journal of Clinical Medicine 13, no. 8: 2184. https://doi.org/10.3390/jcm13082184
APA StyleKim, Y.-J., & Park, K.-M. (2024). Possible Mechanisms for Adverse Cardiac Events Caused by Exercise-Induced Hypertension in Long-Distance Middle-Aged Runners: A Review. Journal of Clinical Medicine, 13(8), 2184. https://doi.org/10.3390/jcm13082184