

Topical Treatments in Atopic Dermatitis: An Expansive Review

Abstract
:1. Introduction
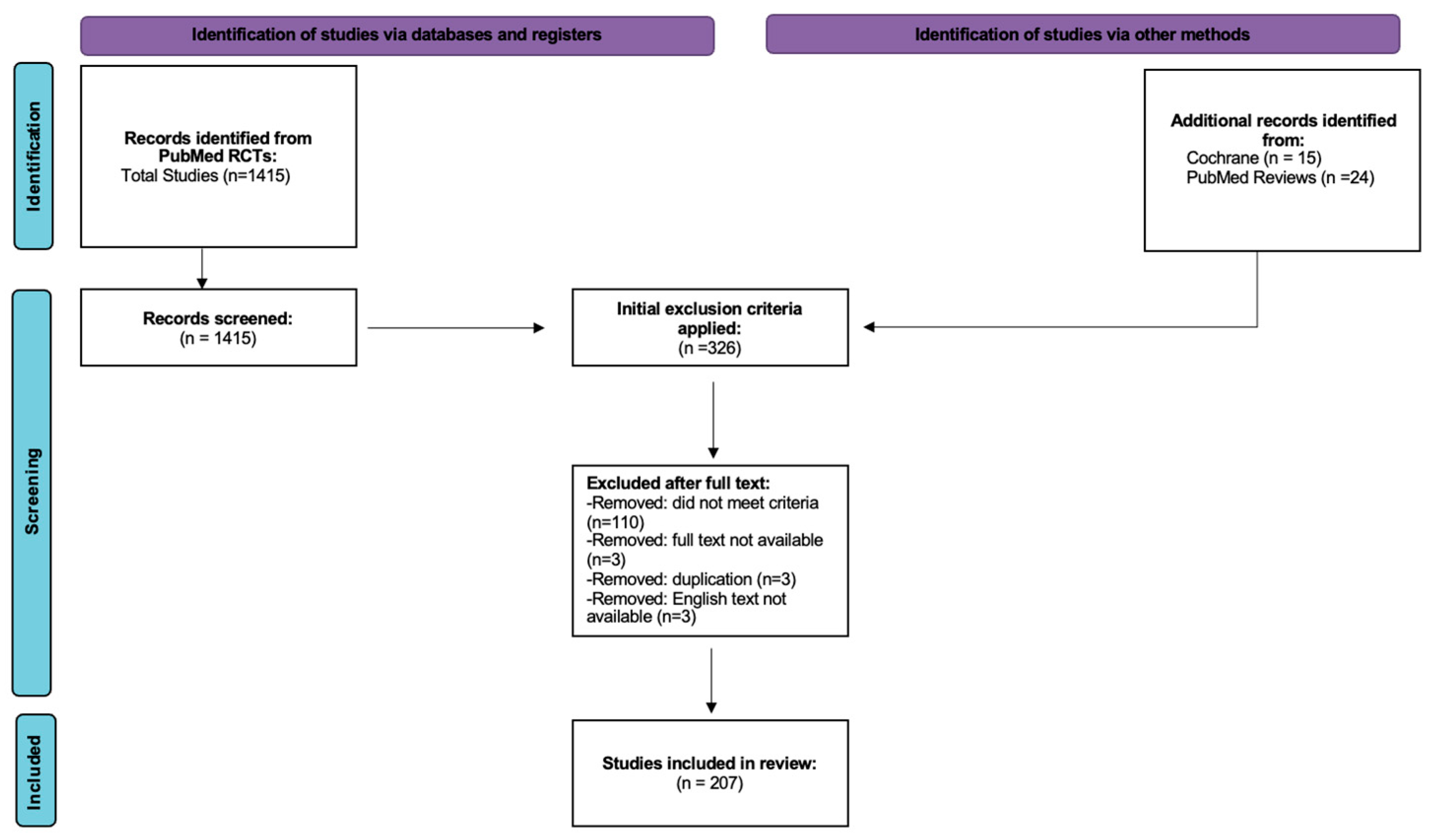
2. Materials and Methods
3. Results
3.1. Demographic Data of Studies
3.2. Commonly Utilized Treatments
3.3. Statistical Significance
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raimondo, A.; Lembo, S. Atopic Dermatitis: Epidemiology and Clinical Phenotypes. Dermatol. Pract. Concept. 2021, 11, e2021146. [Google Scholar] [CrossRef]
- Smith Begolka, W.; Chovatiya, R.; Thibau, I.J.; Silverberg, J.I. Financial Burden of Atopic Dermatitis Out-of-Pocket Health Care Expenses in the United States. Dermatitis 2021, 32, S62–S70. [Google Scholar] [CrossRef] [PubMed]
- David Boothe, W.; Tarbox, J.A.; Tarbox, M.B. Atopic Dermatitis: Pathophysiology. Manag. Atopic Dermat. Methods Chall. 2017, 1027, 21–37. [Google Scholar] [CrossRef]
- Loset, M.; Brown, S.J.; Saunes, M.; Hveem, K. Genetics of Atopic Dermatitis: From DNA Sequence to Clinical Relevance. Dermatology 2019, 235, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Galli, E.; Gianni, S.; Auricchio, G.; Brunetti, E.; Mancino, G.; Rossi, P. Atopic dermatitis and asthma. Allergy Asthma Proc. 2007, 28, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Baghoomian, W.; Grinich, E.; Leshem, Y.A.; Jacobson, M.; Simpson, E.L. The Eczema Area and Severity Index-A Practical Guide. Dermatitis 2022, 33, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.L.; Bissonnette, R.; Paller, A.S.; King, B.; Silverberg, J.I.; Reich, K.; Thyssen, J.P.; Doll, H.; Sun, L.; DeLozier, A.M.; et al. The Validated Investigator Global Assessment for Atopic Dermatitis (vIGA-AD): A clinical outcome measure for the severity of atopic dermatitis. Br. J. Dermatol. 2022, 187, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Schallreuter, K.; Levenig, C.; Berger, J.; Umbert, J.; Winkelmann, R.; Wegener, L.; Correia, O.; Chosidow, O.; Saiag, P.; Bastuji-Garin, S.; et al. Severity scoring of atopic dermatitis: The SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology 1993, 186, 23–31. [Google Scholar] [CrossRef]
- Nicol, N.H.; Boguniewicz, M. Wet Wrap Therapy in Moderate to Severe Atopic Dermatitis. Immunol. Allergy Clin. 2017, 37, 123–139. [Google Scholar] [CrossRef]
- Atherton, D.J. Topical corticosteroids in atopic dermatitis. BMJ 2003, 327, 942–943. [Google Scholar] [CrossRef]
- Musters, A.H.; Mashayekhi, S.; Harvey, J.; Axon, E.; Lax, S.J.; Flohr, C.; Drucker, A.M.; Gerbens, L.; Ferguson, J.; Ibbotson, S.; et al. Phototherapy for atopic eczema. Cochrane Database Syst. Rev. 2021, 10, CD013870. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, S.; Kamalinejad, M.; Babaie, D.; Shams, S.; Sadr, Z.; Gheysari, M.; Askari, V.R.; Rakhshandeh, H. A new topical treatment of atopic dermatitis in pediatric patients based on Ficus carica L. (Fig): A randomized, placebo-controlled clinical trial. Complement. Ther. Med. 2017, 35, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Abramovits, W.; Boguniewicz, M.; Adult Atopiclair Study, G. A multicenter, randomized, vehicle-controlled clinical study to examine the efficacy and safety of MAS063DP (Atopiclair) in the management of mild to moderate atopic dermatitis in adults. J. Drugs Dermatol. 2006, 5, 236–244. [Google Scholar] [PubMed]
- Abramovits, W.; Fleischer, A.B., Jr.; Jaracz, E.; Breneman, D. Adult patients with moderate atopic dermatitis: Tacrolimus ointment versus pimecrolimus cream. J. Drugs Dermatol. 2008, 7, 1153–1158. [Google Scholar] [PubMed]
- Abramovits, W.; Hebert, A.A.; Boguniewicz, M.; Kempers, S.E.; Tschen, E.; Jarratt, M.T.; Lucky, A.W.; Cornelison, R.L.; Swinyer, L.J.; Jones, T.M. Patient-reported outcomes from a multicenter, randomized, vehicle-controlled clinical study of MAS063DP (Atopiclair) in the management of mild-to-moderate atopic dermatitis in adults. J. Dermatol. Treat. 2008, 19, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Abramovits, W.; Oquendo, M. Hydrocortisone butyrate 0.1% lipocream in pediatric patients with atopic dermatitis. Skinmed 2010, 8, 72–79. [Google Scholar]
- Ahn, J.H.; Yun, Y.; Kim, M.H.; Ko, S.G.; Kim, K.S.; Choi, I. Exploring the efficacy and safety of topical Jaungo application in patients with atopic dermatitis: A pilot randomized, double-blind, placebo-controlled study. Complement. Ther. Med. 2018, 40, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Akerstrom, U.; Reitamo, S.; Langeland, T.; Berg, M.; Rustad, L.; Korhonen, L.; Loden, M.; Wiren, K.; Grande, M.; Skare, P.; et al. Comparison of Moisturizing Creams for the Prevention of Atopic Dermatitis Relapse: A Randomized Double-blind Controlled Multicentre Clinical Trial. Acta Derm.-Venereol. 2015, 95, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, A.; Dakoutrou, M.; Nasi, L.; Thanopoulou, I.; Kakourou, T.; Kontara, L.; Douladiris, N.; Galani, M.; Xepapadaki, P.; Doxani, C.; et al. A randomized, observer-blind, vehicle-control, multi-center clinical investigation for assessing the efficacy and tolerability of a 1% ectoine and hyaluronic acid 0.1%-containing medical device in pediatric patients with mild-to-moderate atopic dermatitis. Pediatr. Dermatol. 2023, 40, 78–83. [Google Scholar] [CrossRef]
- Amichai, B.; Grunwald, M.H. A randomized, double-blind, placebo-controlled study to evaluate the efficacy in AD of liquid soap containing 12% ammonium lactate + 20% urea. Clin. Exp. Dermatol. 2009, 34, e602–e604. [Google Scholar] [CrossRef]
- Antiga, E.; Volpi, W.; Torchia, D.; Fabbri, P.; Caproni, M. Effects of tacrolimus ointment on Toll-like receptors in atopic dermatitis. Clin. Exp. Dermatol. 2011, 36, 235–241. [Google Scholar] [CrossRef]
- Arenberger, P.; Arenbergerova, M.; Drozenova, H.; Hladikova, M.; Holcova, S. Effect of topical heparin and levomenol on atopic dermatitis: A randomized four-arm, placebo-controlled, double-blind clinical study. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Bangert, C.; Strober, B.E.; Cork, M.; Ortonne, J.P.; Luger, T.; Bieber, T.; Ferguson, A.; Ecker, R.C.; Kopp, T.; Weise-Riccardi, S.; et al. Clinical and cytological effects of pimecrolimus cream 1% after resolution of active atopic dermatitis lesions by topical corticosteroids: A randomized controlled trial. Dermatology 2011, 222, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.; Lange, N.; Matterne, U.; Meurer, M.; Braeutigam, M.; Diepgen, T.L. Efficacy of pimecrolimus 1% cream in the long term management of atopic hand dermatitis. A double-blind RCT. JDDG J. Dtsch. Dermatol. Ges. 2012, 10, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Belloni, G.; Pinelli, S.; Veraldi, S. A randomised, double-blind, vehicle-controlled study to evaluate the efficacy and safety of MAS063D (Atopiclair) in the treatment of mild to moderate atopic dermatitis. Eur. J. Dermatol. 2005, 15, 31–36. [Google Scholar] [PubMed]
- Berberian, B.J.; Breneman, D.L.; Drake, L.A.; Gratton, D.; Raimir, S.S.; Phillips, S.; Sulica, V.I.; Bernstein, J.E. The addition of topical doxepin to corticosteroid therapy: An improved treatment regimen for atopic dermatitis. Int. J. Dermatol. 1999, 38, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Berth-Jones, J.; Damstra, R.J.; Golsch, S.; Livden, J.K.; Van Hooteghem, O.; Allegra, F.; Parker, C.A.; Multinational Study, G. Twice weekly fluticasone propionate added to emollient maintenance treatment to reduce risk of relapse in atopic dermatitis: Randomised, double blind, parallel group study. BMJ 2003, 326, 1367. [Google Scholar] [CrossRef] [PubMed]
- Berth-Jones, J.; Pollock, I.; Hearn, R.M.; Lewis-Jones, S.; Goodfield, M.; Griffiths, C.E.; Gulati, R.; McHenry, P.; Abdullah, A.; Ott, J.; et al. A randomised, controlled trial of a 4% cutaneous emulsion of sodium cromoglicate in treatment of atopic dermatitis in children. J. Dermatol. Treat. 2015, 26, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, P.; Theunis, J.; Casas, C.; Villeneuve, C.; Patrizi, A.; Phulpin, C.; Bacquey, A.; Redoules, D.; Mengeaud, V.; Schmitt, A.M. Effects of a New Emollient-Based Treatment on Skin Microflora Balance and Barrier Function in Children with Mild Atopic Dermatitis. Pediatr. Dermatol. 2016, 33, 165–171. [Google Scholar] [CrossRef]
- Bieber, T.; Vick, K.; Folster-Holst, R.; Belloni-Fortina, A.; Stadtler, G.; Worm, M.; Arcangeli, F. Efficacy and safety of methylprednisolone aceponate ointment 0.1% compared to tacrolimus 0.03% in children and adolescents with an acute flare of severe atopic dermatitis. Allergy 2007, 62, 184–189. [Google Scholar] [CrossRef]
- Bigliardi, P.L.; Stammer, H.; Jost, G.; Rufli, T.; Buchner, S.; Bigliardi-Qi, M. Treatment of pruritus with topically applied opiate receptor antagonist. J. Am. Acad. Dermatol. 2007, 56, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Chen, G.; Bolduc, C.; Maari, C.; Lyle, M.; Tang, L.; Webster, J.; Zhou, Y. Efficacy and safety of topical WBI-1001 in the treatment of atopic dermatitis: Results from a phase 2A, randomized, placebo-controlled clinical trial. Arch. Dermatol. 2010, 146, 446–449. [Google Scholar] [CrossRef]
- Bissonnette, R.; Maari, C.; Provost, N.; Bolduc, C.; Nigen, S.; Rougier, A.; Seite, S. A double-blind study of tolerance and efficacy of a new urea-containing moisturizer in patients with atopic dermatitis. J. Cosmet. Dermatol. 2010, 9, 16–21. [Google Scholar] [CrossRef]
- Bissonnette, R.; Papp, K.A.; Poulin, Y.; Gooderham, M.; Raman, M.; Mallbris, L.; Wang, C.; Purohit, V.; Mamolo, C.; Papacharalambous, J.; et al. Topical tofacitinib for atopic dermatitis: A phase IIa randomized trial. Br. J. Dermatol. 2016, 175, 902–911. [Google Scholar] [CrossRef]
- Bissonnette, R.; Poulin, Y.; Zhou, Y.; Tan, J.; Hong, H.C.; Webster, J.; Ip, W.; Tang, L.; Lyle, M. Efficacy and safety of topical WBI-1001 in patients with mild to severe atopic dermatitis: Results from a 12-week, multicentre, randomized, placebo-controlled double-blind trial. Br. J. Dermatol. 2012, 166, 853–860. [Google Scholar] [CrossRef]
- Blauvelt, A.; Kircik, L.; Papp, K.A.; Simpson, E.L.; Silverberg, J.I.; Kim, B.S.; Kwatra, S.G.; Kuligowski, M.E.; Venturanza, M.E.; Wei, S.; et al. Rapid pruritus reduction with ruxolitinib cream treatment in patients with atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Bleehen, S.S.; Chu, A.C.; Hamann, I.; Holden, C.; Hunter, J.A.; Marks, R. Fluticasone propionate 0.05% cream in the treatment of atopic eczema: A multicentre study comparing once-daily treatment and once-daily vehicle cream application versus twice-daily treatment. Br. J. Dermatol. 1995, 133, 592–597. [Google Scholar] [CrossRef]
- Bloudek, L.; Eichenfield, L.F.; Silverberg, J.I.; Joish, V.N.; Lofland, J.H.; Sun, K.; Augustin, M.; Migliaccio-Walle, K.; Sullivan, S.D. Impact of Ruxolitinib Cream on Work Productivity and Activity Impairment and Associated Indirect Costs in Patients with Atopic Dermatitis: Pooled Results From Two Phase III Studies. Am. J. Clin. Dermatol. 2023, 24, 109–117. [Google Scholar] [CrossRef]
- Boguniewicz, M.; Fiedler, V.C.; Raimer, S.; Lawrence, I.D.; Leung, D.Y.; Hanifin, J.M.; Pediatric Tacrolimus Study Group. A randomized, vehicle-controlled trial of tacrolimus ointment for treatment of atopic dermatitis in children. J. Allergy Clin. Immunol. 1998, 102, 637–644. [Google Scholar] [CrossRef]
- Boguniewicz, M.; Zeichner, J.A.; Eichenfield, L.F.; Hebert, A.A.; Jarratt, M.; Lucky, A.W.; Paller, A.S. MAS063DP is effective monotherapy for mild to moderate atopic dermatitis in infants and children: A multicenter, randomized, vehicle-controlled study. J. Pediatr. 2008, 152, 854–859. [Google Scholar] [CrossRef]
- Boralevi, F.; Saint Aroman, M.; Delarue, A.; Raudsepp, H.; Kaszuba, A.; Bylaite, M.; Tiplica, G.S. Long-term emollient therapy improves xerosis in children with atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Breneman, D.; Fleischer, A.B., Jr.; Abramovits, W.; Zeichner, J.; Gold, M.H.; Kirsner, R.S.; Shull, T.F.; Crowe, A.W.; Jaracz, E.; Hanifin, J.M.; et al. Intermittent therapy for flare prevention and long-term disease control in stabilized atopic dermatitis: A randomized comparison of 3-times-weekly applications of tacrolimus ointment versus vehicle. J. Am. Acad. Dermatol. 2008, 58, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Breneman, D.; Fleischer, A.B., Jr.; Kaplan, D.; Lebwohl, M.; Miller, B.; Pariser, D.; Rist, T.; Swinyer, L.; Liu, Y.; Foley, V. Clobetasol propionate 0.05% lotion in the treatment of moderate to severe atopic dermatitis: A randomized evaluation versus clobetasol propionate emollient cream. J. Drugs Dermatol. 2005, 4, 330–336. [Google Scholar] [PubMed]
- Broberg, A.; Faergemann, J. Topical antimycotic treatment of atopic dermatitis in the head/neck area. A double-blind randomised study. Acta Derm.-Venereol. 1995, 75, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Zhao, Y.; Zheng, M.; Zhang, F.; Sun, Q.; Liu, Q.; Hu, J.; Shen, J.; Zhang, J. A multi-center, double-blind, randomized, placebo- and positive-controlled phase II clinical study of benvitimod for the treatment of atopic dermatitis. Chin. Med. J. 2023, 136, 251–252. [Google Scholar] [CrossRef] [PubMed]
- Callender, V.D.; Alexis, A.F.; Stein Gold, L.F.; Lebwohl, M.G.; Paller, A.S.; Desai, S.R.; Tan, H.; Ports, W.C.; Zielinski, M.A.; Tallman, A.M. Efficacy and Safety of Crisaborole Ointment, 2%, for the Treatment of Mild-to-Moderate Atopic Dermatitis Across Racial and Ethnic Groups. Am. J. Clin. Dermatol. 2019, 20, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Canpolat, F.; Erkocoglu, M.; Tezer, H.; Kocabas, C.N.; Kandi, B. Hydrocortisone acetate alone or combined with mupirocin for atopic dermatitis in infants under two years of age—A randomized double blind pilot trial. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1989–1993. [Google Scholar] [PubMed]
- Capone, K.; Kirchner, F.; Klein, S.L.; Tierney, N.K. Effects of Colloidal Oatmeal Topical Atopic Dermatitis Cream on Skin Microbiome and Skin Barrier Properties. J. Drugs Dermatol. 2020, 19, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Cato, A.; Swinehart, J.M.; Griffin, E.I.; Sutton, L.; Kaplan, A.S. Azone enhances clinical effectiveness of an optimized formulation of triamcinolone acetonide in atopic dermatitis. Int. J. Dermatol. 2001, 40, 232–236. [Google Scholar] [CrossRef]
- Chapman, M.S.; Schachner, L.A.; Breneman, D.; Boguniewicz, M.; Gold, M.H.; Shull, T.; Linowski, G.J.; Jaracz, E.; Group, U.S.T.O.S. Tacrolimus ointment 0.03% shows efficacy and safety in pediatric and adult patients with mild to moderate atopic dermatitis. J. Am. Acad. Dermatol. 2005, 53, S177–S185. [Google Scholar] [CrossRef]
- Chung, B.Y.; Kim, H.O.; Kim, J.H.; Cho, S.I.; Lee, C.H.; Park, C.W. The proactive treatment of atopic dermatitis with tacrolimus ointment in Korean patients: A comparative study between once-weekly and thrice-weekly applications. Br. J. Dermatol. 2013, 168, 908–910. [Google Scholar] [CrossRef]
- Czarnowicki, T.; Dohlman, A.B.; Malik, K.; Antonini, D.; Bissonnette, R.; Chan, T.C.; Zhou, L.; Wen, H.C.; Estrada, Y.; Xu, H.; et al. Effect of short-term liver X receptor activation on epidermal barrier features in mild to moderate atopic dermatitis: A randomized controlled trial. Ann. Allergy Asthma Immunol. 2018, 120, 631–640.e11. [Google Scholar] [CrossRef] [PubMed]
- Dang, Y.; Yang, L.; Jia, Y.; Zhu, D. Clinical efficacy of mucopolysaccharide polysulfate ointment combined with desonide ointment in treatment of infantile eczema. Pak. J. Pharm. Sci. 2019, 32, 1423–1426. [Google Scholar] [PubMed]
- De Belilovsky, C.; Roo-Rodriguez, E.; Baudouin, C.; Menu, F.; Chadoutaud, B.; Msika, P. Natural peroxisome proliferator-activated receptor-alpha agonist cream demonstrates similar therapeutic response to topical steroids in atopic dermatitis. J. Dermatol. Treat. 2011, 22, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Del Rosso, J.Q.; Bhambri, S. Daily application of fluocinonide 0.1% cream for the treatment of atopic dermatitis. J. Clin. Aesthet. Dermatol. 2009, 2, 24–32. [Google Scholar]
- Doss, N.; Kamoun, M.R.; Dubertret, L.; Cambazard, F.; Remitz, A.; Lahfa, M.; de Prost, Y. Efficacy of tacrolimus 0.03% ointment as second-line treatment for children with moderate-to-severe atopic dermatitis: Evidence from a randomized, double-blind non-inferiority trial vs. fluticasone 0.005% ointment. Pediatr. Allergy Immunol. 2010, 21, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Doss, N.; Reitamo, S.; Dubertret, L.; Fekete, G.L.; Kamoun, M.R.; Lahfa, M.; Ortonne, J.P. Superiority of tacrolimus 0.1% ointment compared with fluticasone 0.005% in adults with moderate to severe atopic dermatitis of the face: Results from a randomized, double-blind trial. Br. J. Dermatol. 2009, 161, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Dou, X.; Liu, L.; Zhu, X.; Wen, W.; Ni, C.; Zhao, Y.; He, Z.; Li, H.; Sun, Q.; Yang, Q.; et al. Safety and efficacy of Pimecrolimus in atopic dermatitis among Chinese infants: A sub-group analysis of a five-year open-label study. J. Dermatol. Treat. 2023, 34, 2229464. [Google Scholar] [CrossRef]
- Draelos, Z.D. The effect of ceramide-containing skin care products on eczema resolution duration. Cutis 2008, 81, 87–91. [Google Scholar]
- Draelos, Z.D.; Traub, M.; Gold, M.H.; Green, L.J.; Amster, M.; Barak-Shinar, D.; Kircik, L.H. Efficacy of Topical Botanical Treatment of Children With Mild to Moderate Atopic Dermatitis. J. Drugs Dermatol. 2019, 18, 1038–1045. [Google Scholar]
- Drake, L.; Prendergast, M.; Maher, R.; Breneman, D.; Korman, N.; Satoi, Y.; Beusterien, K.M.; Lawrence, I. The impact of tacrolimus ointment on health-related quality of life of adult and pediatric patients with atopic dermatitis. J. Am. Acad. Dermatol. 2001, 44, S65–S72. [Google Scholar] [CrossRef] [PubMed]
- Drake, L.A.; Fallon, J.D.; Sober, A.; The Doxepin Study Group. Relief of pruritus in patients with atopic dermatitis after treatment with topical doxepin cream. J. Am. Acad. Dermatol. 1994, 31, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.M.; Bibawy, D.; Matthews, S.; Tongue, N.; Arshad, S.H.; Lodrup Carlsen, K.; Oymar, K.; Pollock, I.; Clifford, R.; Thomas, A.; et al. Long-term use of a 4% sodium cromoglicate cutaneous emulsion in the treatment of moderate to severe atopic dermatitis in children. J. Dermatol. Treat. 2015, 26, 541–547. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Gower, R.G.; Xu, J.; Alam, M.S.; Su, J.C.; Myers, D.E.; Sanders, P.; Vlahos, B.; Zang, C.; Lan, J.; et al. Once-Daily Crisaborole Ointment, 2%, as a Long-Term Maintenance Treatment in Patients Aged ≥3 Months with Mild-to-Moderate Atopic Dermatitis: A 52-Week Clinical Study. Am. J. Clin. Dermatol. 2023, 24, 623–635. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Yosipovitch, G.; Stein Gold, L.F.; Kalabis, M.; Zang, C.; Vlahos, B.; Sanders, P.; Myers, D.E.; Bushmakin, A.G.; Cappelleri, J.C.; et al. Improvement in disease severity and pruritus outcomes with crisaborole ointment, 2%, by baseline atopic dermatitis severity in children and adolescents with mild-to-moderate atopic dermatitis. Pediatr. Dermatol. 2020, 37, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Lucky, A.W.; Boguniewicz, M.; Langley, R.G.; Cherill, R.; Marshall, K.; Bush, C.; Graeber, M. Safety and efficacy of pimecrolimus (ASM 981) cream 1% in the treatment of mild and moderate atopic dermatitis in children and adolescents. J. Am. Acad. Dermatol. 2002, 46, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Lucky, A.W.; Langley, R.G.; Lynde, C.; Kaufmann, R.; Todd, G.; Lindsley, L.; Barbier, N.; Felser, J.M. Use of pimecrolimus cream 1% (Elidel) in the treatment of atopic dermatitis in infants and children: The effects of ethnic origin and baseline disease severity on treatment outcome. Int. J. Dermatol. 2005, 44, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Miller, B.H.; Cutivate Lotion Study, G. Two randomized, double-blind, placebo-controlled studies of fluticasone propionate lotion 0.05% for the treatment of atopic dermatitis in subjects from 3 months of age. J. Am. Acad. Dermatol. 2006, 54, 715–717. [Google Scholar] [CrossRef]
- Evangelista, M.T.; Abad-Casintahan, F.; Lopez-Villafuerte, L. The effect of topical virgin coconut oil on SCORAD index, transepidermal water loss, and skin capacitance in mild to moderate pediatric atopic dermatitis: A randomized, double-blind, clinical trial. Int. J. Dermatol. 2014, 53, 100–108. [Google Scholar] [CrossRef]
- Fleischer, A.B., Jr.; Abramovits, W.; Breneman, D.; Jaracz, E. Tacrolimus ointment is more effective than pimecrolimus cream in adult patients with moderate to very severe atopic dermatitis. J. Dermatol. Treat. 2007, 18, 151–157. [Google Scholar] [CrossRef]
- Foelster Holst, R.; Reitamo, S.; Yankova, R.; Worm, M.; Kadurina, M.; Thaci, D.; Bieber, T.; Tsankov, N.; Enk, A.; Luger, T.; et al. The novel protease inhibitor SRD441 ointment is not effective in the treatment of adult subjects with atopic dermatitis: Results of a randomized, vehicle-controlled study. Allergy 2010, 65, 1594–1599. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.; Johnson, A.; Chen, M.; Abrams, K. Improvement in pruritus in children with atopic dermatitis using pimecrolimus cream 1%. Cutis 2007, 79, 65–72. [Google Scholar] [PubMed]
- Furue, M.; Kitahara, Y.; Akama, H.; Hojo, S.; Hayashi, N.; Nakagawa, H.; The JAPANESE E6005 Study Investigators. Safety and efficacy of topical E6005, a phosphodiesterase 4 inhibitor, in Japanese adult patients with atopic dermatitis: Results of a randomized, vehicle-controlled, multicenter clinical trial. J. Dermatol. 2014, 41, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Li, Y.; Tan, Y.; Liu, W.; Ouaddi, S.; McCoy, J.; Kovacevic, M.; Situm, M.; Stanimirovic, A.; Li, M.; et al. Novel cannabidiol aspartame combination treatment (JW-100) significantly reduces ISGA score in atopic dermatitis: Results from a randomized double-blinded placebo-controlled interventional study. J. Cosmet. Dermatol. 2022, 21, 1647–1650. [Google Scholar] [CrossRef] [PubMed]
- Gayraud, F.; Sayag, M.; Jourdan, E. Efficacy and tolerance assessment of a new type of dermocosmetic in infants and children with moderate atopic dermatitis. J. Cosmet. Dermatol. 2015, 14, 107–112. [Google Scholar] [CrossRef]
- Giordano-Labadie, F.; Cambazard, F.; Guillet, G.; Combemale, P.; Mengeaud, V. Evaluation of a new moisturizer (Exomega milk) in children with atopic dermatitis. J. Dermatol. Treat. 2006, 17, 78–81. [Google Scholar] [CrossRef]
- Glazenburg, E.J.; Wolkerstorfer, A.; Gerretsen, A.L.; Mulder, P.G.; Oranje, A.P. Efficacy and safety of fluticasone propionate 0.005% ointment in the long-term maintenance treatment of children with atopic dermatitis: Differences between boys and girls? Pediatr. Allergy Immunol. 2009, 20, 59–66. [Google Scholar] [CrossRef]
- Gollnick, H.; Kaufmann, R.; Stough, D.; Heikkila, H.; Andriano, K.; Grinienko, A.; Jimenez, P.; Pimecrolimus Cream 1% in Eczema: Prevention of Progression Multicentre Investigator Study Group. Pimecrolimus cream 1% in the long-term management of adult atopic dermatitis: Prevention of flare progression. A randomized controlled trial. Br. J. Dermatol. 2008, 158, 1083–1093. [Google Scholar] [CrossRef]
- Gooderham, M.; Kircik, L.; Zirwas, M.; Lee, M.; Kempers, S.; Draelos, Z.; Ferris, L.; Jones, T.; Saint-Cyr Proulx, E.; Bissonnette, R.; et al. The Safety and Efficacy of Roflumilast Cream 0.15% and 0.05% in Patients With Atopic Dermatitis: Randomized, Double-Blind, Phase 2 Proof of Concept Study. J. Drugs Dermatol. 2023, 22, 139–147. [Google Scholar] [CrossRef]
- Grimalt, R.; Mengeaud, V.; Cambazard, F.; Study Investigators, G. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: A randomized controlled study. Dermatology 2007, 214, 61–67. [Google Scholar] [CrossRef]
- Gueniche, A.; Knaudt, B.; Schuck, E.; Volz, T.; Bastien, P.; Martin, R.; Rocken, M.; Breton, L.; Biedermann, T. Effects of nonpathogenic gram-negative bacterium Vitreoscilla filiformis lysate on atopic dermatitis: A prospective, randomized, double-blind, placebo-controlled clinical study. Br. J. Dermatol. 2008, 159, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Ramam, M.; Sharma, V.K.; Sethuraman, G.; Pandey, R.M.; Bhari, N. Evaluation of a paraffin-based moisturizer compared to a ceramide-based moisturizer in children with atopic dermatitis: A double-blind, randomized controlled trial. Pediatr. Dermatol. 2023, 40, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Handa, S.; Chandrasegaran, A.; Kanwar, A.; Mahajan, R. Comparing the Effectiveness of Topical Fluticasone 0.05% Cream versus Topical Tacrolimus 0.1% Ointment in Pediatric Atopic Dermatitis A Randomized Control Trial. Indian. J. Paediatr. Dermatol. 2022, 23, 111–115. [Google Scholar] [CrossRef]
- Hanifin, J.; Gupta, A.K.; Rajagopalan, R. Intermittent dosing of fluticasone propionate cream for reducing the risk of relapse in atopic dermatitis patients. Br. J. Dermatol. 2002, 147, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Ellis, C.N.; Frieden, I.J.; Folster-Holst, R.; Stein Gold, L.F.; Secci, A.; Smith, A.J.; Zhao, C.; Kornyeyeva, E.; Eichenfield, L.F. OPA-15406, a novel, topical, nonsteroidal, selective phosphodiesterase-4 (PDE4) inhibitor, in the treatment of adult and adolescent patients with mild to moderate atopic dermatitis (AD): A phase-II randomized, double-blind, placebo-controlled study. J. Am. Acad. Dermatol. 2016, 75, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Ling, M.R.; Langley, R.; Breneman, D.; Rafal, E. Tacrolimus ointment for the treatment of atopic dermatitis in adult patients: Part I, efficacy. J. Am. Acad. Dermatol. 2001, 44, S28–S38. [Google Scholar] [CrossRef] [PubMed]
- Hebert, A.A.; Cook-Bolden, F.E.; Basu, S.; Calvarese, B.; Trancik, R.J.; Desonide Hydrogel Study, G. Safety and efficacy of desonide hydrogel 0.05% in pediatric subjects with atopic dermatitis. J. Drugs Dermatol. 2007, 6, 175–181. [Google Scholar] [PubMed]
- Herzog, J.L.; Solomon, J.A.; Draelos, Z.; Fleischer, A., Jr.; Stough, D.; Wolf, D.I.; Abramovits, W.; Werschler, W.; Green, E.; Duffy, M.; et al. A randomized, double-blind, vehicle-controlled crossover study to determine the anti-pruritic efficacy, safety and local dermal tolerability of a topical formulation (srd174 cream) of the long-acting opiod antagonist nalmefene in subjects with atopic dermatitis. J. Drugs Dermatol. 2011, 10, 853–860. [Google Scholar]
- Hiratsuka, S.; Yoshida, A.; Ishioka, C.; Kimata, H. Enhancement of in vitro spontaneous IgE production by topical steroids in patients with atopic dermatitis. J. Allergy Clin. Immunol. 1996, 98, 107–113. [Google Scholar] [CrossRef]
- Hlela, C.; Lunjani, N.; Gumedze, F.; Kakande, B.; Khumalo, N.P. Affordable moisturisers are effective in atopic eczema: A randomised controlled trial. S. Afr. Med. J. 2015, 105, 780–784. [Google Scholar] [CrossRef]
- Ho, V.C.; Gupta, A.; Kaufmann, R.; Todd, G.; Vanaclocha, F.; Takaoka, R.; Folster-Holst, R.; Potter, P.; Marshall, K.; Thurston, M.; et al. Safety and efficacy of nonsteroid pimecrolimus cream 1% in the treatment of atopic dermatitis in infants. J. Pediatr. 2003, 142, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, P.H.; Lee, K.H.; Jautova, J.; Wohlrab, J.; Guettner, A.; Mizutani, G.; Hultsch, T. The treatment of facial atopic dermatitis in children who are intolerant of, or dependent on, topical corticosteroids: A randomized, controlled clinical trial. Br. J. Dermatol. 2009, 160, 415–422. [Google Scholar] [CrossRef]
- Sikder, M.A.U.; Al Mamun, S.; Khan, R.M.; Chowdhury, A.H.; Khan, H.M.; Hoque, M.M. Topical 0.03% tacrolimus ointment, 0.05% clobetasone butyrate cream alone and their combination in older children with atopic dermatitis—An open randomized comparative study. J. Pak. Assoc. Dermatol. 2005, 15, 304–312. [Google Scholar]
- Horev, A.; Sher, M.; Weissmann, S.; Golan, L.; Horev, A. Medihoney Derma Cream Treatment for Mild to Moderate Atopic Dermatitis in Children: An Open-Label Randomized Pilot Study. Dermatitis 2022, 33, S147–S149. [Google Scholar] [CrossRef] [PubMed]
- Iraji, F.; Farhadi, S.; Faghihi, G.; Mokhtari, F.; Basiri, A.; Jafari-Koshki, T.; Nilforoushzadeh, M.A. Efficacy of topical azathioprine and betamethasone versus betamethasone-only emollient cream in 2–18 years old patients with moderate-to-severe atopic dermatitis: A randomized controlled trial. Adv. Biomed. Res. 2015, 4, 228. [Google Scholar] [CrossRef]
- Jacobson, M.E.; Myles, I.A.; Paller, A.S.; Eichenfield, L.F.; Simpson, E.L. A Randomized, Double-Blind, Placebo-Controlled, Multicenter, 16-Week Trial to Evaluate the Efficacy and Safety of FB-401 in Children, Adolescents, and Adult Subjects (Ages 2 Years and Older) with Mild-to-Moderate Atopic Dermatitis. Dermatology 2024, 240, 85–94. [Google Scholar] [CrossRef]
- Jorizzo, J.; Levy, M.; Lucky, A.; Shavin, J.; Goldberg, G.; Dunlap, F.; Hinds, A.; Strelka, L.; Baker, M.; Tuley, M.; et al. Multicenter trial for long-term safety and efficacy comparison of 0.05% desonide and 1% hydrocortisone ointments in the treatment of atopic dermatitis in pediatric patients. J. Am. Acad. Dermatol. 1995, 33, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Kapp, A.; Papp, K.; Bingham, A.; Folster-Holst, R.; Ortonne, J.P.; Potter, P.C.; Gulliver, W.; Paul, C.; Molloy, S.; Barbier, N.; et al. Long-term management of atopic dermatitis in infants with topical pimecrolimus, a nonsteroid anti-inflammatory drug. J. Allergy Clin. Immunol. 2002, 110, 277–284. [Google Scholar] [CrossRef]
- Kasrae, H.; Amiri Farahani, L.; Yousefi, P. Efficacy of topical application of human breast milk on atopic eczema healing among infants: A randomized clinical trial. Int. J. Dermatol. 2015, 54, 966–971. [Google Scholar] [CrossRef]
- Kaufmann, R.; Bieber, T.; Helgesen, A.L.; Andersen, B.L.; Luger, T.; Poulin, Y.; Al-Hafidh, J.; Paul, C.; multicentre investigator group. Onset of pruritus relief with pimecrolimus cream 1% in adult patients with atopic dermatitis: A randomized trial. Allergy 2006, 61, 375–381. [Google Scholar] [CrossRef]
- Kaufmann, R.; Folster-Holst, R.; Hoger, P.; Thaci, D.; Loffler, H.; Staab, D.; Brautigam, M.; The CASM981CDE04-Study Group. Onset of action of pimecrolimus cream 1% in the treatment of atopic eczema in infants. J. Allergy Clin. Immunol. 2004, 114, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Kempers, S.; Boguniewicz, M.; Carter, E.; Jarratt, M.; Pariser, D.; Stewart, D.; Stiller, M.; Tschen, E.; Chon, K.; Wisseh, S.; et al. A randomized investigator-blinded study comparing pimecrolimus cream 1% with tacrolimus ointment 0.03% in the treatment of pediatric patients with moderate atopic dermatitis. J. Am. Acad. Dermatol. 2004, 51, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Howell, M.D.; Sun, K.; Papp, K.; Nasir, A.; Kuligowski, M.E.; Investigators, I.S. Treatment of atopic dermatitis with ruxolitinib cream (JAK1/JAK2 inhibitor) or triamcinolone cream. J. Allergy Clin. Immunol. 2020, 145, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Sun, K.; Papp, K.; Venturanza, M.; Nasir, A.; Kuligowski, M.E. Effects of ruxolitinib cream on pruritus and quality of life in atopic dermatitis: Results from a phase 2, randomized, dose-ranging, vehicle- and active-controlled study. J. Am. Acad. Dermatol. 2020, 82, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Kimata, H.; Igarashi, M. Topical cromolyn (disodium cromoglycate) solution in the treatment of young children with atopic dermatitis. Clin. Exp. Allergy 1990, 20, 281–283. [Google Scholar] [CrossRef]
- Kimball, A.B.; Gold, M.H.; Zib, B.; Davis, M.W.; Clobetasol Propionate Emulsion Formulation Foam Phase III Clinical Study Group. Clobetasol propionate emulsion formulation foam 0.05%: Review of phase II open-label and phase III randomized controlled trials in steroid-responsive dermatoses in adults and adolescents. J. Am. Acad. Dermatol. 2008, 59, 448–454.e1. [Google Scholar] [CrossRef]
- Kirsner, R.S.; Heffernan, M.P.; Antaya, R. Safety and efficacy of tacrolimus ointment versus pimecrolimus cream in the treatment of patients with atopic dermatitis previously treated with corticosteroids. Acta Derm. Venereol. 2010, 90, 58–64. [Google Scholar] [CrossRef]
- Kohn, L.L.; Kang, Y.; Antaya, R.J. A randomized, controlled trial comparing topical steroid application to wet versus dry skin in children with atopic dermatitis (AD). J. Am. Acad. Dermatol. 2016, 75, 306–311. [Google Scholar] [CrossRef]
- Korting, H.C.; Schollmann, C.; Cholcha, W.; Wolff, L.; Collaborative Study, G. Efficacy and tolerability of pale sulfonated shale oil cream 4% in the treatment of mild to moderate atopic eczema in children: A multicentre, randomized vehicle-controlled trial. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.H.; Lim, C.J.; Jung, J.; Kim, H.J.; Park, K.; Shin, J.W.; Huh, C.H.; Park, K.C.; Na, J.I. The effect of autophagy-enhancing peptide in moisturizer on atopic dermatitis: A randomized controlled trial. J. Dermatol. Treat. 2019, 30, 558–564. [Google Scholar] [CrossRef]
- Namazova-Baranova, L.S.; Vishneva, E.A.; Torshhoeva, R.M.; Dzagoeva, Z.N.; Alexeeva, A.A.; Levina, J.G. Non-steroidal Topical Medications in the Treatment of Atopic Dermatitis in Children. Pediatr. Pharmacol. 2012, 9, 66–70. [Google Scholar] [CrossRef]
- Landis, M.N.; Arya, M.; Smith, S.; Draelos, Z.; Usdan, L.; Tarabar, S.; Pradhan, V.; Aggarwal, S.; Banfield, C.; Peeva, E.; et al. Efficacy and safety of topical brepocitinib for the treatment of mild-to-moderate atopic dermatitis: A phase IIb, randomized, double-blind, vehicle-controlled, dose-ranging and parallel-group study. Br. J. Dermatol. 2022, 187, 878–887. [Google Scholar] [CrossRef]
- Langley, R.G.; Eichenfield, L.F.; Lucky, A.W.; Boguniewicz, M.; Barbier, N.; Cherill, R. Sustained efficacy and safety of pimecrolimus cream 1% when used long-term (up to 26 weeks) to treat children with atopic dermatitis. Pediatr. Dermatol. 2008, 25, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; The mometasone furoate study group. Efficacy and safety of fluticasone propionate ointment, 0.005%, in the treatment of eczema. Cutis 1996, 57, 62–68. [Google Scholar]
- Lebwohl, M. A comparison of once-daily application of mometasone furoate 0.1% cream compared with twice-daily hydrocortisone valerate 0.2% cream in pediatric atopic dermatitis patients who failed to respond to hydrocortisone. Int. J. Dermatol. 1999, 38, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.W.; Won, C.H.; Jung, K.; Nam, H.J.; Choi, G.; Park, Y.H.; Park, M.; Kim, B. Efficacy and safety of PAC-14028 cream—A novel, topical, nonsteroidal, selective TRPV1 antagonist in patients with mild-to-moderate atopic dermatitis: A phase IIb randomized trial. Br. J. Dermatol. 2019, 180, 1030–1038. [Google Scholar] [CrossRef]
- Leung, D.Y.; Hanifin, J.M.; Pariser, D.M.; Barber, K.A.; Langley, R.G.; Schlievert, P.M.; Abrams, B.; Hultsch, T. Effects of pimecrolimus cream 1% in the treatment of patients with atopic dermatitis who demonstrate a clinical insensitivity to topical corticosteroids: A randomized, multicentre vehicle-controlled trial. Br. J. Dermatol. 2009, 161, 435–443. [Google Scholar] [CrossRef]
- Lin, Y.K.; Chang, S.H.; Yang, C.Y.; See, L.C.; Lee, B.H.; Shih, I.H. Efficacy and safety of indigo naturalis ointment in Treating Atopic Dermatitis: A randomized clinical trial. J. Ethnopharmacol. 2020, 250, 112477. [Google Scholar] [CrossRef]
- Ling, M.; Gottlieb, A.; Pariser, D.; Caro, I.; Stewart, D.; Scott, G.; Abrams, K. A randomized study of the safety, absorption and efficacy of pimecrolimus cream 1% applied twice or four times daily in patients with atopic dermatitis. J. Dermatol. Treat. 2005, 16, 142–148. [Google Scholar] [CrossRef]
- Lisante, T.A.; Kizoulis, M.; Nunez, C.; Hartman, C.L. A 1% colloidal oatmeal OTC cream is clinically effective for the management of mild to moderate atopic dermatitis in Black or African American children. J. Dermatol. Treat. 2023, 34, 2241587. [Google Scholar] [CrossRef]
- Lisante, T.A.; Nunez, C.; Zhang, P. Efficacy and safety of an over-the-counter 1% colloidal oatmeal cream in the management of mild to moderate atopic dermatitis in children: A double-blind, randomized, active-controlled study. J. Dermatol. Treat. 2017, 28, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Ong, G. A randomized, open-label study to evaluate an intermittent dosing regimen of fluticasone propionate 0.05% cream in combination with regular emollient skin care in reducing the risk of relapse in pediatric patients with stabilized atopic dermatitis. J. Dermatol. Treat. 2018, 29, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhou, Q.; Dai, W.; Wang, S.; Liang, Y.; Li, Y.; Shen, C.; Li, D.; Li, Y.; Jiao, L.; et al. Is antibiotics prescription needed in infants with topical corticosteroids treatment for moderate-to-severe atopic dermatitis? Dermatol. Ther. 2020, 33, e14215. [Google Scholar] [CrossRef]
- Loden, M.; Andersson, A.C.; Anderson, C.; Bergbrant, I.M.; Frodin, T.; Ohman, H.; Sandstrom, M.H.; Sarnhult, T.; Voog, E.; Stenberg, B.; et al. A double-blind study comparing the effect of glycerin and urea on dry, eczematous skin in atopic patients. Acta Derm. Venereol. 2002, 82, 45–47. [Google Scholar] [CrossRef]
- Luger, T.A.; Lahfa, M.; Folster-Holst, R.; Gulliver, W.P.; Allen, R.; Molloy, S.; Barbier, N.; Paul, C.; Bos, J.D. Long-term safety and tolerability of pimecrolimus cream 1% and topical corticosteroids in adults with moderate to severe atopic dermatitis. J. Dermatol. Treat. 2004, 15, 169–178. [Google Scholar] [CrossRef]
- Luger, T.; Van Leent, E.J.; Graeber, M.; Hedgecock, S.; Thurston, M.; Kandra, A.; Berth-Jones, J.; Bjerke, J.; Christophers, E.; Knop, J.; et al. SDZ ASM 981: An emerging safe and effective treatment for atopic dermatitis. Br. J. Dermatol. 2001, 144, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Li, P.; Tang, J.; Guo, Y.; Shen, C.; Chang, J.; Kerrouche, N. Prolonging Time to Flare in Pediatric Atopic Dermatitis: A Randomized, Investigator-Blinded, Controlled, Multicenter Clinical Study of a Ceramide-Containing Moisturizer. Adv. Ther. 2017, 34, 2601–2611. [Google Scholar] [CrossRef]
- Ma, L.; Zhang, L.; Kobayashi, M.; Tao, X.; Qian, Q.; Cheng, H.; Liu, S.; Zhou, Y.; Chen, Y.; Zhang, J. Efficacy and safety of crisaborole ointment in Chinese and Japanese patients aged >/=2 years with mild-to-moderate atopic dermatitis. J. Dermatol. 2023, 50, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Mainzer, C.; Le Guillou, M.; Vyumvuhore, R.; Chadoutaud, B.; Bordes, S.; Closs, B. Clinical Efficacy of Oligofructans from Ophiopogon japonicus in Reducing Atopic Dermatitis Flare-ups in Caucasian Patients. Acta Derm. Venereol. 2019, 99, 858–864. [Google Scholar] [CrossRef]
- Maloney, J.M.; Morman, M.R.; Stewart, D.M.; Tharp, M.D.; Brown, J.J.; Rajagopalan, R. Clobetasol propionate emollient 0.05% in the treatment of atopic dermatitis. Int. J. Dermatol. 1998, 37, 142–144. [Google Scholar] [CrossRef]
- Mandelin, J.; Remitz, A.; Virtanen, H.; Reitamo, S. One-year treatment with 0.1% tacrolimus ointment versus a corticosteroid regimen in adults with moderate to severe atopic dermatitis: A randomized, double-blind, comparative trial. Acta Derm. Venereol. 2010, 90, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Marseglia, A.; Licari, A.; Agostinis, F.; Barcella, A.; Bonamonte, D.; Puviani, M.; Milani, M.; Marseglia, G. Local rhamnosoft, ceramides and L-isoleucine in atopic eczema: A randomized, placebo controlled trial. Pediatr. Allergy Immunol. 2014, 25, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Matheson, R.; Kempers, S.; Breneman, D.; Draelos, Z.; Johnson, C.E.; Loss, R.; Hogan, D.J.; Schoenfeld, R.; Checketts, S.; Kircik, L.; et al. Hydrocortisone butyrate 0.1% lotion in the treatment of atopic dermatitis in pediatric subjects. J. Drugs Dermatol. 2008, 7, 266–271. [Google Scholar] [PubMed]
- Mayser, P.; Kupfer, J.; Nemetz, D.; Schafer, U.; Nilles, M.; Hort, W.; Gieler, U. Treatment of head and neck dermatitis with ciclopiroxolamine cream--results of a double-blind, placebo-controlled study. Ski. Pharmacol. Physiol. 2006, 19, 153–158. [Google Scholar] [CrossRef]
- Meurer, M.; Eichenfield, L.F.; Ho, V.; Potter, P.C.; Werfel, T.; Hultsch, T. Addition of pimecrolimus cream 1% to a topical corticosteroid treatment regimen in paediatric patients with severe atopic dermatitis: A randomized, double-blind trial. J. Dermatol. Treat. 2010, 21, 157–166. [Google Scholar] [CrossRef]
- Meurer, M.; Fartasch, M.; Albrecht, G.; Vogt, T.; Worm, M.; Ruzicka, T.; Altmeyer, P.J.; Schneider, D.; Weidinger, G.; Braeutigam, M.; et al. Long-term efficacy and safety of pimecrolimus cream 1% in adults with moderate atopic dermatitis. Dermatology 2004, 208, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Meurer, M.; Folster-Holst, R.; Wozel, G.; Weidinger, G.; Junger, M.; Brautigam, M.; The CASM-DE-01 Study Group. Pimecrolimus cream in the long-term management of atopic dermatitis in adults: A six-month study. Dermatology 2002, 205, 271–277. [Google Scholar] [CrossRef]
- Meysami, M.; Hashempur, M.H.; Kamalinejad, M.; Emtiazy, M. Efficacy of Short Term Topical Malva sylvestris L. Cream in Pediatric Patients with Atopic Dermatitis: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Endocr. Metab. Immune Disord.-Drug Targets 2021, 21, 1673–1678. [Google Scholar] [CrossRef]
- Miller, D.W.; Koch, S.B.; Yentzer, B.A.; Clark, A.R.; O’Neill, J.R.; Fountain, J.; Weber, T.M.; Fleischer, A.B., Jr. An over-the-counter moisturizer is as clinically effective as, and more cost-effective than, prescription barrier creams in the treatment of children with mild-to-moderate atopic dermatitis: A randomized, controlled trial. J. Drugs Dermatol. 2011, 10, 531–537. [Google Scholar]
- Mori, K.; Seki, T.; Kaizu, K.; Takagi, Y.; Miyaki, M.; Ishizaki, C.; Katayama, I. Efficacy of a moisturizer containing a pseudo-ceramide and a eucalyptus extract for Japanese patients with mild atopic dermatitis in the summer. J. Cosmet. Dermatol. 2019, 18, 850–856. [Google Scholar] [CrossRef]
- Msika, P.; De Belilovsky, C.; Piccardi, N.; Chebassier, N.; Baudouin, C.; Chadoutaud, B. New emollient with topical corticosteroid-sparing effect in treatment of childhood atopic dermatitis: SCORAD and quality of life improvement. Pediatr. Dermatol. 2008, 25, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Mudaliyar, V.R.; Pathak, A.; Dixit, A.; Kumar, S.S. An Open-Label Prospective Study to Compare the Efficacy and Safety of Topical Fluticasone Versus Tacrolimus in the Proactive Treatment of Atopic Dermatitis. Dermatol. Pract. Concept. 2020, 10, e2020094. [Google Scholar] [CrossRef] [PubMed]
- Murrell, D.F.; Calvieri, S.; Ortonne, J.P.; Ho, V.C.; Weise-Riccardi, S.; Barbier, N.; Paul, C.F. A randomized controlled trial of pimecrolimus cream 1% in adolescents and adults with head and neck atopic dermatitis and intolerant of, or dependent on, topical corticosteroids. Br. J. Dermatol. 2007, 157, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Nadora, D.; Burney, W.; Chaudhuri, R.K.; Galati, A.; Min, M.; Fong, S.; Lo, K.; Chambers, C.J.; Sivamani, R.K. Prospective Randomized Double-Blind Vehicle-Controlled Study of Topical Coconut and Sunflower Seed Oil-Derived Isosorbide Diesters on Atopic Dermatitis. Dermatitis 2024, 35, S62–S69. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Nagata, T. Efficacy and safety of topical JTE-052, a Janus kinase inhibitor, in Japanese adult patients with moderate-to-severe atopic dermatitis: A phase II, multicentre, randomized, vehicle-controlled clinical study. Br. J. Dermatol. 2018, 178, 424–432. [Google Scholar] [CrossRef]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Kabashima, K.; Oda, M.; Nagata, T. Delgocitinib ointment in pediatric patients with atopic dermatitis: A phase 3, randomized, double-blind, vehicle-controlled study and a subsequent open-label, long-term study. J. Am. Acad. Dermatol. 2021, 85, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Kaino, H.; Nagata, T. Delgocitinib ointment, a topical Janus kinase inhibitor, in adult patients with moderate to severe atopic dermatitis: A phase 3, randomized, double-blind, vehicle-controlled study and an open-label, long-term extension study. J. Am. Acad. Dermatol. 2020, 82, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Oda, M.; Kabashima, K.; Nagata, T. Phase 2 clinical study of delgocitinib ointment in pediatric patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 144, 1575–1583. [Google Scholar] [CrossRef] [PubMed]
- Nakai, K.; Kubota, Y.; Soma, G.I.; Kohchi, C. The Effect of Lipopolysaccharide-containing Moisturizing Cream on Skin Care in Patients With Mild Atopic Dermatitis. Vivo 2019, 33, 109–114. [Google Scholar] [CrossRef]
- Nemoto, O.; Hayashi, N.; Kitahara, Y.; Furue, M.; Hojo, S.; Nomoto, M.; Shima, S.; The Japanese E6005 Study Investigators. Effect of topical phosphodiesterase 4 inhibitor E6005 on Japanese children with atopic dermatitis: Results from a randomized, vehicle-controlled exploratory trial. J. Dermatol. 2016, 43, 881–887. [Google Scholar] [CrossRef]
- Niemeyer-van der Kolk, T.; Buters, T.P.; Krouwels, L.; Boltjes, J.; de Kam, M.L.; van der Wall, H.; van Alewijk, D.; van den Munckhof, E.H.A.; Becker, M.J.; Feiss, G.; et al. Topical antimicrobial peptide omiganan recovers cutaneous dysbiosis but does not improve clinical symptoms in patients with mild to moderate atopic dermatitis in a phase 2 randomized controlled trial. J. Am. Acad. Dermatol. 2022, 86, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Ohba, F.; Matsuki, S.; Imayama, S.; Matsuguma, K.; Hojo, S.; Nomoto, M.; Akama, H. Efficacy of a novel phosphodiesterase inhibitor, E6005, in patients with atopic dermatitis: An investigator-blinded, vehicle-controlled study. J. Dermatol. Treat. 2016, 27, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Onumah, N.; Kircik, L. Pimecrolimus cream and Tacrolimus ointment in the treatment of atopic dermatitis: A pilot study on patient preference. J. Drugs Dermatol. 2013, 12, 1145–1148. [Google Scholar] [PubMed]
- Paller, A.; Eichenfield, L.F.; Leung, D.Y.; Stewart, D.; Appell, M. A 12-week study of tacrolimus ointment for the treatment of atopic dermatitis in pediatric patients. J. Am. Acad. Dermatol. 2001, 44, S47–S57. [Google Scholar] [CrossRef]
- Paller, A.S.; Eichenfield, L.F.; Kirsner, R.S.; Shull, T.; Jaracz, E.; Simpson, E.L.; Group, U.S.T.O.S. Three times weekly tacrolimus ointment reduces relapse in stabilized atopic dermatitis: A new paradigm for use. Pediatrics 2008, 122, e1210–e1218. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Nimmagadda, S.; Schachner, L.; Mallory, S.B.; Kahn, T.; Willis, I.; Eichenfield, L.F. Fluocinolone acetonide 0.01% in peanut oil: Therapy for childhood atopic dermatitis, even in patients who are peanut sensitive. J. Am. Acad. Dermatol. 2003, 48, 569–577. [Google Scholar] [CrossRef]
- Paller, A.S.; Stein Gold, L.; Soung, J.; Tallman, A.M.; Rubenstein, D.S.; Gooderham, M. Efficacy and patient-reported outcomes from a phase 2b, randomized clinical trial of tapinarof cream for the treatment of adolescents and adults with atopic dermatitis. J. Am. Acad. Dermatol. 2021, 84, 632–638. [Google Scholar] [CrossRef]
- Paller, A.S.; Tom, W.L.; Lebwohl, M.G.; Blumenthal, R.L.; Boguniewicz, M.; Call, R.S.; Eichenfield, L.F.; Forsha, D.W.; Rees, W.C.; Simpson, E.L.; et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J. Am. Acad. Dermatol. 2016, 75, 494–503.e6. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.; Szepietowski, J.C.; Kircik, L.; Toth, D.; Eichenfield, L.F.; Leung, D.Y.M.; Forman, S.B.; Venturanza, M.E.; Sun, K.; Kuligowski, M.E.; et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: Results from 2 phase 3, randomized, double-blind studies. J. Am. Acad. Dermatol. 2021, 85, 863–872. [Google Scholar] [CrossRef]
- Park, C.W.; Kim, B.J.; Lee, Y.W.; Won, C.; Park, C.O.; Chung, B.Y.; Lee, D.H.; Jung, K.; Nam, H.J.; Choi, G.; et al. Asivatrep, a TRPV1 antagonist, for the topical treatment of atopic dermatitis: Phase 3, randomized, vehicle-controlled study (CAPTAIN-AD). J. Allergy Clin. Immunol. 2022, 149, 1340–1347.e4. [Google Scholar] [CrossRef]
- Patrizi, A.; Capitanio, B.; Neri, I.; Giacomini, F.; Sinagra, J.L.; Raone, B.; Berardesca, E. A double-blind, randomized, vehicle-controlled clinical study to evaluate the efficacy and safety of MAS063DP (ATOPICLAIR) in the management of atopic dermatitis in paediatric patients. Pediatr. Allergy Immunol. 2008, 19, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Patrizi, A.; Raone, B.; Neri, I.; Gurioli, C.; Carbonara, M.; Cassano, N.; Vena, G.A. Randomized, controlled, double-blind clinical study evaluating the safety and efficacy of MD2011001 cream in mild-to-moderate atopic dermatitis of the face and neck in children, adolescents and adults. J. Dermatol. Treat. 2016, 27, 346–350. [Google Scholar] [CrossRef]
- Perala, M.; Salava, A.; Malmberg, P.; Pelkonen, A.S.; Makela, M.J.; Remitz, A. Topical tacrolimus versus corticosteroids in childhood moderate-to-severe atopic dermatitis and the impact on airway inflammation: A long-term randomized open-label study. Clin. Exp. Dermatol. 2023, 48, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Peserico, A.; Stadtler, G.; Sebastian, M.; Fernandez, R.S.; Vick, K.; Bieber, T. Reduction of relapses of atopic dermatitis with methylprednisolone aceponate cream twice weekly in addition to maintenance treatment with emollient: A multicentre, randomized, double-blind, controlled study. Br. J. Dermatol. 2008, 158, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Poole, C.D.; Chambers, C.; Allsopp, R.; Currie, C.J. Quality of life and health-related utility analysis of adults with moderate and severe atopic dermatitis treated with tacrolimus ointment vs. topical corticosteroids. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Poole, C.D.; Chambers, C.; Sidhu, M.K.; Currie, C.J. Health-related utility among adults with atopic dermatitis treated with 0.1% tacrolimus ointment as maintenance therapy over the long term: Findings from the Protopic CONTROL study. Br. J. Dermatol. 2009, 161, 1335–1340. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.F.; Nandi, A.K.; Kabir, S.; Kamal, M.; Basher, M.S.; Banu, L.A. Topical Tacrolimus versus Hydrocortisone on Atopic Dermatitis in Paediatric Patients: A Randomized Controlled Trial. Mymensingh Med. J. 2015, 24, 457–463. [Google Scholar] [PubMed]
- Reitamo, S.; Harper, J.; Bos, J.D.; Cambazard, F.; Bruijnzeel-Koomen, C.; Valk, P.; Smith, C.; Moss, C.; Dobozy, A.; Palatsi, R.; et al. 0.03% Tacrolimus ointment applied once or twice daily is more efficacious than 1% hydrocortisone acetate in children with moderate to severe atopic dermatitis: Results of a randomized double-blind controlled trial. Br. J. Dermatol. 2004, 150, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Reitamo, S.; Ortonne, J.P.; Sand, C.; Cambazard, F.; Bieber, T.; Folster-Holst, R.; Vena, G.; Bos, J.D.; Fabbri, P.; Groenhoej Larsen, C.; et al. A multicentre, randomized, double-blind, controlled study of long-term treatment with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis. Br. J. Dermatol. 2005, 152, 1282–1289. [Google Scholar] [CrossRef]
- Reitamo, S.; Rustin, M.; Ruzicka, T.; Cambazard, F.; Kalimo, K.; Friedmann, P.S.; Schoepf, E.; Lahfa, M.; Diepgen, T.L.; Judodihardjo, H.; et al. Efficacy and safety of tacrolimus ointment compared with that of hydrocortisone butyrate ointment in adult patients with atopic dermatitis. J. Allergy Clin. Immunol. 2002, 109, 547–555. [Google Scholar] [CrossRef]
- Reitamo, S.; Van Leent, E.J.; Ho, V.; Harper, J.; Ruzicka, T.; Kalimo, K.; Cambazard, F.; Rustin, M.; Taieb, A.; Gratton, D.; et al. Efficacy and safety of tacrolimus ointment compared with that of hydrocortisone acetate ointment in children with atopic dermatitis. J. Allergy Clin. Immunol. 2002, 109, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Ridd, M.J.; Santer, M.; MacNeill, S.J.; Sanderson, E.; Wells, S.; Webb, D.; Banks, J.; Sutton, E.; Roberts, A.; Liddiard, L.; et al. Effectiveness and safety of lotion, cream, gel, and ointment emollients for childhood eczema: A pragmatic, randomised, phase 4, superiority trial. Lancet Child. Adolesc. Health 2022, 6, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Gomis, E.; Martinez-Mir, I.; Morales-Olivas, F.J.; Martorell-Aragones, A.; Palop-Larrea, V.; Bernalte-Sese, A.; Cerda-Mir, J.C.; Polo-Martin, P.; Febrer, I.; Aranda-Grau, L.; et al. Fluticasone in mild to moderate atopic dermatitis relapse: A randomized controlled trial. Allergol. Immunopathol. 2018, 46, 378–384. [Google Scholar] [CrossRef]
- Ruer-Mulard, M.; Aberer, W.; Gunstone, A.; Kekki, O.M.; Lopez Estebaranz, J.L.; Vertruyen, A.; Guettner, A.; Hultsch, T. Twice-daily versus once-daily applications of pimecrolimus cream 1% for the prevention of disease relapse in pediatric patients with atopic dermatitis. Pediatr. Dermatol. 2009, 26, 551–558. [Google Scholar] [CrossRef]
- Ruzicka, T.; Bieber, T.; Schopf, E.; Rubins, A.; Dobozy, A.; Bos, J.D.; Jablonska, S.; Ahmed, I.; Thestrup-Pedersen, K.; Daniel, F.; et al. A short-term trial of tacrolimus ointment for atopic dermatitis. N. Engl. J. Med. 1997, 337, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, M.; Morteza-Semnani, K.; Ghoreishi, M.R. The treatment of atopic dermatitis with licorice gel. J. Dermatol. Treat. 2003, 14, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Baba, N.; Ito, K.; Yokota, D.; Tsubouchi, H. Difamilast, a selective phosphodiesterase 4 inhibitor, ointment in paediatric patients with atopic dermatitis: A phase III randomized double-blind, vehicle-controlled trial. Br. J. Dermatol. 2022, 186, 40–49. [Google Scholar] [CrossRef]
- Saeki, H.; Baba, N.; Oshiden, K.; Abe, Y.; Tsubouchi, H. Phase 2, randomized, double-blind, placebo-controlled, 4-week study to evaluate the safety and efficacy of OPA- 15406 (difamilast), a new topical selective phosphodiesterase type-4 inhibitor, in Japanese pediatric patients aged 2–14 years with atopic dermatitis. J. Dermatol. 2020, 47, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Ito, K.; Yokota, D.; Tsubouchi, H. Difamilast ointment in adult patients with atopic dermatitis: A phase 3 randomized, double-blind, vehicle-controlled trial. J. Am. Acad. Dermatol. 2022, 86, 607–614. [Google Scholar] [CrossRef]
- Schachner, L.A.; Lamerson, C.; Sheehan, M.P.; Boguniewicz, M.; Mosser, J.; Raimer, S.; Shull, T.; Jaracz, E.; The US Tacrolimus Ointment Study Group. Tacrolimus ointment 0.03% is safe and effective for the treatment of mild to moderate atopic dermatitis in pediatric patients: Results from a randomized, double-blind, vehicle-controlled study. Pediatrics 2005, 116, e334–e342. [Google Scholar] [CrossRef]
- Schuttelaar, M.L.; Coenraads, P.J. A randomized, double-blind study to assess the efficacy of addition of tetracycline to triamcinolone acetonide in the treatment of moderate to severe atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Sears, H.W.; Bailer, J.W.; Yeadon, A. Efficacy and safety of hydrocortisone buteprate 0.1% cream in patients with atopic dermatitis. Clin. Ther. 1997, 19, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Siegfried, E.; Korman, N.; Molina, C.; Kianifard, F.; Abrams, K. Safety and efficacy of early intervention with pimecrolimus cream 1% combined with corticosteroids for major flares in infants and children with atopic dermatitis. J. Dermatol. Treat. 2006, 17, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Sigurgeirsson, B.; Boznanski, A.; Todd, G.; Vertruyen, A.; Schuttelaar, M.L.; Zhu, X.; Schauer, U.; Qaqundah, P.; Poulin, Y.; Kristjansson, S.; et al. Safety and efficacy of pimecrolimus in atopic dermatitis: A 5-year randomized trial. Pediatrics 2015, 135, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Sigurgeirsson, B.; Ho, V.; Ferrandiz, C.; Andriano, K.; Grinienko, A.; Jimenez, P.; The Pimecrolimus 1% cream in (paediatric) Eczema: Prevention of Progression multi-centre investigator study group. Effectiveness and safety of a prevention-of-flare-progression strategy with pimecrolimus cream 1% in the management of paediatric atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1290–1301. [Google Scholar] [CrossRef]
- Simpson, E.L.; Kircik, L.; Blauvelt, A.; Kallender, H.; Kuo, Y.; Ren, H.; Sturm, D.; Eichenfield, L.F. Clinically relevant improvements in adults and adolescents with atopic dermatitis who did not achieve Investigator’s Global Assessment treatment success following 8 weeks of ruxolitinib cream monotherapy. J. Dermatol. 2023, 50, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Spada, F.; Harrison, I.P.; Barnes, T.M.; Greive, K.A.; Daniels, D.; Townley, J.P.; Mostafa, N.; Fong, A.T.; Tong, P.L.; Shumack, S. A daily regimen of a ceramide-dominant moisturizing cream and cleanser restores the skin permeability barrier in adults with moderate eczema: A randomized trial. Dermatol. Ther. 2021, 34, e14970. [Google Scholar] [CrossRef] [PubMed]
- Stainer, R.; Matthews, S.; Arshad, S.H.; McDonald, S.; Robinson, J.; Schapira, C.; Foote, K.D.; Baird-Snell, M.; Gregory, T.; Pollock, I.; et al. Efficacy and acceptability of a new topical skin lotion of sodium cromoglicate (Altoderm) in atopic dermatitis in children aged 2-12 years: A double-blind, randomized, placebo-controlled trial. Br. J. Dermatol. 2005, 152, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Stander, S.; Metz, M.; Ramos, F.M.; Maurer, M.; Schoepke, N.; Tsianakas, A.; Zeidler, C.; Luger, T.A. Anti-pruritic Effect of Sertaconazole 2% Cream in Atopic Dermatitis Subjects: A Prospective, Randomized, Double-blind, Vehicle-controlled, Multi-centre Clinical Trial of Efficacy, Safety and Local Tolerability. Acta Derm. Venereol. 2016, 96, 792–796. [Google Scholar] [CrossRef]
- Stettler, H.; Kurka, P.; Kandzora, J.; Pavel, V.; Breuer, M.; Macura-Biegun, A. A new topical panthenol-containing emollient for maintenance treatment of childhood atopic dermatitis: Results from a multicenter prospective study. J. Dermatol. Treat. 2017, 28, 774–779. [Google Scholar] [CrossRef]
- Sugarman, J.L.; Parish, L.C. Efficacy of a lipid-based barrier repair formulation in moderate-to-severe pediatric atopic dermatitis. J. Drugs Dermatol. 2009, 8, 1106–1111. [Google Scholar]
- Szczepanowska, J.; Reich, A.; Szepietowski, J.C. Emollients improve treatment results with topical corticosteroids in childhood atopic dermatitis: A randomized comparative study. Pediatr. Allergy Immunol. 2008, 19, 614–618. [Google Scholar] [CrossRef]
- Takeuchi, S.; Saeki, H.; Tokunaga, S.; Sugaya, M.; Ohmatsu, H.; Tsunemi, Y.; Torii, H.; Nakamura, K.; Kawakami, T.; Soma, Y.; et al. A randomized, open-label, multicenter trial of topical tacrolimus for the treatment of pruritis in patients with atopic dermatitis. Ann. Dermatol. 2012, 24, 144–150. [Google Scholar] [CrossRef]
- Tan, W.P.; Suresh, S.; Tey, H.L.; Chiam, L.Y.; Goon, A.T. A randomized double-blind controlled trial to compare a triclosan-containing emollient with vehicle for the treatment of atopic dermatitis. Clin. Exp. Dermatol. 2010, 35, e109–e112. [Google Scholar] [CrossRef]
- Thaci, D.; Chambers, C.; Sidhu, M.; Dorsch, B.; Ehlken, B.; Fuchs, S. Twice-weekly treatment with tacrolimus 0.03% ointment in children with atopic dermatitis: Clinical efficacy and economic impact over 12 months. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 1040–1046. [Google Scholar] [CrossRef]
- Thaci, D.; Reitamo, S.; Gonzalez Ensenat, M.A.; Moss, C.; Boccaletti, V.; Cainelli, T.; van der Valk, P.; Buckova, H.; Sebastian, M.; Schuttelaar, M.L.; et al. Proactive disease management with 0.03% tacrolimus ointment for children with atopic dermatitis: Results of a randomized, multicentre, comparative study. Br. J. Dermatol. 2008, 159, 1348–1356. [Google Scholar] [CrossRef]
- Tharp, M.D. A comparison of twice-daily and once-daily administration of fluticasone propionate cream, 0.05%, in the treatment of eczema. Cutis 1996, 57, 19–26. [Google Scholar]
- Thomas, K.S.; Armstrong, S.; Avery, A.; Po, A.L.; O’Neill, C.; Young, S.; Williams, H.C. Randomised controlled trial of short bursts of a potent topical corticosteroid versus prolonged use of a mild preparation for children with mild or moderate atopic eczema. BMJ 2002, 324, 768. [Google Scholar] [CrossRef]
- Tiplica, G.S.; Boralevi, F.; Konno, P.; Malinauskiene, L.; Kaszuba, A.; Laurens, C.; Saint-Aroman, M.; Delarue, A. The regular use of an emollient improves symptoms of atopic dermatitis in children: A randomized controlled study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1180–1187. [Google Scholar] [CrossRef]
- Tiplica, G.S.; Kaszuba, A.; Malinauskiene, L.; Konno, P.; Boralevi, F.; Garrigue, E.; Saint-Aroman, M.; Delarue, A. Prevention of Flares in Children with Atopic Dermatitis with Regular Use of an Emollient Containing Glycerol and Paraffin: A Randomized Controlled Study. Pediatr. Dermatol. 2017, 34, 282–289. [Google Scholar] [CrossRef]
- Torok, H.M.; Maas-Irslinger, R.; Slayton, R.M. Clocortolone pivalate cream 0.1% used concomitantly with tacrolimus ointment 0.1% in atopic dermatitis. Cutis 2003, 72, 161–166. [Google Scholar] [CrossRef]
- Tripodi, S.; Di Rienzo Businco, A.; Panetta, V.; Pingitore, G.; Volterrani, A.; Frediani, T.; Pelosi, S.; Miceli Sopo, S. Lack of efficacy of topical furfuryl palmitate in pediatric atopic dermatitis: A randomized double-blind study. J. Investig. Allergol. Clin. Immunol. 2009, 19, 204–209. [Google Scholar]
- Ucak, H.; Demir, B.; Cicek, D.; Dertlioglu, S.B.; Akkurt, Z.M.; Ucmak, D.; Halisdemir, N. Efficacy of topical tacrolimus for the treatment of persistent pruritus ani in patients with atopic dermatitis. J. Dermatol. Treat. 2013, 24, 454–457. [Google Scholar] [CrossRef]
- Van Der Meer, J.B.; Glazenburg, E.J.; Mulder, P.G.; Eggink, H.F.; Coenraads, P.J.; The Netherlands Adult Atopic Dermatitis Study Group. The management of moderate to severe atopic dermatitis in adults with topical fluticasone propionate. Br. J. Dermatol. 1999, 140, 1114–1121. [Google Scholar] [CrossRef]
- Vernon, H.J.; Lane, A.T.; Weston, W. Comparison of mometasone furoate 0.1% cream and hydrocortisone 1.0% cream in the treatment of childhood atopic dermatitis. J. Am. Acad. Dermatol. 1991, 24, 603–607. [Google Scholar] [CrossRef]
- Wahn, U.; Bos, J.D.; Goodfield, M.; Caputo, R.; Papp, K.; Manjra, A.; Dobozy, A.; Paul, C.; Molloy, S.; Hultsch, T.; et al. Efficacy and safety of pimecrolimus cream in the long-term management of atopic dermatitis in children. Pediatrics 2002, 110, e2. [Google Scholar] [CrossRef]
- Wang, S.; Wang, L.; Li, P.; Shu, H.; Shen, C.; Wu, Y.; Luo, Z.; Miao, L.; Wang, H.; Jiao, L.; et al. The improvement of infantile atopic dermatitis during the maintenance period: A multicenter, randomized, parallel controlled clinical study of emollients in Prinsepia utilis Royle. Dermatol. Ther. 2020, 33, e13153. [Google Scholar] [CrossRef]
- Weber, T.M.; Samarin, F.; Babcock, M.J.; Filbry, A.; Rippke, F. Steroid-Free Over-the-Counter Eczema Skin Care Formulations Reduce Risk of Flare, Prolong Time to Flare, and Reduce Eczema Symptoms in Pediatric Subjects With Atopic Dermatitis. J. Drugs Dermatol. 2015, 14, 478–485. [Google Scholar]
- Williams, H.C. Twice-weekly topical corticosteroid therapy may reduce atopic dermatitis relapses. Arch. Dermatol. 2004, 140, 1151–1152. [Google Scholar] [CrossRef]
- Wiren, K.; Nohlgard, C.; Nyberg, F.; Holm, L.; Svensson, M.; Johannesson, A.; Wallberg, P.; Berne, B.; Edlund, F.; Loden, M. Treatment with a barrier-strengthening moisturizing cream delays relapse of atopic dermatitis: A prospective and randomized controlled clinical trial. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 1267–1272. [Google Scholar] [CrossRef]
- Wolkerstorfer, A.; Strobos, M.A.; Glazenburg, E.J.; Mulder, P.G.; Oranje, A.P. Fluticasone propionate 0.05% cream once daily versus clobetasone butyrate 0.05% cream twice daily in children with atopic dermatitis. J. Am. Acad. Dermatol. 1998, 39, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Wollenberg, A.; Reitamo, S.; Atzori, F.; Lahfa, M.; Ruzicka, T.; Healy, E.; Giannetti, A.; Bieber, T.; Vyas, J.; Deleuran, M.; et al. Proactive treatment of atopic dermatitis in adults with 0.1% tacrolimus ointment. Allergy 2008, 63, 742–750. [Google Scholar] [CrossRef]
- Worm, M.; Bauer, A.; Elsner, P.; Mahler, V.; Molin, S.; Nielsen, T.S.S. Efficacy and safety of topical delgocitinib in patients with chronic hand eczema: Data from a randomized, double-blind, vehicle-controlled phase IIa study. Br. J. Dermatol. 2020, 182, 1103–1110. [Google Scholar] [CrossRef]
- Wu, S.H.; Chen, X.Q.; Liu, B.; Wu, H.J.; Dong, L. Efficacy and safety of 15(R/S)-methyl-lipoxin A(4) in topical treatment of infantile eczema. Br. J. Dermatol. 2013, 168, 172–178. [Google Scholar] [CrossRef]
- Xu, Z.; Liu, X.; Niu, Y.; Shen, C.; Heminger, K.; Moulton, L.; Yu, A.; Allen, T.; Zhang, L.; Yue, F.; et al. Skin benefits of moisturising body wash formulas for children with atopic dermatitis: A randomised controlled clinical study in China. Australas. J. Dermatol. 2020, 61, e54–e59. [Google Scholar] [CrossRef]
- Yen, C.Y.; Hsieh, C.L. Therapeutic Effect of Tzu-Yun Ointment on Patients with Atopic Dermatitis: A Preliminary, Randomized, Controlled, Open-Label Study. J. Altern. Complement. Med. 2016, 22, 237–243. [Google Scholar] [CrossRef]
- Yosipovitch, G.; Gold, L.F.; Lebwohl, M.G.; Silverberg, J.I.; Tallman, A.M.; Zane, L.T. Early Relief of Pruritus in Atopic Dermatitis with Crisaborole Ointment, A Non-steroidal, Phosphodiesterase 4 Inhibitor. Acta Derm. Venereol. 2018, 98, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Zelenkova, H.; Kerob, D.; Salah, S.; Demessant-Flavigny, A.L. Impact of daily use of emollient ‘plus’ on corticosteroid consumption in patients with atopic dermatitis: An open, randomized controlled study. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 27–34. [Google Scholar] [CrossRef]
- Zhu, J.R.; Wang, J.; Wang, S.S. A single-center, randomized, controlled study on the efficacy of niacinamide-containing body emollients combined with cleansing gel in the treatment of mild atopic dermatitis. Skin. Res. Technol. 2023, 29, e13475. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Brautigam, M. Long-term management of facial atopic eczema with pimecrolimus cream 1% in paediatric patients with mild to moderate disease. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 718–721. [Google Scholar] [CrossRef]
- Zuberbier, T.; Heinzerling, L.; Bieber, T.; Schauer, U.; Klebs, S.; Brautigam, M. Steroid-sparing effect of pimecrolimus cream 1% in children with severe atopic dermatitis. Dermatology 2007, 215, 325–330. [Google Scholar] [CrossRef]
- Societies, I.L.o.D. Global Atopic Dermatitis Atlas; Global Atopic Dermatitis Atlas (GABA): London, UK, 2022; Available online: https://www.atopicdermatitisatlas.org/en/ (accessed on 17 March 2024).
- Wood, A.M.; White, I.R.; Thompson, S.G. Are missing outcome data adequately handled? A review of published randomized controlled trials in major medical journals. Clin. Trials 2004, 1, 368–376. [Google Scholar] [CrossRef]
- Campbell, M.K.; Snowdon, C.; Francis, D.; Elbourne, D.; McDonald, A.M.; Knight, R.; Entwistle, V.; Garcia, J.; Roberts, I.; Grant, A.; et al. Recruitment to randomised trials: Strategies for trial enrollment and participation study. The STEPS study. Health Technol. Assess. 2007, 11, ix-105. [Google Scholar] [CrossRef]
- Sulzberger, M.B.; Witten, V.H. The effect of topically applied compound F in selected dermatoses. J. Investig. Dermatol. 1952, 19, 101–102. [Google Scholar] [CrossRef]
- Marshall, H.F.; Leung, D.Y.M.; Lack, G.; Sindher, S.; Ciaccio, C.E.; Chan, S.; Nadeau, K.C.; Brough, H.A. Topical steroid withdrawal and atopic dermatitis. Ann. Allergy Asthma Immunol. 2023, 132, 423–425. [Google Scholar] [CrossRef]
- Maghen, P.; Unrue, E.L.; Oussedik, E.; Cline, A.; Cardwell, L.A.; Feldman, S.R. Regardless of how risks are framed, patients seem hesitant to use topical steroids for atopic dermatitis. Br. J. Dermatol. 2019, 181, 842–844. [Google Scholar] [CrossRef]
- Gutfreund, K.; Bienias, W.; Szewczyk, A.; Kaszuba, A. Topical calcineurin inhibitors in dermatology. Part I: Properties, method and effectiveness of drug use. Postep. Dermatol. I Alergol. 2013, 30, 165–169. [Google Scholar] [CrossRef]
- Kamata, M.; Tada, Y. Optimal Use of Jak Inhibitors and Biologics for Atopic Dermatitis on the Basis of the Current Evidence. JID Innov. 2023, 3, 100195. [Google Scholar] [CrossRef]
- Milakovic, M.; Gooderham, M.J. Phosphodiesterase-4 Inhibition in Psoriasis. Psoriasis Targets Ther. 2021, 11, 21–29. [Google Scholar] [CrossRef]
- Yang, H.; Wang, J.; Zhang, X.; Zhang, Y.; Qin, Z.L.; Wang, H.; Luo, X.Y. Application of Topical Phosphodiesterase 4 Inhibitors in Mild to Moderate Atopic Dermatitis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019, 155, 585–593. [Google Scholar] [CrossRef]
- Nair, A.S. Publication bias—Importance of studies with negative results! Indian. J. Anaesth. 2019, 63, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Manjelievskaia, J.; Boytsov, N.; Brouillette, M.A.; Onyekwere, U.; Pierce, E.; Goldblum, O.; Bonafede, M. The direct and indirect costs of adult atopic dermatitis. J. Manag. Care Spec. Pharm. 2021, 27, 1416–1425. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | Average | Minimum | Maximum |
|---|---|---|---|
| Total (n) | 226 | 20 | 2439 |
| Total Completed (n) | 207 | - | - |
| Attrition Rate | 15.49% | 0% | 79.07% |
| Age | - | 2 weeks | 87 years |
| Treatment Arms | 2.43 | 2 | 8 |
| Duration (days) | 82.98 | 7 | 1825 |
| Corticosteroids | Calcineruin Inhibitors | JAK Inhibitors | Phosphodiesterase Inhibitors |
|---|---|---|---|
| 96 arms | 87 arms | 22 arms | 14 arms |
| Metrics | Number of Trials |
|---|---|
| Analysis of AD severity | 171 trials |
| Decreased AD severity with treatment, significant | 156 trials |
| Analysis of AD relapse rate | 31 trials |
| Decreased AD relapse rate, significant | 23 trials |
| QoL analysis | 50 trials |
| Improved QoL with treatment, significant | 24 trials |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazar, M.; Zhang, A.D.; Vashi, N.A. Topical Treatments in Atopic Dermatitis: An Expansive Review. J. Clin. Med. 2024, 13, 2185. https://doi.org/10.3390/jcm13082185
Lazar M, Zhang AD, Vashi NA. Topical Treatments in Atopic Dermatitis: An Expansive Review. Journal of Clinical Medicine. 2024; 13(8):2185. https://doi.org/10.3390/jcm13082185
Chicago/Turabian StyleLazar, Michelle, Aurore D. Zhang, and Neelam A. Vashi. 2024. "Topical Treatments in Atopic Dermatitis: An Expansive Review" Journal of Clinical Medicine 13, no. 8: 2185. https://doi.org/10.3390/jcm13082185