
The Importance of Lung Ultrasound and IGFBP7 (Insulin-like Growth Factor Binding Protein 7) Assessment in Diagnosing Patients with Heart Failure



 ,
,
Abstract
1. Introduction
- Heart failure with preserved ejection fraction (HFpEF) with EF range ≥ 50%;
- Heart failure with mildly reduced ejection fraction (HFmrEF) with EF range 41–49%;
- Heart failure with reduced ejection fraction (HFrEF) with EF range ≤ 40%.
- To assess the usefulness of LUS as a quick diagnostic method to confirm the cardiac cause of dyspnea in patients with HFpEF and HFmrEF;
- To determine the correlation between the ultrasound image of the lungs and classic (NTproBNP) and new (IGFBP7) biomarkers and echocardiographic markers of HF;
- To assess the importance of B-lines in lung ultrasound and IGFBP7 concentration as a prognostic factor in patients with HFpEF and HFmrEF hospitalized due to exacerbations of HF symptoms.
2. Materials and Methods
2.1. Study Population
2.2. Ethical Issues
2.3. Biochemical Evaluation
2.4. Lung Ultrasonography
2.5. Echocardiography
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Echocardiography
3.3. Pharmacological Treatment
3.4. Biochemical Tests
3.5. Lung Ultrasonography
3.6. Duration of Hospitalization
3.6.1. Patients with Preserved LV Ejection Fraction—EF ≥ 50%
3.6.2. Patients with Mildly Impaired LV Ejection Fraction—EF 41–49%
3.7. Follow-Up
3.7.1. Rehospitalizations
3.7.2. Mortality
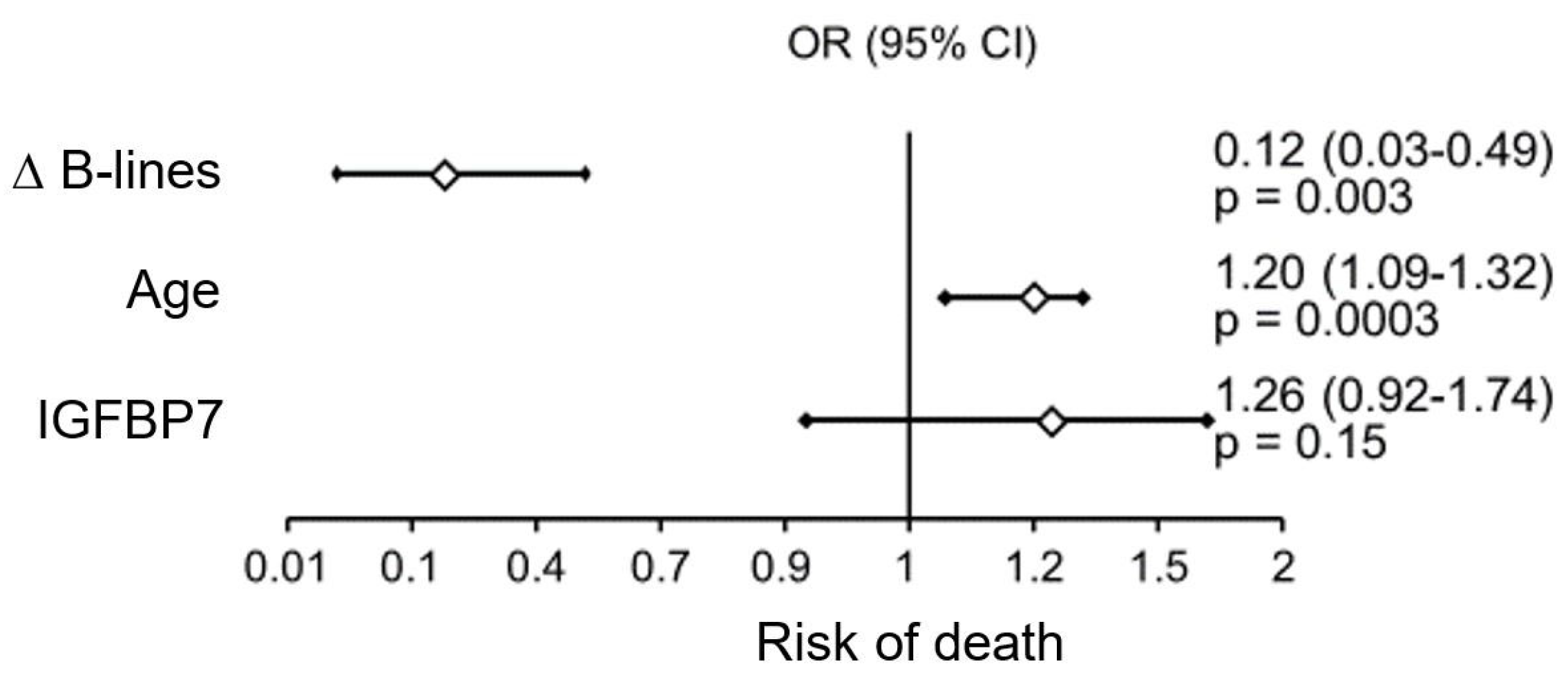
3.8. Multivariate Analysis
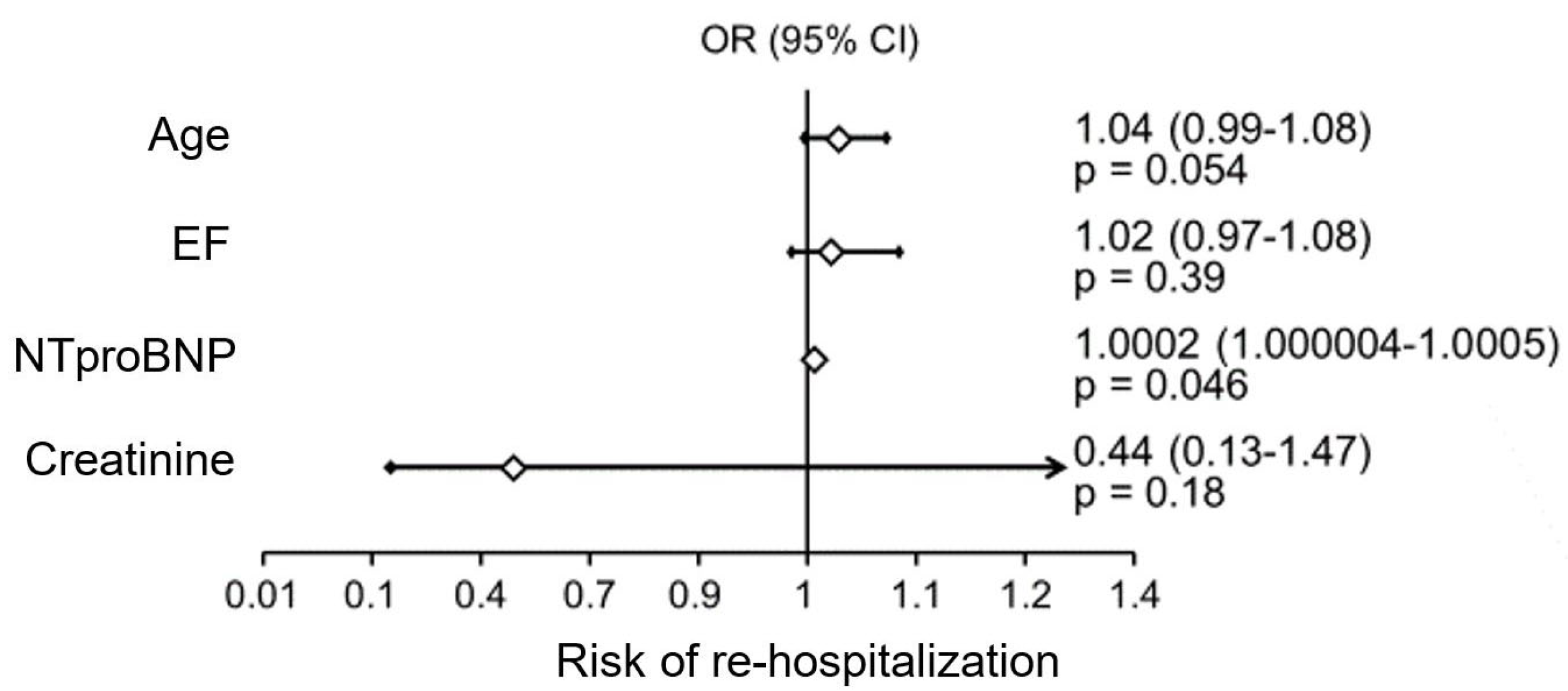
- A significant independent factor influencing the risk of rehospitalization was NTproBNP levels (Figure 3);
- Factors significantly impacting mortality in the study patient population were patient age and the difference between the number of B-lines on ultrasound on admission and at hospital discharge (Figure 4).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef]
- Ceia, F.; Fonseca, C.; Mota, T.; Morais, H.; Matias, F.; de Sousa, A.; Oliveira, A.G. Prevalence of chronic heart failure in Southwestern Europe: The EPICA study. Eur. J. Heart Fail. 2002, 4, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Bleumink, G.S.; Knetsch, A.M.; Sturkenboom, M.C.; Straus, S.M.; Hofman, A.; Deckers, J.W.; Witteman, J.C.; Stricker, B.H. Quantifying the heart failure epidemic: Prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. Eur. Heart J. 2004, 25, 1614–1619. [Google Scholar] [CrossRef]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef]
- Tsao, C.W.; Lyass, A.; Enserro, D.; Larson, M.G.; Ho, J.E.; Kizer, J.R.; Gottdiener, J.S.; Psaty, B.M.; Vasan, R.S. Temporal Trends in the Incidence of and Mortality Associated with Heart Failure with Preserved and Reduced Ejection Fraction. JACC Heart Fail. 2018, 6, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Szyszkowska, A.; Knapp, M.; Kamiński, K.; Lisowska, A. Insulin-like growth factor-binding protein 7 (IGFBP7): Novel, independent marker of cardiometabolic diseases? Postępy Hig. Med. Doświadczalnej 2019, 73, 735–740. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, M.; Ling, J.; Cai, L.; Zhang, D.; Gu, H.F.; Wang, H.; Zhu, Y.; Lai, M. Serum IGFBP7 levels associate with insulin resistance and the risk of metabolic syndrome in a Chinese population. Sci. Rep. 2015, 5, 10227. [Google Scholar] [CrossRef]
- Abboud, A.; Kui, N.; Gaggin, H.K.; Ibrahim, N.E.; Chen-Tournoux, A.A.; Christenson, R.H.; Hollander, J.E.; Levy, P.D.; Nagurney, J.T.; Nowak, R.M.; et al. Multiple Cardiac Biomarker Testing Among Patients with Acute Dyspnea From the ICON-RELOADED Study. J. Card. Fail. 2022, 28, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Kalayci, A.; Peacock, W.F.; Nagurney, J.T.; Hollander, J.E.; Levy, P.D.; Singer, A.J.; Shapiro, N.I.; Cheng, R.K.; Cannon, C.M.; Blomkalns, A.L.; et al. Echocardiographic assessment of insulin-like growth factor binding protein-7 and early identification of acute heart failure. ESC Heart Fail. 2020, 7, 1664–1675. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, M.; Poggioni, C.; Pini, R. Can Chest Ultrasonography Replace Standard Chest Radiography for Evaluation of Acute Dyspnea in the ED? Chest 2011, 139, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, Ø.; Myhre, P.L.; Omland, T. Assessing congestion in acute heart failure using cardiac and lung ultrasound—A review. Expert Rev. Cardiovasc. Ther. 2021, 19, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Brainin, P.; Claggett, B.; Lewis, E.F.; Dwyer, K.H.; Merz, A.A.; Silverman, M.B.; Swamy, V.; Biering-Sørensen, T.; Rivero, J.; Cheng, S.; et al. Body mass index and B-lines on lung ultrasonography in chronic and acute heart failure. ESC Heart Fail. 2020, 7, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Miger, K.C.; Fabricius-Bjerre, A.; Maschmann, C.P.; Wamberg, J.; Wille, M.M.W.; Abild-Nielsen, A.G.; Pedersen, L.; Schultz, H.H.L.; Nybing, J.D.; Nielsen, O.W. Clinical Applicability of Lung Ultrasound Methods in the Emergency Department to Detect Pulmonary Congestion on Computed Tomography. Ultraschall Med. 2021, 42, e21–e30. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Lasarte, M.; Alvarez-Garcia, J.; Fernández-Martínez, J.; Maestro, A.; López-López, L.; Solé-González, E.; Pirla, M.J.; Mesado, N.; Mirabet, S.; Fluvià, P.; et al. Lung ultrasound-guided treatment in ambulatory patients with heart failure: A randomized controlled clinical trial (LUS-HF study). Eur. J. Heart Fail. 2019, 21, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Lasarte, M.; Álvarez-García, J.; Mirabet, S.; Sionis, A.; Roig, E.; Cinca, J. Is lung ultrasound monitoring really useful for impacting rehospitalization and mortality in worsening heart failure? Reply. Eur. J. Heart Fail. 2020, 22, 386–387. [Google Scholar] [CrossRef]
- Muniz, R.T.; Mesquita, E.T.; Junior, C.V.S.; Martins, W.d.A. Pulmonary Ultrasound in Patients with Heart Failure—Systematic Review. Arq. Bras. Cardiol. 2018, 110, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Birolleau, S.; Lefort, Y.; Becquemin, M.-H.; Beigelman, C.; Isnard, R.; Teixeira, A.; Arthaud, M.; Riou, B.; Boddaert, J. Acute respiratory failure in the elderly: Etiology, emergency diagnosis and prognosis. Crit. Care 2006, 10, R82. [Google Scholar] [CrossRef] [PubMed]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults with Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Al Deeb, M.; Barbic, S.; Featherstone, R.; Dankoff, J.; Barbic, D. Point-of-care Ultrasonography for the Diagnosis of Acute Cardiogenic Pulmonary Edema in Patients Presenting with Acute Dyspnea: A Systematic Review and Meta-analysis. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2014, 21, 843–852. [Google Scholar] [CrossRef]
- Pivetta, E.; Goffi, A.; Lupia, E.; Tizzani, M.; Porrino, G.; Ferreri, E.; Volpicelli, G.; Balzaretti, P.; Banderali, A.; Iacobucci, A.; et al. Lung Ultrasound-Implemented Diagnosis of Acute Decompensated Heart Failure in the ED: A SIMEU Multicenter Study. Chest 2015, 148, 202–210. [Google Scholar] [CrossRef]
- Chiu, L.; Jairam, M.P.; Chow, R.; Chiu, N.; Shen, M.; Alhassan, A.; Lo, C.-H.; Chen, A.; Kennel, P.J.; Poterucha, T.J.; et al. Meta-Analysis of Point-of-Care Lung Ultrasonography Versus Chest Radiography in Adults with Symptoms of Acute Decompensated Heart Failure. Am. J. Cardiol. 2022, 174, 89–95. [Google Scholar] [CrossRef]
- Martindale, J.L.; Wakai, A.; Collins, S.P.; Levy, P.D.; Diercks, D.; Hiestand, B.C.; Fermann, G.J.; Desouza, I.; Sinert, R. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2016, 23, 223–242. [Google Scholar] [CrossRef] [PubMed]
- Palazzuoli, A.; Ruocco, G.; Beltrami, M.; Nuti, R.; Cleland, J.G. Combined use of lung ultrasound, B-type natriuretic peptide, and echocardiography for outcome prediction in patients with acute HFrEF and HFpEF. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Palazzuoli, A.; Evangelista, I.; Beltrami, M.; Pirrotta, F.; Tavera, M.C.; Gennari, L.; Ruocco, G. Clinical, Laboratory and Lung Ultrasound Assessment of Congestion in Patients with Acute Heart Failure. J. Clin. Med. 2022, 11, 1642. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Caramello, V.; Cardinale, L.; Mussa, A.; Bar, F.; Frascisco, M.F. Bedside ultrasound of the lung for the monitoring of acute decompensated heart failure. Am. J. Emerg. Med. 2008, 26, 585–591. [Google Scholar] [CrossRef]
- Gargani, L.; Pang, P.S.; Frassi, F.; Miglioranza, M.; Dini, F.L.; Landi, P.; Picano, E. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: A lung ultrasound study. Cardiovasc. Ultrasound 2015, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Mhanna, M.; Beran, A.; Nazir, S.; Sajdeya, O.; Srour, O.; Ayesh, H.; Eltahawy, E.A. Lung ultrasound–guided management to reduce hospitalization in chronic heart failure: A systematic review and meta-analysis. Heart Fail. Rev. 2022, 27, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Li, T.; Maybaum, S.; Fridman, D.; Gordon, M.; Shi, D.; Nelson, M.; Stevens, G.R. Pulmonary Congestion on Lung Ultrasound Predicts Increased Risk of 30-Day Readmission in Heart Failure Patients. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2023, 42, 1809–1818. [Google Scholar] [CrossRef] [PubMed]
- Rattarasarn, I.; Yingchoncharoen, T.; Assavapokee, T. Prediction of rehospitalization in patients with acute heart failure using point-of-care lung ultrasound. BMC Cardiovasc. Disord. 2022, 22, 330. [Google Scholar] [CrossRef] [PubMed]
- Domingo, M.; Lupón, J.; Girerd, N.; Conangla, L.; de Antonio, M.; Moliner, P.; Santiago-Vacas, E.; Codina, P.; Cediel, G.; Spitaleri, G.; et al. Lung ultrasound in outpatients with heart failure: The wet-to-dry HF study. ESC Heart Fail. 2021, 8, 4506–4516. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.; Merz, A.A.; Jhund, P.S.; Vazir, A.; Campbell, R.; McMurray, J.J. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: A systematic review. Eur. J. Heart Fail. 2017, 19, 1154–1163. [Google Scholar] [CrossRef]
- He, J.; Yi, S.; Zhou, Y.; Hu, X.; Lun, Z.; Dong, H.; Zhang, Y. B-Lines by Lung Ultrasound Can Predict Worsening Heart Failure in Acute Myocardial Infarction During Hospitalization and Short-Term Follow-Up. Front. Cardiovasc. Med. 2022, 9, 895133. [Google Scholar] [CrossRef]
- Marini, C.; Fragasso, G.; Italia, L.; Sisakian, H.; Tufaro, V.; Ingallina, G.; Stella, S.; Ancona, F.; Loiacono, F.; Innelli, P.; et al. Lung ultrasound-guided therapy reduces acute decompensation events in chronic heart failure. Heart Br. Card. Soc. 2020, 106, 1934–1939. [Google Scholar] [CrossRef]
- Rubio-Gracia, J.; Giménez-López, I.; Josa-Laorden, C.; Sánchez-Marteles, M.; Garcés-Horna, V.; Ruiz-Laiglesia, F.; Legarre, P.S.; Juana, E.B.; Amores-Arriaga, B.; Pérez-Calvo, J. Prognostic value of multimodal assessment of congestion in acute heart failure. Rev. Clin. Esp. 2021, 221, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Bajraktari, G.; Pugliese, N.R.; D’agostino, A.; Rosa, G.M.; Ibrahimi, P.; Perçuku, L.; Miccoli, M.; Galeotti, G.G.; Fabiani, I.; Pedrinelli, R.; et al. Echo- and B-Type Natriuretic Peptide-Guided Follow-Up versus Symptom-Guided Follow-Up: Comparison of the Outcome in Ambulatory Heart Failure Patients. Cardiol. Res. Pract. 2018, 2018, 3139861. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Damman, K.; Harjola, V.; Mebazaa, A.; Rocca, H.B.; Martens, P.; Testani, J.M.; Tang, W.W.; Orso, F.; Rossignol, P.; et al. The use of diuretics in heart failure with congestion—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.S.; Russell, F.M.; Ehrman, R.; Ferre, R.; Gargani, L.; Levy, P.D.; Noble, V.; Lane, K.A.; Li, X.; Collins, S.P. Lung Ultrasound–Guided Emergency Department Management of Acute Heart Failure (BLUSHED-AHF): A Randomized Controlled Pilot Trial. JACC Heart Fail. 2021, 9, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Li, N.; Wu, M.; Peng, Z.; Huang, H.; Zhao, W.; Yi, L.; Liao, M.; Liu, Z.; Peng, Y.; et al. Impact of B-lines-guided intensive heart failure management on outcome of discharged heart failure patients with residual B-lines. ESC Heart Fail. 2022, 9, 2713–2718. [Google Scholar] [CrossRef]
- Liteplo, A.S.; Marill, K.A.; Villen, T.; Miller, R.M.; Murray, A.F.; Croft, P.E.; Capp, R.; Noble, V.E. Emergency Thoracic Ultrasound in the Differentiation of the Etiology of Shortness of Breath (ETUDES): Sonographic B-lines and N-terminal Pro-brain-type Natriuretic Peptide in Diagnosing Congestive Heart Failure. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2009, 16, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Frassi, F.; Soldati, G.; Tesorio, P.; Gheorghiade, M.; Picano, E. Ultrasound lung comets for the differential diagnosis of acute cardiogenic dyspnoea: A comparison with natriuretic peptides. Eur. J. Heart Fail. 2008, 10, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, P.U.; Gaggin, H.K.; Sheftel, A.D.; Belcher, A.M.; Weiner, R.B.; Baggish, A.L.; Motiwala, S.R.; Liu, P.P.; Januzzi, J.L. Prognostic Usefulness of Insulin-Like Growth Factor-Binding Protein 7 in Heart Failure with Reduced Ejection Fraction: A Novel Biomarker of Myocardial Diastolic Function? Am. J. Cardiol. 2014, 114, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, P.U.; Chow, S.L.; Rector, T.S.; Krum, H.; Gaggin, H.K.; McMurray, J.J.; Zile, M.R.; Komajda, M.; McKelvie, R.S.; Carson, P.E.; et al. Prognostic Value of Insulin-Like Growth Factor-Binding Protein 7 in Patients with Heart Failure and Preserved Ejection Fraction. J. Card. Fail. 2017, 23, 20–28. [Google Scholar] [CrossRef]
- Lisowska, A.; Święcki, P.; Knapp, M.; Gil, M.; Musiał, W.J.; Kamiński, K.; Hirnle, T.; Tycińska, A. Insulin-like growth factor-binding protein 7 (IGFBP 7) as a new biomarker in coronary heart disease. Adv. Med. Sci. 2019, 64, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Barroso, M.C.; Kramer, F.; Greene, S.J.; Scheyer, D.; Köhler, T.; Karoff, M.; Seyfarth, M.; Gheorghiade, M.; Dinh, W. Serum insulin-like growth factor-1 and its binding protein-7: Potential novel biomarkers for heart failure with preserved ejection fraction. BMC Cardiovasc. Disord. 2016, 16, 199. [Google Scholar] [CrossRef]
- Chen, S.; Huang, Z.; Liang, Y.; Zhao, X.; Aobuliksimu, X.; Wang, B.; He, Y.; Kang, Y.; Huang, H.; Li, Q.; et al. Five-year mortality of heart failure with preserved, mildly reduced, and reduced ejection fraction in a 4880 Chinese cohort. ESC Heart Fail. 2022, 9, 2336–2347. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.S.; Xu, H.; Matsouaka, R.A.; Bhatt, D.L.; Heidenreich, P.A.; Hernandez, A.F.; Devore, A.D.; Yancy, C.W.; Fonarow, G.C. Heart Failure with Preserved, Borderline, and Reduced Ejection Fraction: 5-Year Outcomes. J. Am. Coll. Cardiol. 2017, 70, 2476–2486. [Google Scholar] [CrossRef]
- Curtis, J.P.; Sokol, S.I.; Wang, Y.; Rathore, S.S.; Ko, D.T.; Jadbabaie, F.; Portnay, E.L.; Marshalko, S.J.; Radford, M.J.; Krumholz, H.M. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J. Am. Coll. Cardiol. 2003, 42, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Quiroz, R.; Doros, G.; Shaw, P.; Liang, C.-S.; Gauthier, D.F.; Sam, F. Comparison of Characteristics and Outcomes of Patients with Heart Failure Preserved Ejection Fraction Versus Reduced Left Ventricular Ejection Fraction in an Urban Cohort. Am. J. Cardiol. 2014, 113, 691–696. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 143) | EF ≥ 50% (n = 86) | EF 41–49% (n = 57) | p | |
|---|---|---|---|---|
| Age, years | 72.28 ± 10.54 | 72.28 ± 10.79 | 72.28 ± 10.26 | 0.99 |
| Sex (female, %) | 89 (62.24%) | 59 (68.60%) | 30 (52.63%) | 0.08 |
| Left ventricle ejection fraction (%) | 51.04 ± 6.5 | 55.23 ± 4.71 | 44.70 ± 2.38 | |
| NYHA Class II | 114 (79.7%) | 74 (86.05%) | 41 (71.93%) | 0.08 |
| NYHA Class III, IV | 29 (20.3%) | 12 (13.95%) | 16 (28.07%) | 0.08 |
| Systolic BP, mmHg | 145.7 ± 27.9 | 150.3 ± 28.3 | 138.9 ± 26 | 0.02 |
| Diastolic BP, mmHg | 83.4 ± 15.4 | 84.7 ± 14.9 | 81.4 ± 16.1 | 0.21 |
| Heart rate on admission (u/min) | 80.2 ± 20.6 | 79.2 ± 20 | 81.6 ± 21.6 | 0.49 |
| BMI, kg/m2 | 30.02 ± 5.89 | 29.38 ± 5.43 | 31.01 ± 6.5 | 0.15 |
| BSA (m2) | 1.92 ± 0.24 | 1.91 ± 0.23 | 1.93 ± 0.26 | 0.66 |
| Length of hospitalization, days | 4.78 ± 2.73 | 4.62 ± 2.49 | 5.04 ± 3.07 | 0.37 |
| Atrial fibrillation, n (%) | 53 (37.06%) | 28 (32.56%) | 25 (43.86%) | 0.22 |
| Hypertension, n (%) | 128 (89.51%) | 81 (94.19%) | 47 (82.46%) | 0.05 |
| Diabetes t.2, n (%) | 56 (39.16%) | 29 (33.72%) | 27 (47.37%) | 0.12 |
| Hyperlipidemia, n (%) | 103 (72.03%) | 60 (69.77%) | 43 (75.44%) | 0.57 |
| History of myocardial infarction, n (%) | 17 (11.89%) | 2 (2.33%) | 15 (26.32%) | <0.001 |
| Smoking in the present, n (%) | 20 (14.08%) | 7 (8.24%) | 13 (22.81%) | 0.03 |
| EF ≥ 50% (n = 86) | EF 41–49% (n = 57) | p | |
|---|---|---|---|
| LVDd (cm) | 4.82 ± 0.51 | 5.2 ± 0.7 | <0.001 |
| IVSd (cm) | 1.2 ± 0.52 | 1.18 ± 0.19 | 0.72 |
| PWd (cm) | 1.05 ± 0.13 | 1.08 ± 0.13 | 0.16 |
| RVID (cm) | 2.98 ± 0.47 | 3.11 ± 0.5 | 0.13 |
| LVMI (g/m2) | 108.81 ± 29.66 | 124.88 ± 29.13 | 0.003 |
| Ao (cm) | 3.43 ± 0.41 | 3.46 ± 0.39 | 0.67 |
| LA (cm) | 4.36 ± 0.56 | 4.6 ± 0.68 | 0.03 |
| Pulmonary artery systolic pressure (mmHg) | 31.1 ± 11.32 | 38.8 ± 16.39 | 0.009 |
| Mean pulmonary artery pressure (mmHg) | 23.41 ± 8.37 | 29.97 ± 9.45 | 0.02 |
| Right ventricular dimension (cm) | 3.63 ± 0.86 | 4.48 ± 0.84 | <0.001 |
| Inferior vena cava diameter (cm) | 1.82 ± 1.85 | 1.89 ± 0.54 | 0.79 |
| Stiff inferior vena cava (yes, %) | 75 (93.75%) | 40 (81.63%) | 0.04 |
| Hypokinetic right ventricle (yes, %) | 4 (4.88%) | 9 (16.98%) | 0.03 |
| EF ≥ 50% (n = 86) | EF 41–49% (n = 57) | p | |
|---|---|---|---|
| Anticoagulant treatment, n (%) | 41 (47.67%) | 32 (56.14%) | 0.40 |
| Acetylsalicylic acid, n (%) | 25 (29.07%) | 19 (33.33%) | 0.71 |
| Angiotensin-converting enzyme inhibitor, n (%) | 62 (72.09%) | 46 (82.14%) | 0.23 |
| Sartan, n (%) | 17 (19.77%) | 8 (14.04%) | 0.50 |
| Beta-blocker, n (%) | 73 (84.88%) | 51 (89.47%) | 0.46 |
| Aldosterone receptor antagonist, n (%) | 18 (20.93%) | 21 (36.84%) | 0.05 |
| Calcium antagonist, n (%) | 41 (47.67%) | 12 (21.05%) | 0.001 |
| Diuretic, n (%) | 61 (70.93%) | 47 (82.46%) | 0.16 |
| Statin, n (%) | 71 (82.56%) | 41 (71.93%) | 0.15 |
| Antiarrhythmic drug, n (%) | 12 (13.95%) | 9 (15.79%) | 0.81 |
| Oral antidiabetic drug, n (%) | 21 (24.42%) | 21 (37.50%) | 0.13 |
| Insulin, n (%) | 7 (8.14%) | 4 (7.02%) | 1.00 |
| EF ≥ 50% (n = 86) | EF 41–49% (n = 57) | p | |
|---|---|---|---|
| NTproBNP (Me, IQR) (pg/mL) | 649 (256–1421) | 845 (431–2229) | 0.04 |
| Creatinine (mg/dL) | 1.00 ± 0.3 | 1.075 ± 0.44 | 0.24 |
| eGFR (mL/min/1.73 m2) | 71.22 ± 23.84 | 74.26 ± 31.07 | 0.51 |
| Total cholesterol (mg/dL) | 173.42 ± 50.76 | 157.84 ± 58.49 | 0.10 |
| LDL cholesterol (mg/dL) | 111.17 ± 43.89 | 99.93 ± 48.65 | 0.16 |
| HDL cholesterol (mg/dL) | 46.07 ± 12.7 | 40.65 ± 11.85 | 0.01 |
| Triglycerides (mg/dL) | 119.80 ± 52.5 | 111.71 ± 51.44 | 0.37 |
| Glucose (mg/dL) | 109.05 ± 37.37 | 111.75 ± 37.47 | 0.68 |
| CRP (Me, IQR) | 4.05 ± 6.44 | 3.4 ± 11.2 | 0.04 |
| PT (s) | 21.65 ± 12.13 | 23.015 ± 15.68 | 0.67 |
| APTT (s) | 31.92 + 12.66 | 30.98 ± 15.61 | 0.83 |
| INR | 1.67 ± 0.95 | 1.71 ± 1.07 | 0.87 |
| Fibrinogen (mg/dL) | 475.06 ± 257.71 | 331.63 ± 86.93 | 0.16 |
| Hb (g/dL) | 13.32 ± 1.57 | 13.105 ± 1.88 | 0.46 |
| WBC (×109/L) | 7.56 ± 2.00 | 6.85 ± 2.28 | 0.05 |
| PLT (×109/L) | 226.71 ± 72.03 | 198.411 ± 61.41 | 0.02 |
| IGFBP-7 (ng/mL) | 2.59 ± 1.85 | 2.75 ± 2.05 | 0.66 |
| Patients with HFpEF | Patients with HFmrEF | |
|---|---|---|
| Age | r = 0.22, p = 0.03 | NS |
| NYHA class | r = 0.45, p < 0.001 | r = 0.41, p = 0.001 |
| Creatinine concentration | NS | r = 0.3, p = 0.02 |
| NTproBNP concentration | NS | r = 0.41, p = 0.001 |
| Pulmonary artery systolic pressure | r = 0.29, p = 0.02 | r = 0.49, p = 0.002 |
| Number of days of hospitalization | r = 0.33, p = 0.001 | r = 0.47, p = 0.0002 |
| BMI | r = −0.26, p = 0.03 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szyszkowska, A.; Olesiewicz, T.; Płońska-Korabiewska, I.; Tarasiuk, E.; Olesiewicz, B.; Knapp, M.; Śledziewski, R.; Sobkowicz, B.; Lisowska, A. The Importance of Lung Ultrasound and IGFBP7 (Insulin-like Growth Factor Binding Protein 7) Assessment in Diagnosing Patients with Heart Failure. J. Clin. Med. 2024, 13, 2220. https://doi.org/10.3390/jcm13082220
Szyszkowska A, Olesiewicz T, Płońska-Korabiewska I, Tarasiuk E, Olesiewicz B, Knapp M, Śledziewski R, Sobkowicz B, Lisowska A. The Importance of Lung Ultrasound and IGFBP7 (Insulin-like Growth Factor Binding Protein 7) Assessment in Diagnosing Patients with Heart Failure. Journal of Clinical Medicine. 2024; 13(8):2220. https://doi.org/10.3390/jcm13082220
Chicago/Turabian StyleSzyszkowska, Anna, Tomasz Olesiewicz, Izabela Płońska-Korabiewska, Ewa Tarasiuk, Barbara Olesiewicz, Małgorzata Knapp, Rafał Śledziewski, Bożena Sobkowicz, and Anna Lisowska. 2024. "The Importance of Lung Ultrasound and IGFBP7 (Insulin-like Growth Factor Binding Protein 7) Assessment in Diagnosing Patients with Heart Failure" Journal of Clinical Medicine 13, no. 8: 2220. https://doi.org/10.3390/jcm13082220
APA StyleSzyszkowska, A., Olesiewicz, T., Płońska-Korabiewska, I., Tarasiuk, E., Olesiewicz, B., Knapp, M., Śledziewski, R., Sobkowicz, B., & Lisowska, A. (2024). The Importance of Lung Ultrasound and IGFBP7 (Insulin-like Growth Factor Binding Protein 7) Assessment in Diagnosing Patients with Heart Failure. Journal of Clinical Medicine, 13(8), 2220. https://doi.org/10.3390/jcm13082220