
Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade


Abstract
:1. Introduction
2. Current Disparities in ART
3. What Has Been Proposed?
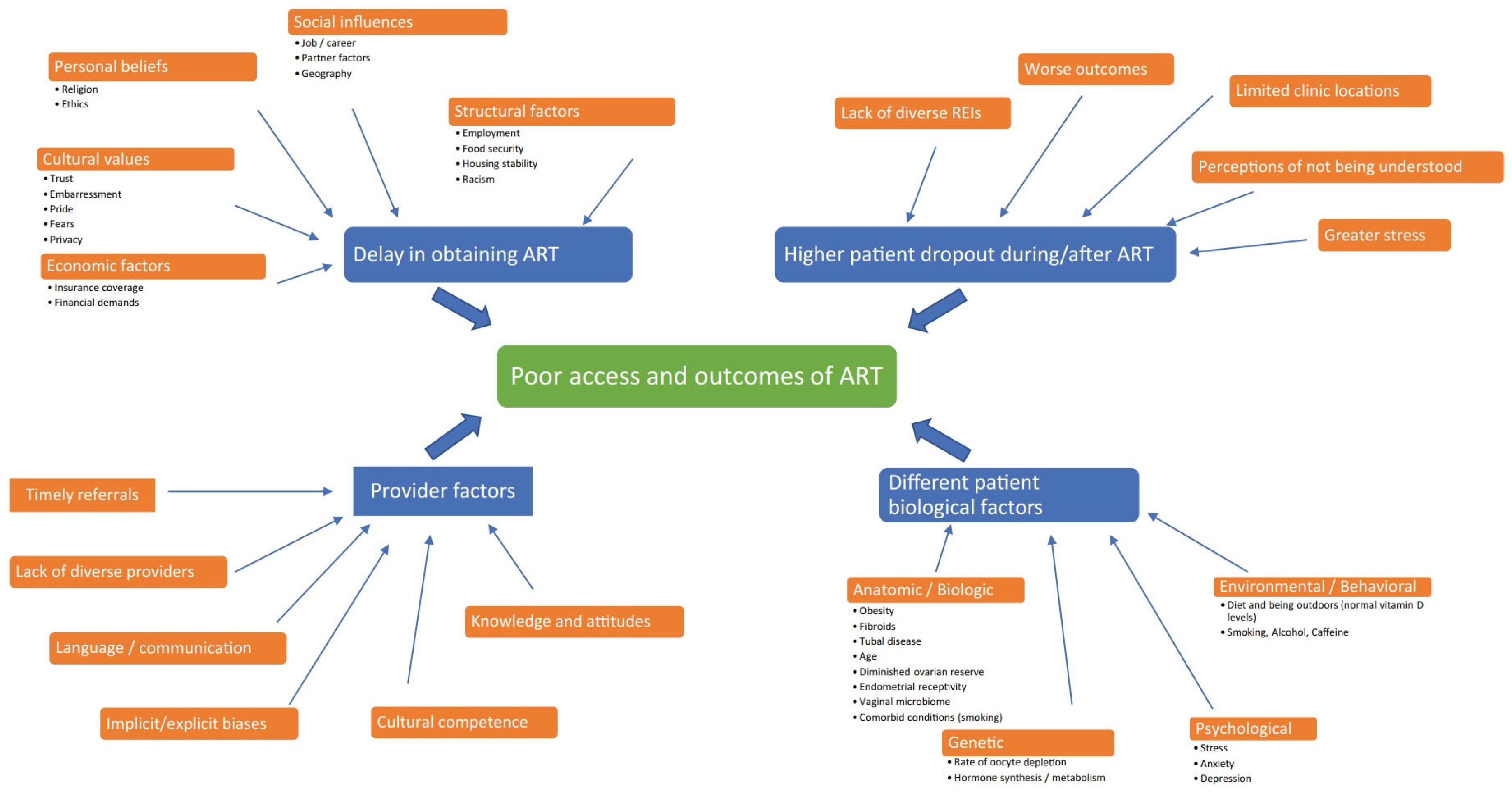
4. Pathways for Accelerated Change—DART Hypothesis Revisited
5. Conclusions
6. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Zegers-Hochschild, F.; Adamson, G.D.; De Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Van Der Poel, S. The International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) Revised Glossary on ART Terminology, 2009. Hum. Reprod. 2009, 24, 2683–2687. [Google Scholar] [CrossRef]
- Shah, P.K.; Gher, J.M. Human Rights Approaches to Reducing Infertility. Int. J. Gynecol. Obstet. 2023, 162, 368–374. [Google Scholar] [CrossRef] [PubMed]
- United Nations. General Assembly. Universal Declaration of Human Rights; United Nations: New York, NY, USA, 1948; Volume 302, pp. 14–25. [Google Scholar]
- Ethics Committee of the American Society for Reproductive Medicine. Disparities in Access to Effective Treatment for Infertility in the United States: An Ethics Committee Opinion. Fertil. Steril. 2021, 116, 54–63. [Google Scholar] [CrossRef] [PubMed]
- ASRM Task Force on Diversity, Equity and Inclusion. Statement of Interest and Concern. Available online: https://www.asrm.org/globalassets/_asrm/about-us/committees/asrm-dei-task-force-report-11-30-2020.pdf (accessed on 1 February 2024).
- Dongarwar, D.; Mercado-Evans, V.; Adu-Gyamfi, S.; Laracuente, M.-L.; Salihu, H.M. Racial/Ethnic Disparities in Infertility Treatment Utilization in the US, 2011–2019. Syst. Biol. Reprod. Med. 2022, 68, 180–189. [Google Scholar] [CrossRef]
- Beroukhim, G.; Mahabamunuge, J.; Pal, L. Racial Disparities in Access to Reproductive Health and Fertility Care in the United States. Curr. Opin. Obstet. Gynecol. 2022, 34, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, E.; Callegari, L.S.; Sileanu, F.E.; Zhao, X.; Schwarz, E.B.; Mor, M.K.; Borrero, S. Racial and Ethnic Disparities in Contraceptive Knowledge among Women Veterans in the ECUUN Study. Contraception 2017, 96, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Buck DiSilvestro, J.; Ulmer, K.K.; Hedges, M.; Kardonsky, K.; Bruegl, A.S. Cervical Cancer. Obstet. Gynecol. Clin. N. Am. 2024, 51, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.W.; Lattimore, D.C.; Harlin, E.; Davis, L.; Erholtz, V.; Brandt, H.M. Medical and Public Health Professionals’ Perceived Facilitators and Barriers of Human Papillomavirus (HPV) Vaccination among African American Adolescents in Shelby County, Tennessee. BMC Health Serv. Res. 2023, 23, 469. [Google Scholar] [CrossRef] [PubMed]
- Garcia, G.; Richardson, D.M.; Gonzales, K.L.; Cuevas, A.G. Trends and Disparities in Postpartum Sterilization after Cesarean Section, 2000 through 2008. Women’s Health Issues 2015, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Bleil, M.E.; Gregorich, S.E.; Adler, N.E.; Sternfeld, B.; Rosen, M.P.; Cedars, M.I. Race/Ethnic Disparities in Reproductive Age: An Examination of Ovarian Reserve Estimates across Four Race/Ethnic Groups of Healthy, Regularly Cycling Women. Fertil. Steril. 2014, 101, 199–207. [Google Scholar] [CrossRef]
- Seifer, D.B.; Zackula, R.; Grainger, D.A. Trends of Racial Disparities in Assisted Reproductive Technology Outcomes in Black Women Compared with White Women: Society for Assisted Reproductive Technology 1999 and 2000 vs. 2004–2006. Fertil. Steril. 2010, 93, 626–635. [Google Scholar] [CrossRef]
- Craig, L.B.; Peck, J.D.; Janitz, A.E. The Prevalence of Infertility in American Indian/Alaska Natives and Other Racial/Ethnic Groups: National Survey of Family Growth. Paediatr. Perinat. Epidemiol. 2019, 33, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.H.; Homan, P. Structural Racism and Health Stratification: Connecting Theory to Measurement. J. Health Soc. Behav. 2024, 65, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Smedley, A.; Smedley, B.D. Race as Biology Is Fiction, Racism as a Social Problem Is Real: Anthropological and Historical Perspectives on the Social Construction of Race. Am. Psychol. 2005, 60, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. 2021 National ART Summary; Center for Disease Control and Prevention: Atlanta, GA, USA, 2023. [Google Scholar]
- Janitz, A.E.; Peck, J.D.; Craig, L.B. Racial/Ethnic Differences in the Utilization of Infertility Services: A Focus on American Indian/Alaska Natives. Matern. Child Health J. 2019, 23, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Chin, H.B.; Howards, P.P.; Kramer, M.R.; Mertens, A.C.; Spencer, J.B. Racial Disparities in Seeking Care for Help Getting Pregnant. Paediatr. Perinat. Epidemiol. 2015, 29, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Gadson, A.K.; Sauerbrun-Cutler, M.-T.; Eaton, J.L. Racial Disparities in Fertility Care: A Narrative Review of Challenges in the Utilization of Fertility Preservation and ART in Minority Populations. J. Clin. Med. 2024, 13, 1060. [Google Scholar] [CrossRef]
- Katler, Q.S.; Shandley, L.M.; Hipp, H.S.; Kawwass, J.F. National Egg-Freezing Trends: Cycle and Patient Characteristics with a Focus on Race/Ethnicity. Fertil. Steril. 2021, 116, 528–537. [Google Scholar] [CrossRef]
- Tarrash, M.; Kuyoro, O.; Goldman, R.; Mullin, C. Characteristics of Patients Seeking Fertility Care in a Low-Income Setting. JBRA Assist. Reprod. 2024, 28, 59. [Google Scholar] [CrossRef] [PubMed]
- Mackay, A.; Taylor, S.; Glass, B. Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies. Pharmacy 2023, 11, 17. [Google Scholar] [CrossRef]
- Letourneau, J.M.; Smith, J.F.; Ebbel, E.E.; Craig, A.; Katz, P.P.; Cedars, M.I.; Rosen, M.P. Racial, Socioeconomic, and Demographic Disparities in Access to Fertility Preservation in Young Women Diagnosed with Cancer: Fertility Preservation Disparities. Cancer 2012, 118, 4579–4588. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.A.; Spurlin, E.E.; Jimenez, P.T. Disparities in Female Oncofertility Care in the United States: More Questions Than Answers. Life 2023, 13, 1547. [Google Scholar] [CrossRef] [PubMed]
- Goodman, L.R.; Balthazar, U.; Kim, J.; Mersereau, J.E. Trends of Socioeconomic Disparities in Referral Patterns for Fertility Preservation Consultation. Hum. Reprod. 2012, 27, 2076–2081. [Google Scholar] [CrossRef]
- Missmer, S.A.; Seifer, D.B.; Jain, T. Cultural Factors Contributing to Health Care Disparities among Patients with Infertility in Midwestern United States. Fertil. Steril. 2011, 95, 1943–1949. [Google Scholar] [CrossRef]
- Blair, I.V.; Steiner, J.F.; Fairclough, D.L.; Hanratty, R.; Price, D.W.; Hirsh, H.K.; Wright, L.A.; Bronsert, M.; Karimkhani, E.; Magid, D.J.; et al. Clinicians’ Implicit Ethnic/Racial Bias and Perceptions of Care Among Black and Latino Patients. Ann. Fam. Med. 2013, 11, 43–52. [Google Scholar] [CrossRef]
- Gonzalez, C.M.; Ark, T.K.; Fisher, M.R.; Marantz, P.R.; Burgess, D.J.; Milan, F.; Samuel, M.T.; Lypson, M.L.; Rodriguez, C.J.; Kalet, A.L. Racial Implicit Bias and Communication Among Physicians in a Simulated Environment. JAMA Netw. Open 2024, 7, e242181. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetrics and Gynecology. Joint Statement: Collective Action Addressing Racism; American College of Obstetrics and Gynecology: Washington, DC, USA, 2020. [Google Scholar]
- Beroukhim, G.; Seifer, D.B. Racial and Ethnic Disparities in Access to and Outcomes of Infertility Treatment and Assisted Reproductive Technology in the United States. Endocrinol. Metab. Clin. N. Am. 2023, 52, 659–675. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, E.C.; Larsen, F.W.; Catherino, W.H.; Zhang, J.; Armstrong, A.Y. Comparison of Assisted Reproductive Technology Utilization and Outcomes between Caucasian and African American Patients in an Equal-Access-to-Care Setting. Fertil. Steril. 2006, 85, 888–894. [Google Scholar] [CrossRef] [PubMed]
- McQueen, D.B.; Schufreider, A.; Lee, S.M.; Feinberg, E.C.; Uhler, M.L. Racial Disparities in In Vitro Fertilization Outcomes. Fertil. Steril. 2015, 104, 398–402.e1. [Google Scholar] [CrossRef] [PubMed]
- Csokmay, J.M.; Hill, M.J.; Maguire, M.; Payson, M.D.; Fujimoto, V.Y.; Armstrong, A.Y. Are There Ethnic Differences in Pregnancy Rates in African-American versus White Women Undergoing Frozen Blastocyst Transfers? Fertil. Steril. 2011, 95, 89–93. [Google Scholar] [CrossRef]
- Seifer, D.B.; Simsek, B.; Wantman, E.; Kotlyar, A.M. Status of Racial Disparities between Black and White Women Undergoing Assisted Reproductive Technology in the US. Reprod. Biol. Endocrinol. 2020, 18, 113. [Google Scholar] [CrossRef]
- Heyward, Q.; Walter, J.R.; Alur-Gupta, S.; Lal, A.; Berger, D.S.; Koelper, N.; Butts, S.F.; Gracia, C.R. Racial Disparities in Frozen Embryo Transfer Success. J. Assist. Reprod. Genet. 2021, 38, 3069–3075. [Google Scholar] [CrossRef]
- Makhijani, R.; Godiwala, P.; Grady, J.; Christy, A.; Thornton, K.; Grow, D.; Engmann, L. Black Race Associated with Lower Live Birth Rate in Frozen-Thawed Blastocyst Transfer Cycles: An Analysis of 7,002 Society for Assisted Reproductive Technology Frozen-Thawed Blastocyst Transfer Cycles. Fertil. Steril. 2022, 117, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Craig, L.B.; Weedin, E.A.; Walker, W.D.; Janitz, A.E.; Hansen, K.R.; Peck, J.D. Racial and Ethnic Differences in Pregnancy Rates Following Intrauterine Insemination with a Focus on American Indians. J. Racial Ethn. Health Disparities 2018, 5, 1077–1083. [Google Scholar] [CrossRef]
- Andre, K.E.; Hood, R.B.; Gaskins, A.J.; Kawwass, J.F.; Almquist, R.G.; Kramer, M.R.; Hipp, H.S. Neighborhood Deprivation and Racial Differences in In Vitro Fertilization Outcomes. Am. J. Obstet. Gynecol. 2024, 230, 352.e1–352.e18. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, I.; Batsis, M.; Petrozza, J.C.; Souter, I. Racial Disparities in Fertility Care: An Analysis of 4537 Intrauterine Insemination Cycles. J. Racial Ethn. Health Disparities 2017, 4, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Seifer, D.B.; Golub, E.T.; Lambert-Messerlian, G.; Benning, L.; Anastos, K.; Watts, D.H.; Cohen, M.H.; Karim, R.; Young, M.A.; Minkoff, H.; et al. Variations in Serum Müllerian Inhibiting Substance between White, Black, and Hispanic Women. Fertil. Steril. 2009, 92, 1674–1678. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Berger, D.S.; Koelper, N.; Senapati, S.; Mainigi, M. Race, Ovarian Responsiveness, and Live Birth after In Vitro Fertilization. Fertil. Steril. 2023, 120, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hipp, H.S.; Nagy, Z.P.; Capelouto, S.M.; Shapiro, D.B.; Spencer, J.B.; Gaskins, A.J. The Effect of Donor and Recipient Race on Outcomes of Assisted Reproduction. Am. J. Obstet. Gynecol. 2021, 224, 374-e1. [Google Scholar] [CrossRef]
- Hill, M.J.; Royster, G.D.; Taneja, M.; Healy, M.W.; Zarek, S.M.; Christy, A.Y.; DeCherney, A.H.; Widra, E.; Devine, K. Does Elevated Progesterone on Day of Oocyte Maturation Play a Role in the Racial Disparities in IVF Outcomes? Reprod. Biomed. Online 2017, 34, 154–161. [Google Scholar] [CrossRef]
- McKenzie-Sampson, S.; Baer, R.J.; Jelliffe-Pawlowski, L.L.; Karasek, D.; Riddell, C.A.; Torres, J.M.; Blebu, B.E. Structural Racism, Nativity and Risk of Adverse Perinatal Outcomes among Black Women. Paediatr. Perinat. Epidemiol. 2024, 38, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Janevic, T.; McCarthy, K.; Liu, S.H.; Huyhn, M.; Kennedy, J.; Tai Chan, H.; Mayer, V.L.; Vieira, L.; Tabaei, B.; Howell, F.; et al. Racial and Ethnic Inequities in Development of Type 2 Diabetes After Gestational Diabetes Mellitus. Obstet. Gynecol. 2023, 142, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Garland, C.E.; Geller, S.E.; Koch, A.R. Adverse Delivery and Neonatal Outcomes Among Women with Severe Maternal Morbidity in Illinois, 2018–2019. J. Women’s Health 2024, 33, 163–170. [Google Scholar] [CrossRef] [PubMed]
- McCarthy-Keith, D.M.; Schisterman, E.F.; Robinson, R.D.; O’Leary, K.; Lucidi, R.S.; Armstrong, A.Y. Will Decreasing Assisted Reproduction Technology Costs Improve Utilization and Outcomes among Minority Women? Fertil. Steril. 2010, 94, 2587–2589. [Google Scholar] [CrossRef] [PubMed]
- Kawwass, J.F.; Penzias, A.S.; Adashi, E.Y. Fertility—A Human Right Worthy of Mandated Insurance Coverage: The Evolution, Limitations, and Future of Access to Care. Fertil. Steril. 2021, 115, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Korkidakis, A.; DeSantis, C.E.; Kissin, D.M.; Hacker, M.R.; Koniares, K.; Yartel, A.; Adashi, E.Y.; Penzias, A.S. State Insurance Mandates and Racial and Ethnic Inequities in Assisted Reproductive Technology Utilization. Fertil. Steril. 2024, 121, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Vu, M.; Stuehling, D.; Li, D.; Alur-Gupta, S. Fertility Care for All: Impact of New York State’s Medicaid Expansion on Infertility Care. J. Assist. Reprod. Genet. 2023, 41, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Kotlyar, A.M.; Seifer, D.B. Effect of State Insurance Mandates on Racial/Ethnic Disparities in the Utilization and Outcomes of Donor Oocyte–Assisted Reproductive Technologies. Fertil. Steril. 2023, 120, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Correia, K.F.B.; Kraschel, K.; Seifer, D.B. State Insurance Mandates for In Vitro Fertilization Are Not Associated with Improving Racial and Ethnic Disparities in Utilization and Treatment Outcomes. Am. J. Obstet. Gynecol. 2023, 228, 313.e1–313.e8. [Google Scholar] [CrossRef] [PubMed]
- Koniares, K.G.; Penzias, A.S.; Roosevelt, J.; Adashi, E.Y. The Massachusetts Infertility Insurance Mandate: Not Nearly Enough. FS Rep. 2022, 3, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Hariton, E.; Alvero, R.; Hill, M.J.; Mersereau, J.E.; Perman, S.; Sable, D.; Wang, F.; Adamson, G.D.; Coutifaris, C.; Craig, L.B.; et al. Meeting the Demand for Fertility Services: The Present and Future of Reproductive Endocrinology and Infertility in the United States. Fertil. Steril. 2023, 120, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Adeleye, A.J.; Kawwass, J.F.; Brauer, A.; Storment, J.; Patrizio, P.; Feinberg, E. The Mismatch in Supply and Demand: Reproductive Endocrinology and Infertility Workforce Challenges and Controversies. Fertil. Steril. 2023, 120, 403–405. [Google Scholar] [CrossRef]
- Brodeur, T.Y.; Grow, D.; Esfandiari, N. Access to Fertility Care in Geographically Underserved Populations, a Second Look. Reprod. Sci. 2022, 29, 1983–1987. [Google Scholar] [CrossRef]
- Blakemore, J.K.; Maxwell, S.M.; Hodes-Wertz, B.; Goldman, K.N. Access to Infertility Care in a Low-Resource Setting: Bridging the Gap through Resident and Fellow Education in a New York City Public Hospital. J. Assist. Reprod. Genet. 2020, 37, 1545–1552. [Google Scholar] [CrossRef]
- Seifer, D.B.; Sharara, F.I.; Jain, T. Toward a Better Understanding of Racial Disparities in Utilization and Outcomes of IVF Treatment in the USA. In Ethnic Differences in Fertility and Assisted Reproduction; Sharara, F.I., Ed.; Springer: New York, NY, USA, 2013; pp. 239–244. [Google Scholar] [CrossRef]
- Seifer, D.B.; Sharara, F.I.; Jain, T. The Disparities in ART (DART) Hypothesis of Racial and Ethnic Disparities in Access and Outcomes of IVF Treatment in the USA. Reprod. Sci. 2022, 29, 2084–2088. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, V.Y.; Jain, T.; Alvero, R.; Nelson, L.M.; Catherino, W.H.; Olatinwo, M.; Marsh, E.E.; Broomfield, D.; Taylor, H.; Armstrong, A.Y. Proceedings from the Conference on Reproductive Problems in Women of Color. Fertil. Steril. 2010, 94, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Delbaere, I.; Verbiest, S.; Tydén, T. Knowledge about the Impact of Age on Fertility: A Brief Review. Ups. J. Med. Sci. 2020, 125, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.J.; Danhof, N.A.; Mochtar, M.H.; Van Wely, M.; McLernon, D.J.; Custers, I.; Lee, E.; Dreyer, K.; Cahill, D.J.; Gillett, W.R.; et al. Age-Related Natural Fertility Outcomes in Women over 35 Years: A Systematic Review and Individual Participant Data Meta-Analysis. Hum. Reprod. 2020, 35, 1808–1820. [Google Scholar] [CrossRef] [PubMed]
- Kudesia, R.; Chernyak, E.; McAvey, B. Low Fertility Awareness in United States Reproductive-Aged Women and Medical Trainees: Creation and Validation of the Fertility & Infertility Treatment Knowledge Score (FIT-KS). Fertil. Steril. 2017, 108, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Rayburn, W.F. Diversity in Academic Obstetrics and Gynecology. Obstet. Gynecol. Clin. N. Am. 2024, 51, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Gomez, L.E.; Bernet, P. Diversity Improves Performance and Outcomes. J. Natl. Med. Assoc. 2019, 111, 383–392. [Google Scholar] [CrossRef]
- Galic, I.; Swanson, A.; Warren, C.; Negris, O.; Bozen, A.; Brown, D.; Lawson, A.; Jain, T. Infertility in the Midwest: Perceptions and Attitudes of Current Treatment. Am. J. Obstet. Gynecol. 2021, 225, 61.e1–61.e11. [Google Scholar] [CrossRef] [PubMed]
- Almquist, R.G.; Barrera, C.M.; Fried, R.; Boulet, S.L.; Kawwass, J.F.; Hipp, H.S. Impact of Access to Care and Race/Ethnicity on IVF Care Discontinuation. Reprod. Biomed. Online 2022, 44, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Chambers, G.M.; Sullivan, E.A.; Ishihara, O.; Chapman, M.G.; Adamson, G.D. The Economic Impact of Assisted Reproductive Technology: A Review of Selected Developed Countries. Fertil. Steril. 2009, 91, 2281–2294. [Google Scholar] [CrossRef]
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [CrossRef] [PubMed]
- Polyzos, N.P.; Ayoubi, J.M.; Pirtea, P. General Infertility Workup in Times of High Assisted Reproductive Technology Efficacy. Fertil. Steril. 2022, 118, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Alkon-Meadows, T.; Hernandez-Nieto, C.; Jackson-Bey, T.; Cacchione, T.A.; Lee, J.; Luna-Rojas, M.; Gounko, D.; Copperman, A.; Buyuk, E. Correlation of Self-Reported Racial Background to Euploidy Status and Live Birth Rates in Assisted Reproductive Technology Cycles. J. Assist. Reprod. Genet. 2024, 41, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Gopal, D.P.; Chetty, U.; O’Donnell, P.; Gajria, C.; Blackadder-Weinstein, J. Implicit Bias in Healthcare: Clinical Practice, Research and Decision Making. Future Healthc. J. 2021, 8, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Olive, E.; Bull, C.; Gordon, A.; Davies-Tuck, M.; Wang, R.; Callander, E. Economic Evaluations of Assisted Reproductive Technologies in High-Income Countries: A Systematic Review. Hum. Reprod. 2024, deae039. [Google Scholar] [CrossRef] [PubMed]
- Butts, S.F. Health Disparities of African Americans in Reproductive Medicine. Fertil. Steril. 2021, 116, 287–291. [Google Scholar] [CrossRef]
- Volovsky, M.; Seifer, D.B. State Insurance Mandates Are Necessary but Not Sufficient for Closing the Racial and Ethnic Disparity Gap in Assisted Reproductive Technology. Fertil. Steril. 2024, 121, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Seifer, D.B.; Wantman, E.; Sparks, A.E.; Luke, B.; Doody, K.J.; Toner, J.P.; Van Voorhis, B.J.; Lin, P.C.; Reindollar, R.H. National Survey of the Society for Assisted Reproductive Technology Membership Regarding Insurance Coverage for Assisted Reproductive Technologies. Fertil. Steril. 2018, 110, 1081–1088.e1. [Google Scholar] [CrossRef] [PubMed]
- Seifer, D.B.; Richard-Davis, G.; Alvero, R. Closing the Gap on Racial Disparities—Increasing Race/Ethnicity Demographics Reporting in the SART CORS Registry. Fertil. Steril. 2024. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Problem | Solution |
|---|---|
| Financial obstacles leading to decreased care utilization |
|
| Delayed presentation due to insufficient understanding of age-related infertility and available resources |
|
| Delayed presentation for care due to stigma and shame |
|
| Delayed presentation due to difficulty finding providers patients are comfortable with |
|
| Provider bias and inconsistent counseling |
|
| Inconsistent follow up due to burden of travel outside of underserved areas |
|
| Inadequate research identifying and addressing factors contributing to poorer outcomes |
|
| Poorer ART outcomes in racial/ethnic minorities |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahabamunuge, J.; Seifer, D.B. Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade. J. Clin. Med. 2024, 13, 2224. https://doi.org/10.3390/jcm13082224
Mahabamunuge J, Seifer DB. Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade. Journal of Clinical Medicine. 2024; 13(8):2224. https://doi.org/10.3390/jcm13082224
Chicago/Turabian StyleMahabamunuge, Jasmin, and David B. Seifer. 2024. "Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade" Journal of Clinical Medicine 13, no. 8: 2224. https://doi.org/10.3390/jcm13082224
APA StyleMahabamunuge, J., & Seifer, D. B. (2024). Moving toward Narrowing the United States Gap in Assisted Reproductive Technology (ART) Racial and Ethnic Disparities in the Next Decade. Journal of Clinical Medicine, 13(8), 2224. https://doi.org/10.3390/jcm13082224