
Assessment of the Impact of SARS-CoV-2 Infection on the Sexual Function of Women, Levels of Oxytocin and Prolactin: A Prospective Cohort Study
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
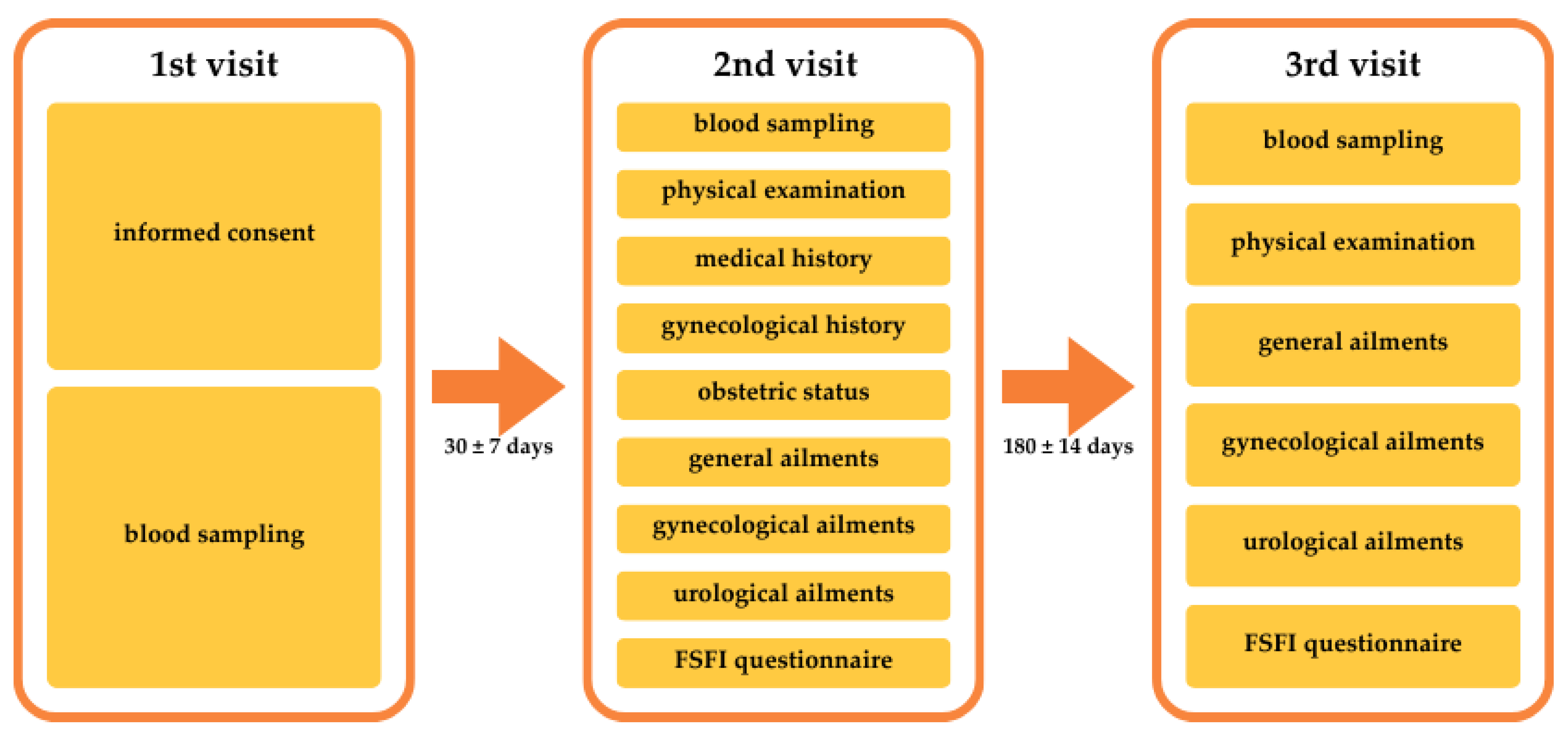
2.2. Study Procedures
2.3. Clinical Assessment
2.4. Blood Sampling and Analysis
2.5. FSFI
2.6. Oxytocin and Prolactin Assessment
2.7. Statistical Analysis
3. Results
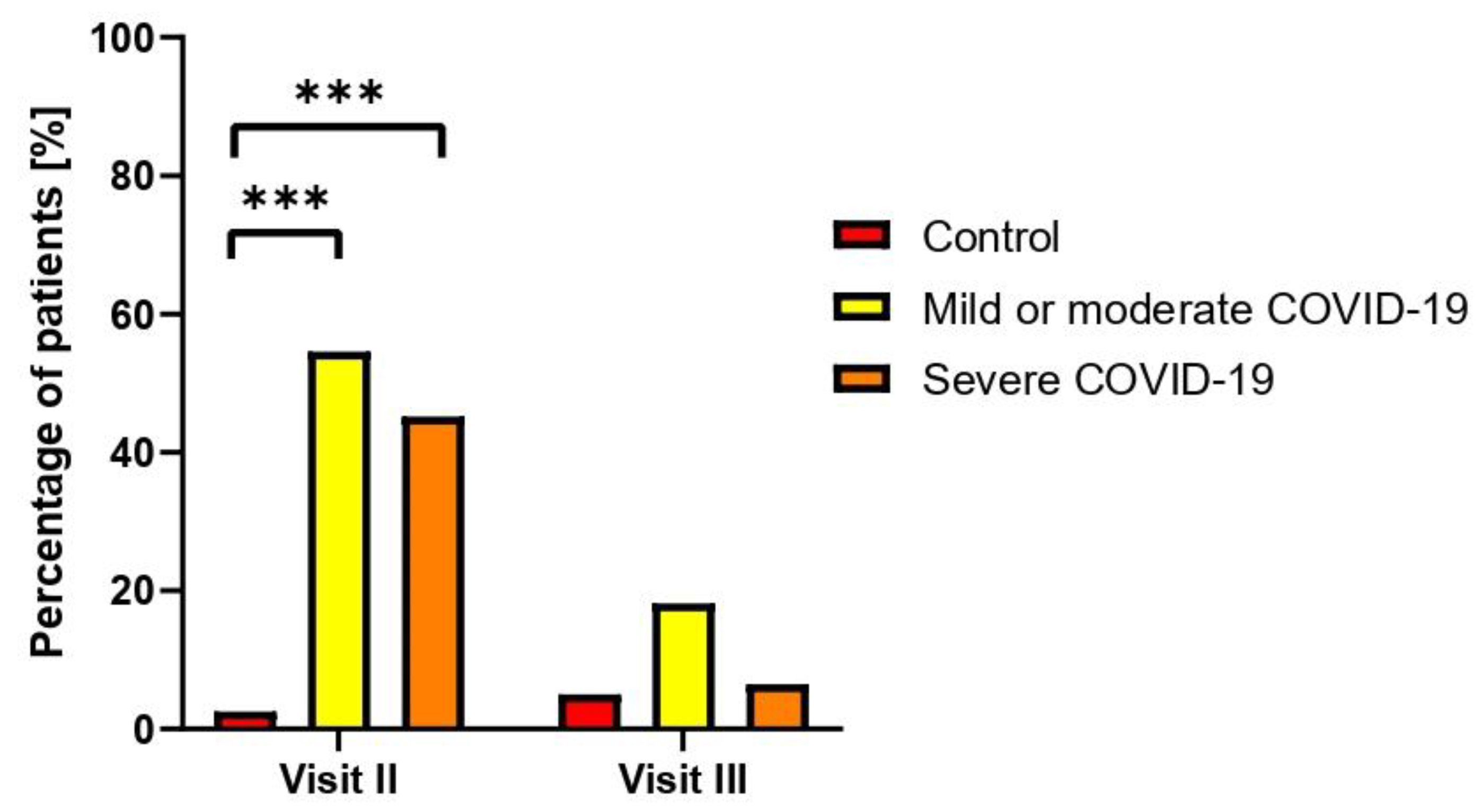
3.1. Clinical Assessment
3.2. FSFI Evaluation
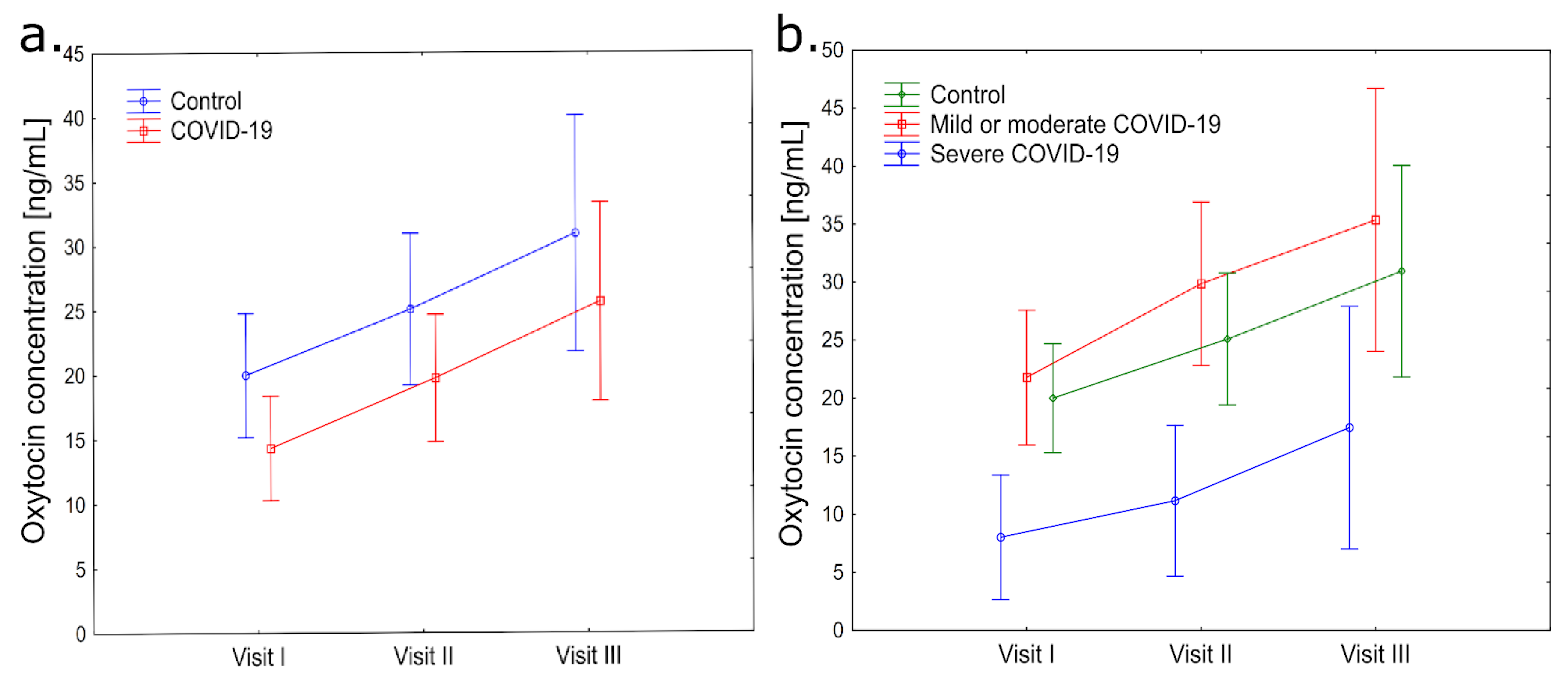
3.3. Oxytocin
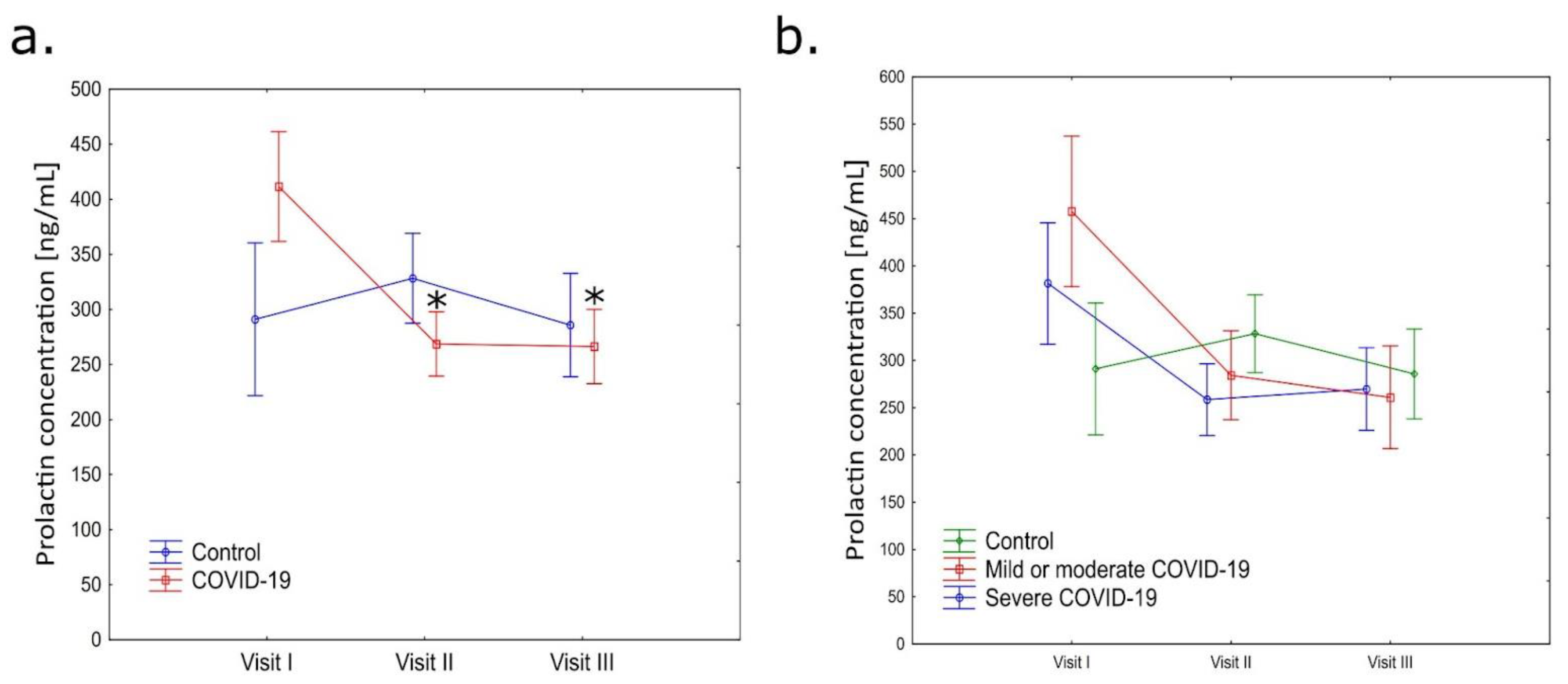
3.4. Prolactin
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chakraborty, I.; Maity, P. COVID-19 Outbreak: Migration, Effects on Society, Global Environment and Prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Miyah, Y.; Benjelloun, M.; Lairini, S.; Lahrichi, A. COVID-19 Impact on Public Health, Environment, Human Psychology, Global Socioeconomy, and Education. Sci. World J. 2022, 2022, 5578284. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.A.; Mohammad, D.; Qureshi, M.F.H.; Abbas, M.Z.; Aleem, S. Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Ment. Health J. 2021, 57, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Tarazona, V.; Kirouchena, D.; Clerc, P.; Pinsard-Laventure, F.; Bourrion, B. Quality of Life in COVID-19 Outpatients: A Long-Term Follow-Up Study. J. Clin. Med. 2022, 11, 6478. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The Psychological Impact of COVID-19 on the Mental Health in the General Population. QJM Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Alzueta, E.; Perrin, P.; Baker, F.C.; Caffarra, S.; Ramos-Usuga, D.; Yuksel, D.; Arango-Lasprilla, J.C. How the COVID-19 Pandemic Has Changed Our Lives: A Study of Psychological Correlates across 59 Countries. J. Clin. Psychol. 2021, 77, 556–570. [Google Scholar] [CrossRef]
- Wang, X.; Lei, S.M.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional Influence of the COVID-19 Pandemic Lockdowns on Health Behaviors and Quality of Life among Chinese Adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef]
- Fuchs, A.; Matonóg, A.; Pilarska, J.; Sieradzka, P.; Szul, M.; Czuba, B.; Drosdzol-Cop, A. The Impact of COVID-19 on Female Sexual Health. Int. J. Environ. Res. Public Health 2020, 17, 7152. [Google Scholar] [CrossRef]
- Toldam, N.E.; Graugaard, C.; Meyer, R.; Thomsen, L.; Dreier, S.; Jannini, E.A.; Giraldi, A. Sexual Health During COVID-19: A Scoping Review. Sex. Med. Rev. 2022, 10, 714–753. [Google Scholar] [CrossRef]
- Sexual Health. Available online: https://www.who.int/health-topics/sexual-health (accessed on 3 June 2023).
- Furukawa, A.P.; Patton, P.E.; Amato, P.; Li, H.; Leclair, C.M. Dyspareunia and Sexual Dysfunction in Women Seeking Fertility Treatment. Fertil. Steril. 2012, 98, 1544–1548. [Google Scholar] [CrossRef] [PubMed]
- Hussein, J. COVID-19: What Implications for Sexual and Reproductive Health and Rights Globally? Sex. Reprod. Health Matters 2020, 28, 1746065. [Google Scholar] [CrossRef] [PubMed]
- Roser, K.; Baenziger, J.; Ilic, A.; Mitter, V.R.; Mader, L.; Dyntar, D.; Michel, G.; Sommer, G. Health-Related Quality of Life before and during the COVID-19 Pandemic in Switzerland: A Cross-Sectional Study. Qual. Life Res. 2023, 32, 2695–2706. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, B.; Ozgor, F. Effect of the COVID-19 Pandemic on Female Sexual Behavior. Int. J. Gynaecol. Obstet. 2020, 150, 98–102. [Google Scholar] [CrossRef]
- Narkkul, U.; Jiet Ng, J.; Saraluck, A. Impact of the COVID-19 Pandemic on the Female Sexual Function Index and Female Behavioral Changes: A Cross-Sectional Survey Study in Thailand. Int. J. Environ. Res. Public Health 2022, 19, 15565. [Google Scholar] [CrossRef] [PubMed]
- Hessami, K.; Sayegh, N.; Abdolmaleki, A.S.; Bakht, S.; Qaderi, S.; Darabi, M.; Shamsi, T.; Bagheri, F. Women’s Sexual Function before and during COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Obstet. Gynaecol. Res. 2022, 48, 2285–2295. [Google Scholar] [CrossRef] [PubMed]
- Qaderi, K.; Yazdkhasti, M.; Zangeneh, S.; Behbahani, B.M.; Kalhor, M.; Shamsabadi, A.; Jesmani, Y.; Norouzi, S.; Kajbafvala, M.; Khodavirdilou, R.; et al. Changes in Sexual Activities, Function, and Satisfaction during the COVID-19 Pandemic Era: A Systematic Review and Meta-Analysis. Sex. Med. 2023, 11, qfad005. [Google Scholar] [CrossRef] [PubMed]
- Pérez-López, F.R.; López-Baena, M.T.; Pérez-Roncero, G.; Dieste-Pérez, P.; Savirón-Cornudella, R.; Tajada, M. Female Sexual Function before and during the Severe Acute Respiratory Syndrome Coronavirus-2 Pandemic: A Systematic Review and Meta-Analysis of Longitudinal Studies. Gynecol. Endocrinol. 2022, 38, 632–638. [Google Scholar] [CrossRef]
- Iuliano, S.; Zagari, M.C.; Frasca Polara, G.; Rotella, G.; LA Vignera, S.; Greco, E.A.; Liuzza, M.T.; Aversa, A. Global Olfactory Function Correlates with Global Sexual Functioning in Men and Women. Minerva Med. 2023, 114, 785–794. [Google Scholar] [CrossRef]
- Gencer, F.K.; Yuksel, S.; Salman, S.; Kumbasar, S.; Kobaner, N. Evaluation of Women’s Sexual Functions after COVID-19 Infection. Med. Bull. Sisli Etfal Hosp. 2022, 56, 328–333. [Google Scholar] [CrossRef]
- Nawaz, M.U.; Rivera, E.; Vinayak, S.; Elahi, K.; Kumar, M.; Chand, M.; Ezae, S.; Khalid, D.; Naz, S.; Shaukat, F. Comparison of Sexual Function before and after COVID-19 Infection in Female Patients. Cureus 2021, 13, e18156. [Google Scholar] [CrossRef]
- Kaya, Y.; Kaya, C.; Tahta, T.; Kartal, T.; Tokgöz, V.Y. Examination of the Effect of COVID-19 on Sexual Dysfunction in Women. Int. J. Clin. Pract. 2021, 75, e13923. [Google Scholar] [CrossRef]
- Davis, S.R.; Guay, A.T.; Shifren, J.L.; Mazer, N.A. Endocrine Aspects of Female Sexual Dysfunction. J. Sex. Med. 2004, 1, 82–86. [Google Scholar] [CrossRef]
- Gomuła, A. Wpływ hormonów płciowych i neurotransmiterów na funkcje i zachowania seksualne. J. Sex. Ment. Health 2006, 4, 21–33. [Google Scholar]
- Afshari, P.; Zakerkish, M.; Abedi, P.; Beheshtinasab, M.; Maraghi, E.; Meghdadi, H. Effect of COVID-19 Infection on Sex Hormone Levels in Hospitalized Patients: A Prospective Longitudinal Study in Iran. Health Sci. Rep. 2022, 6, e1011. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Zhong, J.; Jiang, Y.; Zhang, J. Associations between COVID-19 Infection and Sex Steroid Hormones. Front. Endocrinol. 2022, 13, 940675. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.C.; Wang, Y.-F. Cardiovascular Protective Properties of Oxytocin against COVID-19. Life Sci. 2021, 270, 119130. [Google Scholar] [CrossRef]
- Diep, P.-T. TRPV1, Nrf2, and COVID-19: Could Oxytocin Have a Beneficial Role to Play? Int. Arch. Allergy Immunol. 2022, 183, 246–247. [Google Scholar] [CrossRef]
- Imami, A.S.; O’Donovan, S.M.; Creeden, J.F.; Wu, X.; Eby, H.; McCullumsmith, C.B.; Uvnäs-Moberg, K.; McCullumsmith, R.E.; Andari, E. Oxytocin’s Anti-Inflammatory and Proimmune Functions in COVID-19: A Transcriptomic Signature-Based Approach. Physiol. Genom. 2020, 52, 401–407. [Google Scholar] [CrossRef]
- Wang, S.C.; Zhang, F.; Zhu, H.; Yang, H.; Liu, Y.; Wang, P.; Parpura, V.; Wang, Y.-F. Potential of Endogenous Oxytocin in Endocrine Treatment and Prevention of COVID-19. Front. Endocrinol. 2022, 13, 799521. [Google Scholar] [CrossRef]
- Diep, P.-T.; Talash, K.; Kasabri, V. Hypothesis: Oxytocin Is a Direct COVID-19 Antiviral. Med. Hypotheses 2020, 145, 110329. [Google Scholar] [CrossRef] [PubMed]
- Diep, P.-T.; Chaudry, M.; Dixon, A.; Chaudry, F.; Kasabri, V. Oxytocin, the Panacea for Long-COVID? A Review. Horm. Mol. Biol. Clin. Investig. 2022, 43, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Butnariu, M.; Batiha, G.E.-S. The Crucial Role of Prolactin-Lactogenic Hormone in Covid-19. Mol. Cell. Biochem. 2022, 477, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Goel, H.; Gupta, I.; Mourya, M.; Gill, S.; Chopra, A.; Ranjan, A.; Rath, G.K.; Tanwar, P. A Systematic Review of Clinical and Laboratory Parameters of 3,000 COVID-19 Cases. Obstet. Gynecol. Sci. 2021, 64, 174–189. [Google Scholar] [CrossRef] [PubMed]
- Ding, T.; Wang, T.; Zhang, J.; Cui, P.; Chen, Z.; Zhou, S.; Yuan, S.; Ma, W.; Zhang, M.; Rong, Y.; et al. Analysis of Ovarian Injury Associated With COVID-19 Disease in Reproductive-Aged Women in Wuhan, China: An Observational Study. Front. Med. 2021, 8, 635255. [Google Scholar] [CrossRef] [PubMed]
- Sen, A. Repurposing Prolactin as a Promising Immunomodulator for the Treatment of COVID-19: Are Common Antiemetics the Wonder Drug to Fight Coronavirus? Med. Hypotheses 2020, 144, 110208. [Google Scholar] [CrossRef] [PubMed]
- Zik, J.B.; Roberts, D.L. The Many Faces of Oxytocin: Implications for Psychiatry. Psychiatry Res. 2015, 226, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Yang, H.; Han, L.; Ma, M. Oxytocin in Women’s Health and Disease. Front. Endocrinol. 2022, 13, 786271. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, M.S.; Humbert, R.; Dixen, J.; Palmisano, G.; Greenleaf, W.; Davidson, J.M. Plasma Oxytocin Increases in the Human Sexual Response. J. Clin. Endocrinol. Metab. 1987, 64, 27–31. [Google Scholar] [CrossRef]
- Carmichael, M.S.; Warburton, V.L.; Dixen, J.; Davidson, J.M. Relationships among Cardiovascular, Muscular, and Oxytocin Responses during Human Sexual Activity. Arch. Sex. Behav. 1994, 23, 59–79. [Google Scholar] [CrossRef]
- Yang, H.-P.; Wang, L.; Han, L.; Wang, S.C. Nonsocial Functions of Hypothalamic Oxytocin. ISRN Neurosci. 2013, 2013, 179272. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.E.; Kanyicska, B.; Lerant, A.; Nagy, G. Prolactin: Structure, Function, and Regulation of Secretion. Physiol. Rev. 2000, 80, 1523–1631. [Google Scholar] [CrossRef]
- Saleem, M.; Martin, H.; Coates, P. Prolactin Biology and Laboratory Measurement: An Update on Physiology and Current Analytical Issues. Clin. Biochem. Rev. 2018, 39, 3–16. [Google Scholar] [PubMed]
- Kruger, T.H.C.; Leeners, B.; Naegeli, E.; Schmidlin, S.; Schedlowski, M.; Hartmann, U.; Egli, M. Prolactin Secretory Rhythm in Women: Immediate and Long-Term Alterations after Sexual Contact. Hum. Reprod. 2012, 27, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Verhelst, J.; Abs, R. Hyperprolactinemia: Pathophysiology and Management. Treat. Endocrinol. 2003, 2, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Clinical Spectrum. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 4 June 2023).
- Wiegel, M.; Meston, C.; Rosen, R. The Female Sexual Function Index (FSFI): Cross-Validation and Development of Clinical Cutoff Scores. J. Sex Marital Ther. 2005, 31, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Meston, C.M.; Freihart, B.K.; Handy, A.B.; Kilimnik, C.D.; Rosen, R.C. Scoring and Interpretation of the FSFI: What Can Be Learned From 20 Years of Use? J. Sex. Med. 2020, 17, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.; Brown, J.; Heiman, S.; Leib, R. The Female Sexual Function Index (FSFI): A Multidimensional Self-Report Instrument for the Assessment of Female Sexual Function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, J.M.; Houman, J.; Caron, A.T.; Anger, J. Female Sexual Dysfunction: A Systematic Review of Outcomes Across Various Treatment Modalities. Sex. Med. Rev. 2019, 7, 223–250. [Google Scholar] [CrossRef]
- Romero Starke, K.; Petereit-Haack, G.; Schubert, M.; Kämpf, D.; Schliebner, A.; Hegewald, J.; Seidler, A. The Age-Related Risk of Severe Outcomes Due to COVID-19 Infection: A Rapid Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2020, 17, 5974. [Google Scholar] [CrossRef]
- Romero Starke, K.; Reissig, D.; Petereit-Haack, G.; Schmauder, S.; Nienhaus, A.; Seidler, A. The Isolated Effect of Age on the Risk of COVID-19 Severe Outcomes: A Systematic Review with Meta-Analysis. BMJ Glob. Health 2021, 6, e006434. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.H.; Tipih, T.; Makoah, N.A.; Vermeulen, J.-G.; Goedhals, D.; Sempa, J.B.; Burt, F.J.; Taylor, A.; Mahalingam, S. Comorbidities in SARS-CoV-2 Patients: A Systematic Review and Meta-Analysis. mBio 2021, 12, e03647-20. [Google Scholar] [CrossRef] [PubMed]
- Honardoost, M.; Janani, L.; Aghili, R.; Emami, Z.; Khamseh, M.E. The Association between Presence of Comorbidities and COVID-19 Severity: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2021, 50, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Silaghi-Dumitrescu, R.; Patrascu, I.; Lehene, M.; Bercea, I. Comorbidities of COVID-19 Patients. Med. Kaunas Lith. 2023, 59, 1393. [Google Scholar] [CrossRef] [PubMed]
- Marquini, G.V.; Martins, S.B.; Oliveira, L.M.; Dias, M.M.; Takano, C.C.; Sartori, M.G.F. Effects of the COVID-19 Pandemic on Gynecological Health: An Integrative Review. RBGO Gynecol. Obstet. 2022, 44, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Phelan, N.; Behan, L.A.; Owens, L. The Impact of the COVID-19 Pandemic on Women’s Reproductive Health. Front. Endocrinol. 2021, 12, 642755. [Google Scholar] [CrossRef] [PubMed]
- Sharp, G.C.; Fraser, A.; Sawyer, G.; Kountourides, G.; Easey, K.E.; Ford, G.; Olszewska, Z.; Howe, L.D.; Lawlor, D.A.; Alvergne, A.; et al. The COVID-19 Pandemic and the Menstrual Cycle: Research Gaps and Opportunities. Int. J. Epidemiol. 2021, 51, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Chen, G.; Hou, H.; Liao, Q.; Chen, J.; Bai, H.; Lee, S.; Wang, C.; Li, H.; Cheng, L.; et al. Analysis of Sex Hormones and Menstruation in COVID-19 Women of Child-Bearing Age. Reprod. Biomed. Online 2021, 42, 260–267. [Google Scholar] [CrossRef]
- Arcos-Romero, A.I.; Calvillo, C. Sexual Health and Psychological Well-Being of Women: A Systematic Review. Healthcare 2023, 11, 3025. [Google Scholar] [CrossRef]
- Rasmi, Y.; Jalali, L.; Khalid, S.; Shokati, A.; Tyagi, P.; Ozturk, A.; Nasimfar, A. The Effects of Prolactin on the Immune System, Its Relationship with the Severity of COVID-19, and Its Potential Immunomodulatory Therapeutic Effect. Cytokine 2023, 169, 156253. [Google Scholar] [CrossRef]
- Engel, S.; Klusmann, H.; Ditzen, B.; Knaevelsrud, C.; Schumacher, S. Menstrual Cycle-Related Fluctuations in Oxytocin Concentrations: A Systematic Review and Meta-Analysis. Front. Neuroendocrinol. 2019, 52, 144–155. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | Control | Mild or Moderate COVID-19 | Severe COVID-19 | |
|---|---|---|---|---|
| COVID-19 status | No history of COVID-19 patients | COVID-19 patients | ||
| NIH group [47] | n/a | 1. mild illness | 2. moderate illness | 3. severe illness |
| Criteria for assignment | No positive SARS-CoV-2 test or history of symptoms of SARS-CoV-2 infection, and no SARS-CoV-2 within 6 months | Any symptom of COVID-19 *, or abnormal chest imaging | Evidence of lower respiratory disease during clinical assessment or imaging, and SpO2 ≥ 94% | SpO2 < 94%; PaO2/FiO2 < 300 mm Hg; RR > 30 breaths/min, or LI > 50% |
| n | 40 | 33 | 31 | |
| Age (years) | 30 ± 8 | 34 ± 8 | 43 ± 7 | |
| At least one childbirth in anamnesis | 45.0% | 64.52% | 80.65% | |
| Average number of pregnancies | 0.66 | 1.39 | 1.97 | |
| FSFI | Second Visit | Third Visit | ||||
|---|---|---|---|---|---|---|
| Control (n = 40) | Mild or Moderate COVID-19 (n = 31) | Severe COVID-19 (n = 33) | Control (n = 40) | Mild or Moderate COVID-19 (n = 31) | Severe COVID-19 (n = 33) | |
| Total Sexual Function Score | 24.71 ± 9.01 | 25.91 ± 7.79 | 26.46 ± 4.81 | 27.23 ± 7.73 | 25.63 ± 7.35 | 26.98 ± 4.27 |
| Desire | 3.73 ± 1.45 | 3.82 ± 1.39 | 3.36 ± 0.99 | 4.07 ± 1.38 | 3.60 ± 1.31 | 3.44 ± 0.94 |
| Arousal | 4.03 ± 1.70 | 4.18 ± 1.46 | 4.26 ± 0.87 | 4.69 ± 1.35 | 4.08 ± 1.38 | 4.56 ± 1.19 |
| Lubrication | 4.40 ± 1.87 | 5.01 ± 1.54 | 5.12 ± 1.03 | 4.67 ± 1.87 | 4.88 ± 1.41 | 5.34 ± 0.84 |
| Orgasm | 4.42 ± 1.83 | 4.39 ± 1.59 | 4.56 ± 1.08 | 4.57 ± 1.45 | 4.18 ± 1.54 | 4.59 ± 0.96 |
| Satisfaction | 4.67 ± 1.77 | 4.77 ± 1.22 | 4.77 ± 0.71 | 5.14 ± 1.38 | 4.50 ± 1.34 | 4.88 ± 0.58 |
| Pain | 3.46 ± 2.20 | 4.10 ± 1.67 | 4.39 ± 1.57 | 4.08 ± 1.40 | 4.40 ± 1.49 | 4.17 ± 1.47 |
| Female Sexual dysfunction | 33.33% | 50.0% | 36.36% | 35.71% | 50.0% | 16.67% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żak, K.; Starek, E.; Korga-Plewko, A.; Rasoul-Pelińska, K.; Abramiuk, M.; Michalczuk, M.; Rajtak, A.; Kotarski, J.; Frankowska, K.; Bis, L.; et al. Assessment of the Impact of SARS-CoV-2 Infection on the Sexual Function of Women, Levels of Oxytocin and Prolactin: A Prospective Cohort Study. J. Clin. Med. 2024, 13, 2230. https://doi.org/10.3390/jcm13082230
Żak K, Starek E, Korga-Plewko A, Rasoul-Pelińska K, Abramiuk M, Michalczuk M, Rajtak A, Kotarski J, Frankowska K, Bis L, et al. Assessment of the Impact of SARS-CoV-2 Infection on the Sexual Function of Women, Levels of Oxytocin and Prolactin: A Prospective Cohort Study. Journal of Clinical Medicine. 2024; 13(8):2230. https://doi.org/10.3390/jcm13082230
Chicago/Turabian StyleŻak, Klaudia, Ernest Starek, Agnieszka Korga-Plewko, Karolina Rasoul-Pelińska, Monika Abramiuk, Mariola Michalczuk, Alicja Rajtak, Jan Kotarski, Karolina Frankowska, Liliana Bis, and et al. 2024. "Assessment of the Impact of SARS-CoV-2 Infection on the Sexual Function of Women, Levels of Oxytocin and Prolactin: A Prospective Cohort Study" Journal of Clinical Medicine 13, no. 8: 2230. https://doi.org/10.3390/jcm13082230