


Effectiveness of Manual Hysteroscopic Tissue Removal Device for Intrauterine Polyps in Infertile Women in Both Operating and Office Settings
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
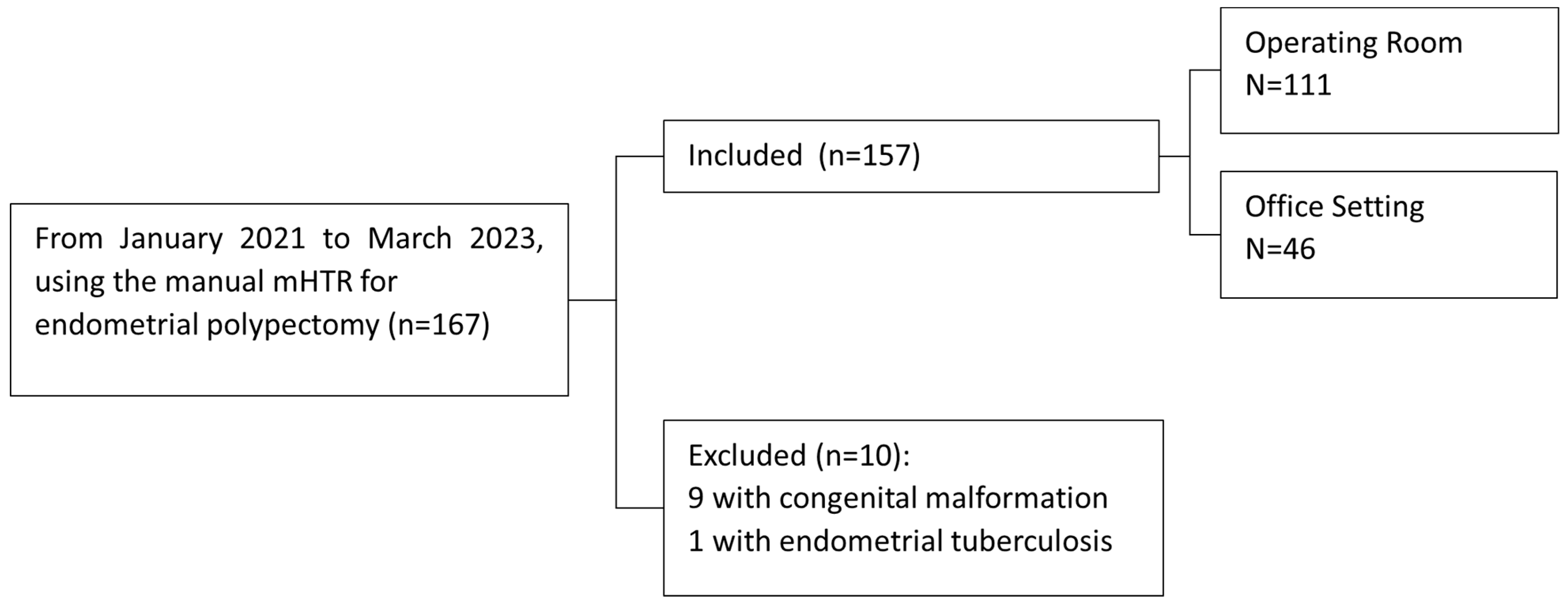
2.1. Study Population
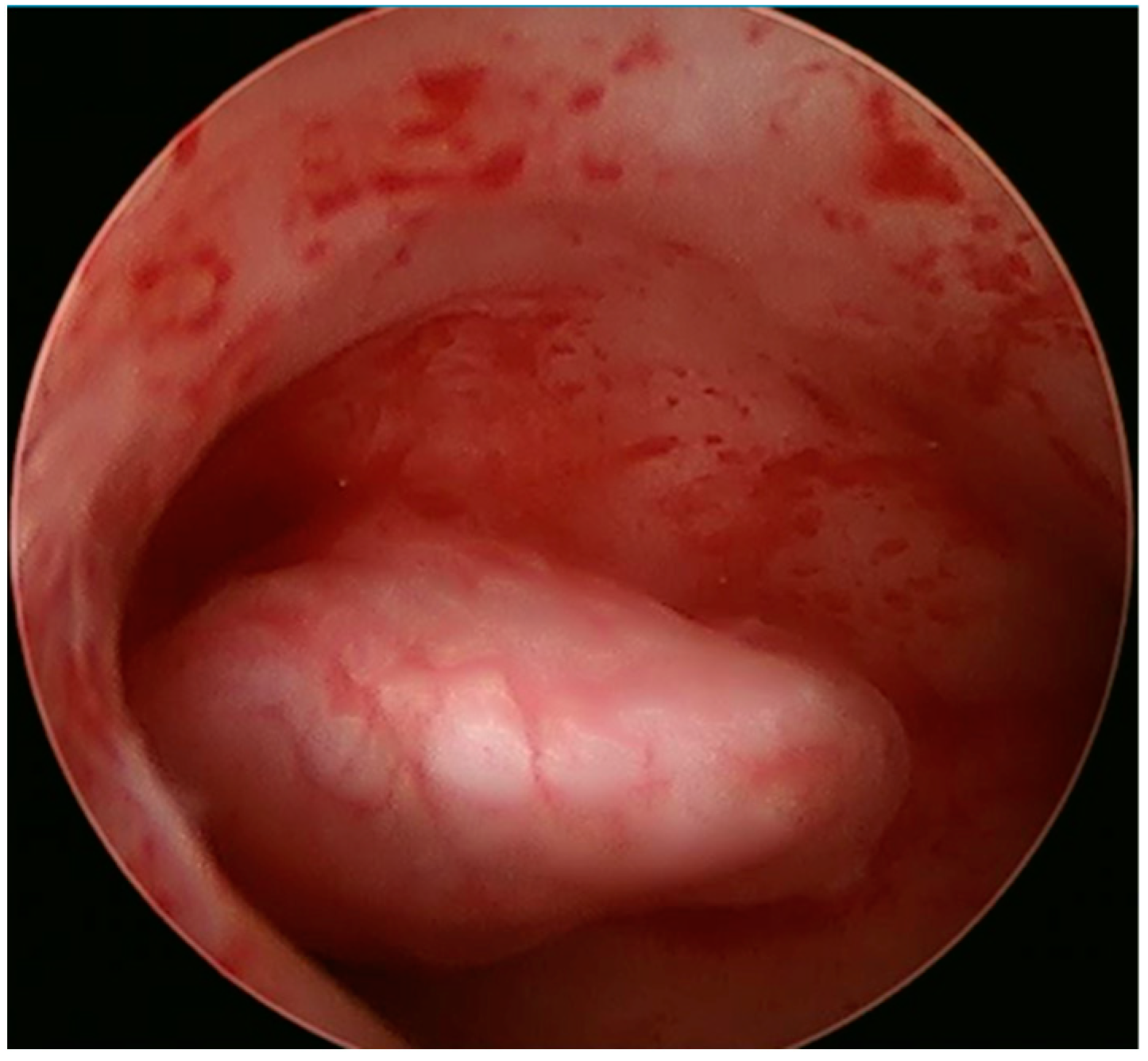
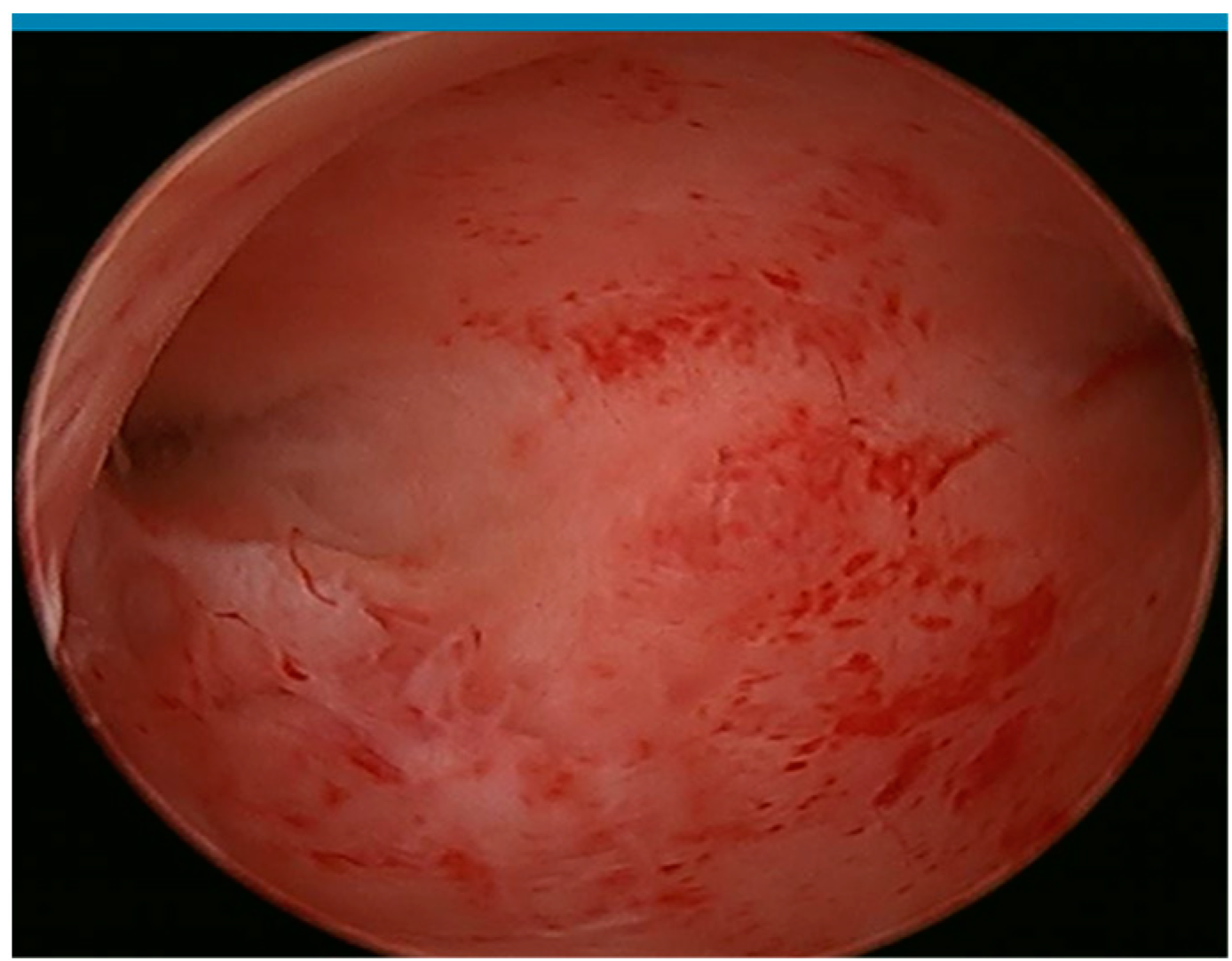
2.2. Surgical Procedure
2.3. Manual Hysteroscopic Tissue Removal System (mHTR)
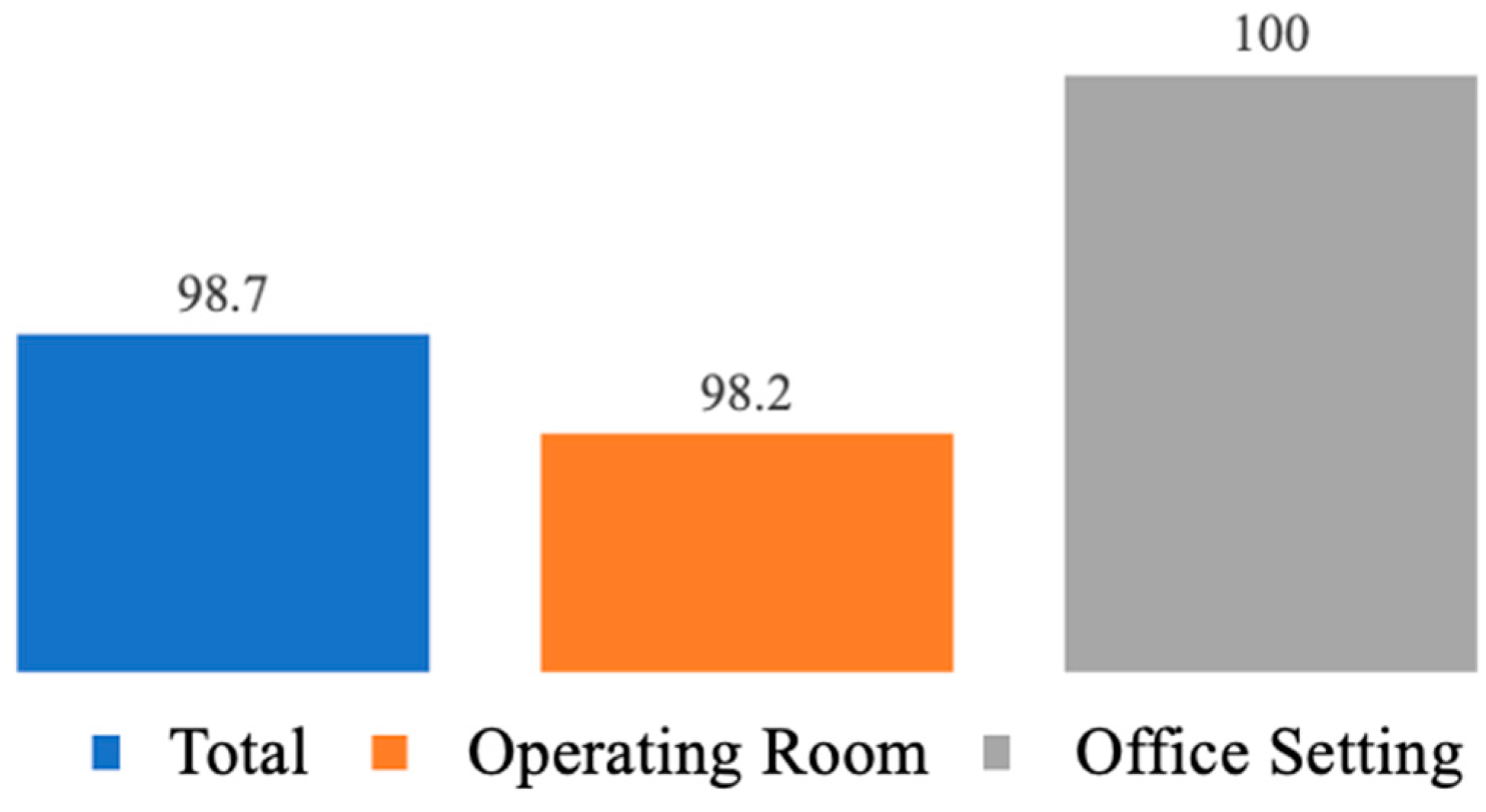
2.4. Outcome Measured
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vitale, S.G.; Haimovich, S.; Laganà, A.S.; Alonso, L.; Sardo, A.D.S.; Carugno, J. Endometrial Polyps. An evidence-based diagnosis and management guide. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 260, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Rackow, B.W.; Jorgensen, E.; Taylor, H.S. Endometrial polyps affect uterine receptivity. Fertil. Steril. 2011, 95, 2690–2692. [Google Scholar] [CrossRef]
- Shokeir, T.A.; Shalan, H.M.; El-Shafei, M.M. Significance of endometrial polyps detected hysteroscopically in eumenorrheic infertile women. J. Obstet. Gynaecol. Res. 2004, 30, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Hinckley, M.D.; Milki, A.A. 1000 office-based hysteroscopies prior to in vitro fertilization: Feasibility and findings. JSLS J. Soc. Laparoendosc. Surg. 2004, 8, 103. [Google Scholar]
- AAGL Advancing Minimally Invasive Gynecology Worldwide. AAGL practice report: Practice guidelines for the diagnosis and management of endometrial polyps. J. Minim. Invasive Gynecol. 2012, 19, 3–10. [Google Scholar] [CrossRef]
- Raz, N.; Feinmesser, L.; Moore, O.; Haimovich, S. Endometrial polyps: Diagnosis and treatment options—A review of literature. Minim. Invasive Ther. Allied Technol. 2021, 30, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Kavoussi, S.K.; Esqueda, A.S.; West, B.T.; Chen, S.H.; London, K.; Lebovic, D.I.; Barsky, M.; Kavoussi, M.M.; Gilkey, M.S.; Chen, J.; et al. The Use of Hysteroscopy for the Diagnosis and Treatment of Intrauterine Pathology: ACOG Committee Opinion, Number 800. Obstet. Gynecol. 2020, 135, e138–e148. [Google Scholar]
- Emanuel, M.H.; Wamsteker, K. The Intra Uterine Morcellator: A new hysteroscopic operating technique to remove intrauterine polyps and myomas. J. Minim. Invasive Gynecol. 2005, 12, 62–66. [Google Scholar] [PubMed]
- Franchini, M.; Ceci, O.; Casadio, P.; Carugno, J.; Giarrè, G.; Gubbini, G.; Catena, U.; de Angelis, M.C.; Sardo, A.D.S. Mechanical hysteroscopic tissue removal or hysteroscopic morcellator: Understanding the past to predict the future. A narrative review. Facts Views Vis. ObGyn 2021, 13, 193. [Google Scholar] [CrossRef] [PubMed]
- Rubino, R.J.; Lukes, A.S. Twelve-month outcomes for patients undergoing hysteroscopic morcellation of uterine polyps and myomas in an office or ambulatory surgical center. J. Minim. Invasive Gynecol. 2015, 22, 285–290. [Google Scholar] [CrossRef]
- Ceci, O.; Franchini, M.; Cardinale, S.; Cannone, R.; Giarrè, G.; Fascilla, F.D.; Bettocchi, S.; Cicinelli, E. Comparison of endometrial polyp recurrence in fertile women after office hysteroscopic endometrial polypectomy using two widely spread techniques. J. Obstet. Gynaecol. Res. 2020, 46, 2084–2091. [Google Scholar] [CrossRef]
- Kavoussi, S.K.; Esqueda, A.S.; West, B.T.; Chen, S.-H.; London, K.; Lebovic, D.I.; Barsky, M.; Kavoussi, M.M.; Gilkey, M.S.; Chen, J.; et al. The effects of hysteroscopic morcellation of endometrial polyps on frozen embryo transfer outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 267, 241–244. [Google Scholar] [CrossRef]
- Yong, J.; Wan, Y.; Ye, M.; Yi, S.; Zeng, F.; Sun, X.; Song, J.; Wang, X.; Zeng, X.; Xiao, S. Comparative analysis of the clinical efficacy and reproductive outcomes of the hysteroscopic tissue removal system (MyoSure) and hysteroscopic electroresection in the treatment of benign intrauterine lesions. Int. J. Gynecol. Obstet. 2023, 163, 115–122. [Google Scholar] [CrossRef]
- Lee, M.M.H. Endometrial Polyp Removed by a Manual Hysteroscopic Tissue Removal Device. Gynecol. Minim. Invasive Ther. 2020, 9, 34–35. [Google Scholar] [CrossRef]
- Groll, J.M. Effectiveness of a New, Lower-Cost Manual Hysteroscopic Tissue Removal Device (Polygon) in an Office Setting. Fertil. Steril. 2020, 114, e479. [Google Scholar] [CrossRef]
- van Wessel, S.; Hamerlynck, T.; van Vliet, H.; Schoot, B.; Weyers, S. Manual morcellation (Resectr™ 9Fr) vs electromechanical morcellation (TruClear™) for hysteroscopic polypectomy: A randomized controlled non-inferiority trial. Acta Obstet. Gynecol. Scand. 2023, 102, 209–217. [Google Scholar] [CrossRef]
- Smith, P.P.; Middleton, L.J.; Connor, M.; Clark, T.J. Hysteroscopic morcellation compared with electrical resection of endometrial polyps: A randomized controlled trial. Obstet. Gynecol. 2014, 123, 745–751. [Google Scholar] [CrossRef]
- Rosenblatt, P.; Barcia, S.; DiSciullo, A.; Warda, H. Improved adequacy of endometrial tissue sampled from postmenopausal women using the MyoSure Lite hysteroscopic tissue removal system versus conventional curettage. Int. J. Womens Health 2017, 9, 789–794. [Google Scholar] [CrossRef]
- Haber, K.; Hawkins, E.; Levie, M.; Chudnoff, S. Hysteroscopic morcellation: Review of the manufacturer and user facility device experience (MAUDE) database. J. Minim. Invasive Gynecol. 2015, 22, 110–114. [Google Scholar] [CrossRef]
- Noventa, M.; Ancona, E.; Quaranta, M.; Vitagliano, A.; Cosmi, E.; D’antona, D.; Gizzo, S. Intrauterine Morcellator Devices: The Icon of Hysteroscopic Future or Merely a Marketing Image? A Systematic Review Regarding Safety, Efficacy, Advantages, and Contraindications. Reprod. Sci. 2015, 22, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Cheng, J.; Ansari, S.H.; Campo, R.; Di, W.; Li, W.; Bigatti, G. Hysteroscopic tissue removal systems for the treatment of intrauterine pathology: A systematic review and meta-analysis. Facts Views Vis. Obgyn 2018, 10, 207–213. [Google Scholar]
- Guo, T.; Zhou, H.; Yang, J.; Wu, P.; Liu, P.; Liu, Z.; Li, Z. Identifying the superior surgical procedure for endometrial polypectomy: A network meta-analysis. Int. J. Surg. 2019, 62, 28–33. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 157) | Operating Room (n = 111) | Office Setting (n = 46) | p-Value |
|---|---|---|---|---|
| Age (yrs) | 32.9± 5.5 | 33.1 ± 4.1 | 31.4 ± 5.9 | 0.24 |
| Gravidity | 0.9 ± 1.2 | 0.95 ± 1.24 | 1.0 ± 1.3 | 0.92 |
| Parity | 0.3 ± 1.2 | 0.3 ± 0.5 | 1.0 ± 1.3 | 0.91 |
| BMI (kg/m2) Primary infertility Secondary infertility Total number of polyps | 23.0 ± 3.877 (49%) 80 (51%) 6.3 ± 3.0 | 22.1 ± 3 54 (48.6%) 57 (51.4%) 6.73 ± 2.7 | 23.9 ± 4.5 23 (50%) 23 (50%) 1.6 ± 1.2 | <0.01 <0.01 0.88 <0.001 |
| Characteristic | Overall (n = 157) | Operating Room (n = 111) | Office (n = 46) | p-Value |
|---|---|---|---|---|
| Anesthesia | <0.001 | |||
| MAC | 111 | 100% (111) | 0 | |
| Paracervical | 5 | 0 | 10.8% (5) | |
| None | 41 | 0 | 89.2% (41) | |
| Number of polyps | <0.001 | |||
| 1 | 21.7% (34) | 4.5% (5) | 63% (29) | |
| 2 | 9.6% (15) | 1.8% (2) | 28.2% (13) | |
| 3 | 5.1% (8) | 7.2% (8) | 0% (0) | |
| 4 | 5.1% (8) | 7.2% (8) | 0% (0) | |
| 5 or more | 58.9% (92) | 79.3% (88) | 8.7% (4) | |
| Cervical dilation | 111 (70.7%) | 111 (100%) | 0 (0%) | <0.001 |
| Blood loss (cc) | 2.6 ± 2.3 (0–10) | 2.9 ± 2.3 (1.00–10.00) | 0 | <0.001 |
| Total time for procedure (min) | 26 ± 7.6 (5–60) | 27.1 ± 6.4 | 7.3 ± 1.8 | <0.001 |
| Complications | 0 (0%) | 0 (0%) | 0 (0%) | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Chen, H.; Morgan, I.; Prytkova, V.; Kohl-Thomas, B.; Parry, J.P.; Lindheim, S.R. Effectiveness of Manual Hysteroscopic Tissue Removal Device for Intrauterine Polyps in Infertile Women in Both Operating and Office Settings. J. Clin. Med. 2024, 13, 2244. https://doi.org/10.3390/jcm13082244
Wang C, Chen H, Morgan I, Prytkova V, Kohl-Thomas B, Parry JP, Lindheim SR. Effectiveness of Manual Hysteroscopic Tissue Removal Device for Intrauterine Polyps in Infertile Women in Both Operating and Office Settings. Journal of Clinical Medicine. 2024; 13(8):2244. https://doi.org/10.3390/jcm13082244
Chicago/Turabian StyleWang, Chen, Hui Chen, India Morgan, Valeriya Prytkova, Belinda Kohl-Thomas, J. Preston Parry, and Steven R. Lindheim. 2024. "Effectiveness of Manual Hysteroscopic Tissue Removal Device for Intrauterine Polyps in Infertile Women in Both Operating and Office Settings" Journal of Clinical Medicine 13, no. 8: 2244. https://doi.org/10.3390/jcm13082244
APA StyleWang, C., Chen, H., Morgan, I., Prytkova, V., Kohl-Thomas, B., Parry, J. P., & Lindheim, S. R. (2024). Effectiveness of Manual Hysteroscopic Tissue Removal Device for Intrauterine Polyps in Infertile Women in Both Operating and Office Settings. Journal of Clinical Medicine, 13(8), 2244. https://doi.org/10.3390/jcm13082244