
Exploring the Associations of Inflammatory and Oxidative Stress Biomarkers with Pancreatic Diseases: An Observational and Mendelian Randomisation Study

 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
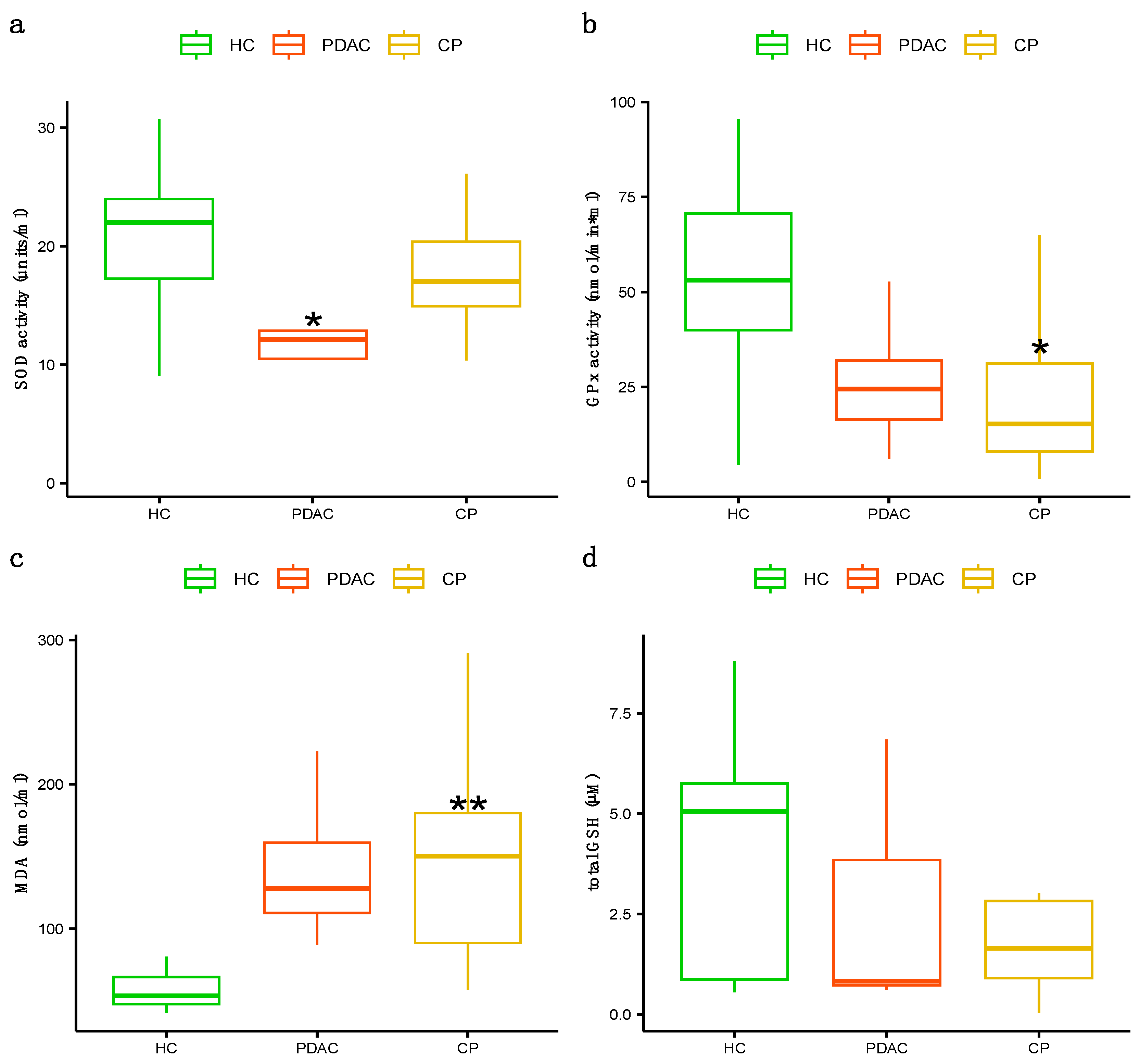
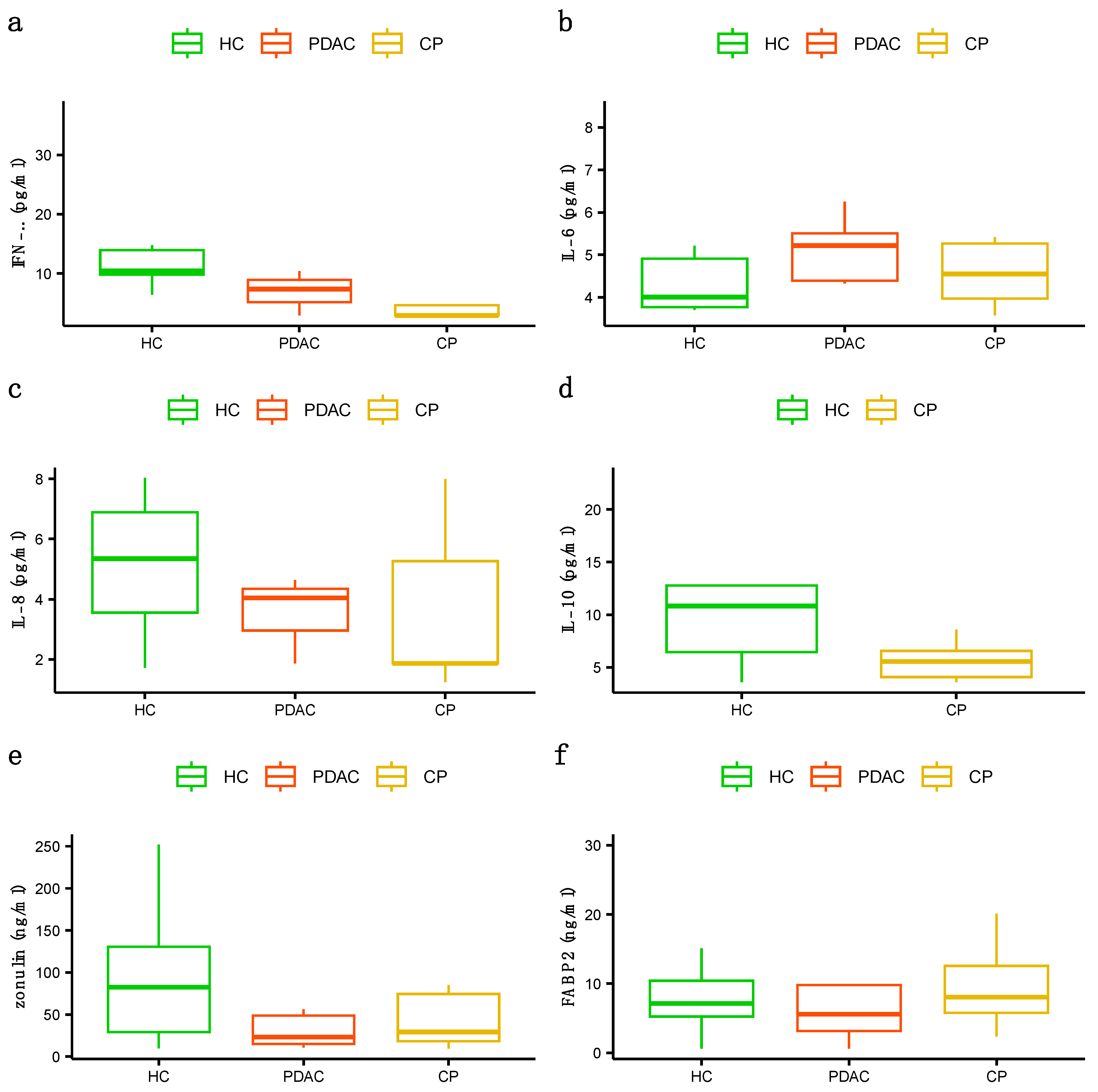
3.2. Association Analysis of Serological Biomarkers
3.3. Mendelian Randomisation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Ammer-Herrmenau, C.; Pfisterer, N.; Weingarten, M.F.; Neesse, A. The microbiome in pancreatic diseases: Recent advances and future perspectives. United Eur. Gastroenterol. J. 2020, 8, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Baine, M.J.; Jain, M.; Sasson, A.R.; Batra, S.K. Early diagnosis of pancreatic cancer: Challenges and new developments. Biomark. Med. 2012, 6, 597–612. [Google Scholar] [CrossRef] [PubMed]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.W.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013, 62, 339–347, Erratum in Gut 2014, 63, 178. [Google Scholar] [CrossRef] [PubMed]
- Muniraj, T.; Aslanian, H.R.; Farrell, J.; Jamidar, P.A. Chronic pancreatitis, a comprehensive review and update. Part I: Epidemiology, etiology, risk factors, genetics, pathophysiology, and clinical features. Dis. Mon. 2014, 60, 530–550. [Google Scholar] [CrossRef] [PubMed]
- Etemad, B.; Whitcomb, D.C. Chronic pancreatitis: Diagnosis, classification, and new genetic developments. Gastroenterology 2001, 120, 682–707. [Google Scholar] [CrossRef] [PubMed]
- Kirkegård, J.; Mortensen, F.V.; Cronin-Fenton, D. Chronic Pancreatitis and Pancreatic Cancer Risk: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2017, 112, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Lowenfels, A.B.; Maisonneuve, P.; DiMagno, E.P.; Elitsur, Y.; Gates, L.K., Jr.; Perrault, J.; Whitcomb, D.C. Hereditary pancreatitis and the risk of pancreatic cancer. International Hereditary Pancreatitis Study Group. J. Natl. Cancer Inst. 1997, 89, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Duell, E.J.; Lucenteforte, E.; Olson, S.H.; Bracci, P.M.; Li, D.; Risch, H.A.; Silverman, D.T.; Ji, B.T.; Gallinger, S.; Holly, E.A.; et al. Pancreatitis and pancreatic cancer risk: A pooled analysis in the International Pancreatic Cancer Case-Control Consortium (PanC4). Ann. Oncol. 2012, 23, 2964–2970. [Google Scholar] [CrossRef]
- Yu, J.; Ploner, A.; Kordes, M.; Löhr, M.; Nilsson, M.; de Maturana, M.E.L.; Estudillo, L.; Renz, H.; Carrato, A.; Molero, X.; et al. Plasma protein biomarkers for early detection of pancreatic ductal adenocarcinoma. Int. J. Cancer 2021, 148, 2048–2058. [Google Scholar] [CrossRef]
- Chan, A.; Diamandis, E.P.; Blasutig, I.M. Strategies for discovering novel pancreatic cancer biomarkers. J. Proteom. 2013, 81, 126–134. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, R.S.; Stoita, A. Biomarkers in the diagnosis of pancreatic cancer: Are we closer to finding the golden ticket? World J. Gastroenterol. 2021, 27, 4045–4087. [Google Scholar] [CrossRef]
- Yako, Y.Y.; Kruger, D.; Smith, M.; Brand, M. Cytokines as Biomarkers of Pancreatic Ductal Adenocarcinoma: A Systematic Review. PLoS ONE 2016, 11, e0154016. [Google Scholar] [CrossRef] [PubMed]
- Habtezion, A. Inflammation in acute and chronic pancreatitis. Curr. Opin. Gastroenterol. 2015, 31, 395–399. [Google Scholar] [CrossRef]
- Kodydkova, J.; Vavrova, L.; Stankova, B.; Macasek, J.; Krechler, T.; Zak, A. Antioxidant status and oxidative stress markers in pancreatic cancer and chronic pancreatitis. Pancreas 2013, 42, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Useros, J.; Li, W.; Cabeza-Morales, M.; Garcia-Foncillas, J. Oxidative Stress: A New Target for Pancreatic Cancer Prognosis and Treatment. J. Clin. Med. 2017, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, C.; Fasano, A. Zonulin, a regulator of epithelial and endothelial barrier functions, and its involvement in chronic inflammatory diseases. Tissue Barriers 2016, 4, e1251384. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.M.; Brummer, R.J.; Derrien, M.; MacDonald, T.T.; Troost, F.; Cani, P.D.; Theodorou, V.; Dekker, J.; Méheust, A.; de Vos, W.M.; et al. Homeostasis of the gut barrier and potential biomarkers. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G171–G193. [Google Scholar] [CrossRef]
- Seethaler, B.; Basrai, M.; Neyrinck, A.M.; Nazare, J.-A.; Walter, J.; Delzenne, N.M.; Bischoff, S.C. Biomarkers for assessment of intestinal permeability in clinical practice. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 321, G11–G17. [Google Scholar] [CrossRef]
- Smith, G.D.; Hemani, G. Mendelian randomization: Genetic anchors for causal inference in epidemiological studies. Hum. Mol. Genet. 2014, 23, R89–R98. [Google Scholar] [CrossRef]
- Schreiber-Gregory, D.N. Ridge Regression and multicollinearity: An in-depth review. Model Assist. Stat. Appl. 2018, 13, 359–365. [Google Scholar] [CrossRef]
- Cule, E.; De Iorio, M. Ridge regression in prediction problems: Automatic choice of the ridge parameter. Genet. Epidemiol. 2013, 37, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.; Newman, T.B. Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Appendix 6A; p. 73. [Google Scholar]
- Chow, S.-C.; Shao, J.; Wang, H. Sample Size Calculations in Clinical Research, 2nd ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2008; p. 58. [Google Scholar]
- Lawlor, D.A. Commentary: Two-sample Mendelian randomization: Opportunities and challenges. Int. J. Epidemiol. 2016, 45, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, Ł.; Kepinska, M.; Milnerowicz, H. Alterations in Concentration/Activity of Superoxide Dismutases in Context of Obesity and Selected Single Nucleotide Polymorphisms in Genes: SOD1, SOD2, SOD3. Int. J. Mol. Sci. 2020, 21, 5069. [Google Scholar] [CrossRef] [PubMed]
- Ravn-Haren, G.; Olsen, A.; Tjønneland, A.; Dragsted, L.O.; Nexø, B.A.; Wallin, H.; Overvad, K.; Raaschou-Nielsen, O.; Vogel, U. Associations between GPX1 Pro198Leu polymorphism, erythrocyte GPX activity, alcohol consumption and breast cancer risk in a prospective cohort study. Carcinogenesis 2006, 27, 820–825. [Google Scholar] [CrossRef]
- Rhee, E.P.; Surapaneni, A.; Zheng, Z.; Zhou, L.; Dutta, D.; Arking, D.E.; Zhang, J.; Duong, T.; Chatterjee, N.; Luo, S.; et al. Trans-ethnic genome-wide association study of blood metabolites in the Chronic Renal Insufficiency Cohort (CRIC) study. Kidney Int. 2022, 101, 814–823. [Google Scholar] [CrossRef]
- Zhu, Z.; Zhang, F.; Hu, H.; Bakshi, A.; Robinson, M.R.; Powell, J.E.; Montgomery, G.W.; Goddard, M.E.; Wray, N.R.; Visscher, P.M.; et al. Integration of summary data from GWAS and eQTL studies predicts complex trait gene targets. Nat. Genet. 2016, 48, 481–487. [Google Scholar] [CrossRef]
- Burgess, S.; Thompson, S.G.; CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int. J. Epidemiol. 2011, 40, 755–764. [Google Scholar] [CrossRef]
- Burgess, S.; Davies, N.M.; Thompson, S.G. Bias due to participant overlap in two-sample Mendelian randomization. Genet. Epidemiol. 2016, 40, 597–608. [Google Scholar] [CrossRef]
- Jiang, L.; Zheng, Z.; Fang, H.; Yang, J. A generalized linear mixed model association tool for biobank-scale data. Nat. Genet. 2021, 53, 1616–1621. [Google Scholar] [CrossRef]
- Kurki, M.I.; Karjalainen, J.; Palta, P.; Sipilä, T.P.; Kristiansson, K.; Donner, K.M.; Reeve, M.P.; Laivuori, H.; Aavikko, M.; Kaunisto, M.A.; et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature 2023, 613, 508–518, Erratum in Nature 2023, 615, E19. [Google Scholar] [CrossRef]
- Burgess, S.; Butterworth, A.; Thompson, S.G. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet. Epidemiol. 2013, 37, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Faßhauer, M.; Stumvoll, M.; et al. Inflammatory cytokines in general and central obesity and modulating effects of physical activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef]
- Charles, B.A.; Doumatey, A.; Huang, H.; Zhou, J.; Chen, G.; Shriner, D.; Adeyemo, A.; Rotimi, C.N. The roles of IL-6, IL-10, and IL-1RA in obesity and insulin resistance in African-Americans. J. Clin. Endocrinol. Metab. 2011, 96, E2018–E2022. [Google Scholar] [CrossRef] [PubMed]
- Skalicky, J.; Muzakova, V.; Kandar, R.; Meloun, M.; Rousar, T.; Palicka, V. Evaluation of oxidative stress and inflammation in obese adults with metabolic syndrome. Clin. Chem. Lab. Med. 2008, 46, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging. 2018, 13, 757–772. [Google Scholar] [CrossRef]
- Rizvi, S.I.; Maurya, P.K. Markers of oxidative stress in erythrocytes during aging in humans. Ann. N. Y. Acad. Sci. 2007, 1100, 373–382. [Google Scholar] [CrossRef]
- Tower, J.; Pomatto, L.C.D.; Davies, K.J.A. Sex differences in the response to oxidative and proteolytic stress. Redox Biol. 2020, 31, 101488. [Google Scholar] [CrossRef]
- Cullen, J.J.; Mitros, F.A.; Oberley, L.W. Expression of antioxidant enzymes in diseases of the human pancreas: Another link between chronic pancreatitis and pancreatic cancer. Pancreas 2003, 26, 23–27. [Google Scholar] [CrossRef]
- Dhar, S.K.; St Clair, D.K. Manganese superoxide dismutase regulation and cancer. Free Radic. Biol. Med. 2012, 52, 2209–2222. [Google Scholar] [CrossRef] [PubMed]
- Grigsby, B.; Rodriguez-Rilo, H.; Khan, K. Antioxidants and chronic pancreatitis: Theory of oxidative stress and trials of antioxidant therapy. Dig. Dis. Sci. 2012, 57, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Robles, L.; Vaziri, N.D.; Ichii, H. Role of Oxidative Stress in the Pathogenesis of Pancreatitis: Effect of Antioxidant Therapy. Pancreat. Disord. Ther. 2013, 3, 112. [Google Scholar] [CrossRef] [PubMed]
- Quilliot, D.; Walters, E.; Bonte, J.P.; Fruchart, J.-C.; Duriez, P.; Ziegler, O. Diabetes mellitus worsens antioxidant status in patients with chronic pancreatitis. Am. J. Clin. Nutr. 2005, 81, 1117–1125. [Google Scholar] [CrossRef]
- Girish, B.N.; Rajesh, G.; Vaidyanathan, K.; Balakrishnan, V. Assessment of oxidative status in chronic pancreatitis and its relation with zinc status. Indian J. Gastroenterol. 2011, 30, 84–88. [Google Scholar] [CrossRef]
- Zhou, D.; Shao, L.; Spitz, D.R. Reactive oxygen species in normal and tumor stem cells. Adv. Cancer Res. 2014, 122, 1–67. [Google Scholar]



{kind=link}
{kind=link}
| HCs (n = 23) | PDAC (n = 12) | CP (n = 21) | p-Value | |
|---|---|---|---|---|
| Sex, % (F/M) | 52.2/47.8 | 66.7/33.3 | 14.3/85.7 | 0.004 ** |
| Age, yrs | 62.52 ± 10.89 | 69.17 ± 9.51 | 57.71 ± 7.05 | 0.005 ** |
| Tobacco consumption, % (Current/Former/Never) | 8.7/30.4/60.9 | 16.7/41.7/41.6 | 47.6/33.3/19.1 | 0.0005 ** |
| Alcohol consumption, % (High/Moderate/Low) | 8.7/4.3/87.0 | 16.7/8.3/75.0 | 0.0/80.9/19.1 | 0.0005 ** |
| BMI, kg/m2 | 26.59 ± 4.80 | 26.25 ± 6.60 | 24.96 ± 5.16 | 0.64 |
| Diabetes, % (yes/no) | 8.7/91.3 | 33.3/66.7 | 61.9/38.1 | 0.002 ** |
| Insulin treatment, % (yes/no) | 50/50 | 100/0 | 69.2/30.8 | 0.77 |
| Familiar pancreatic disease, % (yes/no) | 4.3/95.67 | 20/80 | 10.5/89.5 | 0.34 |
| PPI treatment, % (yes/no) | 21.7/78.3 | 33.3/66.7 | 57.1/42.9 | 0.05 |
| Previous digestive surgery, % (yes/no) | 26.1/73.9 | 25/75 | 14.3/85.7 | 0.63 |
| PDAC | CP | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| FABP2 (ng/mL) | 15.87 | [0.12, 2029.81] | 0.26 | 1.93 | [0.61, 6.05] | 0.26 |
| Zonulin (ng/mL) | 0.17 | [0.01, 5.31] | 0.31 | 0.61 | [0.20, 1.81] | 0.37 |
| total GSH | 0.46 | [0.07, 3.04] | 0.42 | 0.40 | [0.13, 1.26] | 0.12 |
| GPx (nmol/min × mL) | 0.33 | [0.07, 1.65] | 0.18 | 0.28 | [0.10, 0.79] | 0.02 * |
| SOD (units/mL) | 0.03 | [0.0007, 1.53] | 0.08 | 0.21 | [0.05, 0.89] | 0.03 * |
| MDA (nmol/mL) | 12.88 | [0.46, 353.57] | 0.13 | 2.05 | [1.36, 3.08] | 0.0005 ** |
| IFN-γ (pg/mL) | 0.02 | [0.00002, 11.73] | 0.22 | 0.26 | [0.05, 1.40] | 0.12 |
| IL-6 (pg/mL) | 1.03 | [0.53, 2.02] | 0.92 | 0.83 | [0.16, 4.25] | 0.82 |
| IL-8 (pg/mL) | 0.41 | [0.06, 2.50] | 0.33 | 0.45 | [0.13, 1.59] | 0.22 |
| IL-10 (pg/mL) | - | - | - | 0.002 | [0.000004, 1.49] | 0.06 |
| Proxied Biomarker | Genetic Study | Study N | SNP rs | Gene | R2 | F-Statistic |
|---|---|---|---|---|---|---|
| SOD activity | Lewandowski Ł et al., 2020 [26] | 50 | rs4880 (Val16Ala) | SOD2 | 0.20 | 20.9 |
| GPX activity | Ravn-Haren G et al., 2006 [27] | 377 | rs1050450 (Pro200Leu) | GPX1 | 0.02 | 6.8 |
| MDA levels | Rhee EP et al., 2022 [28] | 822 | rs33965115/ rs80018995/rs59408048 | CDH1/ ALPK2/SMIM21 | - | - |
| Proxied- Biomarker | Outcome | GWAS Cohort | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| SOD activity | PDAC | FinnGen | 0.97 | [0.82, 1.15] | 0.71 |
| UK Biobank | 1.17 | [0.98, 1.40] | 0.09 | ||
| CP | FinnGen | 0.98 | [0.91, 1.06] | 0.70 | |
| UK Biobank | 1.18 | [0.92, 1.53] | 0.17 | ||
| GPX activity | PDAC | FinnGen | 1.26 | [0.76, 2.09] | 0.36 |
| UK Biobank | 1.57 | [0.87, 2.82] | 0.13 | ||
| CP | FinnGen | 1.07 | [0.85, 1.36] | 0.54 | |
| UK Biobank | 0.89 | [0.40, 1.98] | 0.77 | ||
| MDA levels | PDAC | FinnGen | 1.01 | [0.64, 1.58] | 0.97 |
| UK Biobank | 1.48 | [0.87, 2.51] | 0.15 | ||
| CP | FinnGen | 0.92 | [0.76, 1.12] | 0.45 | |
| UK Biobank | 0.59 | [0.29, 1.23] | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilà-Quintana, L.; Fort, E.; Pardo, L.; Albiol-Quer, M.T.; Ortiz, M.R.; Capdevila, M.; Feliu, A.; Bahí, A.; Llirós, M.; Aguilar, E.; et al. Exploring the Associations of Inflammatory and Oxidative Stress Biomarkers with Pancreatic Diseases: An Observational and Mendelian Randomisation Study. J. Clin. Med. 2024, 13, 2247. https://doi.org/10.3390/jcm13082247
Vilà-Quintana L, Fort E, Pardo L, Albiol-Quer MT, Ortiz MR, Capdevila M, Feliu A, Bahí A, Llirós M, Aguilar E, et al. Exploring the Associations of Inflammatory and Oxidative Stress Biomarkers with Pancreatic Diseases: An Observational and Mendelian Randomisation Study. Journal of Clinical Medicine. 2024; 13(8):2247. https://doi.org/10.3390/jcm13082247
Chicago/Turabian StyleVilà-Quintana, Laura, Esther Fort, Laura Pardo, Maria T. Albiol-Quer, Maria Rosa Ortiz, Montserrat Capdevila, Anna Feliu, Anna Bahí, Marc Llirós, Esther Aguilar, and et al. 2024. "Exploring the Associations of Inflammatory and Oxidative Stress Biomarkers with Pancreatic Diseases: An Observational and Mendelian Randomisation Study" Journal of Clinical Medicine 13, no. 8: 2247. https://doi.org/10.3390/jcm13082247