
Effect of Daytime versus Nighttime on Prehospital Care and Outcomes after Severe Traumatic Brain Injury

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
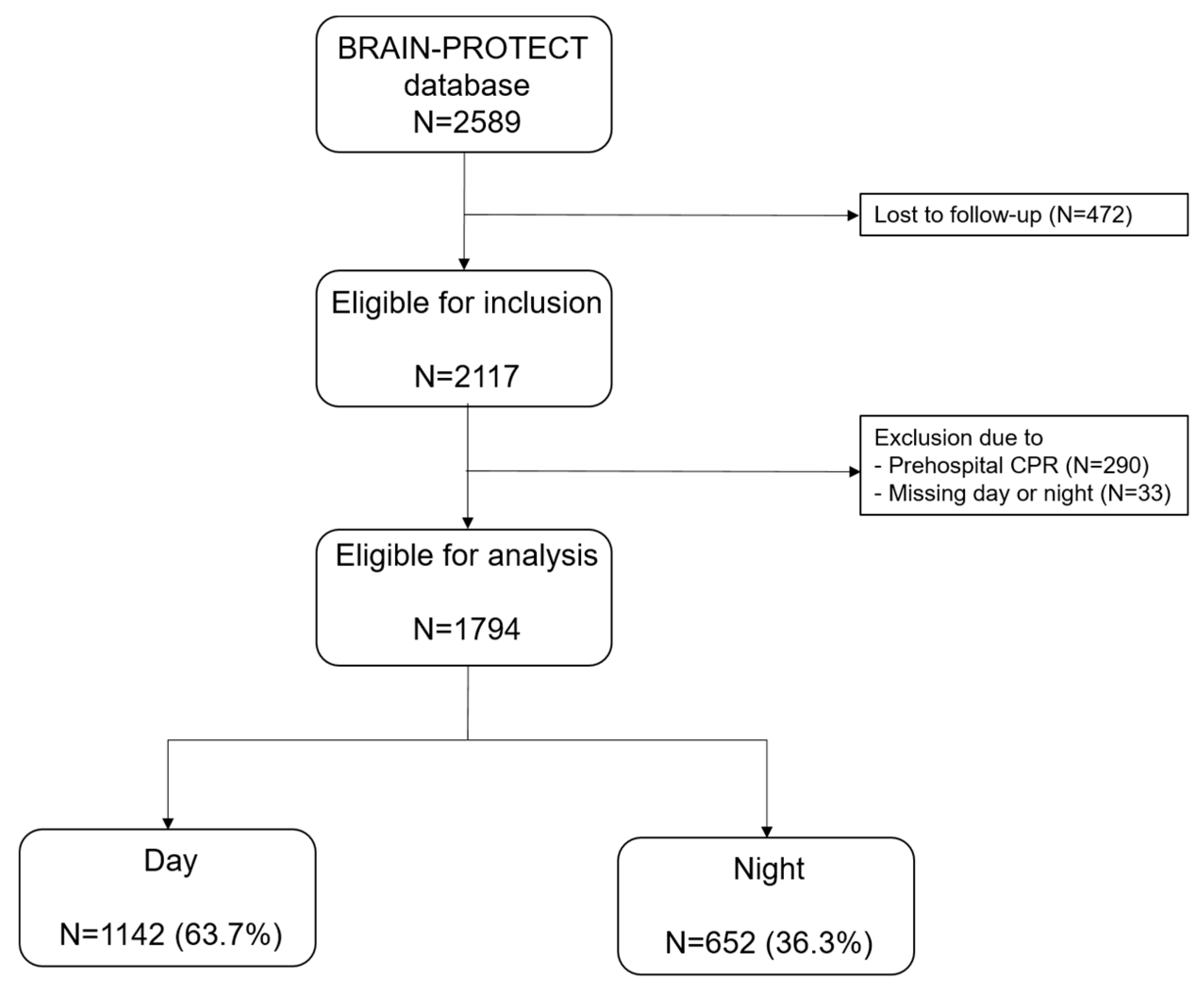
2.1. Patient Selection
2.2. Outcome Measures
2.3. Day- and Nighttime
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Vos, T.; Nichols, E.; Owolabi, M.O.; Carroll, W.M.; Dichgans, M.; Deuschl, G.; Parmar, P.; Brainin, M.; Murray, C. The global burden of neurological disorders: Translating evidence into policy. Lancet Neurol. 2020, 19, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Bossers, S.M.; Boer, C.; Bloemers, F.W.; Van Lieshout, E.M.M.; Den Hartog, D.; Hoogerwerf, N.; Innemee, G.; van der Naalt, J.; Absalom, A.R.; Peerdeman, S.M.; et al. Epidemiology, Prehospital Characteristics and Outcomes of Severe Traumatic Brain Injury in The Netherlands: The BRAIN-PROTECT Study. Prehospital Emerg. Care 2021, 25, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Wiles, M.D.; Braganza, M.; Edwards, H.; Krause, E.; Jackson, J.; Tait, F. Management of traumatic brain injury in the non-neurosurgical intensive care unit: A narrative review of current evidence. Anaesthesia 2023, 78, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Gravesteijn, B.Y.; Sewalt, C.A.; Stocchetti, N.; Citerio, G.; Ercole, A.; Lingsma, H.F.; von Steinbuchel, N.; Steyerberg, E.W.; Wilson, L.; Maas, A.I.R.; et al. Prehospital Management of Traumatic Brain Injury across Europe: A CENTER-TBI Study. Prehospital Emerg. Care 2021, 25, 629–643. [Google Scholar] [CrossRef] [PubMed]
- Franschman, G.; Verburg, N.; Brens-Heldens, V.; Andriessen, T.M.; Van der Naalt, J.; Peerdeman, S.M.; Valk, J.P.; Hoogerwerf, N.; Greuters, S.; Schober, P.; et al. Effects of physician-based emergency medical service dispatch in severe traumatic brain injury on prehospital run time. Injury 2012, 43, 1838–1842. [Google Scholar] [CrossRef] [PubMed]
- Olson, E.J.; Drage, L.A.; Auger, R.R. Sleep deprivation, physician performance, and patient safety. Chest 2009, 136, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Shin, S.D.; Sun, J.T.; Jamaluddin, S.F.; Tanaka, H.; Song, K.J.; Kajino, K.; Kimura, A.; Huang, E.P.; Hsieh, M.J.; et al. Association between prehospital time and outcome of trauma patients in 4 Asian countries: A cross-national, multicenter cohort study. PLoS Med. 2020, 17, e1003360. [Google Scholar] [CrossRef] [PubMed]
- Mauritz, W.; Brazinova, A.; Majdan, M.; Rehorcikova, V.; Leitgeb, J. Effects of time of hospital admission on outcomes after severe traumatic brain injury in Austria. Wien. Klin. Wochenschr. 2014, 126, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.; Ryu, H.H. The off-hour effect on mortality in traumatic brain injury according to age group. PLoS ONE 2023, 18, e0282953. [Google Scholar] [CrossRef] [PubMed]
- Riyapan, S.; Chantanakomes, J.; Somboonkul, B.; Shin, S.D.; Chiang, W.C.; Network, P.C.R. Effect of Nighttime on Prehospital Care and Outcomes of Road Traffic Injuries in Asia: A Cross-Sectional Study of Data from the Pan-Asian Trauma Outcomes Study (PATOS). Prehospital Emerg. Care 2022, 26, 573–581. [Google Scholar] [CrossRef]
- Bossers, S.M.; Boer, C.; Greuters, S.; Bloemers, F.W.; Den Hartog, D.; Van Lieshout, E.M.M.; Hoogerwerf, N.; Innemee, G.; van der Naalt, J.; Absalom, A.R.; et al. Dutch Prospective Observational Study on Prehospital Treatment of Severe Traumatic Brain Injury: The BRAIN-PROTECT Study Protocol. Prehospital Emerg. Care 2019, 23, 820–827. [Google Scholar] [CrossRef]
- Horvath, B.; Kloesel, B.; Todd, M.M.; Cole, D.J.; Prielipp, R.C. The Evolution, Current Value, and Future of the American Society of Anesthesiologists Physical Status Classification System. Anesthesiology 2021, 135, 904–919. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J. Night admission to the emergency department: A factor delaying time to surgery in patients with head injury. J. Clin. Nurs. 2010, 19, 2763–2770. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, M.C.T.; Perel, P.; Arango, M.; Clayton, T.; Edwards, P.; Komolafe, E.; Poccock, S.; Roberts, I.; Shakur, H.; Steyerberg, E.; et al. Predicting outcome after traumatic brain injury: Practical prognostic models based on large cohort of international patients. BMJ 2008, 336, 425–429. [Google Scholar] [CrossRef]
- Peberdy, M.A.; Ornato, J.P.; Larkin, G.L.; Braithwaite, R.S.; Kashner, T.M.; Carey, S.M.; Meaney, P.A.; Cen, L.; Nadkarni, V.M.; Praestgaard, A.H.; et al. Survival from in-hospital cardiac arrest during nights and weekends. JAMA 2008, 299, 785–792. [Google Scholar] [CrossRef]
- Matsumura, Y.; Nakada, T.A.; Shinozaki, K.; Tagami, T.; Nomura, T.; Tahara, Y.; Sakurai, A.; Yonemoto, N.; Nagao, K.; Yaguchi, A.; et al. Nighttime is associated with decreased survival and resuscitation efforts for out-of-hospital cardiac arrests: A prospective observational study. Crit. Care 2016, 20, 141. [Google Scholar] [CrossRef]
- Wallace, S.K.; Abella, B.S.; Shofer, F.S.; Leary, M.; Agarwal, A.K.; Mechem, C.C.; Gaieski, D.F.; Becker, L.B.; Neumar, R.W.; Band, R.A. Effect of time of day on prehospital care and outcomes after out-of-hospital cardiac arrest. Circulation 2013, 127, 1591–1596. [Google Scholar] [CrossRef] [PubMed]
- Schriefl, C.; Mayr, F.B.; Poppe, M.; Zajicek, A.; Nurnberger, A.; Clodi, C.; Herkner, H.; Sulzgruber, P.; Lobmeyr, E.; Schober, A.; et al. Time of out-of-hospital cardiac arrest is not associated with outcome in a metropolitan area: A multicenter cohort study. Resuscitation 2019, 142, 61–68. [Google Scholar] [CrossRef]
- Egol, K.A.; Tolisano, A.M.; Spratt, K.F.; Koval, K.J. Mortality rates following trauma: The difference is night and day. J. Emergencies Trauma Shock. 2011, 4, 178–183. [Google Scholar] [CrossRef]
- Hirose, T.; Kitamura, T.; Katayama, Y.; Sado, J.; Kiguchi, T.; Matsuyama, T.; Kiyohara, K.; Takahashi, H.; Tachino, J.; Nakagawa, Y.; et al. Impact of nighttime and weekends on outcomes of emergency trauma patients: A nationwide observational study in Japan. Medicine 2020, 99, e18687. [Google Scholar] [CrossRef]
- Sutherland, M.; Ehrlich, H.; McKenney, M.; Elkbuli, A. Trauma outcomes for blunt and penetrating injuries by mode of transportation and day/night shift. Am. J. Emerg. Med. 2021, 48, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Guly, H.R.; Leighton, G.; Woodford, M.; Bouamra, O.; Lecky, F.; Trauma, A.; Research, N. The effect of working hours on outcome from major trauma. Emerg. Med. J. 2006, 23, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.G.; Reilly, P.M.; Schwab, C.W.; Branas, C.C.; Geiger, J.; Wiebe, D.J. Weekend and night outcomes in a statewide trauma system. Arch. Surg. 2011, 146, 810–817. [Google Scholar] [CrossRef]
- Laupland, K.B.; Ball, C.G.; Kirkpatrick, A.W. Hospital mortality among major trauma victims admitted on weekends and evenings: A cohort study. J. Trauma Manag. Outcomes 2009, 3, 8. [Google Scholar] [CrossRef]
- Ong, A.W.; Stephenson, J.; Gile, K.J.; Aronow, R.A.; Wang, X.; Xu, Y.; Martin, N.D.; Kim, P.K.; Fernandez, F.B. Outcome of Hypotensive Trauma Patients by Time and Day of Arrival. J. Surg. Res. 2021, 258, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Arbabi, S.; Jurkovich, G.J.; Wahl, W.L.; Kim, H.M.; Maier, R.V. Effect of patient load on trauma outcomes in a Level I trauma center. J. Trauma 2005, 59, 815–818; discussion 819–820. [Google Scholar] [CrossRef]
- Dybdal, B.; Svane, C.; Hesselfeldt, R.; Steinmetz, J.; Sorensen, A.M.; Rasmussen, L.S. Is there a diurnal difference in mortality of severely injured trauma patients? Emerg. Med. J 2015, 32, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Abe, T.; Matsumura, Y.; Hagiwara, S.; Saitoh, D.; Oshima, K. The off-hour effect among severe trauma patients: A nationwide cohort study in Japan. Surg. Today 2020, 50, 1480–1485. [Google Scholar] [CrossRef]
- Fitschen-Oestern, S.; Lippross, S.; Lefering, R.; Kluter, T.; Weuster, M.; Franke, G.M.; Kirsten, N.; Muller, M.; Schroder, O.; Seekamp, A.; et al. Does the time of the day affect multiple trauma care in hospitals? A retrospective analysis of data from the TraumaRegister DGU(R). BMC Emerg. Med. 2021, 21, 134. [Google Scholar] [CrossRef]
- Metcalfe, D.; Perry, D.C.; Bouamra, O.; Salim, A.; Lecky, F.E.; Woodford, M.; Edwards, A.; Costa, M.L. Is there a ‘weekend effect’ in major trauma? Emerg. Med. J. 2016, 33, 836–842. [Google Scholar] [CrossRef]


{kind=link}
| Overall n = 1794 | Day n = 1142 | Night n = 652 | p-Value | Missing | |
|---|---|---|---|---|---|
| Demographic data | |||||
| Age (years) s | 45 (23–65) | 50 (24–68) | 34 (22–57) | <0.001 | 20 |
| Male sex (n (%)) | 1259 (70.3) | 792 (69.4) | 457 (71.8) | 0.279 | 3 |
| ASA pre-injury s | 0.007 ^ | 347 | |||
| ASA 1 | 874 (60.1) | 528 (57.3) | 346 (65.0) | ||
| ASA 2 | 398 (27.4) | 273 (29.6) | 125 (23.5) | ||
| ASA 3 | 182 (12.5) | 121 (13.1) | 61 (11.5) | ||
| Mechanism of injury s | 0.005 ^ | 29 | |||
| MVA | 310 (17.2) | 154 (13.4) | 156 (23.9) | ||
| Motorcycle | 161 (8.9) | 102 (8.9) | 59 (9.0) | ||
| Bicycle | 393 (21.9) | 291 (25.4) | 102 (15.6) | ||
| Pedestrian | 122 (6.8) | 72 (6.3) | 50 (7.6) | ||
| Traffic other | 54 (3.0) | 34 (2.9) | 20 (3.0) | ||
| Fall from height | 622 (34.6) | 396 (34.6) | 226 (34.6) | ||
| Gunshot/stab injury | 34 (1.8) | 22 (1.9) | 12 (1.8) | ||
| Other | 69 (3.8) | 50 (4.3) | 19 (2.9) | ||
| GCS at arrival s | 4 (3–7) | 5 (3–7) | 4 (3–7) | 0.212 ^ | 0 |
| ISS s | 26 (18–34) | 26 (20–35) | 26 (17–34) | 0.243 | 208 |
| Pre-/in-hospital data | |||||
| Distance (km) | 24.2 (13.7–40.1) | 25.4 (15.7–41.9) | 22.1 (9.9–37.1) | <0.001 | 293 |
| Prehospital endotracheal intubation | 0.001 | ||||
| No | 56 (3.1) | 23 (2.0) | 32 (4.9) | 1 | |
| Yes successful | 1709 (93.5) | 1071 (93.8) | 607 (93.1) | 31 | |
| Yes unsuccessful | 38 (2.1) | 30 (2.6) | 7 (1.1) | 1 | |
| On-scene time (min) | 16 (11–24) | 16 (11–25) | 16 (11–24) | 0.426 # | 557 |
| Time to first CT scan | 22 (16–30) | 22 (16–31) | 22 (16–30) | 0.377 | 444 |
| Outcome | |||||
| 30-day mortality ± | 555 (33.0) | 378 (35.5) | 177 (28.7) | 0.004 | 111 |
| Hospital LOS (days) * | 9 (2–23) | 8 (2–23) | 10 (2–24) | 0.502 ^ | 137 |
| GOS at discharge | 0.015 | ||||
| Death | 571 (31.2%) | 382 (33.5%) | 178 (27.9%) | 11 | |
| Neurovegetative | 38 (2.1%) | 25 (2.2%) | 13 (2.0%) | 0 | |
| Severe disability | 596 (32.9%) | 372 (32.6%) | 212 (33.2%) | 12 | |
| Moderate disability | 175 (9.7%) | 105 (9.2%) | 68 (10.6%) | 2 | |
| Good recovery | 266 (14.7%) | 147 (12.9%) | 115 (18.0%) | 4 | |
| TBI category | |||||
| Confirmed | 1364 | 869 (86.6%) | 468 (82.25%) | 0.019 | |
| Isolated | 713 | 455 (45.4%) | 248 (43.5%) | 0.477 |
| Logistic Regression | OR | 95% CI | p-Value |
|---|---|---|---|
| Primary analysis—UDP—univariable | |||
| All patients | 0.74 | 0.60–0.91 | 0.004 * |
| Primary analysis—UDP—multivariable | |||
| All patients | 0.82 | 0.59–1.16 | 0.262 |
| Confirmed TBI | 0.89 | 0.60–1.31 | 0.543 |
| Isolated TBI | 0.51 | 0.34–0.76 | 0.001 * |
| Sensitivity analysis—6 p.m. to 6 a.m.—multivariable | |||
| All patients | 0.82 | 0.56–1.20 | 0.316 |
| Confirmed TBI | 0.88 | 0.57–1.35 | 0.566 |
| Isolated TBI | 0.63 | 0.38–1.05 | 0.077 |
| Logistic Regression | OR | 95% CI | p-Value |
|---|---|---|---|
| Glasgow Outcome Scale | |||
| All patients | 1.16 | 0.89–1.52 | 0.262 |
| Confirmed TBI | 1.02 | 0.72–1.43 | 0.921 |
| Isolated TBI | 1.36 | 0.88–2.09 | 0.168 |
| Hospital length of stay | IRR | ||
| All patients | 0.90 | 0.80–1.01 | 0.065 |
| Confirmed TBI | 0.92 | 0.83–1.02 | 0.097 |
| Isolated TBI | 0.87 | 0.76–0.99 | 0.033 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bulte, C.S.E.; Mansvelder, F.J.; Loer, S.A.; Bloemers, F.W.; Den Hartog, D.; Van Lieshout, E.M.M.; Hoogerwerf, N.; van der Naalt, J.; Absalom, A.R.; Peerdeman, S.M.; et al. Effect of Daytime versus Nighttime on Prehospital Care and Outcomes after Severe Traumatic Brain Injury. J. Clin. Med. 2024, 13, 2249. https://doi.org/10.3390/jcm13082249
Bulte CSE, Mansvelder FJ, Loer SA, Bloemers FW, Den Hartog D, Van Lieshout EMM, Hoogerwerf N, van der Naalt J, Absalom AR, Peerdeman SM, et al. Effect of Daytime versus Nighttime on Prehospital Care and Outcomes after Severe Traumatic Brain Injury. Journal of Clinical Medicine. 2024; 13(8):2249. https://doi.org/10.3390/jcm13082249
Chicago/Turabian StyleBulte, Carolien S. E., Floor J. Mansvelder, Stephan A. Loer, Frank W. Bloemers, Dennis Den Hartog, Esther M. M. Van Lieshout, Nico Hoogerwerf, Joukje van der Naalt, Anthony R. Absalom, Saskia M. Peerdeman, and et al. 2024. "Effect of Daytime versus Nighttime on Prehospital Care and Outcomes after Severe Traumatic Brain Injury" Journal of Clinical Medicine 13, no. 8: 2249. https://doi.org/10.3390/jcm13082249