
Prognostic Value of Standard Heart Failure Medication in Patients with Cardiac Transthyretin Amyloidosis

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Ethics
2.2. Patient Cohort
2.3. Inclusion Criteria
- -
- Age > 18 years;
- -
- Confirmed diagnosis of ATTR-CM;
- -
- Symptomatic heart failure with at least one hospitalization due to cardiac decompensation or symptoms of heart failure requiring treatment with loop diuretics.
2.4. Exclusion Criteria
- -
- Participation in interventional trials;
- -
- Treatment with disease-modifying therapies (silencers, stabilizers);
- -
- Changes in heart failure medication during the observation period;
- -
- Etiology for heart failure not primarily due to ATTR-CM, e.g., severe uncorrected valvular diseases, severe ischemic heart disease;
- -
- Predominantly neurological phenotype in ATTRv.
2.5. Assessment of Organ Involvement and Confirmation of ATTR Diagnosis
2.6. Clinical Examination
2.7. Laboratory Testing
2.8. Echocardiography
2.9. Medication Survey
2.10. Statistics
3. Results
3.1. Baseline Characteristics
3.2. Differences in Treatment
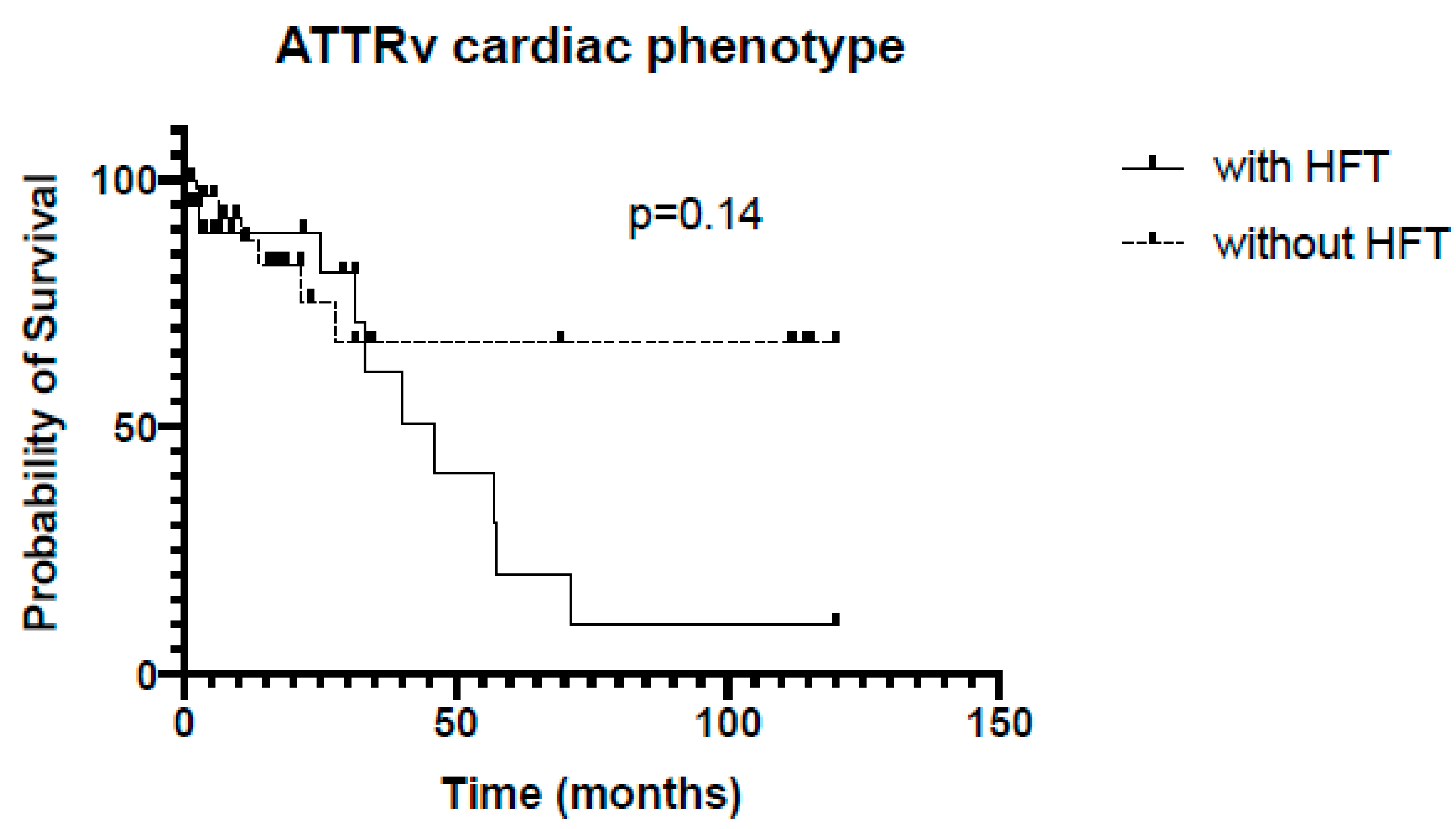
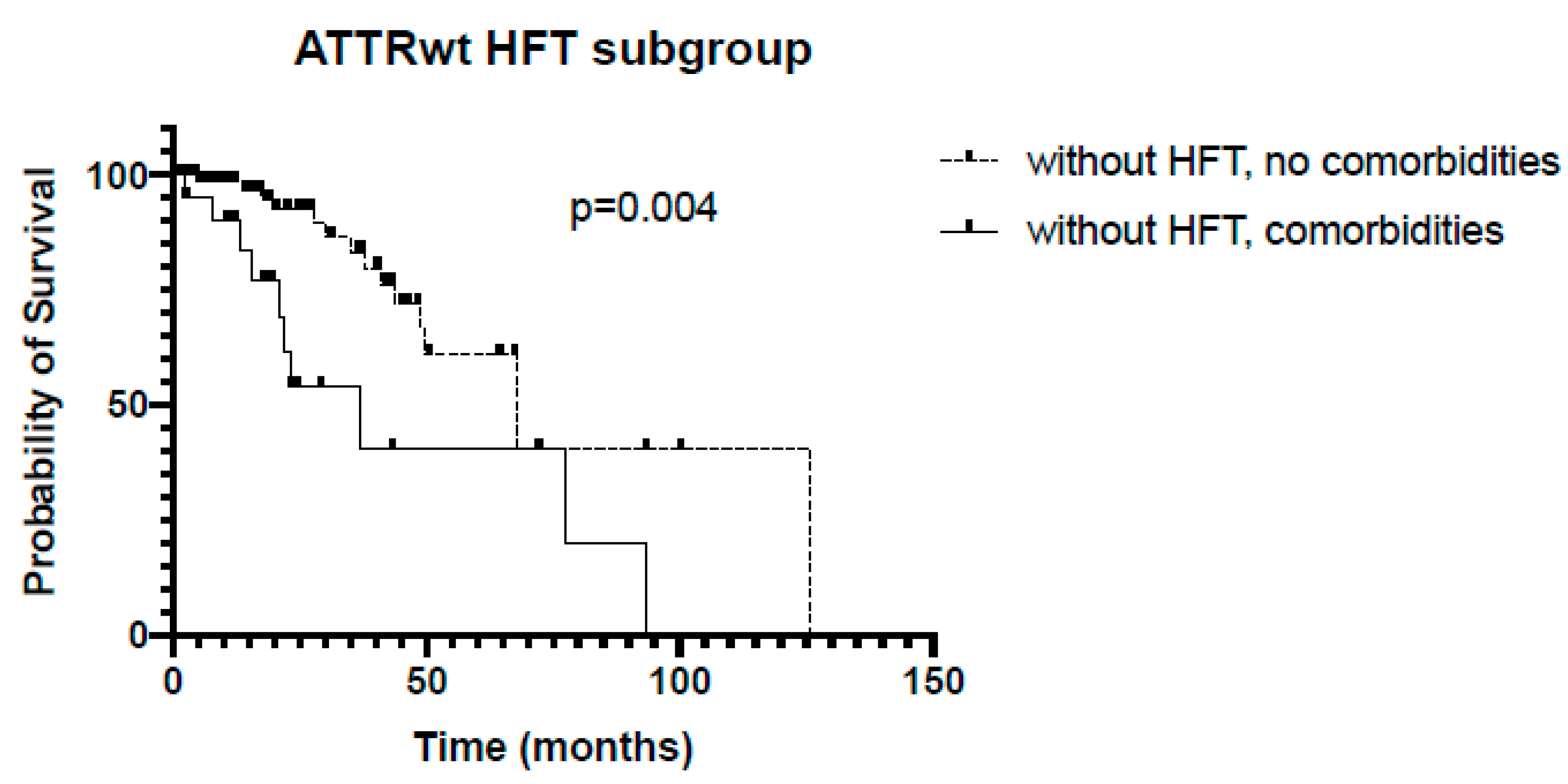
3.3. Subgroup Analysis
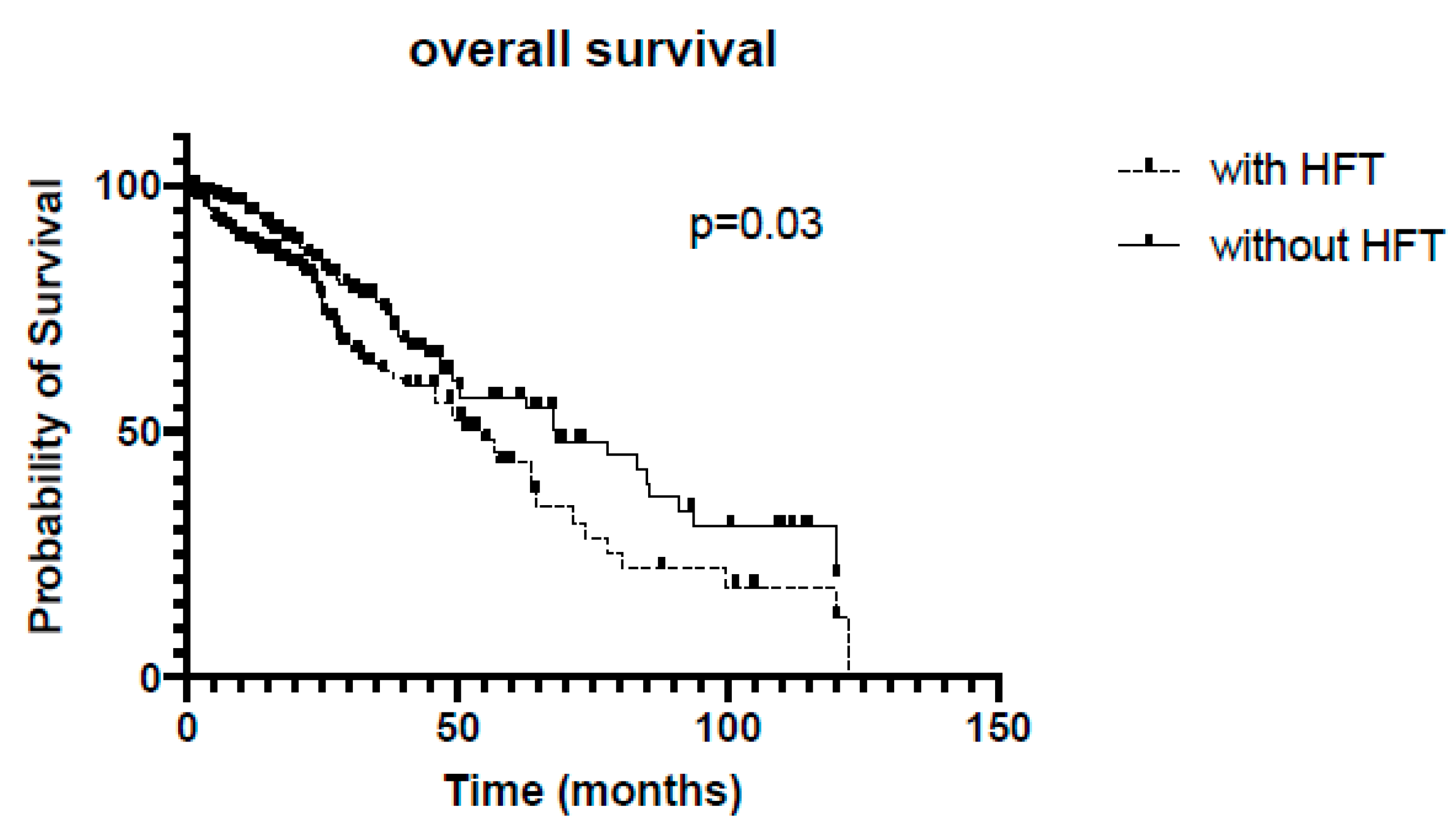
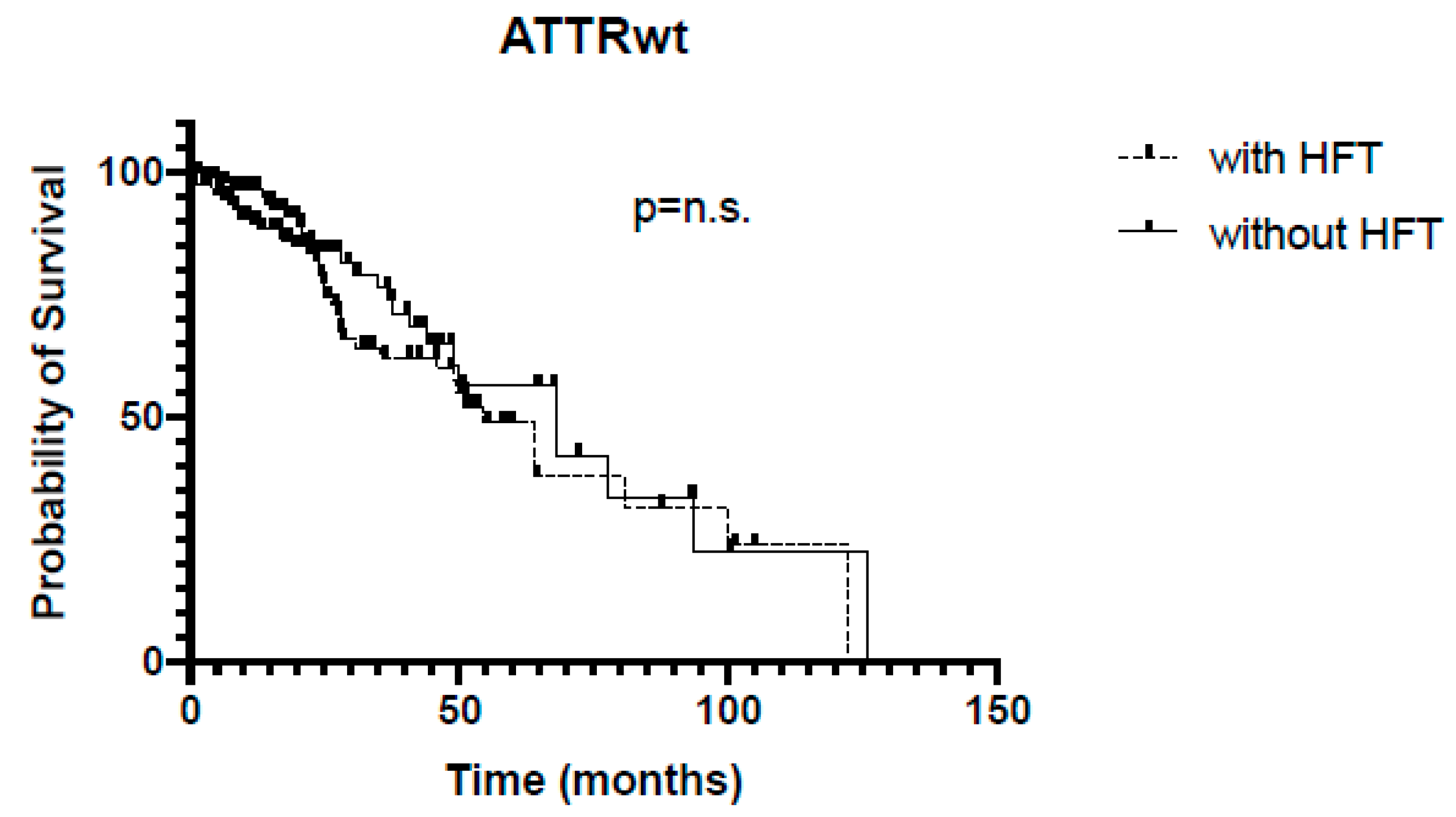
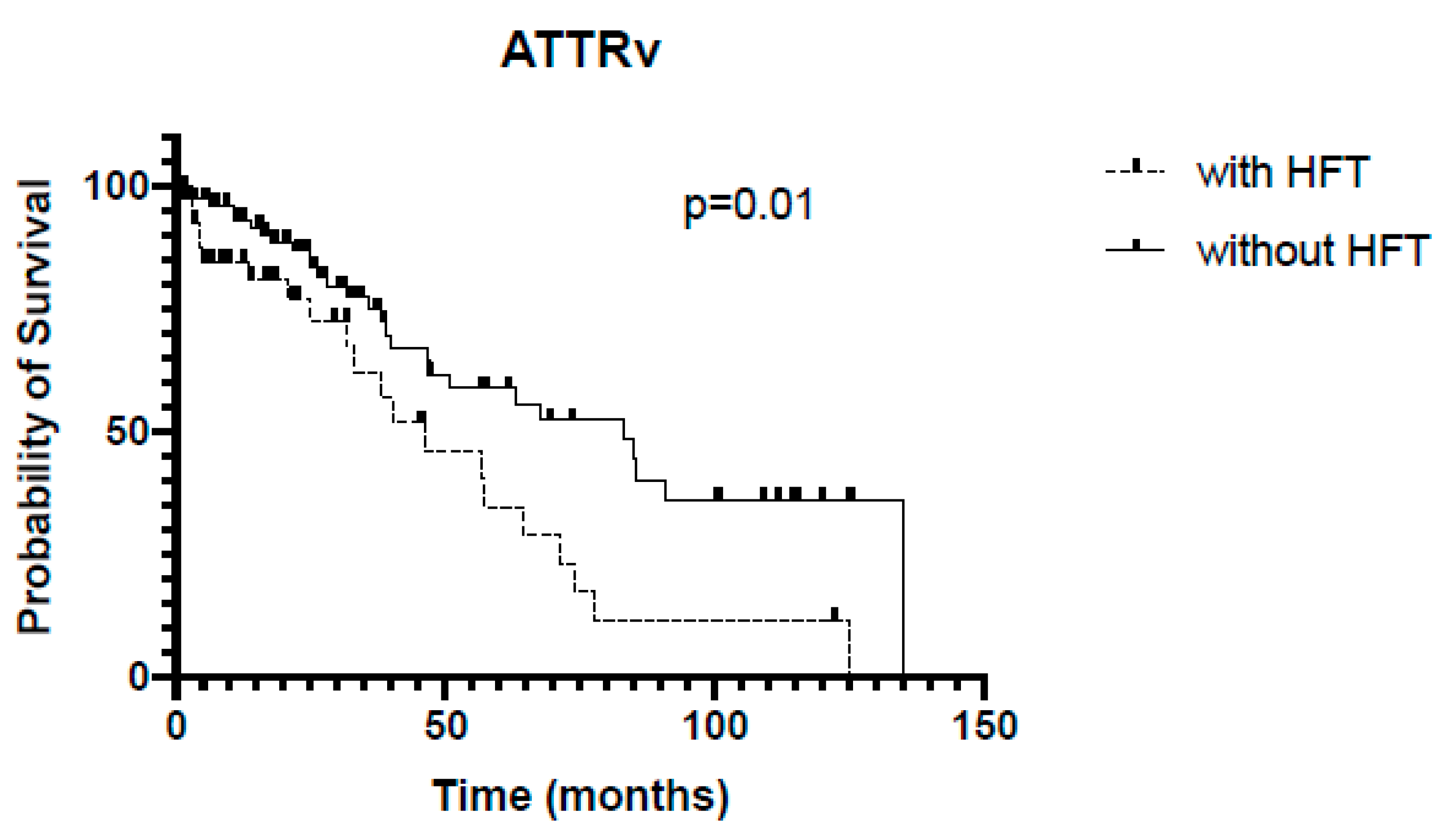
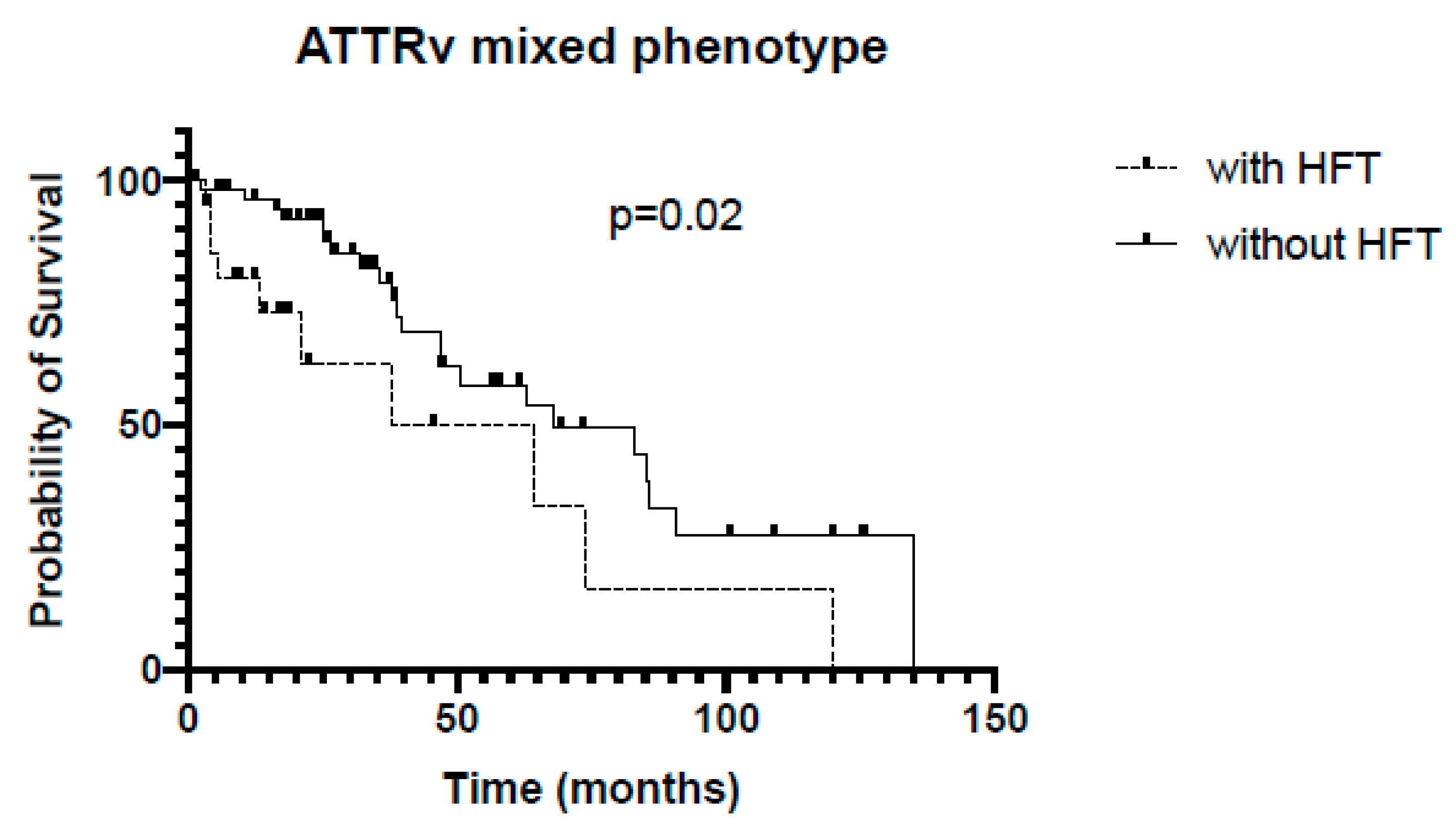
3.4. Survival Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia-Pavia, P.; Dominguez, F.; Gonzalez-Lopez, E. Transthyretin amyloid cardiomyopathy. Med. Clin. 2021, 156, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, V.; Agrawal, V.; Khulbe, Y.; Hanif, M.; Huang, H.; Hameed, M.; Shrestha, A.B.; Perone, F.; Parikh, C.; Gomez, S.I.; et al. Cardiac amyloidosis and aortic stenosis: A state-of-the-art review. Eur. Heart J. Open 2023, 3, oead106. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.F.; Mirzoyev, S.A.; Edwards, W.D.; Dogan, A.; Grogan, D.R.; Dunlay, S.M.; Roger, V.L.; Gertz, M.A.; Dispenzieri, A.; Zeldenrust, S.R.; et al. Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction. JACC Heart Fail. 2014, 2, 113–122. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.M.; Rosenblum, H.; Maurer, M.S. Pathophysiology and Therapeutic Approaches to Cardiac Amyloidosis. Circ. Res. 2021, 128, 1554–1575. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Damy, T.; Fontana, M.; Hutchinson, M.; Lachmann, H.J.; Martinez-Naharro, A.; Quarta, C.C.; Rezk, T.; Whelan, C.J.; Gonzalez-Lopez, E.; et al. A new staging system for cardiac transthyretin amyloidosis. Eur. Heart J. 2018, 39, 2799–2806. [Google Scholar] [CrossRef]
- Grogan, M.; Scott, C.G.; Kyle, R.A.; Zeldenrust, S.R.; Gertz, M.A.; Lin, G.; Klarich, K.W.; Miller, W.L.; Maleszewski, J.J.; Dispenzieri, A. Natural History of Wild-Type Transthyretin Cardiac Amyloidosis and Risk Stratification Using a Novel Staging System. J. Am. Coll. Cardiol. 2016, 68, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Elliott, P.; Comenzo, R.; Semigran, M.; Rapezzi, C. Addressing Common Questions Encountered in the Diagnosis and Management of Cardiac Amyloidosis. Circulation. 2017, 135, 1357–1377. [Google Scholar] [CrossRef]
- Coelho, T.; Maia, L.F.; Martins da Silva, A.; Waddington Cruz, M.; Plante-Bordeneuve, V.; Lozeron, P.; Suhr, O.B.; Campistol, J.M.; Conceição, I.M.; Schmidt, H.H.-J.; et al. Tafamidis for transthyretin familial amyloid polyneuropathy: A randomized, controlled trial. Neurology 2012, 79, 785–792. [Google Scholar] [CrossRef]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef]
- Benson, M.D.; Waddington-Cruz, M.; Berk, J.L.; Polydefkis, M.; Dyck, P.J.; Wang, A.K.; Planté-Bordeneuve, V.; Barroso, F.A.; Merlini, G.; Obici, L.; et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Sultan, M.B.; Rapezzi, C. Tafamidis for Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2019, 380, 196–197. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis treatment of acute chronic heart failure: Developed by the Task Force for the diagnosis treatment of acute chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for heart failure with preserved ejection fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Bohm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, A.; Massa, P.; Patel, R.K.; Razvi, Y.; Porcari, A.; Rauf, M.U.; Jiang, A.; Cabras, G.; Filisetti, S.; E Bolhuis, R.; et al. Conventional heart failure therapy in cardiac ATTR amyloidosis. Eur. Heart J. 2023, 44, 2893–2907. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Yusuf, S.; Bussmann, W.D.; Sleight, P.; Uprichard, A.; Massie, B.; McGrath, B.; Nilsson, B.; Pitt, B.; Magnani, B. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. J. Am. Med. Assoc. 1995, 273, 1450–1456. [Google Scholar] [CrossRef]
- Braunwald, E. SGLT2 inhibitors: The statins of the 21st century. Eur. Heart J. 2022, 43, 1029–1030. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- Patoulias, D.; Papadopoulos, C.; Doumas, M. “SGLT2i in patients with transthyretin cardiac amyloidosis, a well-tolerated option for heart failure treatment? Results from a small, real-world, patients series” comment. Intern. Emerg. Med. 2022, 17, 1553–1554. [Google Scholar] [CrossRef] [PubMed]
- Dobner, S.; Bernhard, B.; Asatryan, B.; Windecker, S.; Stortecky, S.; Pilgrim, T.; Gräni, C.; Hunziker, L. SGLT2 inhibitor therapy for transthyretin amyloid cardiomyopathy: Early tolerance and clinical response to dapagliflozin. ESC Heart Fail. 2023, 10, 397–404. [Google Scholar] [CrossRef]
- Gonzalez-Lopez, E.; Gallego-Delgado, M.; Guzzo-Merello, G.; de Haro-Del Moral, F.J.; Cobo-Marcos, M.; Robles, C.; Bornstein, B.; Salas, C.; Lara-Pezzi, E.; Alonso-Pulpon, L.; et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur. Heart J. 2015, 36, 2585–2594. [Google Scholar] [CrossRef]
- Rubin, J.; Maurer, M.S. Cardiac Amyloidosis: Overlooked, Underappreciated, and Treatable. Annu. Rev. Med. 2020, 71, 203–219. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Siepen, F.A.D.; Donal, E.; Lairez, O.; van der Meer, P.; Kristen, A.V.; Mercuri, M.F.; Michalon, A.; Frost, R.J.; Grimm, J.; et al. Phase 1 Trial of Antibody NI006 for Depletion of Cardiac Transthyretin Amyloid. N. Engl. J. Med. 2023, 389, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Rapezzi, C.; Elliott, P.; Damy, T.; Nativi-Nicolau, J.; Berk, J.L.; Velazquez, E.J.; Boman, K.; Gundapaneni, B.; Patterson, T.A.; Schwartz, J.H.; et al. Efficacy of Tafamidis in Patients with Hereditary and Wild-Type Transthyretin Amyloid Cardiomyopathy: Further Analyses From ATTR-ACT. JACC Heart Fail. 2021, 9, 115–123. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ATTRv (n = 135) | ATTRwt (n = 268) | p-Value | |
|---|---|---|---|
| Age (years) | 63 ± 9 | 74 ± 6 | <0.0001 |
| Gender (n, % male) | 102 (76%) | 246 (92%) | <0.0001 |
| Karnofsky Index (%) | 78 ± 11 | 81 ± 9 | 0.004 |
| aHT (n, %) | 43 (32%) | 167 (62%) | <0.0001 |
| CAD (n, %) | 25 (19%) | 95 (35%) | 0.0002 |
| NYHA (n, %) | 0.001 | ||
| I: | 24 (18%) | 19 (7%) | |
| II: | 54 (40%) | 100 (37%) | |
| III: | 55 (41%) | 145 (54%) | |
| IV: | 2 (1%) | 4 (1%) | |
| TTR variants (n, %): | |||
| p.Val40Ile | 29 (21%) | - | |
| p.Val50Met | 34 (25%) | - | |
| p.Val142Ile | 8 (6%) | - | |
| p.Ile127Val | 9 (7%) | - | |
| p.Cys30Arg | 6 (4%) | - | |
| p.Leu78His | 5 (4%) | - | |
| Other | 44 (33%) | - | |
| Phenotype (n, %): | |||
| cardiac | 52 (39%) | - | |
| mixed (cardiac/neurologic) | 83 (61%) | - |
| ATTRv (n = 135) | ATTRwt (n = 268) | |||||
|---|---|---|---|---|---|---|
| +HFT, n = 43 | −HFT, n = 92 | p-Value | +HFT, n = 140 | −HFT, n = 128 | p-Value | |
| Age (years) | 65 ± 8 | 62 ± 10 | 0.09 | 74 ± 7 | 74 ± 6 | 0.92 |
| Gender (n, % male) | 36 (84%) | 66 (72%) | 0.20 | 130 (93%) | 116 (91%) | 0.51 |
| Karnofsky Index (%) | 78 ± 11 | 77 ± 11 | 0.89 | 80 ± 8 | 82 ± 9 | 0.15 |
| Systolic blood pressure (mmHg) | 111 ± 22 | 118 ± 20 | 0.12 | 121 ± 18 | 125 ± 18 | 0.15 |
| Diastolic blood pressure (mmHg) | 72 ± 13 | 73 ± 13 | 0.57 | 75 ± 11 | 77 ± 11 | 0.07 |
| LVEF (%) | 40 ± 14 | 48 ± 16 | 0.01 | 44 ± 15 | 45 ± 16 | 0.60 |
| IVS (mm) | 19 ± 3 | 20 ± 4 | 0.12 | 19 ± 3 | 19 ± 4 | 0.78 |
| NT-proBNP (ng/L) | 8598 ± 17,557 | 3562 ± 3808 | 0.02 | 5711 ± 4943 | 5811 ± 9924 | 0.92 |
| hsTroponin-T (pg/mL) | 86 ± 143 | 58 ± 38 | 0.14 | 68 ± 52 | 60 ± 61 | 0.29 |
| eGFR (mL/min × 1.73 m2) | 69 ± 31 | 89 ± 33 | 0.002 | 64 ± 23 | 68 ± 22 | 0.25 |
| Comorbidities: | 0.24 | 0.85 | ||||
| aHT (n, %) | 20 (47%) | 23 (25%) | 97 (69%) | 70 (55%) | ||
| CAD (n, %) | 8 (19%) | 17 (18%) | 54 (39%) | 41 (32%) | ||
| NYHA (n, %) | 0.12 | 0.42 | ||||
| I: | 4 (9%) | 20 (22%) | 7 (5%) | 12 (9%) | ||
| II: | 16 (37%) | 38 (41%) | 50 (36%) | 50 (39%) | ||
| III: | 23 (53%) | 32 (35%) | 81 (58%) | 64 (50%) | ||
| IV: | 0 (0%) | 2 (2%) | 2 (1%) | 2 (2%) | ||
| TTR Variants (n, %): | 0.11 | |||||
| p.Val40Ile | 16 (37%) | 13 (14%) | - | - | ||
| p.Val50Met | 8 (19%) | 26 (28%) | - | - | ||
| p.Val142Ile | 3 (7%) | 5 (5%) | - | - | ||
| p.Ile127Val | 3 (7%) | 6 (7%) | - | - | ||
| p.Cys30Arg | 2 (5%) | 4 (4%) | - | - | ||
| p.Leu78His | 1 (2%) | 4 (4%) | - | - | ||
| Other | 10 (23%) | 34 (37%) | - | - | ||
| Phenotype (n, %): | 0.06 | |||||
| cardiac | 22 (51%) | 30 (33%) | - | - | ||
| mixed (cardiac/PNP) | 21 (49%) | 62 (67%) | - | - |
| Cardiac Phenotype | Mixed Phenotype | |||||
|---|---|---|---|---|---|---|
| +HFT, n = 22 | −HFT, n = 31 | p-Value | +HFT, n = 21 | −HFT, n = 62 | p-Value | |
| Age (years) | 63 ± 9 | 62 ± 9 | 0.69 | 67 ± 6 | 62 ± 10 | 0.02 |
| Gender (n, % male) | 17 (77%) | 21 (67%) | 0.54 | 19 (90%) | 45 (73%) | 0.13 |
| Karnofsky Index (%) | 81 ± 7 | 85 ± 9 | 0.20 | 76 ± 13 | 75 ± 10 | 0.83 |
| Systolic blood pressure (mmHg) | 109 ± 21 | 121 ± 17 | 0.04 | 114 ± 23 | 117 ± 21 | 0.63 |
| Diastolic blood pressure (mmHg) | 70 ± 13 | 74 ± 12 | 0.21 | 74 ± 13 | 72 ± 13 | 0.69 |
| LVEF (%) | 40 ± 10 | 39 ± 15 | 0.86 | 40 ± 14 | 46 ± 12 | 0.12 |
| IVS (mm) | 18 ± 2 | 19 ± 3 | 0.29 | 19 ± 4 | 20 ± 4 | 0.68 |
| NT-proBNP (ng/L) | 7811 ± 8088 | 4208 ± 3972 | 0.046 | 9472 ± 24,418 | 2866 ± 3624 | 0.06 |
| hsTroponin-T (pg/mL) | 68 ± 39 | 61 ± 44 | 0.62 | 106 ± 202 | 51 ± 36 | 0.08 |
| eGFR (ml/min) | 60 ± 22 | 72 ± 21 | 0.06 | 79 ± 35 | 96 ± 35 | 0.06 |
| Comorbidities: | 0.45 | 0.46 | ||||
| aHT (n, %) | 14 (64%) | 9 (29%) | 4 (19%) | 14 (23%) | ||
| CAD (n, %) | 4 (18%) | 6 (19%) | 6 (29%) | 10 (16%) | ||
| NYHA (n, %) | 0.34 | 0.40 | ||||
| I: | 1 (5%) | 4 (13%) | 2 (10%) | 11 (18%) | ||
| II: | 7 (32%) | 12 (39%) | 5 (24%) | 19 (31%) | ||
| III: | 14 (64%) | 13 (42%) | 14 (67%) | 31 (50%) | ||
| IV: | 0 (0%) | 2 (6%) | 0 (0%) | 0 (0%) | ||
| Mutations (n, %): | 0.30 | 0.48 | ||||
| p.Val40Ile | 13 (59%) | 9 (29%) | 3 (14%) | 4 (6%) | ||
| p.Val50Met | 1 (5%) | 3 (10%) | 7 (33%) | 23 (37%) | ||
| p.Val142Ile | 2 (9%) | 5 (16%) | 1 (5%) | 0 (0%) | ||
| p.Ile127Val | 0 (0%) | 0 (0%) | 3 (14%) | 6 (10%) | ||
| p.Cys30Arg | 1 (5%) | 2 (6%) | 0 (0%) | 2 (3%) | ||
| p.Leu78His | 0 (0%) | 0 (0%) | 1 (5%) | 4 (6%) | ||
| Other | 5 (23%) | 12 (39%) | 6 (29%) | 23 (37%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
aus dem Siepen, F.; Hein, S.; Hofmann, E.; Nagel, C.; Schwarting, S.K.; Hegenbart, U.; Schönland, S.O.; Weiler, M.; Frey, N.; Kristen, A.V. Prognostic Value of Standard Heart Failure Medication in Patients with Cardiac Transthyretin Amyloidosis. J. Clin. Med. 2024, 13, 2257. https://doi.org/10.3390/jcm13082257
aus dem Siepen F, Hein S, Hofmann E, Nagel C, Schwarting SK, Hegenbart U, Schönland SO, Weiler M, Frey N, Kristen AV. Prognostic Value of Standard Heart Failure Medication in Patients with Cardiac Transthyretin Amyloidosis. Journal of Clinical Medicine. 2024; 13(8):2257. https://doi.org/10.3390/jcm13082257
Chicago/Turabian Styleaus dem Siepen, Fabian, Selina Hein, Eva Hofmann, Christian Nagel, Stéphanie K. Schwarting, Ute Hegenbart, Stefan O. Schönland, Markus Weiler, Norbert Frey, and Arnt V. Kristen. 2024. "Prognostic Value of Standard Heart Failure Medication in Patients with Cardiac Transthyretin Amyloidosis" Journal of Clinical Medicine 13, no. 8: 2257. https://doi.org/10.3390/jcm13082257