
Early Rectal Cancer and Local Excision: A Narrative Review

 , , and
, , and 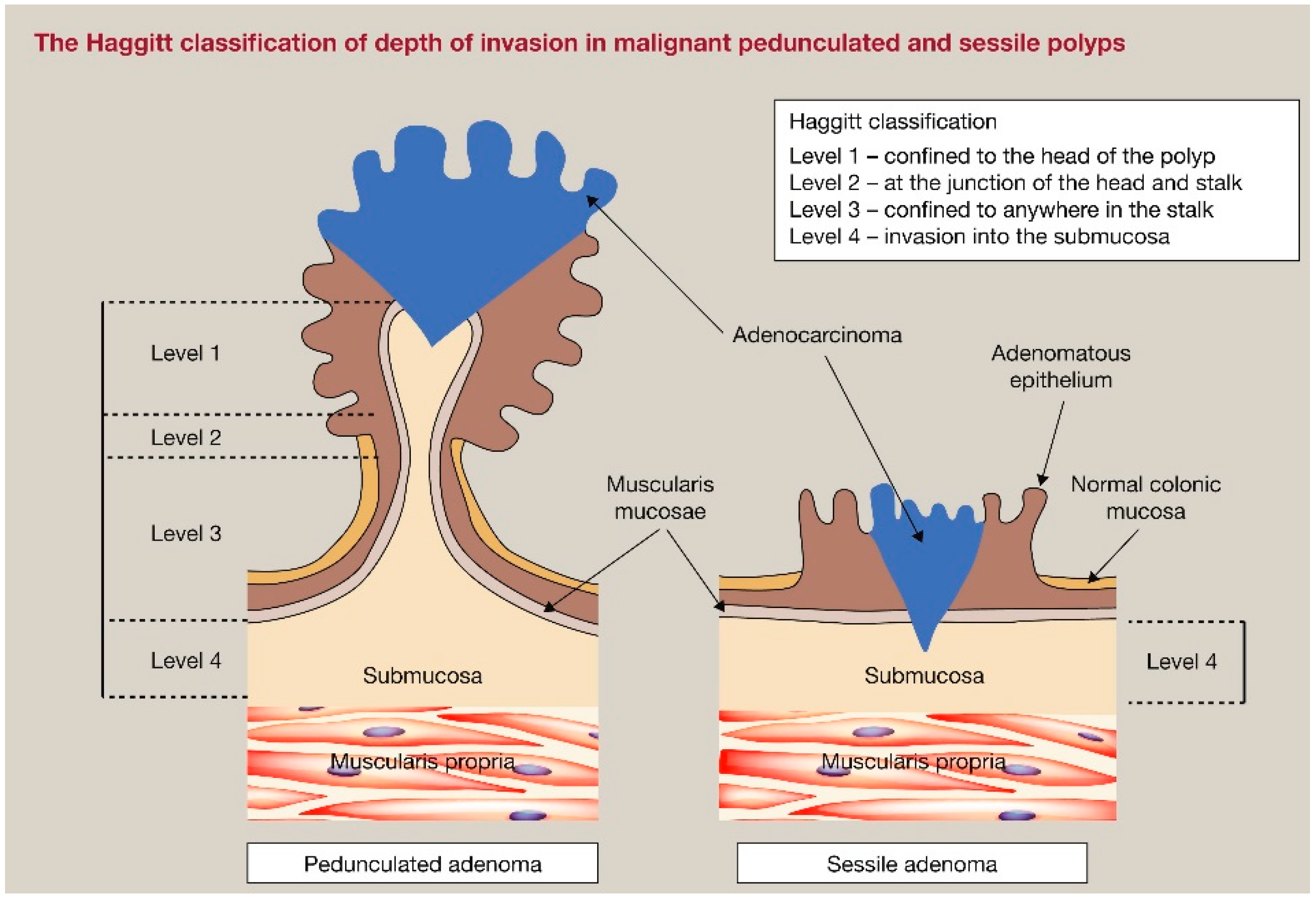{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Staging
3.1. Endoscopic Optic Evaluation
3.2. MRI
3.3. ERUS
4. Surgical and Endoscopic Techniques
4.1. Total Mesorectal Excision (TME)
4.2. Local Excision Techniques
4.2.1. Trans-Sacral (Kraske) or Trans-Sphincteric (York-Mason) Approaches
4.2.2. Transanal Excision (TAE)
4.2.3. Transanal Endoscopic Microsurgery (TEM)
4.2.4. Transanal Minimally Invasive Surgery (TAMIS)
4.2.5. Endoscopic Submucosal Dissection (ESD)
4.2.6. Endoscopic Intermuscular Dissection (EID)
4.2.7. Endoscopic Full-Thickness Resection (EFTR)
5. Risk-Adapted Early Rectal Cancer Management
5.1. Low-Risk Early Rectal Cancer
5.2. High-Risk Early Rectal Cancer
5.3. Worsening Restaging on Pathology after Local Excision
6. Chemotherapy and Radiotherapy in Early Rectal Cancer
6.1. Neoadjuvant Therapy
6.2. Adjuvant Therapy
7. Future Perspectives
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Giesen, L.J.X.; Olthof, P.B.; Elferink, M.A.G.; van Westreenen, H.L.; Beets, G.L.; Verhoef, C.; Dekker, J.W.T. Changes in Rectal Cancer Treatment after the Introduction of a National Screening Program; Increasing Use of Less Invasive Strategies within a National Cohort. Eur. J. Surg. Oncol. 2022, 48, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.J.A.; Whitehouse, L.E.; Farrell, T.; Nickerson, C.; Thomas, J.D.; Quirke, P.; Rutter, M.D.; Rees, C.; Finan, P.J.; Wilkinson, J.R.; et al. A Retrospective Observational Study Examining the Characteristics and Outcomes of Tumours Diagnosed within and without of the English NHS Bowel Cancer Screening Programme. Br. J. Cancer 2012, 107, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterology 2020, 158, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.-G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-Onset Colorectal Cancer in Young Individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C. Local Excision for Early Rectal Cancer. Clin. Oncol. R. Coll. Radiol. 2023, 35, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Altomare, N.J.; Mulcahy, M.F. Evolution of Therapy for Locally Advanced Rectal Cancer. J. Surg. Oncol. 2024, 129, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Knol, J.; Keller, D.S. Total Mesorectal Excision Technique-Past, Present, and Future. Clin. Colon. Rectal Surg. 2020, 33, 134–143. [Google Scholar] [CrossRef]
- van der Heijden, J.A.G.; Koëter, T.; Smits, L.J.H.; Sietses, C.; Tuynman, J.B.; Maaskant-Braat, A.J.G.; Klarenbeek, B.R.; de Wilt, J.H.W. Functional Complaints and Quality of Life after Transanal Total Mesorectal Excision: A Meta-Analysis. Br. J. Surg. 2020, 107, 489–498. [Google Scholar] [CrossRef]
- Rizzo, G.; Pafundi, D.P.; Sionne, F.; Pietricola, G.; D’Agostino, L.; Gambacorta, M.A.; Valentini, V.; Coco, C. Transanal Endoscopic Microsurgery Versus Total Mesorectal Excision in ypT0-1 Rectal Cancer After Preoperative Radiochemotherapy: Postoperative Morbidity, Functional Results, and Long-Term Oncologic Outcome. Dis. Colon. Rectum 2022, 65, 1306–1315. [Google Scholar] [CrossRef]
- Young, D.O.; Kumar, A.S. Local Excision of Rectal Cancer. Surg. Clin. N. Am. 2017, 97, 573–585. [Google Scholar] [CrossRef]
- Jones, H.J.S.; Hompes, R.; Mortensen, N.; Cunningham, C. Modern Management of T1 Rectal Cancer by Transanal Endoscopic Microsurgery: A 10-Year Single-Centre Experience. Colorectal Dis. 2018, 20, 586–592. [Google Scholar] [CrossRef]
- Stitzenberg, K.B.; Barnes, E. Advances in Rectal Cancer Surgery. Clin. Colorectal Cancer 2022, 21, 55–62. [Google Scholar] [CrossRef]
- Ung, L.; Chua, T.C.; Engel, A.F. A Systematic Review of Local Excision Combined with Chemoradiotherapy for Early Rectal Cancer. Colorectal Dis. 2014, 16, 502–515. [Google Scholar] [CrossRef]
- Borstlap, W.A.A.; Tanis, P.J.; Koedam, T.W.A.; Marijnen, C.A.M.; Cunningham, C.; Dekker, E.; van Leerdam, M.E.; Meijer, G.; van Grieken, N.; Nagtegaal, I.D.; et al. A Multi-Centred Randomised Trial of Radical Surgery versus Adjuvant Chemoradiotherapy after Local Excision for Early Rectal Cancer. BMC Cancer 2016, 16, 513. [Google Scholar] [CrossRef]
- Weiser, M.R. AJCC 8th Edition: Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 1454–1455. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. ESMO Guidelines Committee Rectal Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Choi, Y.S.; Kim, W.S.; Hwang, S.W.; Park, S.H.; Yang, D.-H.; Ye, B.D.; Myung, S.-J.; Yang, S.-K.; Byeon, J.-S. Clinical Outcomes of Submucosal Colorectal Cancer Diagnosed after Endoscopic Resection: A Focus on the Need for Surgery. Intest. Res. 2020, 18, 96–106. [Google Scholar] [CrossRef]
- Yamada, M.; Saito, Y.; Sakamoto, T.; Nakajima, T.; Kushima, R.; Parra-Blanco, A.; Matsuda, T. Endoscopic Predictors of Deep Submucosal Invasion in Colorectal Laterally Spreading Tumors. Endoscopy 2016, 48, 456–464. [Google Scholar] [CrossRef]
- D’Amico, F.; Amato, A.; Iannone, A.; Trovato, C.; Romana, C.; Angeletti, S.; Maselli, R.; Radaelli, F.; Fiori, G.; Viale, E.; et al. Risk of Covert Submucosal Cancer in Patients with Granular Mixed Laterally Spreading Tumors. Clin. Gastroenterol. Hepatol. 2021, 19, 1395–1401. [Google Scholar] [CrossRef]
- Backes, Y.; Moss, A.; Reitsma, J.B.; Siersema, P.D.; Moons, L.M.G. Narrow Band Imaging, Magnifying Chromoendoscopy, and Gross Morphological Features for the Optical Diagnosis of T1 Colorectal Cancer and Deep Submucosal Invasion: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2017, 112, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.-J.; Huang, X.-X.; Lu, Z.-Z.; Wu, H.-F.; Lv, D.-D. A Diagnostic Test: Diagnostic Value of Gastrointestinal Endoscopy Narrow-Band Imaging (NBI) for Colorectal Laterally Spreading Tumor (LST) and Submucosal Invasion. Transl. Cancer Res. 2022, 11, 4389–4396. [Google Scholar] [CrossRef]
- Saito, S.; Tajiri, H.; Ikegami, M. Endoscopic Features of Submucosal Deeply Invasive Colorectal Cancer with NBI Characteristics: S Saito et al. Endoscopic Images of Early Colorectal Cancer. Clin. J. Gastroenterol. 2015, 8, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Sano, Y.; Tanaka, S.; Kudo, S.-E.; Saito, S.; Matsuda, T.; Wada, Y.; Fujii, T.; Ikematsu, H.; Uraoka, T.; Kobayashi, N.; et al. Narrow-Band Imaging (NBI) Magnifying Endoscopic Classification of Colorectal Tumors Proposed by the Japan NBI Expert Team. Dig. Endosc. 2016, 28, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yang, Z.; Yao, Y.; Liu, G.; Chen, R. Diagnostic Accuracy of Magnifying Chromoendoscopy in the Assessment of Tumor Invasion Depth in Early Colorectal Cancer: A Systematic Review and Meta-Analysis. Tech. Coloproctol. 2023, 27, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Davila, R.E. Chromoendoscopy. Gastrointest. Endosc. Clin. N. Am. 2009, 19, 193–208.e1. [Google Scholar] [CrossRef] [PubMed]
- Tischendorf, J.J.W.; Wasmuth, H.E.; Koch, A.; Hecker, H.; Trautwein, C.; Winograd, R. Value of Magnifying Chromoendoscopy and Narrow Band Imaging (NBI) in Classifying Colorectal Polyps: A Prospective Controlled Study. Endoscopy 2007, 39, 1092–1096. [Google Scholar] [CrossRef]
- Detering, R.; van Oostendorp, S.E.; Meyer, V.M.; van Dieren, S.; Bos, A.C.R.K.; Dekker, J.W.T.; Reerink, O.; van Waesberghe, J.H.T.M.; Marijnen, C.A.M.; Moons, L.M.G.; et al. MRI cT1-2 Rectal Cancer Staging Accuracy: A Population-Based Study. Br. J. Surg. 2020, 107, 1372–1382. [Google Scholar] [CrossRef]
- Rosén, R.; Nilsson, E.; Rahman, M.; Rönnow, C.-F. Accuracy of MRI in Early Rectal Cancer: National Cohort Study. Br. J. Surg. 2022, 109, 570–572. [Google Scholar] [CrossRef]
- Brodsky, J.T.; Richard, G.K.; Cohen, A.M.; Minsky, B.D. Variables Correlated with the Risk of Lymph Node Metastasis in Early Rectal Cancer. Cancer 1992, 69, 322–326. [Google Scholar] [CrossRef]
- Gormly, K. Rectal MRI: The Importance of High Resolution T2 Technique. Abdom. Radiol. 2021, 46, 4090–4095. [Google Scholar] [CrossRef]
- Hope, T.A.; Kassam, Z.; Loening, A.; McNamara, M.M.; Paspulati, R. The Use of PET/MRI for Imaging Rectal Cancer. Abdom. Radiol. 2019, 44, 3559–3568. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Friedman, K.; Chandarana, H.; Melsaether, A.; Moy, L.; Ding, Y.-S.; Jhaveri, K.; Beltran, L.; Jain, R. Current Status of Hybrid PET/MRI in Oncologic Imaging. AJR Am. J. Roentgenol. 2016, 206, 162–172. [Google Scholar] [CrossRef]
- Dj, K.; Jh, K.; Yh, R.; Tj, J.; Js, Y.; Jj, C. Nodal Staging of Rectal Cancer: High-Resolution Pelvic MRI versus 18F-FDGPET/CT. J. Comput. Assist. Tomogr. 2011, 35, 531–534. [Google Scholar] [CrossRef]
- Patel, R.K.; Sayers, A.E.; Kumar, P.; Khulusi, S.; Razack, A.; Hunter, I.A. The Role of Endorectal Ultrasound and Magnetic Resonance Imaging in the Management of Early Rectal Lesions in a Tertiary Center. Clin. Colorectal Cancer 2014, 13, 245–250. [Google Scholar] [CrossRef]
- Luglio, G.; Pagano, G.; Tropeano, F.P.; Spina, E.; Maione, R.; Chini, A.; Maione, F.; Galloro, G.; Giglio, M.C.; De Palma, G.D. Endorectal Ultrasonography and Pelvic Magnetic Resonance Imaging Show Similar Diagnostic Accuracy in Local Staging of Rectal Cancer: An Update Systematic Review and Meta-Analysis. Diagnostics 2021, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.P.H.; Patel, R.; Mbuagbaw, L.; Thabane, L.; Yaghoobi, M. EUS versus Magnetic Resonance Imaging in Staging Rectal Adenocarcinoma: A Diagnostic Test Accuracy Meta-Analysis. Gastrointest. Endosc. 2019, 90, 196–203.e1. [Google Scholar] [CrossRef]
- Gibiino, G.; Sbrancia, M.; Binda, C.; Coluccio, C.; Fabbri, S.; Giuffrida, P.; Gallo, G.; Saragoni, L.; Maselli, R.; Repici, A.; et al. Usefulness of Contrast-Enhanced Endoscopic Ultrasound (CH-EUS) to Guide the Treatment Choice in Superficial Rectal Lesions: A Case Series. Diagnostics 2023, 13, 2267. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef]
- You, Y.N.; Hardiman, K.M.; Bafford, A.; Poylin, V.; Francone, T.D.; Davis, K.; Paquette, I.M.; Steele, S.R.; Feingold, D.L.; On Behalf of the Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Rectal Cancer. Dis. Colon. Rectum 2020, 63, 1191–1222. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Chokshi, R.V. Low Anterior Resection Syndrome. Curr. Gastroenterol. Rep. 2020, 22, 48. [Google Scholar] [CrossRef]
- Bleier, J.I.S.; Maykel, J.A. Outcomes Following Proctectomy. Surg. Clin. N. Am. 2013, 93, 89–106. [Google Scholar] [CrossRef]
- Celentano, V.; Cohen, R.; Warusavitarne, J.; Faiz, O.; Chand, M. Sexual Dysfunction Following Rectal Cancer Surgery. Int. J. Colorectal Dis. 2017, 32, 1523–1530. [Google Scholar] [CrossRef]
- Weinberg, B.A.; Marshall, J.L.; Salem, M.E. The Growing Challenge of Young Adults with Colorectal Cancer. Oncology 2017, 31, 381–389. [Google Scholar]
- Sengupta, S.; Tjandra, J.J. Local Excision of Rectal Cancer: What Is the Evidence? Dis. Colon. Rectum 2001, 44, 1345–1361. [Google Scholar] [CrossRef]
- Onaitis, M.; Ludwig, K.; Perez-Tamayo, A.; Gottfried, M.; Russell, L.; Shadduck, P.; Pappas, T.; Seigler, H.F.; Tyler, D.S. The Kraske Procedure: A Critical Analysis of a Surgical Approach for Mid-Rectal Lesions. J. Surg. Oncol. 2006, 94, 194–202. [Google Scholar] [CrossRef]
- Wei, R.; Okocha, M.; Lotfollahzadeh, S. Rectal Cancer Microsurgery. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Clancy, C.; Burke, J.P.; Albert, M.R.; O’Connell, P.R.; Winter, D.C. Transanal Endoscopic Microsurgery versus Standard Transanal Excision for the Removal of Rectal Neoplasms: A Systematic Review and Meta-Analysis. Dis. Colon. Rectum 2015, 58, 254–261. [Google Scholar] [CrossRef]
- Stipa, F.; Tierno, S.M.; Russo, G.; Burza, A. Trans-Anal Minimally Invasive Surgery (TAMIS) versus Trans-Anal Endoscopic Microsurgery (TEM): A Comparative Case-Control Matched-Pairs Analysis. Surg. Endosc. 2022, 36, 2081–2086. [Google Scholar] [CrossRef]
- Quaresima, S.; Balla, A.; Franceschilli, L.; La Torre, M.; Iafrate, C.; Shalaby, M.; Di Lorenzo, N.; Sileri, P. Transanal Minimally Invasive Surgery for Rectal Lesions. J. Soc. Laparosc. Robot. Surg. 2016, 20, e2016.00032. [Google Scholar] [CrossRef]
- Levic, K.; Bulut, O.; Hesselfeldt, P.; Bülow, S. The Outcome of Rectal Cancer after Early Salvage TME Following TEM Compared with Primary TME: A Case-Matched Study. Tech. Coloproctol. 2013, 17, 397–403. [Google Scholar] [CrossRef]
- Chaouch, M.A.; Khan, J.; Gill, T.S.; Mehrabi, A.; Reissfelder, C.; Rahberi, N.; Elhadedy, H.; Oweira, H. Early Salvage Total Mesorectal Excision (sTME) after Organ Preservation Failure in Rectal Cancer Does Not Worsen Postoperative Outcomes Compared to Primary TME: Systematic Review and Meta-Analysis. Int. J. Colorectal Dis. 2021, 36, 2375–2386. [Google Scholar] [CrossRef]
- Yamamoto, H.; Koiwai, H.; Yube, T.; Isoda, N.; Sato, Y.; Sekine, Y.; Higashizawa, T.; Utsunomiya, K.; Ido, K.; Sugano, K. A Successful Single-Step Endoscopic Resection of a 40 Millimeter Flat-Elevated Tumor in the Rectum: Endoscopic Mucosal Resection Using Sodium Hyaluronate. Gastrointest. Endosc. 1999, 50, 701–704. [Google Scholar] [CrossRef]
- Libânio, D.; Pimentel-Nunes, P.; Bastiaansen, B.; Bisschops, R.; Bourke, M.J.; Deprez, P.H.; Esposito, G.; Lemmers, A.; Leclercq, P.; Maselli, R.; et al. Endoscopic Submucosal Dissection Techniques and Technology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Review. Endoscopy 2023, 55, 361–389. [Google Scholar] [CrossRef]
- Tanaka, S.; Oka, S.; Kaneko, I.; Hirata, M.; Mouri, R.; Kanao, H.; Yoshida, S.; Chayama, K. Endoscopic Submucosal Dissection for Colorectal Neoplasia: Possibility of Standardization. Gastrointest. Endosc. 2007, 66, 100–107. [Google Scholar] [CrossRef]
- Venkat, M.; Visrodia, K. Management of Adverse Events of Submucosal Endoscopy. Gastrointest. Endosc. Clin. N. Am. 2023, 33, 183–196. [Google Scholar] [CrossRef]
- Dang, H.; Hardwick, J.C.H.; Boonstra, J.J. Endoscopic Intermuscular Dissection with Intermuscular Tunneling for Local Resection of Rectal Cancer with Deep Submucosal Invasion. VideoGIE 2022, 7, 273–277. [Google Scholar] [CrossRef]
- Tribonias, G.; Komeda, Y.; Leontidis, N.; Anagnostopoulos, G.; Palatianou, M.; Mpellou, G.; Pantoula, P.; Manola, M.-E.; Paspatis, G.; Tzouvala, M.; et al. Endoscopic Intermuscular Dissection (EID) for Removing Early Rectal Cancers and Benign Fibrotic Rectal Lesions. Tech. Coloproctol. 2023, 27, 1393–1400. [Google Scholar] [CrossRef]
- Rajan, E.; Wong Kee Song, L.M. Endoscopic Full Thickness Resection. Gastroenterology 2018, 154, 1925–1937.e2. [Google Scholar] [CrossRef]
- Schmidt, A.; Meier, B.; Caca, K. Endoscopic Full-Thickness Resection: Current Status. World J. Gastroenterol. 2015, 21, 9273–9285. [Google Scholar] [CrossRef]
- Zwager, L.W.; Mueller, J.; Stritzke, B.; Montazeri, N.S.M.; Caca, K.; Dekker, E.; Fockens, P.; Schmidt, A.; Bastiaansen, B.A.J. Dutch eFTR Working Group and German collaborating centers Adverse Events of Endoscopic Full-Thickness Resection: Results from the German and Dutch Nationwide Colorectal FTRD Registry. Gastrointest. Endosc. 2023, 97, 780–789.e4. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Yang, T.W.W.; Johnson, N.; Bell, S.; Chin, M.; Simpson, P.; Carne, P.; Farmer, C.; Skinner, S.; Warrier, S.K.; et al. Latest Evidence on the Management of Early-Stage and Locally Advanced Rectal Cancer: A Narrative Review. ANZ J. Surg. 2022, 92, 365–372. [Google Scholar] [CrossRef]
- Haggitt, R.C.; Glotzbach, R.E.; Soffer, E.E.; Wruble, L.D. Prognostic Factors in Colorectal Carcinomas Arising in Adenomas: Implications for Lesions Removed by Endoscopic Polypectomy. Gastroenterology 1985, 89, 328–336. [Google Scholar] [CrossRef]
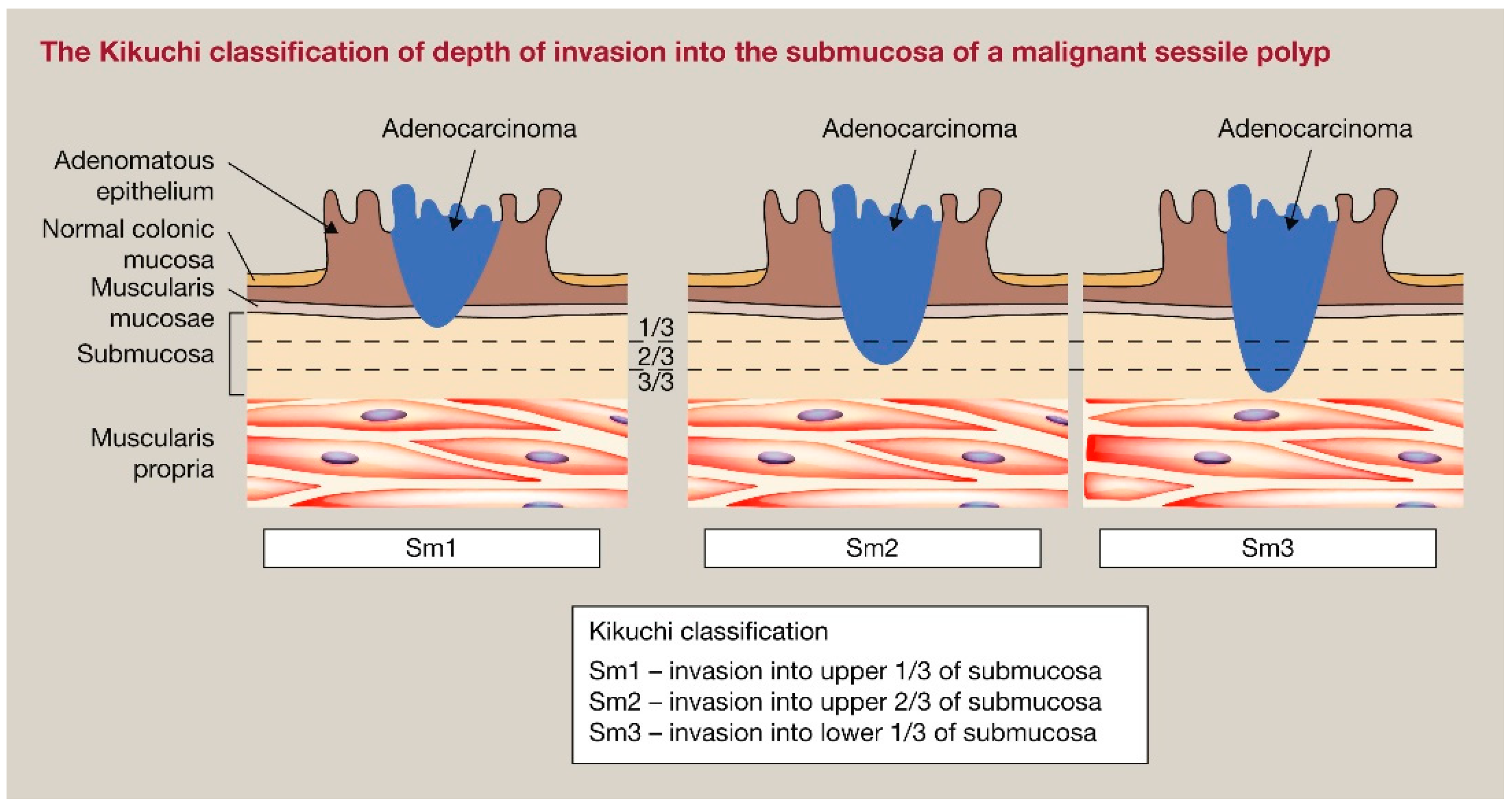
- Kikuchi, R.; Takano, M.; Takagi, K.; Fujimoto, N.; Nozaki, R.; Fujiyoshi, T.; Uchida, Y. Management of Early Invasive Colorectal Cancer. Risk of Recurrence and Clinical Guidelines. Dis. Colon. Rectum 1995, 38, 1286–1295. [Google Scholar] [CrossRef]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2019 for the Treatment of Colorectal Cancer. Int. J. Clin. Oncol. 2020, 25, 1–42. [Google Scholar] [CrossRef]
- Smits, L.J.H.; van Lieshout, A.S.; Grüter, A.A.J.; Horsthuis, K.; Tuynman, J.B. Multidisciplinary Management of Early Rectal Cancer - The Role of Surgical Local Excision in Current and Future Clinical Practice. Surg. Oncol. 2022, 40, 101687. [Google Scholar] [CrossRef]
- McKigney, N.; Coyne, P.E. Bowel Cancer Screening. Surg. Oxf. Int. Ed. 2020, 38, 18–26. [Google Scholar] [CrossRef]
- Ferlitsch, M.; Moss, A.; Hassan, C.; Bhandari, P.; Dumonceau, J.-M.; Paspatis, G.; Jover, R.; Langner, C.; Bronzwaer, M.; Nalankilli, K.; et al. Colorectal Polypectomy and Endoscopic Mucosal Resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017, 49, 270–297. [Google Scholar] [CrossRef]
- Kidane, B.; Chadi, S.A.; Kanters, S.; Colquhoun, P.H.; Ott, M.C. Local Resection Compared with Radical Resection in the Treatment of T1N0M0 Rectal Adenocarcinoma: A Systematic Review and Meta-Analysis. Dis. Colon. Rectum 2015, 58, 122–140. [Google Scholar] [CrossRef]
- Miyachi, H.; Kudo, S.-E.; Ichimasa, K.; Hisayuki, T.; Oikawa, H.; Matsudaira, S.; Kouyama, Y.; Kimura, Y.J.; Misawa, M.; Mori, Y.; et al. Management of T1 Colorectal Cancers after Endoscopic Treatment Based on the Risk Stratification of Lymph Node Metastasis. J. Gastroenterol. Hepatol. 2016, 31, 1126–1132. [Google Scholar] [CrossRef]
- Oka, S.; Tanaka, S.; Nakadoi, K.; Kanao, H.; Chayama, K. Risk Analysis of Submucosal Invasive Rectal Carcinomas for Lymph Node Metastasis to Expand Indication Criteria for Endoscopic Resection. Dig. Endosc. 2013, 25 (Suppl. S2), 21–25. [Google Scholar] [CrossRef]
- Yasue, C.; Chino, A.; Takamatsu, M.; Namikawa, K.; Ide, D.; Saito, S.; Igarashi, M.; Fujisaki, J. Pathological Risk Factors and Predictive Endoscopic Factors for Lymph Node Metastasis of T1 Colorectal Cancer: A Single-Center Study of 846 Lesions. J. Gastroenterol. 2019, 54, 708–717. [Google Scholar] [CrossRef]
- Kouyama, Y.; Kudo, S.-E.; Miyachi, H.; Ichimasa, K.; Hisayuki, T.; Oikawa, H.; Matsudaira, S.; Kimura, Y.J.; Misawa, M.; Mori, Y.; et al. Practical Problems of Measuring Depth of Submucosal Invasion in T1 Colorectal Carcinomas. Int. J. Colorectal Dis. 2016, 31, 137–146. [Google Scholar] [CrossRef]
- Stornes, T.; Wibe, A.; Nesbakken, A.; Myklebust, T.Å.; Endreseth, B.H. National Early Rectal Cancer Treatment Revisited. Dis. Colon. Rectum 2016, 59, 623–629. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Gama-Rodrigues, J.; São Julião, G.P.; Proscurshim, I.; Sabbagh, C.; Lynn, P.B.; Perez, R.O. Local Recurrence after Complete Clinical Response and Watch and Wait in Rectal Cancer after Neoadjuvant Chemoradiation: Impact of Salvage Therapy on Local Disease Control. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 822–828. [Google Scholar] [CrossRef]
- Bujko, K.; Richter, P.; Smith, F.M.; Polkowski, W.; Szczepkowski, M.; Rutkowski, A.; Dziki, A.; Pietrzak, L.; Kołodziejczyk, M.; Kuśnierz, J.; et al. Preoperative Radiotherapy and Local Excision of Rectal Cancer with Immediate Radical Re-Operation for Poor Responders: A Prospective Multicentre Study. Radiother. Oncol. 2013, 106, 198–205. [Google Scholar] [CrossRef]
- Perez, R.O.; Habr-Gama, A.; Lynn, P.B.; São Julião, G.P.; Bianchi, R.; Proscurshim, I.; Gama-Rodrigues, J. Transanal Endoscopic Microsurgery for Residual Rectal Cancer (ypT0-2) Following Neoadjuvant Chemoradiation Therapy: Another Word of Caution. Dis. Colon. Rectum 2013, 56, 6–13. [Google Scholar] [CrossRef]
- Stijns, R.C.H.; de Graaf, E.J.R.; Punt, C.J.A.; Nagtegaal, I.D.; Nuyttens, J.J.M.E.; van Meerten, E.; Tanis, P.J.; de Hingh, I.H.J.T.; van der Schelling, G.P.; Acherman, Y.; et al. Long-Term Oncological and Functional Outcomes of Chemoradiotherapy Followed by Organ-Sparing Transanal Endoscopic Microsurgery for Distal Rectal Cancer: The CARTS Study. JAMA Surg. 2019, 154, 47–54. [Google Scholar] [CrossRef]
- Lezoche, G.; Paganini, A.M.; Campagnacci, R.; Ghiselli, R.; Pelloni, M.; Rombini, A.; Guerrieri, M. Treatment of Rectal Cancer by Transanal Endoscopic Microsurgery: Review of the Literature. Minerva Chir. 2013, 68, 1–9. [Google Scholar]
- Kennecke, H.F.; O’Callaghan, C.J.; Loree, J.M.; Moloo, H.; Auer, R.; Jonker, D.J.; Raval, M.; Musselman, R.; Ma, G.; Caycedo-Marulanda, A.; et al. Neoadjuvant Chemotherapy, Excision, and Observation for Early Rectal Cancer: The Phase II NEO Trial (CCTG CO.28) Primary End Point Results. J. Clin. Oncol. 2023, 41, 233–242. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Perez, R.O.; Nadalin, W.; Sabbaga, J.; Ribeiro, U.; Silva e Sousa, A.H.; Campos, F.G.; Kiss, D.R.; Gama-Rodrigues, J. Operative versus Nonoperative Treatment for Stage 0 Distal Rectal Cancer Following Chemoradiation Therapy: Long-Term Results. Ann. Surg. 2004, 240, 711–717, discussion 717–718. [Google Scholar] [CrossRef]
- Bao, Q.R.; Ferrari, S.; Capelli, G.; Ruffolo, C.; Scarpa, M.; Agnes, A.; Chiloiro, G.; Palazzari, E.; Urso, E.D.L.; Pucciarelli, S.; et al. Rectal Sparing Approaches after Neoadjuvant Treatment for Rectal Cancer: A Systematic Review and Meta-Analysis Comparing Local Excision and Watch and Wait. Cancers 2023, 15, 465. [Google Scholar] [CrossRef] [PubMed]
- Cutting, J.E.; Hallam, S.E.; Thomas, M.G.; Messenger, D.E. A Systematic Review of Local Excision Followed by Adjuvant Therapy in Early Rectal Cancer: Are pT1 Tumours the Limit? Colorectal Dis. 2018, 20, 854–863. [Google Scholar] [CrossRef] [PubMed]
- van Oostendorp, S.E.; Smits, L.J.H.; Vroom, Y.; Detering, R.; Heymans, M.W.; Moons, L.M.G.; Tanis, P.J.; de Graaf, E.J.R.; Cunningham, C.; Denost, Q.; et al. Local Recurrence after Local Excision of Early Rectal Cancer: A Meta-Analysis of Completion TME, Adjuvant (Chemo)Radiation, or No Additional Treatment. Br. J. Surg. 2020, 107, 1719–1730. [Google Scholar] [CrossRef]
- Jeong, J.-U.; Nam, T.-K.; Kim, H.-R.; Shim, H.-J.; Kim, Y.-H.; Yoon, M.S.; Song, J.-Y.; Ahn, S.-J.; Chung, W.-K. Adjuvant Chemoradiotherapy Instead of Revision Radical Resection after Local Excision for High-Risk Early Rectal Cancer. Radiat. Oncol. 2016, 11, 114. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binda, C.; Secco, M.; Tuccillo, L.; Coluccio, C.; Liverani, E.; Jung, C.F.M.; Fabbri, C.; Gibiino, G. Early Rectal Cancer and Local Excision: A Narrative Review. J. Clin. Med. 2024, 13, 2292. https://doi.org/10.3390/jcm13082292
Binda C, Secco M, Tuccillo L, Coluccio C, Liverani E, Jung CFM, Fabbri C, Gibiino G. Early Rectal Cancer and Local Excision: A Narrative Review. Journal of Clinical Medicine. 2024; 13(8):2292. https://doi.org/10.3390/jcm13082292
Chicago/Turabian StyleBinda, Cecilia, Matteo Secco, Luigi Tuccillo, Chiara Coluccio, Elisa Liverani, Carlo Felix Maria Jung, Carlo Fabbri, and Giulia Gibiino. 2024. "Early Rectal Cancer and Local Excision: A Narrative Review" Journal of Clinical Medicine 13, no. 8: 2292. https://doi.org/10.3390/jcm13082292
APA StyleBinda, C., Secco, M., Tuccillo, L., Coluccio, C., Liverani, E., Jung, C. F. M., Fabbri, C., & Gibiino, G. (2024). Early Rectal Cancer and Local Excision: A Narrative Review. Journal of Clinical Medicine, 13(8), 2292. https://doi.org/10.3390/jcm13082292