
Management of Post-Operative Crohn’s Disease: Knowns and Unknowns

 , , , and
, , , and 
Abstract
:1. Introduction
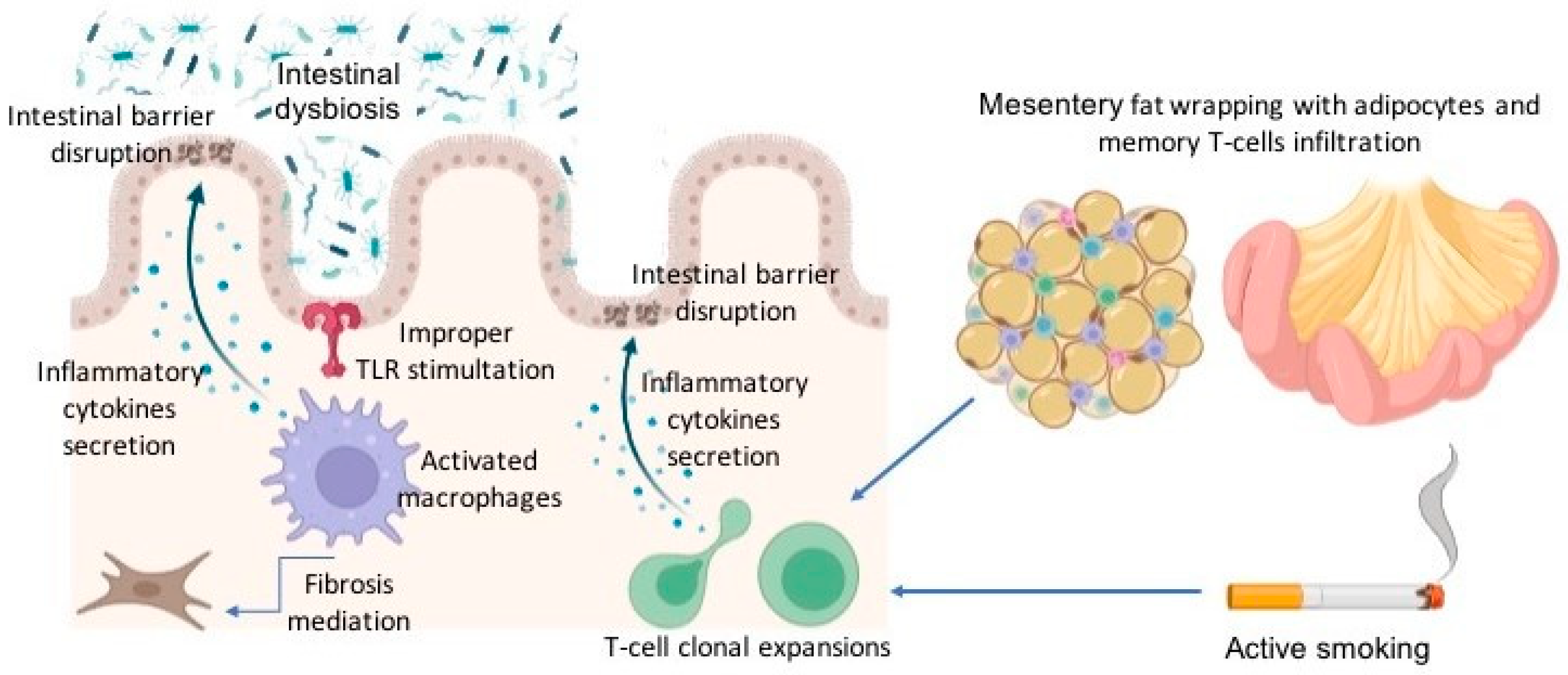
2. Pathophysiology of Post-Operative Recurrence
3. Risk Factors for POR
3.1. Smoking
3.2. Disease Characteristics
3.3. Histological Risk Factors
3.3.1. Granulomas
3.3.2. Plexitis
3.3.3. Resection Margins
3.4. Surgical Risk Factors
3.4.1. Anastomotic Techniques
3.4.2. Kono-S Anastomosis
3.4.3. Mesenteric Excision
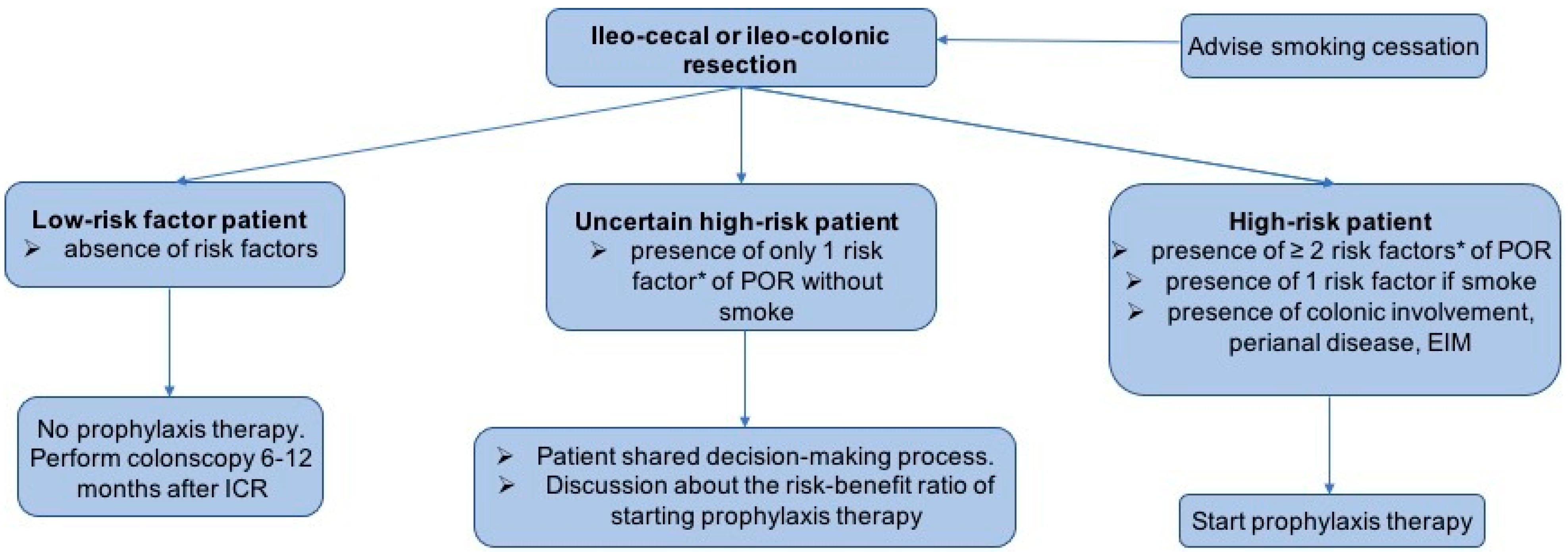
4. Strategies to Prevent POR
5. Medical Therapy to Prevent POR
5.1. Corticosteroids
5.2. Mesalazine
5.3. Antibiotics and Probiotics
5.4. Immunomodulators
5.5. Anti-TNF
5.6. Anti-TNF versus Azathioprine
5.7. Ustekinumab and Vedolizumab
5.8. The Use of Anti-TNF despite Its Use before Surgery
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Laass, M.W.; Roggenbuck, D.; Conrad, K. Diagnosis and Classification of Crohn’s Disease. Autoimmun. Rev. 2014, 13, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N. Epidemiology and Risk Factors for IBD. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef] [PubMed]
- Roda, G.; Chien Ng, S.; Kotze, P.G.; Argollo, M.; Panaccione, R.; Spinelli, A.; Kaser, A.; Peyrin-Biroulet, L.; Danese, S. Crohn’s Disease. Nat. Rev. Dis. Primers 2020, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Tsai, L.; Ma, C.; Dulai, P.S.; Prokop, L.J.; Eisenstein, S.; Ramamoorthy, S.L.; Feagan, B.G.; Jairath, V.; Sandborn, W.J.; Singh, S. Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn’s Disease: A Meta-Analysis of Population-Based Cohorts. Clin. Gastroenterol. Hepatol. 2021, 19, 2031–2045.E11. [Google Scholar] [CrossRef]
- Meima-van Praag, E.M.; Buskens, C.J.; Hompes, R.; Bemelman, W.A. Surgical Management of Crohn’s Disease: A State of the Art Review. Int. J. Color. Dis. 2021, 36, 1133–1145. [Google Scholar] [CrossRef]
- Lee, K.E.; Cantrell, S.; Shen, B.; Faye, A.S. Post-Operative Prevention and Monitoring of Crohn’s Disease Recurrence. Gastroenterol. Rep. 2022, 10, Goac070. [Google Scholar] [CrossRef]
- Petagna, L.; Antonelli, A.; Ganini, C.; Bellato, V.; Campanelli, M.; Divizia, A.; Efrati, C.; Franceschilli, M.; Guida, A.M.; Ingallinella, S.; et al. Pathophysiology of Crohn’s Disease Inflammation and Recurrence. Biol. Direct. 2020, 15, 23. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Parian, A.M.; Shah, N.D.; Colombel, J.F. Short Bowel Syndrome and Intestinal Failure in Crohn’s Disease. Inflamm. Bowel Dis. 2016, 22, 1209–1218. [Google Scholar] [CrossRef]
- Ferrante, M.; Pouillon, L.; Mañosa, M.; Savarino, E.; Allez, M.; Kapizioni, C.; Arebi, N.; Carvello, M.; Myrelid, P.; De Vries, A.C.; et al. Results of the Eighth Scientific Workshop of ECCO: Prevention and Treatment of Postoperative Recurrence in Patients with Crohn’s Disease Undergoing an Ileocolonic Resection with Ileocolonic Anastomosis. J. Crohn’s Colitis 2023, 17, 1707–1722. [Google Scholar] [CrossRef] [PubMed]
- Gionchetti, P.; Dignass, A.; Danese, S.; Magro Dias, F.J.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. ECCO. 3rd European Evidence-Based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 2: Surgical Management and Special Situation. J. Crohn’s Colitis 2017, 11, 135–149. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Loftus, E.V., Jr.; Hirano, I.; Falck-Ytter, Y.; Singh, S.; Sultan, S.; AGA Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease after Surgical Resection. Gastroenterology 2017, 152, 271–275. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology Consensus Guidelines on the Management of Inflammatory Bowel Disease in Adults. Gut 2019, 68, S1–S106. [Google Scholar] [CrossRef] [PubMed]
- Vuitton, L.; Peyrin-Biroulet, L. Pharmacological Prevention of Postoperative Recurrence in Crohn’s Disease. Drugs 2020, 80, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Sensi, B.; Siragusa, L.; Efrati, C.; Petagna, L.; Franceschilli, M.; Bellato, V.; Antonelli, A.; Arcudi, C.; Campanelli, M.; Ingallinella, S.; et al. The Role of Inflammation in Crohn’s Disease Recurrence after Surgical Treatment. J. Immunol. Res. 2020, 2020, 8846982. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Bislenghi, G.; Hammoudi, N.; Verstockt, B.; Brown, S.; Oliveira-Cunha, M.; Bemelman, W.; Pellino, G.; Kotze, P.G.; 8th Scientific Workshop of the European Crohn’s and Colitis Organisation; et al. Results of the Eighth Scientific Workshop of ECCO: Pathophysiology and Risk Factors of Postoperative Crohn’s Disease Recurrence after an Ileocolonic Resection. J. Crohn’s Colitis 2023, 17, 1557–1568. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.R.; Geboes, K.; Peeters, M.; Baert, F.; Penninckx, F.; Rutgeerts, P. Early Lesions of Recurrent Crohn’s Disease Caused by Infusion of Intestinal Contents in Excluded Ileum. Gastroenterology 1998, 114, 262–267. [Google Scholar] [CrossRef]
- Sokol, H.; Brot, L.; Stefanescu, C.; Auzolle, C.; Barnich, N.; Buisson, A.; Fumery, M.; Pariente, B.; Le Bourhis, L.; Treton, X.; et al. Prominence of Ileal Mucosa-Associated Microbiota to Predict Postoperative Endoscopic Recurrence in Crohn’s Disease. Gut 2020, 69, 462–472. [Google Scholar] [CrossRef]
- Dang, J.T.; Dang, T.T.; Wine, E.; Dicken, B.; Madsen, K.; Laffin, M. The Genetics of Postoperative Recurrence in Crohn Disease: A Systematic Review, Meta-Analysis, and Framework for Future Work. Crohns Colitis 360 2021, 3, Otaa094. [Google Scholar] [CrossRef]
- Lissner, D.; Schumann, M.; Batraetal, A. MonocyteandM1 Macrophage-Induced Barrier Defect Contributes to Chronic Intestinal Inflammation in IBD. Inflamm. Bowel Dis. 2015, 21, 1–1305. [Google Scholar] [CrossRef] [PubMed]
- Salvador, P.; Macías-Ceja, D.C.; Gisbert-Ferrándiz, L.; Hernández, C.; Bernardo, D.; Alós, R.; Navarro-Vicente, F.; Esplugues, J.V.; Ortiz-Masiá, D.; Barrachina, M.D.; et al. CD16+ Macrophages Mediate Fibrosis in Inflammatory Bowel Disease. J. Crohn’s Colitis 2018, 12, 589–599. [Google Scholar] [CrossRef]
- Zorzi, F.; Monteleone, I.; Sarra, M.; Calabrese, E.; Marafini, I.; Cretella, M.; Sedda, S.; Biancone, L.; Pallone, F.; Monteleone, G. Distinct Profiles of Effector Cytokines Mark the Different Phases of Crohn’s Disease. PLoS ONE 2013, 8, e54562. [Google Scholar] [CrossRef] [PubMed]
- Allez, M.; Auzolle, C.; Ngollo, M.; Bottois, H.; Chardiny, V.; Corraliza, A.M.; Salas, A.; Perez, K.; Stefanescu, C.; Nancey, S.; et al. T Cell Clonal Expansions in Ileal Crohn’s Disease Are Associated with Smoking Behaviour and Postoperative Recurrence. Gut 2019, 68, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Coffey, C.J.; Kiernan, M.G.; Sahebally, S.M.; Jarrar, A.; Burke, J.P.; Kiely, P.A.; Shen, B.; Waldron, D.; Peirce, C.; Moloney, M.; et al. Inclusion of the Mesentery in Ileocolic Resection for Crohn’s Disease Is Associated With Reduced Surgical Recurrence. J. Crohn’s Colitis 2018, 12, 1139–1150. [Google Scholar] [CrossRef]
- Zhu, Y.; Qian, W.; Huang, L.; Xu, Y.; Guo, Z.; Cao, L.; Gong, J.; Coffey, J.C.; Shen, B.; Li, Y.; et al. Role of Extended Mesenteric Excision in Postoperative Recurrence of Crohn’s Colitis: A Single-Center Study. Clin. Transl. Gastroenterol. 2021, 12, e00407. [Google Scholar] [CrossRef] [PubMed]
- Mineccia, M.; Maconi, G.; Daperno, M.; Cigognini, M.; Cherubini, V.; Colombo, F.; Perotti, S.; Baldi, C.; Massucco, P.; Ardizzone, S.; et al. Has the Removing of the Mesentery during Ileo-Colic Resection an Impact on Post-Operative Complications and Recurrence in Crohn’s Disease? Results from the Resection of the Mesentery Study (Remedy). J. Clin. Med. 2022, 11, 1961. [Google Scholar] [CrossRef]
- Pellino, G.; Keller, D.S.; Sampietro, G.M.; Angriman, I.; Carvello, M.; Celentano, V.; Colombo, F.; Di Candido, F.; Laureti, S.; Luglio, G. Inflammatory Bowel Disease Position Statement of the Italian Society of Colorectal Surgery (SICCR): Crohn’s Disease. Tech. Coloproctol. 2020, 24, 421–448. [Google Scholar] [CrossRef]
- Joustra, V.; Duijvestein, M.; Mookhoek, A.; Bemelman, W.; Buskens, C.; Koželj, M.; Novak, G.; Hindryckx, P.; Mostafavi, N.; D’Haens, G. Natural History and Risk Stratification of Recurrent Crohn’s Disease After Ileocolonic Resection: A Multicenter Retrospective Cohort Study. Inflamm. Bowel Dis. 2022, 28, 1–8. [Google Scholar] [CrossRef]
- Auzolle, C.; Nancey, S.; Tran-Minh, M.L.; Buisson, A.; Pariente, B.; Stefanescu, C.; Fumery, M.; Marteau, P.; Treton, X.; Hammoudi, N.; et al. Male Gender, Active Smoking and Previous Intestinal Resection Are Risk Factors for Post-Operative Endoscopic Recurrence in Crohn‘s Disease: Results from a Prospective Cohort Study. Aliment. Pharmacol. Ther. 2018, 48, 924–932. [Google Scholar] [CrossRef]
- Rocha, C.H.; Walshe, M.; Birch, S.; Sabic, K.; Korie, U.; Chasteau, C.; Miladinova, V.M.; Sabol, W.B.; Mengesha, E.; Hanna, M.; et al. Clinical Predictors of Early and Late Endoscopic Recurrence Following Ileocolonic Resection in Crohn’s Disease. J. Crohn’s Colitis 2023, online ahead of print. [Google Scholar]
- De Cruz, P.; Kamm, M.A.; Hamilton, A.L.; Ritchie, K.J.; Krejany, E.O.; Gorelik, A.; Liew, D.; Prideaux, L.; Lawrance, I.C.; Andrews, J.M.; et al. Crohn’s Disease Management after Intestinal Resection: A Randomised Trial. Lancet 2015, 385, 1406–1417. [Google Scholar] [CrossRef] [PubMed]
- Reese, G.E.; Nanidis, T.; Borysiewicz, C.; Yamamoto, T.; Orchard, T.; Tekkis, P.P. The Effect of Smoking after Surgery for Crohn’s Disease: A Meta-Analysis of Observational Studies. Int. J. Color. Dis. 2008, 23, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Cottone, M.; Orlando, A.; Viscido, A.; Calabrese, E.; Cammà, C.; Casà, A. Review Article: Prevention of Postsurgical Relapse and Recurrence in Crohn’s Disease. Aliment. Pharmacol. Ther. 2003, 17 (Suppl. S2), 38–42. [Google Scholar] [CrossRef] [PubMed]
- To, N.; Gracie, D.J.; Ford, A.C. Systematic Review with Meta-Analysis: The Adverse Effects of Tobacco Smoking on the Natural History of Crohn’s Disease. Aliment. Pharmacol. Ther. 2016, 43, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Kane, S.V.; Flicker, M.; Katz-Nelson, F. Tobacco Use Is Associated with Accelerated Clinical Recurrence of Crohn’s Disease after Surgically Induced Remission. J. Clin. Gastroenterol. 2005, 39, 32–35. [Google Scholar] [PubMed]
- Lindberg, E.; Järnerot, G.; Huitfeldt, B. Smoking in Crohn’s Disease: Effect on Localisation and Clinical Course. Gut 1992, 33, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Keighley, M.R. The Association of Cigarette Smoking with a High Risk of Recurrence after Ileocolonic Resection for Ileocecal Crohn’s Disease. Surg. Today 1999, 29, 579–580. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, L.R.; Ramcharan, S.; Bryant, H.; Fick, G. Effect of Cigarette Smoking on Recurrence of Crohn’s Disease. Gastroenterology 1990, 98, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Ryan, W.R.; Allan, R.N.; Yamamoto, T.; Keighley, M.R. Crohn’s Disease Patients Who Quit Smoking Have a Reduced Risk of Reoperation for Recurrence. Am. J. Surg. 2004, 187, 219–225. [Google Scholar] [CrossRef]
- Bolckmans, R.; Kalman, T.; Singh, S.; Ratnatunga, K.C.; Myrelid, P.; Travis, S.; George, B.D. Does Smoking Cessation Reduce Surgical Recurrence After Primary Ileocolic Resection for Crohn’s Disease? Dis. Colon Rectum. 2020, 63, 200–206. [Google Scholar] [CrossRef]
- McLeod, R.S.; Wolff, B.G.; Ross, S.; Parkes, R.; McKenzie, M. Investigators of the CAST Trial. Recurrence of Crohn’s Disease after Ileocolic Resection Is Not Affected by Anastomotic Type: Results of a Multicenter, Randomized, Controlled Trial. Dis. Colon Rectum. 2009, 52, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, I.; Kulle, C.B.; Buyuk, M.; Ormeci, A.; Akyuz, F.; Balik, E.; Bulut, T.; Keskin, M. What Are the Predictors for Recurrence of Crohn’s Disease after Surgery? Medicine 2021, 100, E25340. [Google Scholar] [CrossRef] [PubMed]
- Beelen, E.M.J.; Nieboer, D.; Arkenbosch, J.H.C.; Regueiro, M.D.; Satsangi, J.; Ardizzone, S.; López-Sanromán, A.; Savarino, E.; Armuzzi, A.; Janneke van der Woude, C.; et al. Risk Prediction and Comparative Efficacy of Anti-TNF vs Thiopurines, for Preventing Postoperative Recurrence in Crohn’s Disease: A Pooled Analysis of 6 Trials. Clin. Gastroenterol. Hepatol. 2022, 20, 2741–2752.e6. [Google Scholar] [CrossRef] [PubMed]
- De Barcelos, I.F.; Kotze, P.G.; Spinelli, A.; Suzuki, Y.; Teixeira, F.V.; de Albuquerque, I.C.; Saad-Hossne, R.; da Silva Kotze, L.M.; Yamamoto, T. Factors Affecting the Incidence of Early Endoscopic Recurrence after Ileocolonic Resection for Crohn’s Disease: A Multicentre Observational Study. Color. Dis. 2017, 19, O39–O45. [Google Scholar] [CrossRef] [PubMed]
- Maggiori, L.; Brouquet, A.; Zerbib, P.; Lefevre, J.H.; Denost, Q.; Germain, A.; Cotte, E.; Beyer-Berjot, L.; Munoz-Bongrand, N.; Desfourneaux, V.; et al. Penetrating Crohn Disease Is Not Associated With a Higher Risk of Recurrence After Surgery: A Prospective Nationwide Cohort Conducted by the Getaid Chirurgie Group. Ann. Surg. 2019, 270, 827–834. [Google Scholar] [CrossRef]
- Sun, X.; Yuan, L.; Li, Y.; Shen, B.; Xie, H.; Liu, X. Association of Granulomas in Mesenteric Lymph Nodes in Crohn’s Disease with Younger Age and Transmural Inflammation. J. Gastroenterol. Hepatol. 2017, 32, 1463–1468. [Google Scholar] [CrossRef]
- Valibouze, C.; Desreumaux, P.; Zerbib, P. Post-Surgical Recurrence of Crohn’s Disease: Situational Analysis and Future Prospects. J. Visc. Surg. 2021, 158, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Jacovides, M.; Reese, G.E.; Yamamoto, T.; Tekkis, P.P. Meta-Analysis of the Role of Granulomas in the Recurrence of Crohn Disease. Dis. Colon Rectum. 2010, 53, 177–185. [Google Scholar] [CrossRef]
- Tandon, P.; Malhi, G.; Abdali, D.; Pogue, E.; Marshall, J.K.; de Buck van Overstraeten, A.; Riddell, R.; Narula, N. Active Margins, Plexitis, and Granulomas Increase Postoperative Crohn’s Recurrence: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 451–462. [Google Scholar] [CrossRef]
- Li, Y.; Stocchi, L.; Liu, X.; Rui, Y.; Liu, G.; Remzi, F.H.; Shen, B. Presence of Granulomas in Mesenteric Lymph Nodes Is Associated with Postoperative Recurrence in Crohn’s Disease. Inflamm. Bowel Dis. 2015, 21, 2613–2618. [Google Scholar] [CrossRef]
- Unger, L.W.; Argeny, S.; Stift, A.; Yang, Y.; Karall, A.; Freilinger, T.; Müller, C.; Bergmann, M.; Stift, J.; Riss, S. Mesenteric Granulomas Independently Predict Long-Term Risk of Surgical Recurrence in Crohn’s Disease. Color. Dis. 2020, 22, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.; de Hertogh, G.; Hlavaty, T.; D’Haens, G.; Penninckx, F.; D’Hoore, A.; Vermeire, S.; Rutgeerts, P.; Geboes, K.; van Assche, G. The Value of Myenteric Plexitis to Predict Early Postoperative Crohn’s Disease Recurrence. Gastroenterology 2006, 130, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- Misteli, H.; Koh, C.E.; Wang, L.M.; Mortensen, N.J.; George, B.; Guy, R. Myenteric Plexitis at the Proximal Resection Margin Is a Predictive Marker for Surgical Recurrence of Ileocaecal Crohn’s Disease. Color. Dis. 2015, 17, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Decousus, S.; Boucher, A.L.; Joubert, J.; Pereira, B.; Dubois, A.; Goutorbe, F.; Déchelotte, P.J.; Bommelaer, G.; Buisson, A. Myenteric Plexitis Is a Risk Factor for Endoscopic and Clinical Postoperative Recurrence after Ileocolonic Resection in Crohn’s Disease. Dig. Liver Dis. 2016, 48, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Sokol, H.; Polin, V.; Lavergne-Slove, A.; Panis, Y.; Treton, X.; Dray, X.; Bouhnik, Y.; Valleur, P.; Marteau, P. Plexitis as a Predictive Factor of Early Postoperative Clinical Recurrence in Crohn’s Disease. Gut 2009, 58, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Bressenot, A.; Chevaux, J.B.; Williet, N.; Oussalah, A.; Germain, A.; Gauchotte, G.; Wissler, M.P.; Vignaud, J.M.; Bresler, L.; Bigard, M.A.; et al. Submucosal Plexitis as a Predictor of Postoperative Surgical Recurrence in Crohn’s Disease. Inflamm. Bowel Dis. 2013, 19, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, B.; de Buck van Overstraeten, A.; Arijs, I.; Sagaert, X.; Van Assche, G.; Vermeire, S.; Tertychnyy, A.; Geboes, K.; Wolthuis, A.; D’Hoore, A.; et al. Submucosal Plexitis as a Predictive Factor for Postoperative Endoscopic Recurrence in Patients with Crohn’s Disease Undergoing a Resection with Ileocolonic Anastomosis: Results from a Prospective Single-Centre Study. J. Crohn’s Colitis 2017, 11, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Kellow, J.E. Myenteric Plexitis in Enteric Dysmotility: What Are the Implications for Clinical Practice? Gut 2009, 58, 1042–1043. [Google Scholar] [CrossRef] [PubMed]
- Bassotti, G.; Villanacci, V.; Nascimbeni, R.; Antonelli, E.; Cadei, M.; Manenti, S.; Lorenzi, L.; Titi, A.; Salerni, B. The Role of Colonic Mast Cells and Myenteric Plexitis in Patients with Diverticular Disease. Int. J. Color. Dis. 2013, 28, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Fazio, V.W.; Marchetti, F.; Church, M.; Goldblum, J.R.; Lavery, C.; Hull, T.L.; Milsom, J.W.; Strong, S.A.; Oakley, J.R.; Secic, M. Effect of Resection Margins on the Recurrence of Crohn’s Disease in the Small Bowel. A Randomized Controlled Trial. Ann. Surg. 1996, 224, 563–573. [Google Scholar] [CrossRef]
- Ryan, J.M.; Rogers, A.C.; O’Toole, A.; Burke, J.P. Meta-Analysis of Histological Margin Positivity in the Prediction of Recurrence After Crohn’s Resection. Dis. Colon Rectum. 2019, 62, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Poredska, K.; Kunovsky, L.; Marek, F.; Kala, Z.; Prochazka, V.; Dolina, J.; Zboril, V.; Kovalcikova, P.; Pavlik, T.; Jabandziev, P.; et al. The Influence of Microscopic Inflammation at Resection Margins on Early Postoperative Endoscopic Recurrence After Ileocaecal Resection for Crohn’s Disease. J. Crohn’s Colitis 2020, 14, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Hammoudi, N.; Cazals-Hatem, D.; Auzolle, C.; Gardair, C.; Ngollo, M.; Bottois, H.; Nancey, S.; Pariente, B.; Buisson, A.; Treton, X.; et al. Association Between Microscopic Lesions at Ileal Resection Margin and Recurrence After Surgery in Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 141–149.E2. [Google Scholar] [CrossRef]
- Wasmann, K.A.T.G.M.; van Amesfoort, J.; van Montfoort, M.L.; Koens, L.; Bemelman, W.A.; Buskens, C.J. The Predictive Value of Inflammation at Ileocecal Resection Margins for Postoperative Crohn’s Recurrence: A Cohort Study. Inflamm. Bowel Dis. 2020, 26, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Kotze, P.G.; Yamamoto, T. Microscopic Inflammation at Ileocaecal Resection Margins in Crohn’s Disease: Prevent Recurrence or Treat Residual Disease? J. Crohn’s Colitis 2020, 14, 872–873. [Google Scholar] [CrossRef] [PubMed]
- Arkenbosch, J.H.C.; Beelen, E.M.J.; Dijkstra, G.; Romberg-Camps, M.; Duijvestein, M.; Hoentjen, F.; van der Marel, S.; Maljaars, P.W.J.; Jansen, S.; de Boer, N.K.H.; et al. Prophylactic Medication for the Prevention of Endoscopic Recurrence in Crohn’s Disease: A Prospective Study Based on Clinical Risk Stratification. J. Crohn’s Colitis 2023, 17, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.L.; Hamilton, S.R.; Coleman, J.; Sitzmann, J.V.; Bayless, T.M. Patterns of Ileal Recurrence in Crohn’s Disease. A Prospective Randomized Study. Ann. Surg. 1992, 215, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Kusunoki, M.; Ikeuchi, H.; Yanagi, H.; Shoji, Y.; Yamamura, T. A Comparison of Stapled and Hand-Sewn Anastomoses in Crohn’s Disease. Dig. Surg. 1998, 15, 679–682. [Google Scholar] [CrossRef]
- Hashemi, M.; Novell, J.R.; Lewis, A.A. Side-to-Side Stapled Anastomosis May Delay Recurrence in Crohn’s Disease. Dis. Colon Rectum. 1998, 41, 1293–1296. [Google Scholar] [CrossRef]
- Yamamoto, T.; Bain, I.M.; Mylonakis, E.; Allan, R.N.; Keighley, M.R. Stapled Functional End-to-End Anastomosis versus Sutured End-to-End Anastomosis after Ileocolonic Resection in Crohn Disease. Scand. J. Gastroenterol. 1999, 34, 708–713. [Google Scholar]
- Muñoz-Juárez, M.; Yamamoto, T.; Wolff, B.G.; Keighley, M.R. Wide-Lumen Stapled Anastomosis vs. Conventional End-to-End Anastomosis in the Treatment of Crohn’s Disease. Dis. Colon Rectum. 2001, 44, 20–26. [Google Scholar] [CrossRef]
- Caprilli, R.; Corrao, G.; Taddei, G.; Tonelli, F.; Torchio, P.; Viscido, A. Prognostic Factors for Postoperative Recurrence of Crohn’s Disease. Dis. Colon Rectum. 1996, 39, 335–341. [Google Scholar] [CrossRef]
- Guo, Z.; Li, Y.; Zhu, W.; Gong, J.; Li, N.; Li, J. Comparing Outcomes between Side-to-Side Anastomosis and Other Anastomotic Configurations after Intestinal Resection for Patients with Crohn’s Disease: A Meta-Analysis. World J. Surg. 2013, 37, 893–901. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Chen, Z.; Huang, J.; Lian, L.; Rouniyar, S.; Wu, X.; Lan, P. Stapled Side-to-Side Anastomosis Might Be Better than Handsewn End-to-End Anastomosis in Ileocolic Resection for Crohn’s Disease: A Meta-Analysis. Dig. Dis. Sci. 2014, 59, 1544–1551. [Google Scholar] [CrossRef]
- Feng, J.S.; Li, J.Y.; Yang, Z.; Chen, X.Y.; Mo, J.J.; Li, S.H. Stapled Side-to-Side Anastomosis Might Be Benefit in Intestinal Resection for Crohn’s Disease: A Systematic Review and Network Meta-Analysis. Medicine 2018, 97, E0315. [Google Scholar] [CrossRef] [PubMed]
- Haanappel, A.E.G.; Bellato, V.; Buskens, C.J.; Armuzzi, A.; van der Bilt, J.D.W.; de Boer, N.K.H.; Danese, S.; van der Does de Willebois, E.M.L.; Duijvestein, M.; van der Horst, D.; et al. Optimising Surgical Anastomosis in Ileocolic Resection for Crohn’s Disease with Respect to Recurrence and Functionality: Two International Parallel Randomized Controlled Trials Comparing Handsewn (END-to-End or Kono-S) to Stapled Anastomosis (HAND2END and the End2End STUDIES). BMC Surg. 2024, 24, 71. [Google Scholar]
- Kono, T.; Ashida, T.; Ebisawa, Y.; Chisato, N.; Okamoto, K.; Katsuno, H.; Maeda, K.; Fujiya, M.; Kohgo, Y.; Furukawa, H. A New Antimesenteric Functional End-to-End Handsewn Anastomosis: Surgical Prevention of Anastomotic Recurrence in Crohn’s Disease. Dis. Colon Rectum. 2011, 54, 586–592. [Google Scholar] [CrossRef]
- Luglio, G.; Rispo, A.; Imperatore, N.; Giglio, M.C.; Amendola, A.; Tropeano, F.P.; Peltrini, R.; Castiglione, F.; De Palma, G.D.; Bucci, L. Surgical Prevention of Anastomotic Recurrence by Excluding Mesentery in Crohn’s Disease: The SuPREMe-CD Study—A Randomized Clinical Trial. Ann. Surg. 2020, 272, 210–217. [Google Scholar] [CrossRef]
- Alshantti, A.; Hind, D.; Hancock, L.; Brown, S.R. The Role of Kono-S Anastomosis and Mesenteric Resection in Reducing Recurrence after Surgery for Crohn’s Disease: A Systematic Review. Color. Dis. 2021, 23, 7–17. [Google Scholar] [CrossRef]
- Ng, C.H.; Chin, Y.H.; Lin, S.Y.; Koh, J.W.H.; Lieske, B.; Koh, F.H.; Chong, C.S.; Foo, F.J. Kono-S Anastomosis for Crohn’s Disease: A Systemic Review, Meta-Analysis, and Meta-Regression. Surg. Today 2021, 51, 493–501. [Google Scholar] [CrossRef]
- Trencheva, K.; Spinelli, A.; Kienle, P.; D’Hoore, A.; Luglio, G.; Flemming, S.; Scaringi, S.; Tropeano, F.; Christos, P.; Michelassi, F. OP20 Postoperative Endoscopic Recurrence after Resection of Crohn’s Terminal Ileitis with Kono-S or Side-to-Side Functional End Anastomosis: Results of a Multicenter Prospective Randomized Trial. J. Crohn’s Colitis 2024, 18 (Suppl. S1), I37. [Google Scholar]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Beyls, J.; Kerremans, R.; Hiele, M. Predictability of the Postoperative Course of Crohn’s Disease. Gastroenterology 1990, 99, 956–963. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, J.R.; Bossuyt, P.; Ferrante, M.; West, R.L.; Dijkstra, G.; Witteman, B.J.; Wildenberg, M.; Hoentjen, F.; Franchimont, D.; Clasquin, E.; et al. High-Dose Vitamin D Does Not Prevent Postoperative Recurrence of Crohn’s Disease in a Randomized Placebo-Controlled Trial. Clin. Gastroenterol. Hepatol. 2021, 19, 1573–1582.E5. [Google Scholar] [CrossRef] [PubMed]
- Joustra, V.; van Sabben, J.; van Der Does de Willebois, E.; Duijvestein, M.; de Boer, N.; Jansen, J.; van der Bilt, J.; Lameris, W.; Bemelman, W.; Buskens, C.; et al. Benefit of Risk-Stratified Prophylactic Treatment on Clinical Outcome in Postoperative Crohn’s Disease. J. Crohn’s Colitis 2023, 17, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Dragoni, G.; Castiglione, F.; Bezzio, C.; Pugliese, D.; Spagnuolo, R.; Viola, A.; Cocomazzi, F.; Aratari, A.; Savarino, E.V.; Balestrieri, P.; et al. Comparison of Two Strategies for the Management of Postoperative Recurrence in Crohn’s Disease Patients with One Clinical Risk Factor: A Multicentre IG-IBD Study. United Eur. Gastroenterol. J. 2023, 11, 271–281. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, F.; Tasopoulou, O.; Fiorino, G.; Zilli, A.; Furfaro, F.; Allocca, M.; Sileri, P.; Spinelli, A.; Peyrin-Biroulet, L.; Danese, S. Early Biological Therapy in Operated Crohn’s Disease Patients Is Associated With a Lower Rate of Endoscopic Recurrence and Improved Long-Term Outcomes: A Single-Center Experience. Inflamm. Bowel Dis. 2023, 29, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Geldof, J.; Truyens, M.; Hanssens, M.; Van Gucht, E.; Holvoet, T.; Elorza, A.; Bouillon, V.; Barros, S.; Martins, V.; Argyriou, K.; et al. Prophylactic versus Endoscopy-Driven Treatment of Crohn’s Postoperative Recurrence: A Retrospective, Multicentric European Study (PORCSE Study). J. Crohn’s Colitis 2024, online ahead of print. [Google Scholar]
- Ewe, K.; Böttger, T.; Buhr, H.J.; Ecker, K.W.; Otto, H.F. Low-Dose Budesonide Treatment for Prevention of Postoperative Recurrence of Crohn’s Disease: A Multicentre Randomized Placebo-Controlled Trial. German Budesonide Study Group. Eur. J. Gastroenterol. Hepatol. 1999, 11, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Hellers, G.; Cortot, A.; Jewell, D.; Leijonmarck, C.E.; Löfberg, R.; Malchow, H.; Nilsson, L.G.; Pallone, F.; Pena, S.; Persson, T.; et al. Oral Budesonide for Prevention of Postsurgical Recurrence in Crohn’s Disease. The IOIBD Budesonide Study Group. Gastroenterology 1999, 116, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Hiele, M.; Geboes, K.; Peeters, M.; Penninckx, F.; Aerts, R.; Kerremans, R. Controlled Trial of Metronidazole Treatment for Prevention of Crohn’s Recurrence after Ileal Resection. Gastroenterology 1995, 108, 1617–1621. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Van Assche, G.; Vermeire, S.; D’Haens, G.; Baert, F.; Noman, M.; Aerden, I.; De Hertogh, G.; Geboes, K.; Hiele, M.; et al. Ornidazole for Prophylaxis of Postoperative Crohn’s Disease Recurrence: A Randomized, Double-Blind, Placebo-Controlled Trial. Gastroenterology 2005, 128, 856–861. [Google Scholar] [CrossRef]
- Herfarth, H.H.; Katz, J.A.; Hanauer, S.B.; Sandborn, W.J.; Loftus, E.V., Jr.; Sands, B.E.; Galanko, J.A.; Walkup, D.; Isaacs, K.L.; Martin, C.F.; et al. Ciprofloxacin for the prevention of postop Ciprofloxacin for the Prevention of Postoperative Recurrence in Patients with Crohn’s Disease: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Inflamm. Bowel Dis. 2013, 19, 1073–1079. [Google Scholar] [CrossRef]
- Florent, C.; Cortot, A.; Quandale, P.; Sahmound, T.; Modigliani, R.; Sarfaty, E.; Valleur, P.; Dupas, J.L.; Daurat, M.; Faucheron, J.L.; et al. Placebo-Controlled Clinical Trial of Mesalazine in the Prevention of Early Endoscopic Recurrences after Resection for Crohn’s Disease. Groupe d’Etudes Thérapeutiques Des Affections Inflammatoires Digestives (GETAID). Eur. J. Gastroenterol. Hepatol. 1996, 8, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Hanauer, S.B.; Korelitz, B.I.; Rutgeerts, P.; Peppercorn, M.A.; Thisted, R.A.; Cohen, R.D.; Present, D.H. Postoperative Maintenance of Crohn’s Disease Remission with 6-Mercaptopurine, Mesalamine, or Placebo: A 2-Year Trial. Gastroenterology 2004, 127, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Lochs, H.; Mayer, M.; Fleig, W.E.; Mortensen, P.B.; Bauer, P.; Genser, D.; Petritsch, W.; Raithel, M.; Hoffmann, R.; Gross, V.; et al. Prophylaxis of Postoperative Relapse in Crohn’s Disease with Mesalamine: European Cooperative Crohn’s Disease Study, V.I. Gastroenterology 2000, 118, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Caprilli, R.; Cottone, M.; Tonelli, F.; Sturniolo, G.; Castiglione, F.; Annese, V.; Papi, C.; Viscido, A.; Cammà, C.; Corrao, G.; et al. Two Mesalazine Regimens in the Prevention of the Post-Operative Recurrence of Crohn’s Disease: A Pragmatic, Double-Blind, Randomized Controlled Trial. Aliment. Pharmacol. Ther. 2003, 17, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Gjuladin-Hellon, T.; Gordon, M.; Iheozor-Ejiofor, Z.; Akobeng, A.K. Oral 5-Aminosalicylic Acid for Maintenance of Surgically-Induced Remission in Crohn’s Disease. Cochrane Database Syst. Rev. 2019, 6, CD008414. [Google Scholar] [CrossRef] [PubMed]
- Mowat, C.; Arnott, I.; Cahill, A.; Smith, M.; Ahmad, T.; Subramanian, S.; Travis, S.; Morris, J.; Hamlin, J.; Dhar, A.; et al. Mercaptopurine versus Placebo to Prevent Recurrence of Crohn’s Disease after Surgical Resection (TOPPIC): A Multicentre, Double-Blind, Randomised Controlled Trial. Lancet Gastroenterol. Hepatol. 2016, 1, 273–282. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.R.; Vermeire, S.; Van Assche, G.; Noman, M.; Aerden, I.; Van Olmen, G.; Rutgeerts, P. Therapy of Metronidazole with Azathioprine to Prevent Postoperative Recurrence of Crohn’s Disease: A Controlled Randomized Trial. Gastroenterology 2008, 135, 1123–1129. [Google Scholar] [CrossRef]
- Mañosa, M.; Cabré, E.; Bernal, I.; Esteve, M.; Garcia-Planella, E.; Ricart, E.; Peñalva, M.; Cortes, X.; Boix, J.; Piñol, M.; et al. Addition of Metronidazole to Azathioprine for the Prevention of Postoperative Recurrence of Crohn’s Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. Inflamm. Bowel Dis. 2013, 19, 1889–1895. [Google Scholar] [CrossRef]
- Reinisch, W.; Angelberger, S.; Petritsch, W.; Shonova, O.; Lukas, M.; Bar-Meir, S.; Teml, A.; Schaeffeler, E.; Schwab, M.; Dilger, K.; et al. Azathioprine versus Mesalazine for Prevention of Postoperative Clinical Recurrence in Patients with Crohn’s Disease with Endoscopic Recurrence: Efficacy and Safety Results of a Randomised, Double-Blind, Double-Dummy, Multicentre Trial. Gut 2010, 59, 752–759. [Google Scholar] [CrossRef]
- Gjuladin-Hellon, T.; Iheozor-Ejiofor, Z.; Gordon, M.; Akobeng, A.K. Azathioprine and 6-Mercaptopurine for Maintenance of Surgically-Induced Remission in Crohn’s Disease. Cochrane Database Syst. Rev. 2019, 8, CD010233. [Google Scholar] [CrossRef]
- Regueiro, M.; Feagan, B.G.; Zou, B.; Johanns, J.; Blank, M.A.; Chevrier, M.; Plevy, S.; Popp, J.; Cornillie, F.J.; Lukas, M.; et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease After Ileocolonic Resection. Gastroenterology 2016, 150, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Sugita, A.; Futami, K.; Takahashi, K.I.; Motoya, S.; Kimura, H.; Yoshikawa, S.; Kinouchi, Y.; Iijima, H.; Endo, K.; et al. Postoperative Therapy with Infliximab for Crohn’s Disease: A 2-Year Prospective Randomized Multicenter Study in Japan. Surg. Today 2018, 48, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Xu, S.; Huang, F.; Wang, X.; Chen, Y.; Xu, Z. A Meta-Analysis of Efficacy and Safety of Infliximab for Prevention of Postoperative Recurrence in Patients with Crohn’s Disease. Biomed. Res. Int. 2018, 2018, 2615978. [Google Scholar] [CrossRef] [PubMed]
- Armuzzi, A.; Felice, C.; Papa, A.; Marzo, M.; Pugliese, D.; Andrisani, G.; Federico, F.; De Vitis, I.; Rapaccini, G.L.; Guidi, L. Prevention of Postoperative Recurrence with Azathioprine or Infliximab in Patients with Crohn’s Disease: An Open-Label Pilot Study. J. Crohn’s Colitis 2013, 7, E623–E629. [Google Scholar] [CrossRef] [PubMed]
- Savarino, E.; Bodini, G.; Dulbecco, P.; Assandri, L.; Bruzzone, L.; Mazza, F.; Frigo, A.C.; Fazio, V.; Marabotto, E.; Savarino, V. Adalimumab Is More Effective than Azathioprine and Mesalamine at Preventing Postoperative Recurrence of Crohn’s Disease: A Randomized Controlled Trial. Am. J. Gastroenterol. 2013, 108, 1731–1742. [Google Scholar] [CrossRef]
- López-Sanromán, A.; Vera-Mendoza, I.; Domènech, E.; Taxonera, C.; Vega Ruiz, V.; Marín-Jiménez, I.; Guardiola, J.; Castro, L.; Esteve, M.; Iglesias, E.; et al. Adalimumab vs Azathioprine in the Prevention of Postoperative Crohn’s Disease Recurrence. A GETECCU Randomised Trial. J. Crohn’s Colitis 2017, 11, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Ong, M.S.; Grand, R.J.; Mandl, K.D. Trends in Pharmacologic Interventions for Preventing Recurrence of Crohn’s Disease After Ileocolonic Surgery. Inflamm. Bowel Dis. 2016, 22, 2432–2441. [Google Scholar] [CrossRef] [PubMed]
- Caprilli, R.; Andreoli, A.; Capurso, L.; Corrao, G.; D’Albasio, G.; Gioieni, A.; Assuero Lanfranchi, G.; Paladini, I.; Pallone, F.; Ponti, V. Oral Mesalazine (5-Aminosalicylic Acid; Asacol) for the Prevention of Post-Operative Recurrence of Crohn’s Disease. Gruppo Italiano per Lo Studio Del Colon e Del Retto (GISC). Aliment. Pharmacol. Ther. 1994, 8, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Brignola, C.; Cottone, M.; Pera, A.; Ardizzone, S.; Scribano, M.L.; De Franchis, R.; D’Arienzo, A.; D’Albasio, G.; Pennestri, D. Mesalamine in the Prevention of Endoscopic Recurrence after Intestinal Resection for Crohn’s Disease. Italian Cooperative Study Group. Gastroenterology 1995, 108, 345–349. [Google Scholar] [CrossRef]
- McLeod, R.S.; Wolff, B.G.; Steinhart, A.H.; Carryer, P.W.; O’Rourke, K.; Andrews, D.F.; Blair, J.E.; Cangemi, J.R.; Cohen, Z.; Cullen, J.B. Prophylactic Mesalamine Treatment Decreases Postoperative Recurrence of Crohn’s Disease. Gastroenterology 1995, 109, 404–413. [Google Scholar] [CrossRef]
- Frieri, G.; Pimpo, M.T.; Andreoli, A.; Annese, V.; Comberlato, M.; Corrao, G.; Palumbo, G.; Sturniolo, G.C.; Tonelli, F.; Caprilli, R. Prevention of Post-Operative Recurrence of Crohn’s Disease Requires Adequate Mucosal Concentration of Mesalazine. Gruppo Italiano per Lo Studio Del Colon e Del Retto. Aliment. Pharmacol. Ther. 1999, 13, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Chermesh, I.; Tamir, A.; Reshef, R.; Chowers, Y.; Suissa, A.; Katz, D.; Gelber, M.; Halpern, Z.; Bengmark, S.; Eliakim, R. Failure of Synbiotic 2000 to Prevent Postoperative Recurrence of Crohn’s Disease. Dig. Dis. Sci. 2007, 52, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Van Gossum, A.; Dewit, O.; Louis, E.; de Hertogh, G.; Baert, F.; Fontaine, F.; DeVos, M.; Enslen, M.; Paintin, M.; Franchimont, D. Multicenter Randomized-Controlled Clinical Trial of Probiotics (Lactobacillus Johnsonii, LA1) on Early Endoscopic Recurrence of Crohn’s Disease after Lleo-Caecal Resection. Inflamm. Bowel Dis. 2007, 13, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Lémann, M.; Seksik, P.; Laharie, D.; Colombel, J.F.; Bouhnik, Y.; Cadiot, G.; Soulé, J.C.; Bourreille, A.; Metman, E.; et al. Ineffectiveness of Lactobacillus Johnsonii LA1 for Prophylaxis of Postoperative Recurrence in Crohn’s Disease: A Randomised, Double Blind, Placebo Controlled GETAID Trial. Gut 2006, 55, 842–847. [Google Scholar] [CrossRef]
- Prantera, C.; Scribano, M.L.; Falasco, G.; Andreoli, A.; Luzi, C. Ineffectiveness of Probiotics in Preventing Recurrence after Curative Resection for Crohn’s Disease: A Randomised Controlled Trial with Lactobacillus GG. Gut 2002, 51, 405–409. [Google Scholar] [CrossRef]
- Sorrentino, D.; Terrosu, G.; Avellini, C.; Maiero, S. Infliximab with Low-Dose Methotrexate for Prevention of Postsurgical Recurrence of Ileocolonic Crohn Disease. Arch. Intern. Med. 2007, 167, 1804–1807. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, D.; Paviotti, A.; Terrosu, G.; Avellini, C.; Geraci, M.; Zarifi, D. Low-Dose Maintenance Therapy with Infliximab Prevents Postsurgical Recurrence of Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2010, 8, 591–599.e1. [Google Scholar] [CrossRef]
- Yoshida, K.; Fukunaga, K.; Ikeuchi, H.; Kamikozuru, K.; Hida, N.; Ohda, Y.; Yokoyama, Y.; Iimuro, M.; Takeda, N.; Kato, K.; et al. Scheduled Infliximab Monotherapy to Prevent Recurrence of Crohn’s Disease Following Ileocolic or Ileal Resection: A 3-Year Prospective Randomized Open Trial. Inflamm. Bowel Dis. 2012, 18, 1617–1623. [Google Scholar] [CrossRef]
- Araki, T.; Uchida, K.; Okita, Y.; Fujikawa, H.; Inoue, M.; Ohi, M.; Tanaka, K.; Inoue, Y.; Mohri, Y.; Kusunoki, M. Impact of Postoperative Infliximab Maintenance Therapy on Preventing the Surgical Recurrence of Crohn’s Disease: A Single-Center Paired Case-Control Study. Surg. Today 2014, 44, 291–296. [Google Scholar] [CrossRef]
- Papamichael, K.; Archavlis, E.; Lariou, C.; Mantzaris, G.J. Adalimumab for the Prevention and/or Treatment of Post-Operative Recurrence of Crohn’s Disease: A Prospective, Two-Year, Single Center, Pilot Study. J. Crohn’s Colitis 2012, 6, 924–931. [Google Scholar] [CrossRef]
- Aguas, M.; Bastida, G.; Cerrillo, E.; Beltrán, B.; Iborra, M.; Sánchez-Montes, C.; Muñoz, F.; Barrio, J.; Riestra, S.; Nos, P. Adalimumab in Prevention of Postoperative Recurrence of Crohn’s Disease in High-Risk Patients. World J. Gastroenterol. 2012, 18, 4391–4398. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, F.; Yoshikawa, D.; Higashi, S.; Morisaki, T.; Oda, H.; Ikeda, M.; Machida, H.; Matsushima, K.; Minami, H.; Akazawa, Y.; et al. Clinical Efficacy of Adalimumab in Crohn’s Disease: A Real Practice Observational Study in Japan. BMC Gastroenterol. 2016, 16, 82. [Google Scholar] [CrossRef] [PubMed]
- Asada, T.; Nakayama, G.; Tanaka, C.; Kobayashi, D.; Ezaka, K.; Hattori, N.; Kanda, M.; Yamada, S.; Koike, M.; Kodera, Y. Postoperative Adalimumab Maintenance Therapy for Japanese Patients with Crohn’s Disease: A Single-Center, Single-Arm Phase II Trial (CCOG-1107 Study). Surg. Today 2018, 48, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Elisei, W.; Picchio, M.; Zampaletta, C.; Pelecca, G.; Faggiani, R.; Brandimarte, G. Comparison of the Effectiveness of Infliximab and Adalimumab in Preventing Postoperative Recurrence in Patients with Crohn’s Disease: An Open-Label, Pilot Study. Tech. Coloproctol. 2014, 18, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.M.; Fulger, L.E.; Negreanu, L.; Manuc, M.; Sandra, I.; Diculescu, M.M. Adalimumab versus Infliximab in Treating Post-Operative Recurrence of Crohn’s Disease: A National Cohort Study. Rev. Esp. Enferm. Dig. 2016, 108, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Kotze, P.G.; Yamamoto, T.; Danese, S.; Suzuki, Y.; Teixeira, F.V.; de Albuquerque, I.C.; Saad-Hossne, R.; de Barcelos, I.F.; da Silva, R.N.; da Silva Kotze, L.M.; et al. Direct Retrospective Comparison of Adalimumab and Infliximab in Preventing Early Postoperative Endoscopic Recurrence after Ileocaecal Resection for Crohn’s Disease: Results from the MULTIPER Database. J. Crohn’s Colitis 2015, 9, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Cañete, F.; Mañosa, M.; Casanova, M.J.; González-Sueyro, R.C.; Barrio, J.; Bermejo, F.; Nos, P.; Iglesias-Flores, E.; García-Planella, E.; Pérez-Calle, J.L.; et al. Adalimumab or Infliximab for the Prevention of Early Postoperative Recurrence of Crohn Disease: Results From the ENEIDA Registry. Inflamm. Bowel Dis. 2019, 25, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Li, N.; Zhan, S.; Tian, Z.; Wu, D.; Li, T.; Zeng, Z.; Zhuang, X. Anti-TNFα Agents in Preventing the Postoperative Recurrence of Crohn’s Disease: Do They Still Play a Role in the Biological Era? Expert. Opin. Biol. Ther. 2021, 21, 1509–1524. [Google Scholar] [CrossRef] [PubMed]
- Erős, A.; Farkas, N.; Hegyi, P.; Szabó, A.; Balaskó, M.; Veres, G.; Czakó, L.; Bajor, J.; Alizadeh, H.; Rakonczay, Z.; et al. Anti-TNFα Agents Are the Best Choice in Preventing Postoperative Crohn’s Disease: A Meta-Analysis. Dig. Liver Dis. 2019, 51, 1086–1095. [Google Scholar] [CrossRef]
- Gangwani, M.K.; Nawras, M.; Aziz, M.; Rani, A.; Priyanka, F.; Dahiya, D.S.; Ahmed, Z.; Sohail, A.H.; Karna, R.; Lee-Smith, W.; et al. Comparing Adalimumab and Infliximab in the Prevention of Postoperative Recurrence of Crohn’s Disease: A Systematic Review and Meta-Analysis. Ann. Gastroenterol. 2023, 36, 293–299. [Google Scholar] [CrossRef]
- De Cruz, P.; Kamm, M.A.; Hamilton, A.L.; Ritchie, K.J.; Krejany, E.O.; Gorelik, A.; Liew, D.; Prideaux, L.; Lawrance, I.C.; Andrews, J.M.; et al. Efficacy of Thiopurines and Adalimumab in Preventing Crohn’s Disease Recurrence in High-Risk Patients—a POCER Study Analysis. Aliment. Pharmacol. Ther. 2015, 42, 867–879. [Google Scholar] [CrossRef]
- Yamada, A.; Komaki, Y.; Patel, N.; Komaki, F.; Pekow, J.; Dalal, S.; Cohen, R.D.; Cannon, L.; Umanskiy, K.; Smith, R.; et al. The Use of Vedolizumab in Preventing Postoperative Recurrence of Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Taxonera, C.; Lopez-Sanroman, A.; Nos Mateu, P.; Danese, S.; Armuzzi, A.; Roblin, X.; Peyrin-Biroulet, L.; West, R.; Witteman, B.; et al. OP14 Prevention of Postoperative Recurrence of Crohn’s Disease with Vedolizumab: First Results of the Prospective Placebo-Controlled Randomised Trial REPREVIO. J. Crohn’s Colitis 2023, 17, I19. [Google Scholar] [CrossRef]
- Buisson, A.; Nancey, S.; Manlay, L.; Rubin, D.T.; Hebuterne, X.; Pariente, B.; Fumery, M.; Laharie, D.; Roblin, X.; Bommelaer, G.; et al. Ustekinumab Is More Effective than Azathioprine to Prevent Endoscopic Postoperative Recurrence in Crohn’s Disease. United Eur. Gastroenterol. J. 2021, 9, 552–560. [Google Scholar] [CrossRef]
- Yanai, H.; Kagramanova, A.; Knyazev, O.; Sabino, J.; Haenen, S.; Mantzaris, G.J.; Mountaki, K.; Armuzzi, A.; Pugliese, D.; Furfaro, F.; et al. Endoscopic Postoperative Recurrence in Crohn’s Disease After Curative Ileocecal Resection with Early Prophylaxis by Anti-TNF, Vedolizumab or Ustekinumab: A Real-World Multicentre European Study. J. Crohn’s Colitis 2022, 16, 1882–1892. [Google Scholar] [CrossRef]
- Axelrad, J.E.; Li, T.; Bachour, S.P.; Nakamura, T.I.; Shah, R.; Sachs, M.C.; Chang, S.; Hudesman, D.P.; Holubar, S.D.; Lightner, A.L.; et al. Early Initiation of Antitumor Necrosis Factor Therapy Reduces Postoperative Recurrence of Crohn’s Disease Following Ileocecal Resection. Inflamm. Bowel Dis. 2023, 29, 888–897. [Google Scholar] [CrossRef]
- Mañosa, M.; Fernández-Clotet, A.; Nos, P.; Martín-Arranz, M.D.; Manceñido, N.; Carbajo, A.; Hinojosa, E.; Hernández-Camba, A.; Muñoz-Pérez, R.; Boscá-Watts, M.; et al. Ustekinumab and Vedolizumab for the Prevention of Postoperative Recurrence of Crohn’s Disease: Results from the ENEIDA Registry. Dig. Liver Dis. 2023, 55, 46–52. [Google Scholar] [CrossRef]
- Collins, M.; Sarter, H.; Gower-Rousseau, C.; Koriche, D.; Libier, L.; Nachury, M.; Cortot, A.; Zerbib, P.; Blanc, P.; Desreumaux, P.; et al. Previous Exposure to Multiple Anti-TNF Is Associated with Decreased Efficiency in Preventing Postoperative Crohn’s Disease Recurrence. J. Crohn’s Colitis 2017, 11, 281–288. [Google Scholar] [CrossRef]
- Assa, A.; Bronsky, J.; Kolho, K.L.; Zarubova, K.; de Meij, T.; Ledder, O.; Sladek, M.; van Biervliet, S.; Strisciuglio, C.; Shamir, R. Anti-TNFα Treatment After Surgical Resection for Crohn’s Disease Is Effective Despite Previous Pharmacodynamic Failure. Inflamm. Bowel Dis. 2017, 23, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Le Cosquer, G.; Altwegg, R.; Rivière, P.; Bournet, B.; Boivineau, L.; Poullenot, F.; Bozon, A.; Buscail, L.; Laharie, D.; Gilletta, C. Prevention of Post-Operative Recurrence of Crohn’s Disease among Patients with Prior Anti-TNFα Failure: A Retrospective Multicenter Study. Dig. Liver Dis. 2023, 55, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Kumar, L.; Doherty, G. The Tortoise (Endoscopy-Driven Treatment) and the Hare (Prophylactic Treatment): Who Wins the Race to Beat Post-Operative Recurrence of Crohn’s Disease? J. Crohn’s Colitis 2023, 17, 309–310. [Google Scholar] [CrossRef]
- Chen, R.; Zheng, J.; Li, C.; Chen, Q.; Zeng, Z.; Li, L.; Chen, M.; Zhang, S. Prognostic Models for Predicting Postoperative Recurrence in Crohn’s Disease: A Systematic Review and Critical Appraisal. Front. Immunol. 2023, 14, 1215116. [Google Scholar] [CrossRef]
- Boube, M.; Laharie, D.; Nancey, S.; Hebuterne, X.; Fumery, M.; Pariente, B.; Roblin, X.; Peyrin-Biroulet, L.; Minet-Quinard, R.; Pereira, B.; et al. Variation of Faecal Calprotectin Level within the First Three Months after Bowel Resection Is Predictive of Endoscopic Postoperative Recurrence in Crohn’s Disease. Dig. Liver Dis. 2020, 52, 740–744. [Google Scholar] [CrossRef]
- Tham, Y.S.; Yung, D.E.; Fay, S.; Yamamoto, T.; Ben-Horin, S.; Eliakim, R.; Koulaouzidis, A.; Kopylov, U. Fecal Calprotectin for Detection of Postoperative Endoscopic Recurrence in Crohn’s Disease: Systematic Review and Meta-Analysis. Therap Adv. Gastroenterol. 2018, 11, 1756284818785571. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factors Considered | Number of Risk Factors to Define a High-Risk Patient | When to Start Prophylactic Therapy | Recommended Therapy | |
|---|---|---|---|---|
| ECCO, 2017 [12] |
| 1 | At least 1 risk factor | Thiopurines or anti-TNFs High-dose mesalamine is an option after an isolated ileal resection |
| AGA, 2017 [13] |
| 1 | Start systematically | Thiopurines or anti-TNFs |
| BSG, 2019 [14] |
| 2 | At least 2 risk factors | Thiopurines or anti-TNFs |
| CORTICOSTEROIDS | |||
| Author and Year of Publication | Number of Patients Included | Drug Investigated | Results |
| Ewe et al., 1999 [89] | RCT (n = 83) | Budesonide 3 mg/day versus placebo | Similar recurrence rate (endoscopic and/or clinical) (57% vs. 70%, p = ns) at 1 year |
| Hellers et al., 1999 [90] | RCT (n = 129) | Budesonide 6 mg/day versus placebo | Similar endoscopic POR at month 3 (31% vs. 52%, p = ns) and at month 12 (52% vs. 58%, p = ns) |
| ANTIBIOTICS | |||
| Author and Year of Publication | Number of Patients Included | Drug Investigated | Results |
| Rutgeerts et al., 1995 [91] | RCT (n = 60) | Metronidazole (20 mg/kg daily) versus placebo for 3 months | Reduced endoscopic (52% vs. 75%, p = 0.09), severe endoscopic (13% vs. 43%, p = 0.02) at month 3 and reduced clinical recurrence at 1 year (4% vs. 25%, p = 0.044) |
| Rutgeerts et al., 2005 [92] | RCT (n = 80) | Ornidazole (1 gr/day) versus placebo for 1 year | Reduced both clinical (7.9% vs. 37.5%; p = 0.0046) and endoscopic recurrence (53.6% vs. 79%; p = 0.037) at 1 year |
| Herfarth et al., 2013 [93] | RCT (n = 33) | Ciprofloxacin (500 mg/twice daily) versus placebo for 6 months | Similar endoscopic (65% vs. 69%, p < 0.805) POR at 6 months |
| MESALAZINE | |||
| Author and Year of Publication | Number of Patients Included | Drug Investigated | Results |
| Florent et al., 1996 [94] | RCT (n = 126) | Mesalazine (3 gr/day) versus placebo for 3 months | Similar endoscopic recurrence at 12 weeks (50% vs. 63%; p = 0.16) |
| Hanauer et al., 2004 [95] | RCT (n = 131) | 6-MP (50 mg/day) versus mesalazine (3 gr/day) versus placebo for 24 months | No statistically significant difference between mesalazine and placebo in terms of clinical recurrence (HR 0.62; p = 0.123) and endoscopic recurrence (HR 1.10; p = 0.82) over 2 years |
| Lochs et al., 2000 [96] | RCT (n = 318) | Pentasa (4 gr/day) versus placebo for 18 months | Similar cumulative relapse rates (24.5% vs. 31.4%; p = 0.10) at 18 months |
| Caprilli et al., 2003 [97] | RCT (n = 206) | Mesalazine: 4 gr/day versus 2.4 gr/day for 1 year | No statistically significant differences between endoscopic recurrence (score > 1) (33% vs. 43%; p = 0.19) and clinical (12% vs. 14%; p = 0.58) POR at 1 year |
| Gjuladin-Hellon et al., 2019 [98] | Meta-analysis (5 studies, n = 730) | Mesalazine versus placebo | During a follow-up period of 12 to 72 months, reduced clinical POR (36% vs. 43%, RR 0.83, 95% CI 0.72–0.96) |
| Gjuladin-Hellon et al., 2019 [98] | Meta-analysis (3 studies, n = 537) | Mesalazine versus placebo | During a follow-up period of 12 to 72 months, similar endoscopic POR (70% vs. 73%, RR 0.83, 95% CI 0.56–1.23) |
| IMMUNOMODULATORS | |||
| Author and Year of Publication | Number of Patients Included | Drug Investigated | Results |
| Hanauer et al., 2004 [95] | RCT (n = 131) | 6-MP (50 mg/day) versus mesalazine (3 gr/day) versus placebo for 24 months | 6-MP (50 mg/day) was more effective than placebo (p < 0.05) in preventing clinical recurrence (50% vs. 77%, respectively) and endoscopic recurrence (43% vs. 64%, respectively) over 2 years |
| Mowat et al., 2016 [99] | RCT (n = 240) | 6-MP (1 mg/kg) versus placebo for 3 years | Similar clinical recurrence (13% vs. 23%, HR 0.54; 95% CI 0.27–1.06), but in the smoker subgroup, 6-MP achieved lower rate of clinical POR (10% vs. 46%, HR 0.13; 95% CI 0.04–0.46) |
| D’Haens et al., 2008 [100] | RCT (n = 81) | AZA for 12 months + metronidazole for 3 months versus metronidazole alone for 3 months | The addition of AZA reduced endoscopic POR at 12 months (43.7% vs. 69.0%; p = 0.048) |
| Mañosa et al., 2013 [101] | RCT (n = 50) | AZA for 12 months + metronidazole for 3 months versus AZA alone for 12 months | No statistically significant difference with the addition of a course of metronidazole in terms of endoscopic POR both at 6 months (28% vs. 44%, p = 0.19) and at 12 months (36% and 56%, p = 0.15) |
| Reinisch et al., 2010 [102] | RCT (n = 78) | AZA (2.0–2.5 mg/kg/day) versus mesalazine (4 g/day) over 1 year | At 12 months, lower clinical recurrence for AZA (0% vs. 10.8%, p = 0.031) in patients with endoscopic recurrence. Additionally, greater median improvement in Rutgeerts score |
| Gjuladin-Hellon et al., 2019 [103] | Meta-analysis (3 studies, n = 408) | Thiopurines versus placebo | Thiopurines reduced clinical (51% vs. 64%, RR 0.79, 95% CI 0.67–0.92) POR after 12–36 months |
| ANTI-TNF | |||
| Author and Year of Publication | Number of Patients Included | Drug Investigated | Results |
| Regueiro et al., 2016 [104] | RCT (n = 297) | Infliximab versus placebo | At week 76, reduction of endoscopic recurrence (30.6% vs. 60.0%, p < 0.001), but regarding clinical recurrence, no statistically significant difference (12.9% vs. 20.0%, p = 0.097) |
| Fukushima et al., 2018 [105] | RCT (n = 38) | Infliximab versus placebo | Lower recurrence rate (clinical and/or endoscopic) (52.6% vs. 94.7%, p = 0.0032) at 2 years |
| Huang et al., 2018 [106] | Meta-analysis (7 trials, n = 455) | Infliximab versus placebo | Reduced endoscopic (RR = 0.421, 95% CI 0.328–0.539; p < 0.001) and clinical POR (RR = 0.519, 95% CI 0.349–0.774; p = 0.001) |
| Armuzzi et al., 2013 [107] | RCT (n = 22) | Infliximab versus AZA | No difference in clinical and endoscopic POR, but clear reduction in histological activity (18% vs. 80%; p = 0.008) at 12 months |
| Savarino et al., 2013 [108] | RCT (n = 51) | ADA versus AZA versus mesalazine | Lower endoscopic POR in the ADA group (6.3%) compared with the AZA (64.7%) and mesalamine groups (83.3%). Similar data also for clinical recurrence |
| López-Sanromán et al., 2017 [109] | RCT (n = 84) | ADA versus AZA, both associated with metronidazole | ADA did not demonstrate superiority over AZA (42.2% vs. 59%, p = 0.12) at week 52 |
| Beelen et al., 2022 [44] | Meta-analysis (6 trials, n = 645) | Anti-TNF versus thiopurine | Lower endoscopic and clinical POR with anti-TNF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spertino, M.; Gabbiadini, R.; Dal Buono, A.; Busacca, A.; Franchellucci, G.; Migliorisi, G.; Repici, A.; Spinelli, A.; Bezzio, C.; Armuzzi, A. Management of Post-Operative Crohn’s Disease: Knowns and Unknowns. J. Clin. Med. 2024, 13, 2300. https://doi.org/10.3390/jcm13082300
Spertino M, Gabbiadini R, Dal Buono A, Busacca A, Franchellucci G, Migliorisi G, Repici A, Spinelli A, Bezzio C, Armuzzi A. Management of Post-Operative Crohn’s Disease: Knowns and Unknowns. Journal of Clinical Medicine. 2024; 13(8):2300. https://doi.org/10.3390/jcm13082300
Chicago/Turabian StyleSpertino, Matteo, Roberto Gabbiadini, Arianna Dal Buono, Anita Busacca, Gianluca Franchellucci, Giulia Migliorisi, Alessandro Repici, Antonino Spinelli, Cristina Bezzio, and Alessandro Armuzzi. 2024. "Management of Post-Operative Crohn’s Disease: Knowns and Unknowns" Journal of Clinical Medicine 13, no. 8: 2300. https://doi.org/10.3390/jcm13082300