
Comparative Efficacy of Transsphenoidal and Transcranial Approaches for Treating Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis

 ,
, 
 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Data Extraction
2.3. Outcomes
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Review
3.2. Data Analysis
3.2.1. Baseline Data
3.2.2. Data Meta-Analysis
Surgical Outcomes
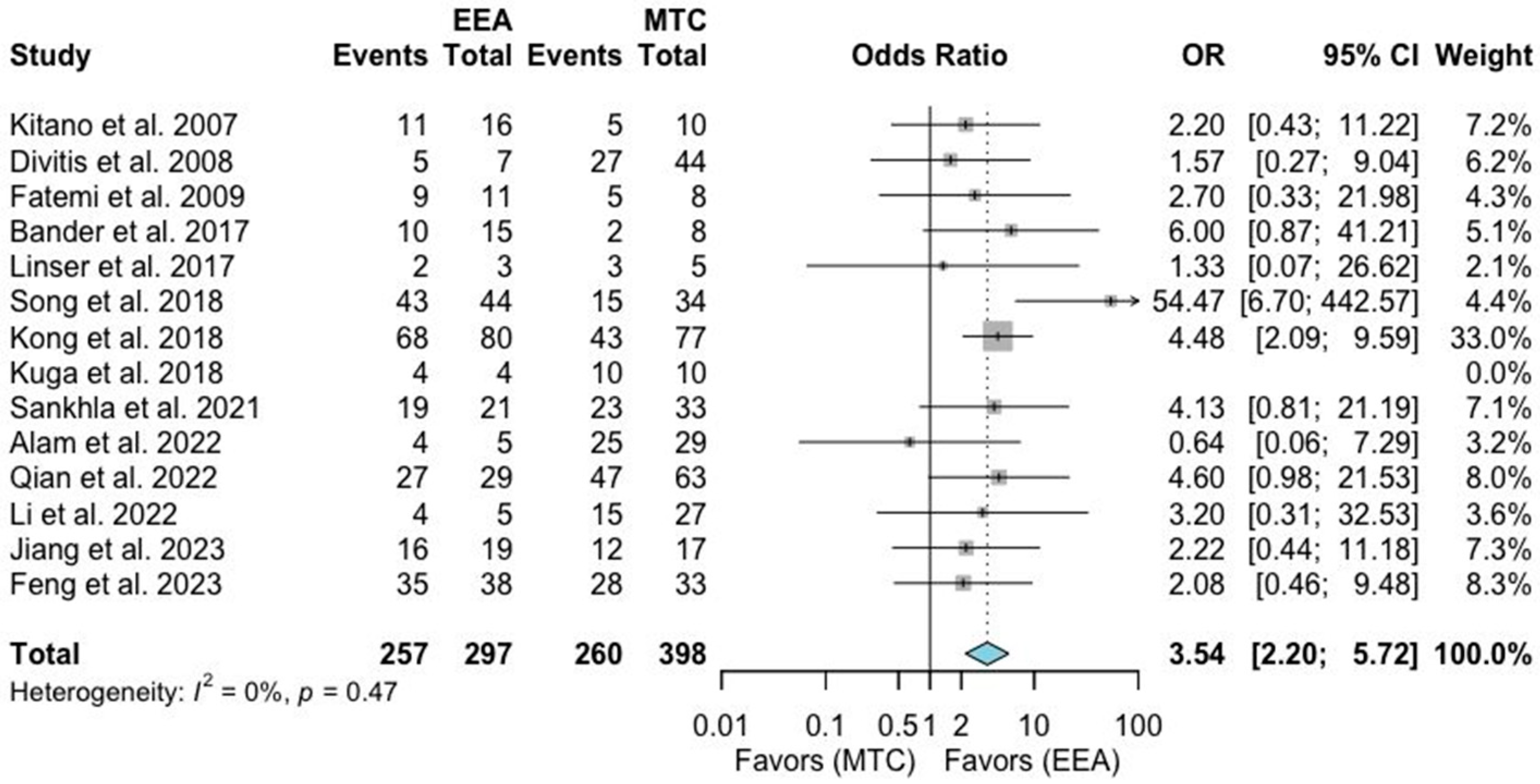
- Visual outcomes
- Gross total resection (GTR)
- Recurrence rate
Postoperative Complications
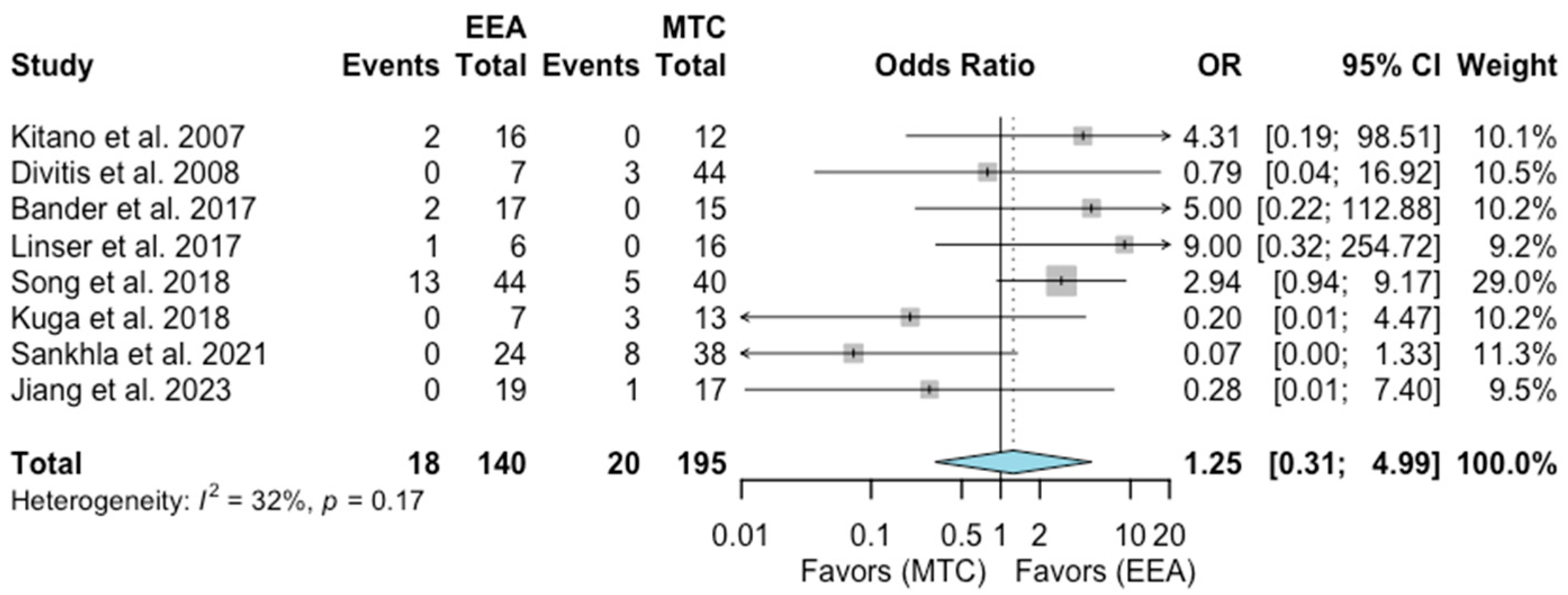
- Cerebrospinal fluid leak (CSF leak)
- Infections
- Dysosmia
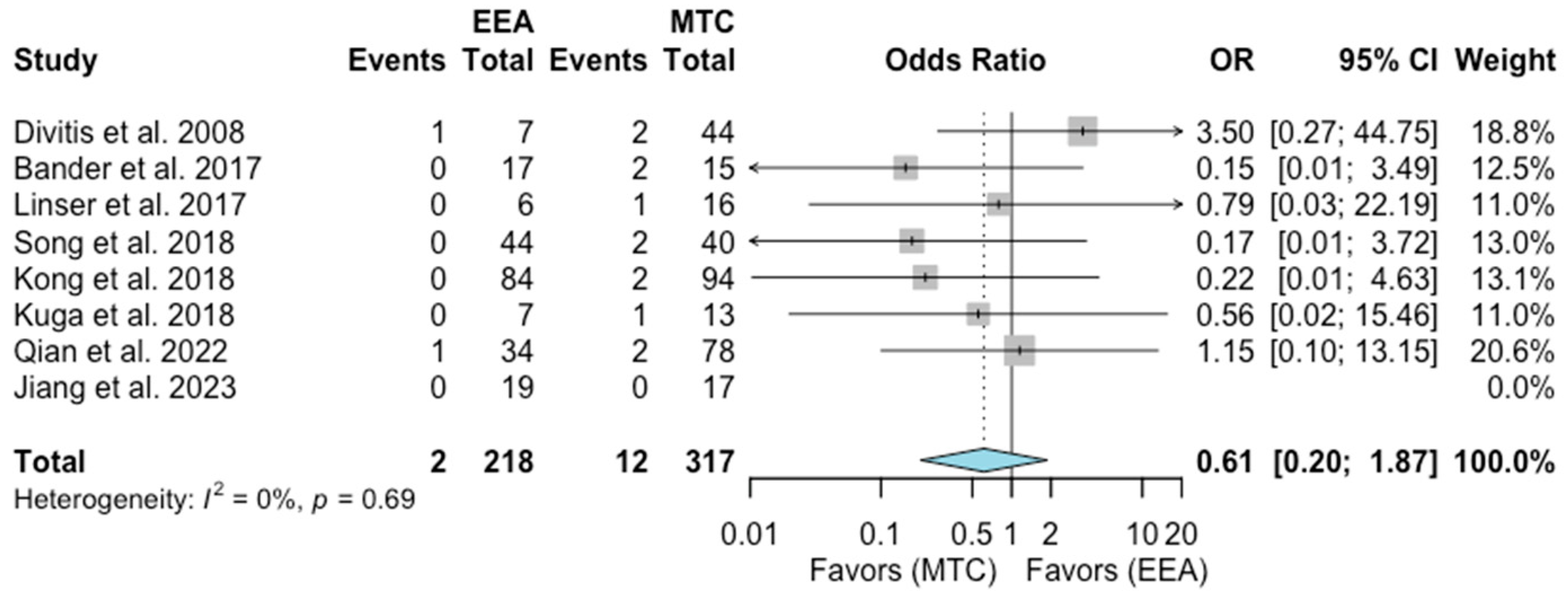
- Intracranial hemorrhage (ICH)
- Endocrine disorders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A

References
- Alam, S.; Ferini, G.; Muhammad, N.; Ahmed, N.; Wakil, A.N.M.; Islam, K.M.A.; Arifin, M.S.; Al Mahbub, A.; Habib, R.; Mojumder, M.R.; et al. Skull Base Approaches for Tuberculum Sellae Meningiomas: Institutional Experience in a Series of 34 Patients. Life 2022, 12, 492. [Google Scholar] [CrossRef]
- Agosti, E.; Saraceno, G.; Rampinelli, V.; Raffetti, E.; Veiceschi, P.; Buffoli, B.; Rezzani, R.; Giorgianni, A.; Hirtler, L.; Alexander, A.Y.; et al. Quantitative Anatomic Comparison of Endoscopic Transnasal and Microsurgical Transcranial Approaches to the Anterior Cranial Fossa. Oper. Neurosurg. 2022, 23, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.H.; McDermott, M.W. Tuberculum sellae meningiomas. Neurosurg. Focus 2003, 14, 6. [Google Scholar] [CrossRef]
- Guduk, M.; Yener, U.; Sun, H.I.; Hacihanefioglu, M.; Ozduman, K.; Pamir, M.N. Pterional and Unifrontal Approaches for the Microsurgical Resection of Olfactory Groove Meningiomas: Experience with 61 Consecutive Patients. Turk. Neurosurg. 2017, 27, 707–715. [Google Scholar]
- Banu, M.A.; Guerrero-Maldonado, A.; McCrea, H.J.; Garcia-Navarro, V.; Souweidane, M.M.; Anand, V.K.; Greenfield, J. Impact of skull base development on endonasal endoscopic surgical corridors. J. Neurosurg. Pediatr. 2014, 13, 155–169. [Google Scholar] [CrossRef]
- Bander, E.D.; Singh, H.; Ogilvie, C.B.; Cusic, R.C.; Pisapia, D.J.; Tsiouris, A.J.; Anand, V.K.; Schwartz, T.H. Endoscopic endonasal versus transcranial approach to tuberculum sellae and planum sphenoidale meningiomas in a similar cohort of patients. J. Neurosurg. 2018, 128, 40–48. [Google Scholar] [CrossRef]
- Bowers, C.A.; Altay, T.; Couldwell, W.T. Surgical decision-making strategies in tuberculum sellae meningioma resection. Neurosurg. Focus 2011, 30, E1. [Google Scholar] [CrossRef]
- Chen, S.H.; Zenonos, G.; Goldschmidt, E.; Sprau, A.; Sedighim, S.; Sur, S.; Cabral, D.F.; Algattas, H.; Jacobs, R.; Wang, E.; et al. A Multi-institutional Comparison of Transcranial versus Endoscopic Endonasal Approaches for Planum and Tuberculum Sellae Meningiomas. J. Neurol. Surg. Part B Skull Base 2019, 80, S1–S244. [Google Scholar]
- de Divitiis, E.; Esposito, F.; Cappabianca, P.; Cavallo, L.M.; de Divitiis, O. Tuberculum sellae meningiomas: High route or low route? A series of 51 consecutive cases. Neurosurgery 2008, 62, 556–563. [Google Scholar] [CrossRef]
- Fatemi, N.; Dusick, J.R.; de Paiva Neto, M.A.; Malkasian, D.; Kelly, D.F. Endonasal versus supraorbital keyhole removal of craniopharyngiomas and tuberculum sellae meningiomas. Neurosurgery 2009, 64, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Li, C.; Cao, L.; Liu, C.; Qiao, N.; Wu, W.; Gui, S. Comparative analysis of outcomes following craniotomy and expanded endoscopic endonasal approach resection of tuberculum sellae meningiomas: A single-institution study. Front. Neurol. 2023, 14, 1139968. [Google Scholar] [CrossRef]
- Jiang, H.; Wang, P.; Wang, J.; Liu, J.; Tang, C.; Zhang, G.; Wu, N. Comparison of supraorbital keyhole approach and extended transsphenoidal approach in endoscopic surgery for tuberculum sellae meningioma: A case series. Exp. Ther. Med. 2023, 25, 215. [Google Scholar] [CrossRef]
- Kitano, M.; Taneda, M.; Nakao, Y. Postoperative improvement in visual function in patients with tuberculum sellae meningiomas: Results of the extended transsphenoidal and transcranial approaches. J. Neurosurg. 2007, 107, 337–346. [Google Scholar] [CrossRef]
- Kong, D.S.; Hong, C.K.; Hong, S.D.; Cheng, G.S. Selection of endoscopic or transcranial surgery for tuberculum sellae meningiomas according to specific anatomical features: A retrospective multicenter analysis (KOSEN-002). J. Neurosurg. 2018, 130, 838–847. [Google Scholar] [CrossRef]
- Kuga, D.; Toda, M.; Yoshida, K. Treatment Strategy for Tuberculum Sellae Meningiomas Based on a Preoperative Radiological Assessment. World Neurosurg. 2018, 120, 1279–1288. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, C.; Su, J.; Qin, C.; Wang, X.; Li, Y.; Liu, Q. Individualized surgical treatment of giant tuberculum sellae meningioma: Unilateral subfrontal approach vs. endoscopic transsphenoidal approach. Front. Surg. 2022, 9, 990646. [Google Scholar] [CrossRef]
- Linsler, S.; Fischer, G.; Skliarenko, V.; Stadie, A.; Oertel, J. Endoscopic Assisted Supraorbital Keyhole Approach or Endoscopic Endonasal Approach in Cases of Tuberculum Sellae Meningioma: Which Surgical Route Should Be Favored? World Neurosurg. 2017, 104, 601–611. [Google Scholar] [CrossRef]
- Magill, S.T.; Morshed, R.A.; Lucas, C.H.G.; Aghi, M.K.; Theodosopoulos, P.V.; Berger, M.S.; de Divitiis, O.; Solari, D.; Cappabianca, P.; Cavallo, L.M.; et al. Tuberculum sellae meningiomas: Grading scale to assess surgical outcomes using the transcranial versus transsphenoidal approach. Neurosurg. Focus 2018, 44, 9. [Google Scholar] [CrossRef]
- Qian, K.; Nie, C.; Zhu, W.; Zhao, H.; Zhang, F.; Wang, H.; Jiang, X. Surgical management of tuberculum sellae meningioma: Transcranial approach or endoscopic endonasal approach? Front. Surg. 2022, 9, 979940. [Google Scholar] [CrossRef] [PubMed]
- Sankhla, S.K.; Jayashankar, N.; Khan, M.; Khan, G.M. Surgical Management of Tuberculum Sellae Meningioma: Our Experience and Review of the Literature. Neurol. India 2021, 69, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.; Signorelli, F.; Rapisarda, A.; D’Onofrio, G.F.; Visocchi, M. Tuberculum Sellae Meningioma: Report of Two Cases and Literature Review of Limits of the Transcranial and Endonasal Endoscopic Approaches. Acta Neurochir. Suppl. 2023, 135, 75–79. [Google Scholar]
- Song, S.W.; Kim, Y.H.; Kim, J.W.; Park, C.K.; Kim, J.E.; Kim, D.G.; Jung, H.W. Outcomes After Transcranial and Endoscopic Endonasal Approach for Tuberculum Meningiomas-A Retrospective Comparison. World Neurosurg. 2018, 109, 434–445. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; E Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis; University of Liverpool: Liverpool, UK, 2000. [Google Scholar]
- Giammattei, L.; Starnoni, D.; Cossu, G.; Bruneau, M.; Cavallo, L.M.; Cappabianca, P.; Meling, T.R.; Jouanneau, E.; Schaller, K.; Benes, V.; et al. Surgical management of Tuberculum sellae Meningiomas: Myths, facts, and controversies. Acta Neurochir. 2020, 162, 631–640. [Google Scholar] [CrossRef]
- Navarro-Olvera, J.L.; Parra-Romero, G.; Carrillo-Ruiz, J.D.; Aguado-Carrillo, G.; Hernández-Valencia, A.F. Resection of meningiomas in a different location (sphenoid wing and tuberculum sellae) through a single craniotomy report of a case and review of the literature. Cir. Cir. 2021, 89, 66–69. [Google Scholar]
- Troude, L.; Boucekine, M.; Baucher, G.; Farah, K.; Boissonneau, S.; Fuentes, S.; Graillon, T.; Dufour, H. Ipsilateral vs controlateral approach in tuberculum sellae meningiomas surgery: A retrospective comparative study. Neurosurg. Rev. 2021, 44, 3581–3591. [Google Scholar] [CrossRef]
- Muskens, I.S.; Briceno, V.; Ouwehand, T.L.; Castlen, J.P.; Gormley, W.B.; Aglio, L.S.; Najafabadi, A.H.Z.; van Furth, W.R.; Smith, T.R.; Mekary, R.A.; et al. The endoscopic endonasal approach is not superior to the microscopic transcranial approach for anterior skull base meningiomas-a meta-analysis. Acta Neurochir. 2018, 160, 59–75. [Google Scholar] [CrossRef]
- Clark, A.J.; Jahangiri, A.; Garcia, R.M.; McDermott, M.W. Endoscopic surgery for tuberculum sellae meningiomas: A systematic review and meta-analysis. Neurosurg. Rev. 2013, 36, 349–359. [Google Scholar] [CrossRef]
- Yu, P.; Xu, T.; Wu, X.; Liu, Z.; Wang, Y.; Wang, Y. The expanded endoscopic endonasal approach for treatment of tuberculum sellae meningiomas in a series of 40 consecutive cases. Sci. Rep. 2021, 11, 4993. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, A.E.; Snyder, M.H.; Rabinovich, E.P.; Malkawi, D.; Chakravarti, S.; Wei, O.; Cheshire, M.; Price, M.C.; Khalafallah, A.M.; Rowan, N.R.; et al. Comparison and evolution of transcranial versus endoscopic endonasal approaches for suprasellar Meningiomas: A systematic review. J. Clin. Neurosci. 2022, 99, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Banu, M.A.; Placantonakis, D.G.; Tsiouris, A.J.; Khan, O.H.; Anand, V.K.; Schwartz, T.H. Endoscopic endonasal resection of suprasellar meningiomas: The importance of case selection and experience in determining extent of resection, visual improvement, and complications. World Neurosurg. 2014, 82, 442–449. [Google Scholar] [CrossRef]
- McCoul, E.D.; Anand, V.K.; Singh, A.; Nyquist, G.G.; Schaberg, M.R.; Schwartz, T.H. Long-term effectiveness of a reconstructive protocol using the nasoseptal flap after endoscopic skull base surgery. World Neurosurg. 2014, 81, 136–143. [Google Scholar] [CrossRef]
- Hadad, G.; Bassagasteguy, L.; Carrau, R.L.; Mataza, J.C.; Kassam, A.; Snyderman, C.H.; Mintz, A.; Msc, A.M. A novel reconstructive technique after endoscopic expanded endonasal approaches: Vascular pedicle nasoseptal flap. Laryngoscope 2006, 116, 1882–1886. [Google Scholar] [CrossRef]
- Cai, X.; Yang, J.; Zhu, J.; Tang, C.; Cong, Z.; Liu, Y.; Ma, C. Reconstruction strategies for intraoperative CSF leak in endoscopic endonasal skull base surgery: Systematic review and meta-analysis. Br. J. Neurosurg. 2022, 36, 436–446. [Google Scholar] [CrossRef]
- Algattas, H.; Setty, P.; Goldschmidt, E.; Wang, E.W. Endoscopic Endonasal Approach for Craniopharyngiomas with Intraventricular Extension: Case Series, Long-Term Outcomes, and Review. World Neurosurg. 2020, 144, 447–459. [Google Scholar] [CrossRef]
- Sigler, A.C.; D’Anza, B.; Lobo, B.C.; Woodard, T.D.; Recinos, P.F.; Sindwani, R. Endoscopic Skull Base Reconstruction: An Evolution of Materials and Methods. Otolaryngol. Clin. N. Am. 2017, 50, 643–653. [Google Scholar] [CrossRef]
- Khan, O.H.; Krischek, B.; Holliman, D.; Klironomos, G.; Kucharczyk, W.; Vescan, A.; Gentili, F.; Zadeh, G. Pure endoscopic expanded endonasal approach for olfactory groove and tuberculum sellae meningiomas. J. Clin. Neurosci. 2014, 21, 927–933. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Country | Study Period | Patients (N) | Age (Mean ± SD) | Female (N; %) | Visual Disturbance (N) | Tumor Size (Volume or Diameter) | Optic Canal Invasion | Follow-Up (Mean, Range) * |
|---|---|---|---|---|---|---|---|---|---|
| Kitano et al. [13] 2007 | Japan | 1994–2006 | EEA: 16 MTA:12 | EEA: 54 ± 10 MTA: 61 ± 9 | 24; 85.7% | EEA: 16 MTA: 10 | EEA: 7.5 ± 5.4 cm3 MTA: 8.9 ± 9.4 cm3 | N/A | N/A; EEA: 3–96 MTA: 108–156 |
| Divitiis et al. [9] 2008 | Italy | 1983–2006 | EEA: 7 MTA:44 | N/A | 41; 80.3% | EEA: 7 MTA: 44 | EEA: <2.0 cm (2 pts); 2.0–4.0 cm (5 pts); MTA: <2.0 cm (6 pts); 2.0–4.0 cm (33 pts); >4.0 cm (5 pts) | EEA: 1/7 MTA: 2/44 | N/A; EEA: 1–20 MTA: 9–252 |
| Fatemi et al. [10] 2009 | USA | 2000–2008 | EEA: 14 MTA:9 | EEA: 51 ± 15 MTA: 49 ± 7 | 16; 69.6% | EEA: 11 MTA: 8 | EEA: 2.5 ± 8 cm MTA: 3.3 ± 10 cm | N/A | EEA: 32 MTA: 15; EEA: 6–65 MTA: 3–28 |
| Bowers et al. [7] 2011 | USA | 2002–2010 | EEA: 5 MTA: 22 | EEA: 58 ± 17 MTA: 53 ± 13 | 22; 81.5% | 23 | EEA: 2.5 ± 7 cm MTA: 3.1 ± 13 cm | N/A | N/A; 12–120 |
| Bander et al. [6] 2018 | USA | 2000–2015 | EEA: 17 MTA: 15 | EEA: 54 ± 14.3 MTA: 56 ± 12.9 | 20; 90.9% | EEA: 15 MTA: 8 | EEA: 5.6 ± 3.4 cm3 MTA: 5.0 ± 3.4 cm3 | N/A | EEA: 25 MTA: 37; N/A |
| Linsler et al. [17] 2017 | Germany | 2011–2016 | EEA: 6 MTA: 16 | EEA: 64 ±12.4 MTA: 61 ± 8.1 | 17; 77.2% | EEA: 3 MTA: 5 | EEA: 2.1 ± 0.8 cm3 MTA: 14.9 ± 8.2 cm3 | N/A | EEA: 15 MTA: 20; 3–60 |
| Song et al. [22] 2018 | Korea | 2004–2015 | EEA: 44 MTA: 40 | EEA: 53 MTA: 54 | 72; 85.7% | EEA: 44 MTA: 34 | EEA: 2.5 ± 6 cm MTA: 2.6 ± 8 cm | EEA: 34/44 MTA: 32/40 | N/A; 0–147 |
| Magill et al. [18] 2018 | USA | 1997–2016 | EEA: 44 MTA: 95 | N/A | N/A | 121 | N/A | EEA: 26/44 MTA: 86/95 | 46; 0–174 |
| Kong et al. [14] 2018 | Korea | 2010–2016 | EEA: 84 MTA: 94 | EEA: 54 ± 14 MTA: 54 ± 11 | 136; 76.4% | EEA: 80 MTA: 77 | EEA: 2.4 ± 7 cm MTA: 2.1 ± 8 cm | EEA: 60/84 MTA: 51/94 | 28; 3–71 |
| Kuga et al. [15] 2018 | Japan | 2010–2018 | EEA: 7 MTA: 13 | EEA: 55 MTA: 57 | 18; 90.0% | EEA: 4 MTA: 10 | EEA: 2.1 cm MTA: 2.3 cm | EEA: 0/7 MTA: 3/13 | EEA: 19 MTA: 40; EEA: 1–39 MTA: 3–82 |
| Chen et al. [8] 2019 | USA | N/A | EEA: 65 MTA: 56 | EEA: 56 MTA: 57 | 92; 76.0% | EEA: 47 MTA: 37 | N/A | N/A | EEA: 19 MTA: 17; N/A |
| Sankhla et al. [20] 2021 | India | 2005–2018 | EEA: 24 MTA: 38 | N/A | 46; 74.2% | EEA: 21 MTA: 33 | 2.3–5.8 cm | N/A | 24; N/A |
| Alam et al. [1] 2022 | Bangladesh | 2015–2020 | EEA: 5 MTA: 29 | N/A | 28; 96.5% | EEA: 5 MTA: 29 | <3.0 cm (15 pts) 3.0–6.0 cm (17 pts) >6.0 cm (2 pts) | N/A | N/A |
| Qian et al. [19] 2022 | China | 2017–2021 | EEA: 34 MTA: 78 | EEA: 52 MTA: 51 | 70; 62.5% | EEA: 29 MTA: 63 | EEA: 10.7 cm3 MTA: 11.5 cm3 | EEA: 22/34 MTA: 45/78 | 21; 3–36 |
| Li et al. [16] 2022 | China | 2012–2021 | EEA: 7 MTA: 31 | N/A | 23; 60.5% | EEA: 5 MTA: 27 | EEA: 3.1 cm MTA: 3.7 cm | EEA: 0/7 MTA: 9/31 | 66; 6–120 |
| Silvestri et al. [21] 2023 | Italy | N/A | EEA: 1 MTA: 1 | EEA: 68 MTA: 45 | N/A | EEA: 1 MTA: 1 | EEA: N/A MTA: 1.8 × 1.7 × 1.9 cm | N/A | N/A |
| Jiang et al. [12] 2023 | China | 2014–2020 | EEA: 19 MTA: 17 | N/A | 32; 88.8% | EEA: 19 MTA: 17 | EEA: 2.8 cm MTA: 3.4 cm | N/A | N/A |
| Feng et al. [11] 2023 | China | 2015–2021 | EEA: 45 MTA: 39 | EEA: 53 MTA: 52 | 11; 13.1% | EEA: 38 MTA: 33 | EEA: 11.3 cm3 MTA: 10.6 cm3 | EEA: 27/45 MTA: 21/39 | EEA: 49 MTA: 42; N/A |
| Authors and Year Age | Surgical Outcomes | Postoperative Complications | ||||||
|---|---|---|---|---|---|---|---|---|
| GTR | Recurrence | Visual Improvement | CSF Leak | Infection | Dysosmia/Anosmia | ICH | Endocrine Disorders | |
| Kitano et al. [13] 2007 | N/A | N/A | EEA: 11/16 MTA: 5/10 | EEA: 2 MTA: 1 | N/A | EEA: 2 MTA: 0 | N/A | N/A |
| Divitiis et al. [9] 2008 | EEA: 6/7 MTA: 39/44 | EEA: 0/6 MTA: 1/39 | EEA: 5/7 MTA: 27/44 | EEA: 2 MTA: 3 | N/A | EEA: 0 MTA: 3 | EEA: 1 MTA: 2 | EEA: 1 MTA: 2 |
| Fatemi et al. [10] 2009 | EEA: 7/14 MTA: 2/9 | EEA: 0/7 MTA: 1/2 | EEA: 9/11 MTA: 5/8 | EEA: 4 MTA: 0 | N/A | N/A | N/A | EEA: 1 MTA: 0 |
| Bowers et al. [7] 2011 | EEA: 2/5 MTA: 20/22 | N/A | N/A | EEA: 1 MTA: 0 | EEA: 0 MTA: 1 | N/A | N/A | EEA: 0 MTA: 1 |
| Bander et al. [6] 2018 | EEA: 14/17 MTA: 8/15 | N/A | EEA: 10/15 MTA: 2/8 | EEA: 2 MTA: 0 | N/A | EEA: 2 MTA: 0 | EEA: 0 MTA: 2 | EEA: 0 MTA: 0 |
| Linsler et al. [17] 2017 | EEA: 5/6 MTA: 14/16 | EEA: 1/5 MTA: 0/14 | EEA: 2/3 MTA: 3/5 | EEA: 0 MTA: 1 | N/A | EEA: 1 MTA: 0 | EEA: 0 MTA: 1 | EEA: 0 MTA: 1 |
| Song et al. [22] 2018 | EEA: 37/44 MTA: 26/38 | EEA: 5/37 MTA: 4/26 | EEA: 43/44 MTA: 15/34 | EEA: 1 MTA: 0 | EEA: 7 MTA: 1 | EEA: 13 MTA: 5 | EEA: 0 MTA: 2 | EEA: 3 MTA: 6 |
| Magill et al. [18] 2018 | EEA: 25/44 MTA: 66/95 | N/A | N/A | EEA: 5 MTA: 2 | EEA: 1 MTA: 5 | N/A | N/A | N/A |
| Kong et al. [14] 2018 | EEA: 70/84 MTA: 75/94 | N/A | EEA: 68/80 MTA: 43/77 | EEA: 4 MTA: 0 | EEA: 7 MTA: 2 | N/A | EEA: 0 MTA: 2 | N/A |
| Kuga et al. [15] 2018 | EEA: 7/7 MTA: 13/13 | EEA: 0/7 MTA: 1/13 | EEA: 4/4 MTA: 10/10 | EEA: 1 MTA: 0 | EEA: 0 MTA: 0 | EEA: 0 MTA: 3 | EEA: 0 MTA: 1 | EEA: 0 MTA: 0 |
| Chen et al. [8] 2019 | N/A | N/A | N/A | EEA: 3 MTA: 3 | EEA: 0 MTA: 1 | N/A | N/A | N/A |
| Sankhla et al. [20] 2021 | EEA: 21/24 MTA: 32/38 | N/A | EEA: 19/21 MTA: 23/33 | EEA: 9 MTA: 1 | EEA: 0 MTA: 1 | EEA: 0 MTA: 8 | N/A | EEA: 3 MTA: 4 |
| Alam et al. [1] 2022 | EEA: 3/5 MTA: 24/29 | N/A | EEA: 4/5 MTA: 25/29 | EEA: 1 MTA: 2 | EEA: 1 MTA: 5 | N/A | N/A | N/A |
| Qian et al. [19] 2022 | EEA: 31/34 MTA: 67/78 | N/A | EEA: 27/29 MTA: 47/63 | EEA: 4 MTA: 0 | EEA: 3 MTA: 2 | N/A | EEA: 1 MTA: 2 | EEA: 7 MTA: 15 |
| Li et al. [16] 2022 | EEA: 6/7 MTA: 27/31 | EEA: 0/6 MTA: 0/27 | EEA: 4/5 MTA: 15/27 | N/A | N/A | N/A | N/A | N/A |
| Silvestri et al. [21] 2023 | EEA: N/A MTA: 1/1 | N/A | EEA: 1/1 MTA: 1/1 | N/A | N/A | N/A | N/A | N/A |
| Jiang et al. [12] 2023 | EEA: 18/19 MTA: 16/17 | EEA: 0/18 MTA: 0/16 | EEA: 16/19 MTA: 12/17 | EEA: 3 MTA: 0 | EEA: 0 MTA: 0 | EEA: 0 MTA: 1 | EEA: 0 MTA: 0 | N/A |
| Feng et al. [11] 2023 | EEA: 41/45 MTA: 34/39 | N/A | EEA: 35/38 MTA: 28/33 | EEA: 1 MTA: 0 | N/A | N/A | N/A | EEA: 7 MTA: 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agosti, E.; Alexander, A.Y.; Antonietti, S.; Zeppieri, M.; Piazza, A.; Panciani, P.P.; Fontanella, M.M.; Pinheiro-Neto, C.; Ius, T.; Peris-Celda, M. Comparative Efficacy of Transsphenoidal and Transcranial Approaches for Treating Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 2356. https://doi.org/10.3390/jcm13082356
Agosti E, Alexander AY, Antonietti S, Zeppieri M, Piazza A, Panciani PP, Fontanella MM, Pinheiro-Neto C, Ius T, Peris-Celda M. Comparative Efficacy of Transsphenoidal and Transcranial Approaches for Treating Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(8):2356. https://doi.org/10.3390/jcm13082356
Chicago/Turabian StyleAgosti, Edoardo, A. Yohan Alexander, Sara Antonietti, Marco Zeppieri, Amedeo Piazza, Pier Paolo Panciani, Marco Maria Fontanella, Carlos Pinheiro-Neto, Tamara Ius, and Maria Peris-Celda. 2024. "Comparative Efficacy of Transsphenoidal and Transcranial Approaches for Treating Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 8: 2356. https://doi.org/10.3390/jcm13082356
APA StyleAgosti, E., Alexander, A. Y., Antonietti, S., Zeppieri, M., Piazza, A., Panciani, P. P., Fontanella, M. M., Pinheiro-Neto, C., Ius, T., & Peris-Celda, M. (2024). Comparative Efficacy of Transsphenoidal and Transcranial Approaches for Treating Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(8), 2356. https://doi.org/10.3390/jcm13082356