
Machine Learning Prediction of Tongue Pressure in Elderly Patients with Head and Neck Tumor: A Cross-Sectional Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Eligibility
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Study Design
2.4. Statistical Analysis
- “max_depth”: 2,3,4,5,6,8,10,20
- “min_samples_split”: 2,3,5
- “n_estimators”: 10,20,30,50
- “max_features”: ‘sqrt’, ‘log2’
- “criterion”: “gini”, “entropy”
- “max_depth: 2,3,5,10
- “booster”: ‘gbtree’,’gblinear’
- “learning_rate”: 0.01,0.1,0.3,0.5
- “n_estimators”: 10,20,30,50
- “gamma”: 0,0.3,1.0
- “reg_lambda”: 0,0.3,0.8,1
- “reg_alpha”: 0,0.3,0.8,1
- “silent”: 1.
2.5. Evaluation of Sample Size
3. Results
4. Discussion
5. Conclusions
- In patients with head and neck tumors aged 65 years or older, the MTP was significantly influenced by factors such as glossectomy, functional teeth, and age, according to the LR model.
- The LR model demonstrated a superior performance relative to the other two models evaluated in a small sample size, indicating the feasibility and applicability of machine learning techniques in predicting tongue pressure outcomes.
- The presence of natural teeth and tumor sites located in the tongue emerged as consistent factors across all four models that influenced MTP, suggesting their potential utility as an early predictive marker for diminished tongue pressure.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoshida, M.; Hiraoka, A.; Takeda, C.; Mori, T.; Maruyama, M.; Yoshikawa, M.; Tsuga, K. Oral Hypofunction and Its Relation to Frailty and Sarcopenia in Community-Dwelling Older People. Gerodontology 2022, 39, 26–32. [Google Scholar] [CrossRef]
- Morimata, J.; Otomaru, T.; Murase, M.; Haraguchi, M.; Sumita, Y.; Taniguchi, H. Investigation of Factor Affecting Health-Related Quality of Life in Head and Neck Cancer Patients. Gerodontology 2013, 30, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, A.; Murase, M.; Sumita, Y.I.; Taniguchi, H. Investigation of Nutritional Status Using the Mini Nutritional Assessment-Short Form and Analysis of the Relevant Factors in Patients with Head and Neck Tumour. Gerodontology 2017, 34, 227–231. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral Hypofunction in the Older Population: Position Paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Izumi, M.; Akifusa, S. Tongue Cleaning in the Elderly and Its Role in the Respiratory and Swallowing Functions: Benefits and Medical Perspectives. J. Oral. Rehabil. 2021, 48, 1395–1403. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, I.; Igarashi, K.; Imamura, Y.; Müller, F.; Abou-Ayash, S.; Schimmel, M. Variability in Tongue Pressure among Elderly and Young Healthy Cohorts: A Systematic Review and Meta-Analysis. J. Oral. Rehabil. 2021, 48, 430–448. [Google Scholar] [CrossRef] [PubMed]
- Fujikawa, N.; Ogino, Y.; Koga, S.; Ueno, M.; Moroi, R.; Koyano, K. Validation of Masticatory Function and Related Factors in Maxillectomy Patients Based on the Concept of “Oral Hypofunction”: A Retrospective Cross-Sectional Study. J. Prosthodont. Res. 2021, 65, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, Y.; Oyama, G.; Umeda, M.; Funahara, M.; Soutome, S.; Nakamura, W.; Kojima, Y.; Iwai, H. Effect of Decreased Tongue Pressure on Dysphagia and Survival Rate in Elderly People Requiring Long-Term Care. J. Dent. Sci. 2022, 17, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, M.; Kosaka, T.; Kida, M.; Fushida, S.; Kasakawa, N.; Fusayama, A.; Akema, S.; Hasegawa, D.; Hishida, E.; Ikebe, K. Factors Related to Masticatory Performance in Patients with Removable Dentures for Jaw Defects Following Oral Tumor Surgery. J. Prosthodont. Res. 2023, 67, 583–587. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Sugahara, K.; Fukuoka, T.; Saito, S.; Sakuramoto, A.; Horii, N.; Sano, S.; Hasegawa, K.; Nakao, Y.; Nanto, T.; et al. Change in Tongue Pressure in Patients with Head and Neck Cancer after Surgical Resection. Odontology 2017, 105, 494–503. [Google Scholar] [CrossRef]
- Nakamori, M.; Imamura, E.; Fukuta, M.; Tachiyama, K.; Kamimura, T.; Hayashi, Y.; Matsushima, H.; Ogawa, K.; Nishino, M.; Hirata, A.; et al. Tongue Thickness Measured by Ultrasonography Is Associated with Tongue Pressure in the Japanese Elderly. PLoS ONE 2020, 15, e0230224. [Google Scholar] [CrossRef] [PubMed]
- De Groot, R.J.; Merkx, M.A.W.; Hamann, M.N.S.; Brand, H.S.; de Haan, A.F.J.; Rosenberg, A.J.W.P.; Speksnijder, C.M. Tongue Function and Its Influence on Masticatory Performance in Patients Treated for Oral Cancer: A Five-Year Prospective Study. Support. Care Cancer 2020, 28, 1491–1501. [Google Scholar] [CrossRef] [PubMed]
- Arakawa-Kaneko, I.; Watarai, Y.; Schimmel, M.; Abou-Ayash, S. Relationship between Tongue Pressure and Handgrip Strength: A Systematic Review and Meta-Analysis. J. Oral. Rehabil. 2022, 49, 1087–1105. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, K.; Soutome, S.; Funahara, M.; Kawashita, Y.; Kitamura, M.; Fukuda, H.; Furugen, R.; Iwasaki, T.; Hayashida, H.; Kawasaki, K.; et al. The Relationship between Dental Findings and Tongue Pressure: A Survey of 745 Community-Dwelling Adults and Elderly Persons in Japan. Gerontology 2021, 67, 517–524. [Google Scholar] [CrossRef]
- Hu, X.-Y.; Liu, H.; Zhao, X.; Sun, X.; Zhou, J.; Gao, X.; Guan, H.-L.; Zhou, Y.; Zhao, Q.; Han, Y.; et al. Automated Machine Learning-Based Model Predicts Postoperative Delirium Using Readily Extractable Perioperative Collected Electronic Data. CNS Neurosci. Ther. 2022, 28, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing Different Supervised Machine Learning Algorithms for Disease Prediction. BMC Med. Inform. Decis. Mak. 2019, 19, 281. [Google Scholar] [CrossRef] [PubMed]
- Christodoulou, E.; Ma, J.; Collins, G.S.; Steyerberg, E.W.; Verbakel, J.Y.; Van Calster, B. A Systematic Review Shows No Performance Benefit of Machine Learning over Logistic Regression for Clinical Prediction Models. J. Clin. Epidemiol. 2019, 110, 12–22. [Google Scholar] [CrossRef]
- Ali, I.E.; Tanikawa, C.; Chikai, M.; Ino, S.; Sumita, Y.; Wakabayashi, N. Applications and Performance of Artificial Intelligence Models in Removable Prosthodontics: A Literature Review. J. Prosthodont. Res. 2023, JPR_D_23_00073. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.; Sherif, A.A.; Jin, C.; Chen, Y.; Cai, P.; Li, P. Machine Learning Predicting Mortality in Sarcoidosis Patients Admitted for Acute Heart Failure. Cardiovasc. Digit. Health J. 2022, 3, 297–304. [Google Scholar] [CrossRef]
- Cui, Y.; Shi, X.; Wang, S.; Qin, Y.; Wang, B.; Che, X.; Lei, M. Machine Learning Approaches for Prediction of Early Death among Lung Cancer Patients with Bone Metastases Using Routine Clinical Characteristics: An Analysis of 19,887 Patients. Front. Public Health 2022, 10, 1019168. [Google Scholar] [CrossRef]
- Wang, Y.; Miao, X.; Xiao, G.; Huang, C.; Sun, J.; Wang, Y.; Li, P.; You, X. Clinical Prediction of Heart Failure in Hemodialysis Patients: Based on the Extreme Gradient Boosting Method. Front. Genet. 2022, 13, 889378. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Cao, Y.; Cao, X.; Shi, X.; Lei, M.; Su, X.; Liu, Y. Machine Learning-Based Algorithms to Predict Severe Psychological Distress among Cancer Patients with Spinal Metastatic Disease. Spine J. 2023, 23, 1255–1269. [Google Scholar] [CrossRef] [PubMed]
- Tseng, Y.-J.; Wang, Y.-C.; Hsueh, P.-C.; Wu, C.-C. Development and Validation of Machine Learning-Based Risk Prediction Models of Oral Squamous Cell Carcinoma Using Salivary Autoantibody Biomarkers. BMC Oral Health 2022, 22, 534. [Google Scholar] [CrossRef] [PubMed]
- Tehrany, P.M.; Zabihi, M.R.; Ghorbani Vajargah, P.; Tamimi, P.; Ghaderi, A.; Norouzkhani, N.; Zaboli Mahdiabadi, M.; Karkhah, S.; Akhoondian, M.; Farzan, R. Risk Predictions of Hospital-acquired Pressure Injury in the Intensive Care Unit Based on a Machine Learning Algorithm. Int. Wound J. 2023, 20, 3768–3775. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Hara, K.; Nakagawa, K.; Yoshimi, K.; Ariya, C.; Nakane, A.; Furuya, J.; Tohara, H. Ultrasonography Shows Age-Related Changes and Related Factors in the Tongue and Suprahyoid Muscles. J. Am. Med. Dir. Assoc. 2021, 22, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Rong, P. A Novel Hierarchical Framework for Measuring the Complexity and Irregularity of Multimodal Speech Signals and Its Application in the Assessment of Speech Impairment in Amyotrophic Lateral Sclerosis. J. Speech Lang. Hear. Res. 2021, 64, 2996–3014. [Google Scholar] [CrossRef] [PubMed]
- Sawaya, Y.; Ishizaka, M.; Kubo, A.; Shiba, T.; Sato, T.; Onoda, K.; Maruyama, H.; Urano, T. Absolute Reliability of Tongue Pressure Measurement in Young Healthy Adults and Elderly Patients with Certification of Needing Long-Term Care or Support. Geriatr. Gerontol. Int. 2020, 20, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, Y.; Ji, X.; Wang, Z. Effective Macrosomia Prediction Using Random Forest Algorithm. Int. J. Environ. Res. Public Health 2022, 19, 3245. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Yang, F.; Ma, F. An Efficient Model Selection for Linear Discriminant Function-Based Recursive Feature Elimination. J. Biomed. Inform. 2022, 129, 104070. [Google Scholar] [CrossRef]
- Rajput, D.; Wang, W.-J.; Chen, C.-C. Evaluation of a Decided Sample Size in Machine Learning Applications. BMC Bioinform. 2023, 24, 48. [Google Scholar] [CrossRef]
- Suzuki, H.; Ayukawa, Y.; Ueno, Y.; Atsuta, I.; Jinnouchi, A.; Koyano, K. Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly. Medicina 2020, 56, 623. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Tai, J.; Hu, R.; Fan, S.; Li, H.; Zhu, Y.; Wu, Y.; Wu, J. Effect of Tongue-Pressure Resistance Training in Poststroke Dysphagia Patients With Oral Motor Dysfunction. Am. J. Phys. Med. Rehabil. 2022, 101, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Endo, Y.; Nishimura, R.; Masuda, S.; Amano, J.; Tsuga, K. Palatal Augmentation Prosthesis (PAP) Can Improve Swallowing Function for the Patients in Rehabilitation Hospital. J. Prosthodont. Res. 2019, 63, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-Y.; Chen, J.-H.; Hsu, K.-J.; Yao, C.-T.; Chen, P.-H.; Hsiao, S.-Y.; Lin, C.-L. Decreased Tongue Pressure Associated with Aging, Chewing and Swallowing Difficulties of Community-Dwelling Older Adults in Taiwan. J. Pers. Med. 2021, 11, 653. [Google Scholar] [CrossRef] [PubMed]
- Satake, A.; Kobayashi, W.; Tamura, Y.; Oyama, T.; Fukuta, H.; Inui, A.; Sawada, K.; Ihara, K.; Noguchi, T.; Murashita, K.; et al. Effects of Oral Environment on Frailty: Particular Relevance of Tongue Pressure. Clin. Interv. Aging 2019, 14, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Ciciliot, S.; Rossi, A.C.; Dyar, K.A.; Blaauw, B.; Schiaffino, S. Muscle Type and Fiber Type Specificity in Muscle Wasting. Int. J. Biochem. Cell Biol. 2013, 45, 2191–2199. [Google Scholar] [CrossRef]
- Namiki, C.; Hara, K.; Yanagida, R.; Nakagawa, K.; Yamaguchi, K.; Okumura, T.; Tamai, T.; Kurosawa, Y.; Komatsu, T.; Tohara, H. Association between Tongue Pressure and Jaw-Opening Force in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 9825. [Google Scholar] [CrossRef]
- Hamahata, A.; Beppu, T.; Shirakura, S.; Hatanaka, A.; Yamaki, T.; Saitou, T.; Sakurai, H. Tongue Pressure in Patients with Tongue Cancer Resection and Reconstruction. Auris Nasus Larynx 2014, 41, 563–567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Total number of patients | 80 |
| Primary tumor site | |
| Maxilla (%) | 29 (36) |
| Mandible (%) | 31 (39) |
| Tongue (%) | 20 (25) |
| Age (years) | 71.98 ± 6.32 |
| Sex | |
| Male (%) | 42 (53) |
| Female (%) | 38 (47) |
| Number of teeth present | 17.05 ± 6.73 |
| Occlusal units (natural teeth) | 5.8 ± 3.98 |
| Occlusal units (with denture) | 12.93 ± 1.44 |
| Functional teeth | 26.58 ± 2.02 |
| Reconstruction | |
| Flap reconstruction (%) | 37 (46) |
| Bone and/or metal plate reconstruction (%) | 20 (25) |
| Perforation in maxilla (%) | 16 (20) |
| None (%) | 7 (9) |
| MTP ≥ 20 kPa (%) | 43 (54) |
| MTP < 20 kPa (%) | 37 (46) |
| Model | Accuracy | F1 Score | Precision | Recall | AUC |
|---|---|---|---|---|---|
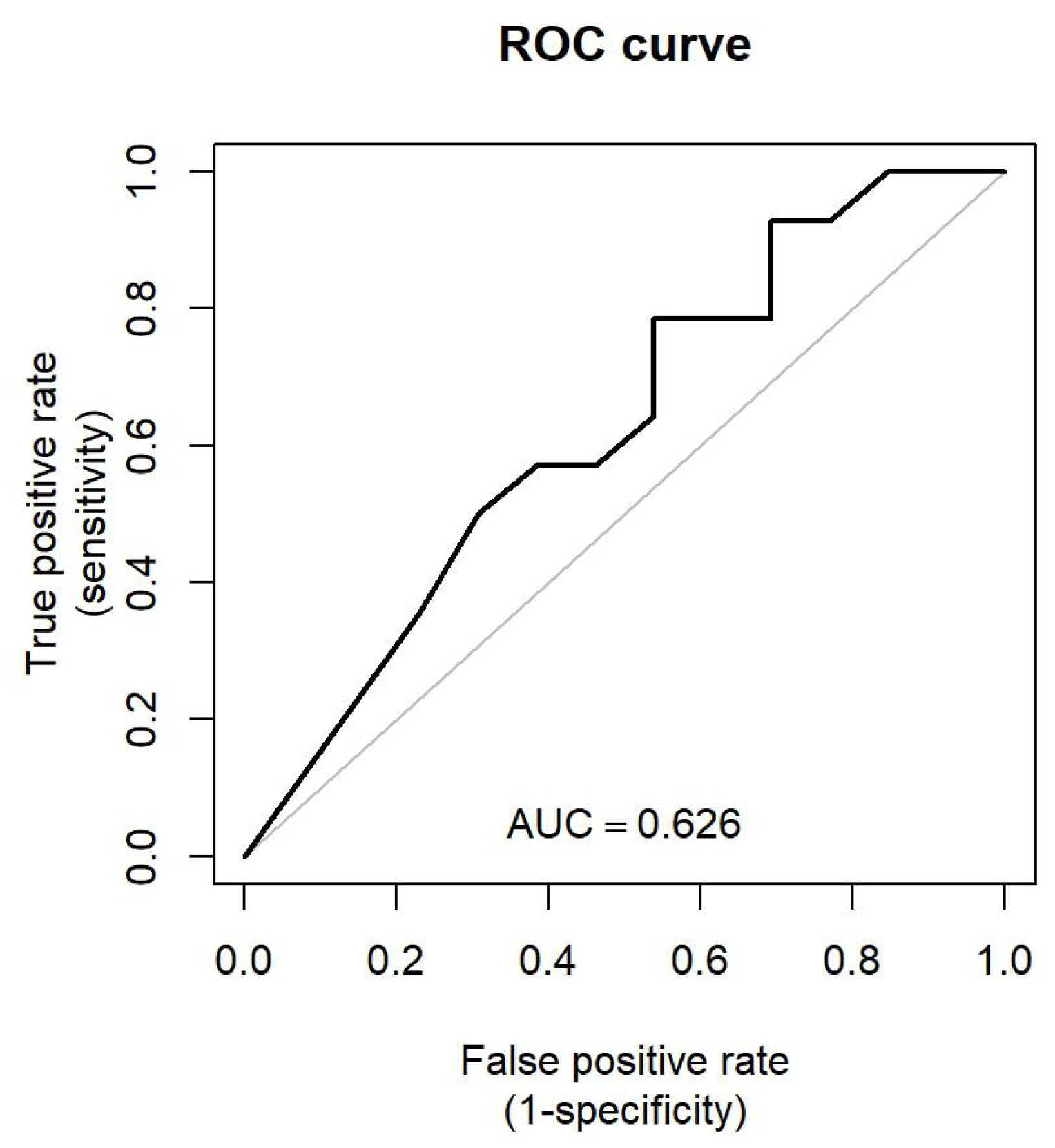
| LR | 0.630 [95% confidence interval (CI): 0.370–0.778] | 0.688 [95% confidence interval (CI): 0.435–0.853] | 0.611 [95% confidence interval (CI): 0.313–0.801] | 0.786 [95% confidence interval (CI): 0.413–0.938] | 0.626 [95% confidence interval (CI): 0.409–0.806] |
| SVM | 0.593 [95% confidence interval (CI): 0.370–0.741] | 0.645 [95% confidence interval (CI): 0.400–0.811] | 0.588 [95% confidence interval (CI): 0.301–0.800] | 0.714 [95% confidence interval (CI): 0.385–0.889] | 0.582 [95% confidence interval (CI): 0.390–0.761] |
| RF | 0.556 [95% confidence interval (CI): 0.370–0.741] | 0.571 [95% confidence interval (CI): 0.320–0.762] | 0.571 [95% confidence interval (CI): 0.294–0.833] | 0.571 [95% confidence interval (CI): 0.308–0.846] | 0.626 [95% confidence interval (CI): 0.385–0.843] |
| XGB | 0.630 [95% confidence interval (CI): 0.444–0.815] | 0.667 [95% confidence interval (CI): 0.435–0.833] | 0.625 [95% confidence interval (CI): 0.375–0.857] | 0.714 [95% confidence interval (CI): 0.462–0.929] | 0.618 [95% confidence interval (CI): 0.405–0.826] |
| Variables | β Coefficient | p-Value |
|---|---|---|
| Glossectomy | −2.059 | 0.039 * |
| Functional teeth | −4.251 | 0.043 * |
| Age | 1.674 | 0.044 * |
| Occlusal units with denture | 4.166 | 0.052 |
| Occlusal units without denture | 2.405 | 0.150 |
| Male sex | 0.731 | 0.221 |
| Hard tissue reconstruction | 1.174 | 0.252 |
| Tongue cancer | −0.263 | 0.750 |
| Soft tissue reconstruction | 0.198 | 0.811 |
| Presence of teeth | −0.179 | 0.901 |
| Glossectomy | −0.206 | 0.993 |
| Perforation | −9.306 | 0.994 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, X.; Bai, Z.; Mogushi, K.; Hase, T.; Takeuchi, K.; Iida, Y.; Sumita, Y.I.; Wakabayashi, N. Machine Learning Prediction of Tongue Pressure in Elderly Patients with Head and Neck Tumor: A Cross-Sectional Study. J. Clin. Med. 2024, 13, 2363. https://doi.org/10.3390/jcm13082363
Han X, Bai Z, Mogushi K, Hase T, Takeuchi K, Iida Y, Sumita YI, Wakabayashi N. Machine Learning Prediction of Tongue Pressure in Elderly Patients with Head and Neck Tumor: A Cross-Sectional Study. Journal of Clinical Medicine. 2024; 13(8):2363. https://doi.org/10.3390/jcm13082363
Chicago/Turabian StyleHan, Xuewei, Ziyi Bai, Kaoru Mogushi, Takeshi Hase, Katsuyuki Takeuchi, Yoritsugu Iida, Yuka I. Sumita, and Noriyuki Wakabayashi. 2024. "Machine Learning Prediction of Tongue Pressure in Elderly Patients with Head and Neck Tumor: A Cross-Sectional Study" Journal of Clinical Medicine 13, no. 8: 2363. https://doi.org/10.3390/jcm13082363
APA StyleHan, X., Bai, Z., Mogushi, K., Hase, T., Takeuchi, K., Iida, Y., Sumita, Y. I., & Wakabayashi, N. (2024). Machine Learning Prediction of Tongue Pressure in Elderly Patients with Head and Neck Tumor: A Cross-Sectional Study. Journal of Clinical Medicine, 13(8), 2363. https://doi.org/10.3390/jcm13082363