Abstract
Background/Objectives: Brodalumab is a monoclonal antibody against the anti-IL-17 receptor A, approved for patients with moderate-to-severe psoriasis. This retrospective study investigated patients in clinical practice to assess the impact of body weight and previous treatments with biologics on the effectiveness of brodalumab. Methods: Patients were treated according to clinical practice, and assessed at baseline, 16, 36 and 52 weeks by means of the Psoriasis Area Severity Index (PASI) and DLQI score. Overall, 299 patients were included (147 naïve to biologics). Results: Mean PASI was significantly reduced compared with the baseline in the overall population by week 4 and continued to decrease at each study time point (15.9 ± 7.9 at baseline, 5.4 ± 5.3 at week 4, 1.9 ± 3.6 at week 6, 1.0 ± 2.1 at week 36, and 0.8 ± 2.1 at week 52; p < 0.001 at each control). PASI improved significantly both in bio-naïve and bio-experienced patients (p < 0.001). The proportions of patients achieving PASI 75, PASI 90, and PASI 100 were comparable between the bio-naïve and bio-experienced groups at all time points. The percentages of patients who achieved PASI 75 were similar in obese and non-obese subjects at all determinations except the visit performed after 36 weeks of treatment (94.3% non-obese vs. 83.1% obese, p = 0.005). PASI 90 was achieved more frequently among non-obese patients than obese patients after 36 weeks (80.7% vs. 64.4%, p = 0.008) and 52 weeks of treatment (84.1% vs. 71.7%, 0.027). The probability of achieving PASI 75 and PASI 100 was independent of nutritional status at any time during the study. Conclusions: In conclusion, our results confirm that brodalumab has both rapid and sustained effectiveness in patients with moderate-to-severe psoriasis; our results could be extended to patients with multiple risk factors impairing treatment response, such as multiple biological failure and obesity.
1. Introduction
Plaque psoriasis is a prevalent, chronic inflammatory disease, characterized by cutaneous scaly erythematous plaques and patches typically located on the extensor surfaces, such as elbows, knees, and the lumbosacral area [1]. Plaque psoriasis carries a great disease burden due to discomfort, itching, and disfigurement, with consequent quality of life impairment and emotional issues. Additionally, it is associated with several systemic comorbidities, including psoriatic arthritis, cardiovascular diseases, diabetes, depression, and inflammatory bowel disease. Indeed, evidence from experimental and clinical studies has shown that psoriasis is a systemic condition linked to chronic inflammation [2]. Interestingly, the prevalence and severity of psoriasis appears to be associated with increased BMI [3,4]. In line with this correlation, obesity should be taken into consideration when therapies are prescribed. For example, since obese patients need higher doses of antipsoriatic drugs in comparison to non-obese patients, they suffer more complications due to adverse effects [5,6]. The goal of treatment is to manage skin lesions and enhance quality of life. While mild cases are typically controlled with topical treatments, moderate-to-severe cases require systemic therapy. Importantly, treatments should be considered based on the patient characteristics, such as comorbidities and body weight [7]. Moreover, multi-failure patients, i.e., patients who have failed multiple biologic drugs [8], have been considered. The choice of systemic treatments depends on the severity, previous therapy, comorbidities, the involvement of difficult to treat areas, and the patient’s medical history. Among the available systemic agents, the new interleukin (IL) inhibitors are highly effective and generally have a better safety profile than traditional systemic therapies [9,10]. A review of phase III clinical trials for three of the IL-17 inhibitors (secukinumab, ixekizumab, and brodalumab) highlighted that IL-17 inhibitors are effective therapeutic options for psoriasis patients [11]. Interestingly, it has recently been reported in an observation retrospective cohort study that IL-17 inhibitors appear to be more effective in decreasing systemic inflammatory markers in moderate-to-severe psoriasis in comparison to IL-23 inhibitors [12,13]. Brodalumab is a fully human monoclonal antibody against the anti-IL-17 receptor A, a key player of the th-17 axis widely involved in the psoriasis pathogenesis [2]. Brodalumab is approved in the EU for treating moderate-to-severe psoriasis in patients who are candidates for systemic therapy (SmPC Kyntheum) and in the USA for inadequate responders to other systemic therapies (SmPC Siliq). Phase II and phase III placebo-controlled clinical trials (AMAGINE-1/-2/-3) demonstrated its efficacy in patients with plaque psoriasis for up to 1 year, with superiority over ustekinumab in a head-to-head comparison and a favorable safety profile [14,15,16,17]. A post-hoc pooled analysis of AMAGINE-2 and AMAGINE-3 showed that the efficacy of brodalumab was maintained up to week 120 [18,19]. Real-life studies in patients with moderate-to-severe psoriasis, albeit with varying designs and endpoints, have shown brodalumab to produce a rapid response and long-term effectiveness up to 3 years, with a high probability of prolonged drug survival and improved quality of life [15,16,20,21,22,23]. A recent report of 5-year pharmacovigilance data confirmed the safety profile of brodalumab as demonstrated by clinical trials and previous reports [24]. Our study aimed to confirm the effectiveness and safety of brodalumab in a large real-world cohort including patients with previous biologic failures and severe body weight abnormalities.
2. Materials and Methods
A retrospective observational study was performed between May 2023 and June 2024 in 41 dermatological centers in Italy. Patients with moderate-to-severe plaque psoriasis treated with brodalumab were enrolled. Psoriasis was considered moderate-to-severe based on the presence of a Psoriasis Area Severity Index (PASI) ≥ 10 or less if the involvement of difficult-to-treat areas (face, palms/soles, genitalia, nails) was present. Brodalumab was administered in accordance with the Italian Guidelines for managing plaque psoriasis [25] and the summary of product characteristics in adult patients who were candidates for systemic treatments [26]. The recommended dose is 210 mg administered by subcutaneous injection at weeks 0, 1, and 2 followed by 210 mg every 2 weeks. Importantly, all patients received brodalumab as monotherapy and no concomitant systemic or topical therapies were used during the study. Institutional review board approval was waived for this study, as the procedures adopted did not deviate from standard clinical practice. All patients provided written informed consent to have their data collected during routine clinical practice, i.e., demographics and clinical parameters, included in this retrospective study, for the retrospective retrieval of anonymized data. The study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments. Data collection and management observed the applicable rules, regulations, and directives concerning patient protection, such as patient privacy.
2.1. Data Collection
Clinical and demographic data collected at baseline included age, sex, disease duration, body mass index (BMI), comorbidities, previous exposure to biologic drugs, and the involvement of difficult-to-treat areas (scalp/face, palms/soles, genitalia, and nails). Baseline patients’ nutritional status was assessed and classified according to WHO recommendations. At baseline and at each scheduled time point (4, 16, 36, and 52 weeks), the following clinical parameters were measured: PASI, PASI improvements of 75%, 90%, and 100%, and Dermatology Life Quality Index (DLQI). For patients who missed scheduled dermatological visits or skipped the dose, the last-observation-carried-forward method was applied. At each visit, the occurrence of any adverse events (AEs; Table S1) was recorded, including serious AEs and those leading to brodalumab discontinuation.
2.2. Statistical Analysis
Data were summarized by means of descriptive analysis. Means and standard deviations (SDs) were calculated for continuous variables, while absolute values and frequency (%) were calculated for categorical variables. A t-test or analysis of variance was performed to compare mean values, while a paired t-test compared mean values at different time points. The chi-squared test was used to compare frequencies. The statistical significance was defined as p < 0.05. All analyses were performed with IBM SPSS Statistics for Windows, Version 26.0.
3. Results
3.1. Patients’ Characteristics
The baseline demographic and clinical characteristics of patients are summarized in Table 1. Overall, 299 patients were included, 198 (66.2%) of whom were males; 63 (21.4%) were obese (BMI > 30) and 124 (42.2%) were overweight (BMI between 25 and 30).

Table 1.
Clinical and demographic characteristics at baseline.
Forty-four patients (14.7%) had joint involvement classified as psoriatic arthritis. The mean BMI was 26.6 ± 5.5 kg/m2. The mean duration of psoriasis was 18.1 ± 12.5 years, the mean PASI value was 15.9 ± 7.9 at baseline, and 267 (89.6%) patients exhibited difficult-to-treat areas involved.
Overall, 147 (49.2%) patients were naïve to biologic agents, and 52 (17.4%) were naïve to any systemic treatments for psoriasis. Among the 152 patients who previously received biologic therapies, 46 (30.3%) were treated with more than one agent. The last biologic preferentially used before brodalumab was adalimumab (n = 48, 31.6%) (Table 1). There were no relevant differences in demographic characteristics between patients naïve to biologics and bio-experienced patients. The baseline PASI score was 17.3 ± 8.2 in bio-naïve patients and 14.7 ± 7.4 in bio-experienced patients (p = 0.004).
3.2. Effectiveness
- Overall population
The PASI score improved significantly when compared with the baseline in the study population by week 4 and continued to decrease during the study follow-up (15.9 ± 7.9 at baseline, 5.4 ± 5.3 at week 4, 1.9 ± 3.6 at week 6, 1.0 ± 2.1 at week 36, and 0.8 ± 2.1 at week 52; p < 0.001). PASI 75 was achieved by 131/299 (43.8%) patients at week 4, 233/297 (78.5%) patients at week 16, and 268/292 (91.8%) at week 36; this proportion was maintained at 52 weeks. PASI 90 was reached by 60/299 (20.1%) patients at week 4, 194/297 (65.3%) at week 16, 225/292 (77.1%) at week 36, and 238/292 (81.5%) at week 52. A complete skin clearance, defined as PASI 100, was observed in 45/299 (15.1%) patients at week 4, 163/297 (54.9%) patients at week 16, 183/292 (62.7%) at week 36, and 204/292 (69.9%) at week 52 (Table 2). The PASI score was ≤2 in 99/297 (33.1%) at week 4, 214/292 (72.1%) at week 16, 257/292 (88.0%) at week 36, and 263/299 (90.1%) at week 52.
Table 2.
Proportion of patients achieving PASI 75, 90, and 100 during the study follow-up.
The speed of action and the consistent effectiveness of brodalumab on the skin were accompanied by a clear improvement in patients’ quality of life. The mean DLQI score decreased at 4.8 ± 5 at week 4, 2.0 ± 3.4 at week 16, 1.3 ± 3.3 at week 36 and 1.0 ± 3.0 at week 52 with only one patient scoring > 21 after 1 year of treatment.
- Impact of previous biologics
In both bio-naïve and bio-experienced patients, a significant improvement in PASI score was observed throughout the study. The mean PASI for bio-naïve patients decreased from 17.3 ± 8.2 at baseline to 1.0 ± 2.5 at 52 weeks, with a significant reduction noted at 4 weeks (5.6 ± 5.5), 16 weeks (2.0 ± 3.6), and 36 weeks (1.1 ± 2.4) (p < 0.001). Bio-experienced patients’ PASI improved to 0.7 ± 1.6 at 52 weeks, with mean PASI scores of 5.2 ± 5.1 at 4 weeks, 1.9 ± 3.6 at 16 weeks, and 0.9 ± 1.8 at 36 weeks (p < 0.001 at all time points). Although baseline PASI was significantly higher in naïve patients vs. experienced patients, the same difference was not observed during the follow-up time points. The trend in PASI 75, 90, and 100 achievement was comparable among bio-naïve and bio-experienced patients across all time-points. The percentage of patients reaching PASI ≤ 2 was high and similar among both groups at each scheduled visit (p-values > 0.46).
- Impact of body weight
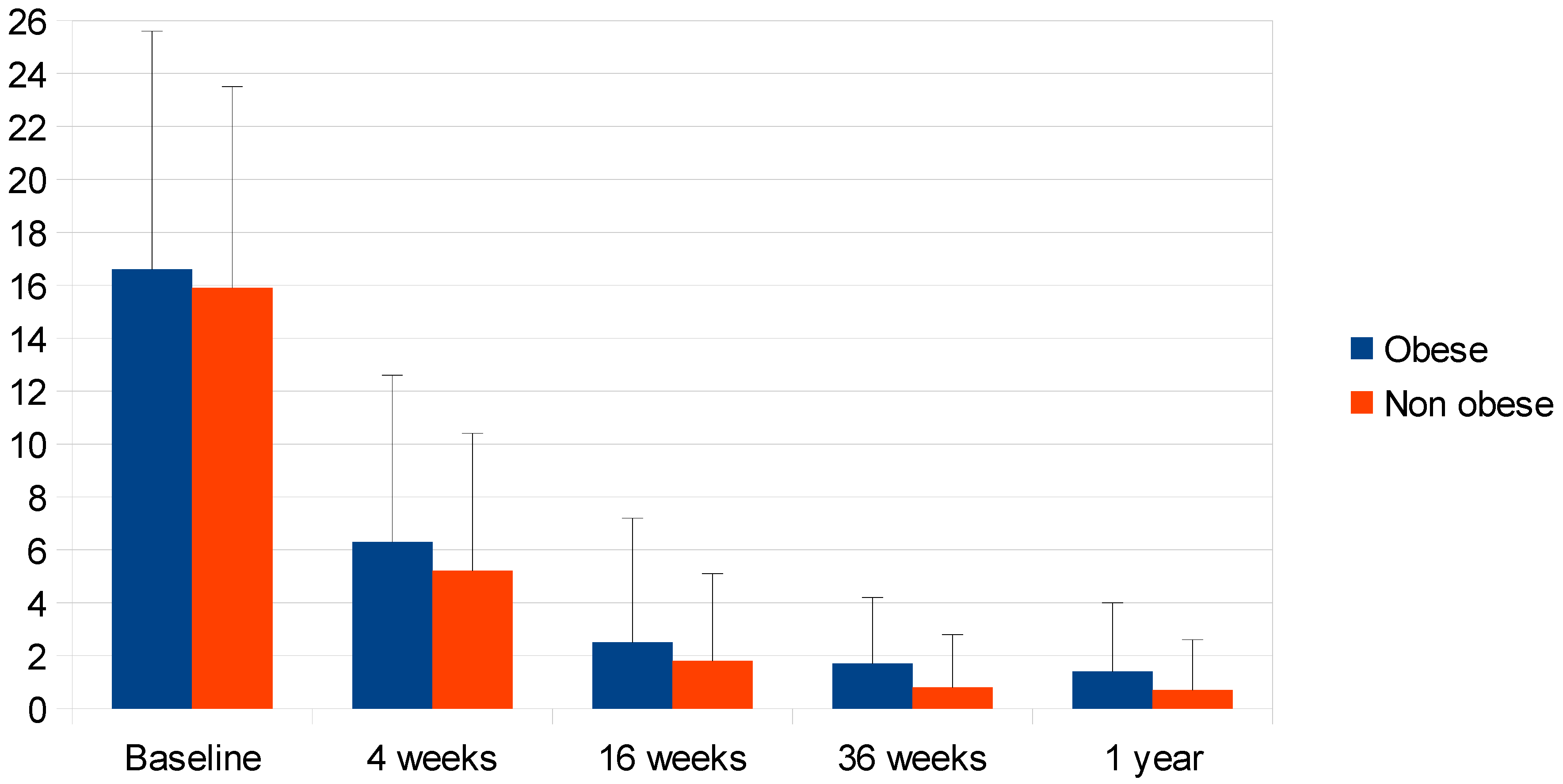
Mean PASI score did not differ significantly in obese patients (16.6 ± 9.0, n = 63) as compared with normal-weight and overweight non-obese patients (15.9 ± 7.6, n = 231) at baseline, nor after 4 and 16 weeks, but was significantly higher in obese patients after 36 weeks (1.7 ± 2.5 vs. 0.8 ± 2.0, p = 0.009) and after 52 weeks (1.4 ± 2.6 vs. 0.7 ± 1.9, p = 0.026). Nevertheless, PASI score reduction was significant at each follow-up visit for both obese and non-obese patients (p < 0.001 in both groups at each time point). Non-obese patients had a higher likelihood of PASI 75 achievement only at week 36 (94.3% of non-obese vs. 83.1% obese, p = 0.005), and of PASI 90 achievement at week 36 (80.7% vs. 64.4%, p = 0.008) and week 52 (84.1% vs. 71.7%, p = 0.027), while the probability of obtaining PASI 100 was similar at any time during the study follow-up (Table 3, Figure 1).
Table 3.
Mean PASI score in bio-naïve and bio-experienced, obese and non-obese patients from baseline to 1 year from the treatment.
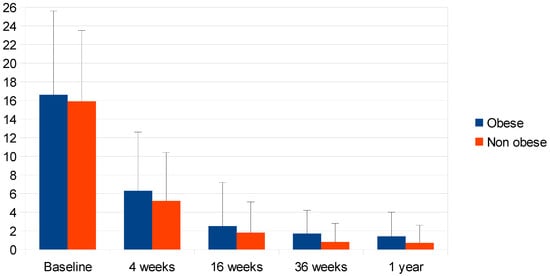
Figure 1.
Mean PASI of obese and non-obese patients from baseline to 1 year from the treatment, as shown in Table 3 (Mean ± SEM).
3.3. Safety
Overall, 15 (5.0%) patients experienced a total of 17 AEs during the observation period of treatment, including positivity of antinuclear antibodies, candidiasis of the oral cavity, non-specific colitis, lower limb edema, hypotension, maculopapular rash, epilepsy, non-specific diffuse erythema, fatigue, oral leucoplakia, and steatosis, each one occurring in one patient (5.9%), with the most frequent being the detection of latent tuberculosis (4/17; 23.5%) and the onset of conjunctivitis (2/17; 11.8%) (Table S1). Therapy was discontinued by 15 patients (5.0%) for various reasons [FIVET and pregnancy research (n = 3, 1.0%); loss of efficacy (n = 3, 1.0%); PSA worsening (n = 1, 0.3%); loss of joint efficacy (n = 1, 0.3%); patient lost at follow-up (n = 1, 0.3%); unknown (n = 1, 0.3%)], including AEs (edema of the lower limbs, hypotension, and maculopapular rash; fatigue; non-specific colitis; latent tuberculosis; leucoplakia) in 5/15 (1.7%) patients. Information on the timing of discontinuation was not available.
4. Discussion
This retrospective study in a real-life setting confirmed the rapid and sustained effectiveness of brodalumab up to 1 year of treatment in patients with moderate-to-severe psoriasis. A significant reduction in mean PASI score was obtained at 4 weeks, regardless of previous treatments with other biological agents and the presence of obesity; the improvement achieved was maintained in the overall cohort and in subgroups for up to 1 year. An improvement in quality of life was also observed. Both obese and non-obese patients obtained significant reductions of PASI and a similar probability of achieving PASI 100 during the follow-up. On the contrary, starting from week 36, the potential of obtaining a significant PASI improvement was influenced by obesity. Our results suggest that obese subjects and patients who have already failed treatment with a biologic agent may benefit from treatment with brodalumab as well as non-obese and bio-naïve ones. The efficacy data observed in this study are in agreement with data from clinical trials [27]. Real-world data are obtained in non-selected populations, including subjects with comorbidities and older age, and are liable to greater variability than clinical trial evidence. On the other hand, they better reflect clinical practice and provide information for clinical decisions in those conditions excluded from trials. Comparison with real-world studies is not direct, because different study designs are used, and the absence of a strict selection may introduce a number of biases. Nevertheless, data from real-world studies will help to optimize and customize the use of available drugs. The efficacy outcomes, in terms of probability of PASI 75, 90, and 100 achievement at 1 year, observed in our patients are similar to those obtained in a Polish register study (92.5% vs. 95.1%, 81.5% vs. 87.3%, and 69.9% vs. 69.7%, respectively) [20]. In both studies, PASI improvement was associated with an improvement in quality of life (DLQI score). Kojanova et al. also found that drug survival probability at 1 year was 84.2%, and that longer drug survival was associated with younger age, higher BMI, and no previous biologic treatment. Indeed, Caldarola et al. [28] found in an Italian retrospective study that higher BMI was predictive for treatment discontinuation, suggesting some difference between this population and the one observed by Kojanova et al. In a German study, the frequency of PASI 75, 90, and 100 increased from 3 months to 1 year of treatment (PASI 100, 37% at 3 months and 51.5% at 1 year), in agreement with our observations [PASI 100, 54.9 at 4 months and 69.9% at 1 year] [21]. A Greek group analyzed data based on the “as observed data”, reporting that 42% of patients obtained PASI 100 after 25.9 ± 3.5 weeks, and 65% of patients achieved PASI 100 at Week 104 [22]. This type of analysis can be particularly useful for supporting physicians in guiding patients’ expectations of treatment effects. Obesity in psoriasis patients is associated with increased skin lesion severity and reduced response to therapy [29]. These events are attributed to the low-level chronic inflammation observed in obese patients and characterized by the higher production of pro-inflammatory cytokines IL-23 and IL-17 [30,31]. Brodalumab, unlike other biologics, does not require dose adjustment based on body weight [32,33]. In a post-hoc analysis of AMAGINE-2 and AMAGINE-3, including patients with obesity (BMI ≥ 30 kg/m2) and without obesity (BMI < 30 kg/m2), the rates of PASI 75, PASI 90, and PASI 100 achieved with continuous treatment with brodalumab at week 12 were independent of obesity status (>97%, >74%, and >49%, respectively), and the differences between the groups were not significant at week 52 [33]. Our real-life observations confirm obesity does not affect brodalumab performance in psoriasis patients. Previous studies suggested that the efficacy of biologics may be reduced after the failure of previous biologics, although data are not always consistent [34,35]. In our experience, we observed that bio-experienced patients had similar improvement from brodalumab treatment compared to bio-naive ones. Limitations of this study include the observational design (which is inherent to a real-life study, and open to special considerations), the follow-up limited to one year, the retrospective design, and the absence of data on drug survival. Nevertheless, other studies have shown the long-term drug survival rate, e.g., a recent study by Mastorino and colleagues that reported the safety profile of brodalumab in a real-world setting for up to 3 years of treatment [36]. Concerning the sample size, it is necessary to underline that due to the retrospective and real-world design of this study, the sample was determined by the data available during the study period. Therefore, this determined the a priori sample size calculation. In addition, the study focused on ensuring the real-world population’s representativeness rather than using a prospective design. Therefore, despite the methodological limitation of retrospective studies, we believe that the findings are clinically meaningful and provide valuable insights applicable to daily practice. Indeed, these findings might be considered in clinical practice in the choice of the best treatment in case of patients for whom the standard therapies are not suitable, e.g., obese and multi-failure patients [8,27].
5. Conclusions
This observational study in a real-life setting confirms that brodalumab has a rapid onset of action and prolonged effectiveness in patients with moderate-to-severe psoriasis; these results may also be extended to subjects with risk factors for reduced response to biologic treatment, such as previous biologic failures and obesity.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm14041087/s1, Table S1: Adverse events.
Author Contributions
Conceptualization, D.O. and D.G.; Validation, D.O., D.G., M.B., A.C. (Anna Campanati), E.C., C.G., A.N., P.P., P.R., M.T., L.Z., L.M.H.A., G.B., R.B., T.B., L.B., A.M.G.B., A.E.C., G.C. (Giacomo Caldarola), G.C. (Gianluca Calianno), A.C. (Anton Carpentieri), M.C., A.C. (Andrea Carugno), F.C., A.C. (Antonio Costanzo), E.C.C., G.D.B., G.C.L.D., A.D., M.D., E.D.C., M.E., C.S.F., M.G., F.G., G.L., M.L., A.L., P.M., F.M., G.M., A.M. (Andrea Muracchioli), A.M. (Attilia Musumeci), M.L.M., G.P., V.P., L.P., E.P., M.R., O.S., D.S., F.V. and M.C.F.; Writing—original draft, D.O., D.G. and M.C.F.; Writing—review & editing, D.O. and M.C.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Institutional review board approval was exempted for this study as its procedure did not deviate from good routine clinical practice. The study was conducted in accordance with the Helsinki Declaration of 1964 and its later amendments.
Informed Consent Statement
All patients gave written informed consent to the publication of anonymized data.
Data Availability Statement
Additional data supporting the findings of this study are available from the Corresponding Author on reasonable request.
Acknowledgments
Editorial assistance was provided by Valentina Mirisola and Laura Brogelli (Polistudium, Milan, Italy).
Conflicts of Interest
D. Orsini has been a speaker and/or consultant for Abbvie, LeoPharma, UCB, Bristol-Meyer-Squibb, and Boehringer-Ingelheim. R. Balestri has received support for attending meetings and/or travel from AbbVie, Amgen, Leo Pharma, Lilly, Novartis, and Sanofi. M. Burlando acted as a speaker or consultant for Abbvie, Eli Lilly, Janssen, Leo-Pharma, UCB, Novartis, Bristol-Meyer-Squibb, and Boehringer-Ingelheim. G. Caldarola has received honoraria as a speaker and consultant for Abbvie, Almirall, Biogen, Eli Lilly, LEO Pharma, Novartis, Janssen, Sanofi, Pfizer, and UCB Pharma outside the submitted work. A. Campanati has served as a speaker, consultant, or advisory board member for Abbvie, Almirall, Amgen, Eli-Lilly, Leo Pharma, Janssen-Cilag, Novartis, Pfizer, Sanofi-Aventis, Boehringer Ingelheim, and UCB Pharma. E. Campione has served as an advisory board member and received fees for lectures and/or research grants from Almirall, Amgen, Abbvie, Bristol Myers Squibb, Incyte, Leo Pharma, and UCB. A. Carugno has been a speaker and/or consultant for Almirall, Amgen, Abbvie, Boehringer-Ingelheim, Eli Lilly, Leo Pharma, Janssen-Cilag, Novartis, and UCB Pharma. A. Costanzo has been a consultant and/or speaker for AbbVie, Almirall, Amgen, Janssen, Leo Pharma, Eli Lilly, Galderma, Boehringer, Novartis, Pfizer, Sandoz, and UCB. E. Cozzani acted as a speaker or consultant for Abbvie, Almirall, Eli Lilly, Leo-Pharma, and Novartis. G. Dal Bello has been a consultant for Abbvie, Eli Lilly, Janssen, Sanofi, UCB, and Novartis. A. Dattola has served as a speaker, consultant, or advisory board member for Abbvie, Almirall, Amgen, Eli Lilly, Leo Pharma, Janssen, Novartis, Boehringer Ingelheim, and UCB Pharma outside the submitted work. M. Esposito has served as a speaker/consultant for Abbvie, Amgen, Almirall, Eli Lilly, Janssen, Leopharma, Novartis, Pfizer, Sanofi, and UCB. M.C. Fargnoli has served on advisory boards and received honoraria for lectures and/or research grants from AMGEN, Almirall, Abbvie, Boehringer-Ingelheim, BMS, Galderma, Kyowa Kyrin, Incyte, LEO Pharma, Pierre Fabre, UCB, Lilly, Pfizer, Janssen, MSD, Novartis, Sanofi, Regeneron, and Sun Pharma. C. Guarneri has received consultation fees and/or grants for research projects, advisory panels and educational lectures from Wyeth-Pfizer, Abbott Immunology-Abbvie, Janssen-Cilag, Novartis, LEO-Pharma, LEO-Pharma Denmark, Ely-Lilly, Celgene, Merck-Serono, UCB Pharma, Sanofi-Aventis, Amgen, and Almirall. P. Malagoli has been a speaker for AbbVie, Lilly, Novartis, Janssen-Cilag, Celgene, Leopharma, and Almirall. A. Narcisi has served on advisory boards and received honoraria for lectures and research grants from Almirall, AbbVie, BMS, Leo Pharma, Celgene, Eli Lilly, Janssen, Novartis, Sanofi-Genzyme, Amgen, and Boehringer Ingelheim. All conflicts of interest did not concern the present manuscript.
References
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Young, M.; Aldredge, L. Recommendations for Initiating Systemic Therapy in Patients with Psoriasis. J. Clin. Aesthet. Dermatol. 2019, 12, 13–26. [Google Scholar] [PubMed]
- Fleming, P.; Kraft, J.; Gulliver, W.P.; Lynde, C. The Relationship of Obesity with the Severity of Psoriasis: A Systematic Review. J. Cutan. Med. Surg. 2015, 19, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.-H.; Chi, C.-C.; Yeh, M.-L.; Wang, S.-H.; Tsai, Y.-S.; Hsu, M.-Y. Lifestyle changes for treating psoriasis. Cochrane Database Syst. Rev. 2019, 7, 1–68. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Skov, L. Psoriasis and Obesity. Dermatology 2016, 232, 633–639. [Google Scholar] [CrossRef]
- Jacobi, A.; Langenbruch, A.; Purwins, S.; Augustin, M.; Radtke, M.A. Prevalence of Obesity in Patients with Psoriasis: Results of the National Study PsoHealth3. Dermatology 2015, 231, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.B.; Lebwohl, M.G. Psoriasis: Which therapy for which patient. J. Am. Acad. Dermatol. 2019, 80, 27–40. [Google Scholar] [CrossRef]
- Viola, R.; Mastorino, L.; Megna, M.; Damiani, G.; Gisondi, P.; Argenziano, G.; Peris, K.; Prignano, F.; Burlando, M.; Conti, A.; et al. Multi-failure psoriasis patients: Characterization of the patients and response to biological therapy in a multicenter Italian cohort. Int. J. Dermatol. 2024, 63, 351–358. [Google Scholar] [CrossRef]
- Darwin, E.; Lebwohl, M.; Han, G. Biologic Vs Conventional Therapies: Comparing Risk of Psoriasis-Associated Comorbidities. J. Drugs Dermatol. 2023, 22, 621–622. [Google Scholar] [CrossRef]
- Zhu, B.; Jing, M.; Yu, Q.; Ge, X.; Yuan, F.; Shi, L. Treatments in psoriasis: From standard pharmacotherapy to nanotechnology therapy. Postepy Dermatol. Alergol. 2022, 39, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Darji, K.; No, D.J.; Bhutani, T.; Wu, J.J. Review of IL-17 inhibitors for psoriasis. J. Dermatol. Treat. 2018, 29, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Wcisło-Dziadecka, D.; Kaźmierczak, A.; Grabarek, B.; Zbiciak-Nylec, M.; Brzezińska-Wcisło, L. Are new variants of psoriasis therapy (IL-17 inhibitors) safe? Int. J. Dermatol. 2019, 58, 1360–1365. [Google Scholar] [CrossRef] [PubMed]
- Demirel Öğüt, N.; Ayanoğlu, M.A.; Koç Yıldırım, S.; Erbağcı, E.; Ünal, S.; Gökyayla, E. Are IL-17 inhibitors superior to IL-23 inhibitors in reducing systemic inflammation in moderate-to-severe plaque psoriasis? A retrospective cohort study. Arch. Dermatol. Res. 2025, 317, 232. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.A.; Leonardi, C.; Menter, A.; Ortonne, J.-P.; Krueger, J.G.; Kricorian, G.; Aras, G.; Li, J.; Russell, C.B.; Thompson, E.H.; et al. Brodalumab, an Anti–Interleukin-17–Receptor Antibody for Psoriasis. N. Engl. J. Med. 2012, 366, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.; Reich, K.; Paul, C.; Blauvelt, A.; Baran, W.; Bolduc, C.; Toth, D.; Langley, R.; Cather, J.; Gottlieb, A.; et al. A prospective phase III, randomized, double-blind, placebo-controlled study of brodalumab in patients with moderate-to-severe plaque psoriasis. Br. J. Dermatol. 2016, 175, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Strober, B.; Menter, A.; Gordon, K.; Weglowska, J.; Puig, L.; Papp, K.; Spelman, L.; Toth, D.; Kerdel, F.; et al. Phase 3 Studies Comparing Brodalumab with Ustekinumab in Psoriasis. N. Engl. J. Med. 2015, 373, 1318–1328. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Niiro, H.; Ootaki, K.; Japanese Brodalumab Study Group. Brodalumab, a human anti-interleukin-17-receptor antibody in the treatment of Japanese patients with moderate-to-severe plaque psoriasis: Efficacy and safety results from a phase II randomized controlled study. J. Dermatol Sci. 2016, 81, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Iversen, L.; Puig, L.; Lambert, J.; Mrowietz, U.; Saday, K.K.; Warren, R. Long-term efficacy and safety of brodalumab in moderate-to-severe plaque psoriasis: A post hoc pooled analysis of AMAGINE-2 and -3. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1275–1283. [Google Scholar] [CrossRef]
- Puig, L.; Lebwohl, M.; Bachelez, H.; Sobell, J.; Jacobson, A.A. Long-term efficacy and safety of brodalumab in the treatment of psoriasis: 120-week results from the randomized, double-blind, placebo- and active comparator-controlled phase 3 AMAGINE-2 trial. J. Am. Acad. Dermatol. 2020, 82, 352–359. [Google Scholar] [CrossRef]
- Kojanova, M.; Turkova, B.; Gkalpakiotis, S.; Cetkovska, P.; Fialova, J.; Dolezal, T.; Machovcova, A.; Apol, E.D.; the BIOREP Study Group. Real-World Data on Brodalumab Treatment in Patients with Moderate-to-Severe Plaque Psoriasis: An Observational Study from the Czech Republic BIOREP Registry. Adv. Ther. 2024, 41, 3951–3971. [Google Scholar] [CrossRef]
- Schaeffer, L.; Ben-Anaya, N.; Sorbe, C.; Rustenbach, S.J.; Mrowietz, U.; Augustin, M. Real-world outcomes and drug survival of brodalumab: Results from the German Psoriasis Registry PsoBest. J. Dermatol. Treat. 2024, 35, 2340107. [Google Scholar] [CrossRef] [PubMed]
- Rigopoulos, D.; Tampouratzi, E.; Angelakopoulos, C.; Apalla, Z.; Barkis, I.; Georgiou, S.; Delli, F.; Drosos, A.; Zafiriou, E.; Katsantonis, J.; et al. Real-world data on the effectiveness of brodalumab in patients with moderate-to severe plaque psoriasis in the Greek clinical setting (the BrIDGE study). J. Eur. Acad. Dermatol. Venereol. 2024, 38, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Fargnoli, M.; Esposito, M.; Dapavo, P.; Parodi, A.; Rossi, M.; Tiberio, R.; Dastoli, S.; Offidani, A.; Argenziano, G.; Gisondi, P.; et al. Brodalumab for the treatment of moderate-to-severe plaque-type psoriasis: A real-life, retrospective 24-week experience. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.G.; Koo, J.Y.; Armstrong, A.W.; Strober, B.E.; Martin, G.M.; Rawnsley, N.N.; Goehring, E.L.; Jacobson, A.A. Brodalumab: 5-Year US Pharmacovigilance Report. Dermatol. Ther. 2024, 14, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Fargnoli, M.C.; Amerio, P.; Argenziano, G.; Bardazzi, F.; Bianchi, L.; Chiricozzi, A.; Conti, A.; Corazza, M.; Costanzo, A.; et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital. J. Dermatol. Venereol. 2022, 157 (Suppl. S1), S1–S78. [Google Scholar] [CrossRef] [PubMed]
- Kyntheum. Available online: https://www.ema.europa.eu/en/documents/product-information/kyntheum-epar-product-information_en.pdf (accessed on 4 February 2025).
- Lebwohl, M.G.; Armstrong, A.W.; Alexis, A.F.; Lain, E.L.; Jacobson, A.A. Efficacy of Brodalumab in Patients with Psoriasis and Risk Factors for Treatment Failure: A Review of Post Hoc Analyses. Dermatol. Ther. 2024, 14, 2709–2726. [Google Scholar] [CrossRef] [PubMed]
- Caldarola, G.; Galluzzo, M.; Bernardini, N.; Botti, E.; De Luca, E.; De Simone, C.; Mariani, M.; Moretta, G.; Pallotta, S.; Campione, E.; et al. Long-Term Effectiveness of Brodalumab for the Treatment of Moderate-To-Severe Psoriasis: A Real-Life Multicenter Study of Up to 3 Years in a Real-Life Italian Cohort. Dermatol. Pract. Concept. 2024, 14, e2024152. [Google Scholar] [CrossRef] [PubMed]
- Kokolakis, G.; Vadstrup, K.; Hansen, J.B.; Carrascosa, J.M. Increased Skin Clearance and Quality of Life Improvement with Brodalumab Compared with Ustekinumab in Psoriasis Patients with Aggravating Lifestyle Factors. Dermatol. Ther. 2021, 11, 2027–2042. [Google Scholar] [CrossRef]
- Carrascosa, J.; Rocamora, V.; Fernandez-Torres, R.; Jimenez-Puya, R.; Moreno, J.; Coll-Puigserver, N.; Fonseca, E. Obesity and psoriasis: Inflammatory nature of obesity, relationship between psoriasis and obesity, and therapeutic implications. Actas Dermosifiliogr. 2014, 105, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Ullah, A.; Singla, R.K.; Batool, Z.; Cao, D.; Shen, B. Pro- and anti-inflammatory cytokines are the game-changers in childhood obesity-associated metabolic disorders (diabetes and non-alcoholic fatty liver diseases). Rev. Endocr. Metab. Disord. 2024, 25, 783–803. [Google Scholar] [CrossRef] [PubMed]
- Bausch Health LLC. Siliq [Package Insert]; Bausch Health LLC.: Bridgewater, NJ, USA, 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761032lbl.pdf (accessed on 14 December 2020).
- Hsu, S.; Green, L.J.; Lebwohl, M.G.; Wu, J.J.; Blauvelt, A.; Jacobson, A.A. Comparable efficacy and safety of brodalumab in obese and nonobese patients with psoriasis: Analysis of two randomized controlled trials. Br. J. Dermatol. 2020, 182, 880–888. [Google Scholar] [CrossRef]
- Russo, F.; Galluzzo, M.; Stingeni, L.; Persechino, S.; Zichichi, L.; Conti, A.; Giofrè, C.; Dini, V.; Vispi, M.; Atzori, L.; et al. Long-Term Drug Survival and Effectiveness of Secukinumab in Patients with Moderate to Severe Chronic Plaque Psoriasis: 42-Month Results from the SUPREME 2.0 Study. Clin. Cosmet. Investig. Dermatol. 2023, 16, 3561–3574. [Google Scholar] [CrossRef] [PubMed]
- Kiltz, U.; Sfikakis, P.P.; Gaffney, K.; Sator, P.-G.; von Kiedrowski, R.; Bounas, A.; Gullick, N.; Conrad, C.; Rigopoulos, D.; Lespessailles, E.; et al. Secukinumab Use in Patients with Moderate to Severe Psoriasis, Psoriatic Arthritis and Ankylosing Spondylitis in Real-World Setting in Europe: Baseline Data from SERENA Study. Adv. Ther. 2020, 37, 2865–2883. [Google Scholar] [CrossRef] [PubMed]
- Mastorino, L.; Dapavo, P.; Burzi, L.; Rosset, F.; Giunipero di Corteranzo, I.; Leo, F.; Verrone, A.; Stroppiana, E.; Ortoncelli, M.; Ribero, S.; et al. Drug survival, effectiveness, and safety of brodalumab for moderate-to-severe psoriasis up to 3 years. Int. J. Dermatol. 2024, 63, 922–928. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).