
COVID-19 Related Retinal Vascular Occlusion: A Systematic Review


Abstract
1. Introduction
2. Methods
2.1. Conduct of Review
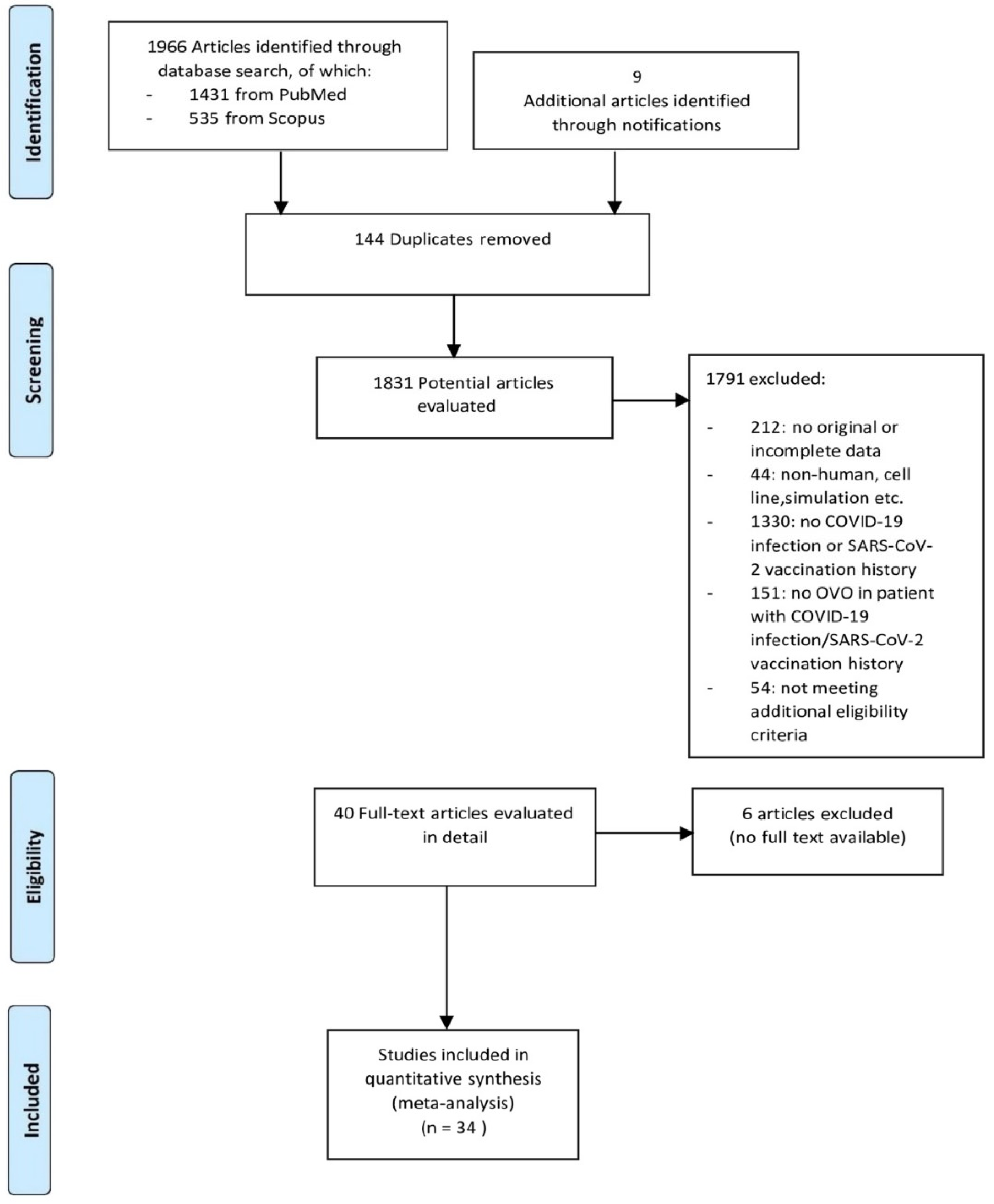
2.2. Search Strategy and Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Martin, A.J.M. Thrombosis and Coagulopathy in COVID-19. Cur. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef] [PubMed]
- Hazar, L.; Karahan, M.; Vural, E.; Ava, S.; Erdem, S.; Dursun, M.E.; Keklikçi, U. Macular vessel density in patients recovered from COVID 19. Photodiagnosis Photodyn. Ther. 2021, 34, 102267. [Google Scholar] [CrossRef] [PubMed]
- Ip, M.; Hendrick, A. Retinal Vein Occlusion Review. Asia Pac. J. Ophthalmol. 2018, 7, 40–45. [Google Scholar] [CrossRef]
- Scott, I.U.; Campochiaro, P.A.; Newman, N.J.; Biousse, V. Retinal vascular occlusions. Lancet Lond Engl. 2020, 396, 1927–4190. [Google Scholar] [CrossRef]
- Acharya, S.; Diamond, M.; Anwar, S.; Glaser, A.; Tyagi, P. Unique case of central retinal artery occlusion secondary to COVID-19 disease. IDCases 2020, 21, e00867. [Google Scholar] [CrossRef]
- Sugihara, K.; Kono, M.; Tanito, M. Branch Retinal Vein Occlusion after Messenger RNA-Based COVID-19 Vaccine. Case Rep. Ophthalmol. 2022, 13, 28–32. [Google Scholar] [CrossRef]
- Gaba, W.H.; Ahmed, D.; Al Nuaimi, R.K.; Dhanhani, A.A.; Eatamadi, H. Bilateral Central Retinal Vein Occlusion in a 40-Year-Old Man with Severe Coronavirus Disease 2019 (COVID-19) Pneumonia. Am. J. Case Rep. 2020, 21, e927691.29. [Google Scholar] [CrossRef]
- Insausti-García, A.; Reche-Sainz, J.A.; Ruiz-Arranz, C.; Vázquez, Á.L.; Ferro-Osuna, M. Papillophlebitis in a COVID-19 patient: Inflammation and hypercoagulable state. Eur. J. Ophthalmol. 2020, 32, NP168–NP172. [Google Scholar] [CrossRef]
- Rego Lorca, D.; Rouco Fernandez, A.; Jimenez Santos, M.; Saenz-Frances, F.; Burgos-Blasco, B.; Donate Lopez, J. Bilateral retinal vein occlusion and diabetic retinopathy after COVID-19. Acta Ophthalmol. 2020, 99, e1246–e1248. [Google Scholar] [CrossRef]
- Kapatayes, N.; Joondeph, B.C. Retinal vein occlusion associated with covid-19. Retin. Today 2020, 2020, 32–33. [Google Scholar]
- Sheth, J.U.; Narayanan, R.; Goyal, J.; Goyal, V. Retinal vein occlusion in COVID-19: A novel entity. Indian J. Ophthalmol. 2020, 68, 2291–2293. [Google Scholar] [CrossRef] [PubMed]
- Walinjkar, J.A.; Makhija, S.C.; Sharma, H.R.; Morekar, S.R.; Natarajan, S. Central retinal vein occlusion with COVID-19 infection as the presumptive etiology. Indian J. Ophthalmol. 2020, 68, 2572–2574. [Google Scholar] [CrossRef] [PubMed]
- Yahalomi, T.; Pikkel, J.; Arnon, R.; Pessach, Y. Central retinal vein occlusion in a young healthy COVID-19 patient: A case report. Am. J. Ophthalmol. Case Rep. 2020, 20, 100992. [Google Scholar] [CrossRef]
- Finn, A.P.; Khurana, R.N.; Chang, L.K. Hemi-retinal vein occlusion in a young patient with COVID-19. Am. J. Ophthalmol. Case Rep. 2021, 22, 101046. [Google Scholar] [CrossRef]
- Raval, N.; Djougarian, A.; Lin, J. Central retinal vein occlusion in the setting of COVID-19 infection. J. Ophthalmic. Inflamm. Infect. 2021, 11, 10. [Google Scholar] [CrossRef]
- Venkatesh, R.; Reddy, N.G.; Agrawal, S.; Pereira, A. COVID-19-associated central retinal vein occlusion treated with oral aspirin. BMJ Case Rep. 2021, 14, e242987. [Google Scholar] [CrossRef]
- Sonawane, N.; Yadav, D.; Kota, A.; Singh, H. Central retinal vein occlusion post-COVID-19 vaccination. Indian Ophthalmol. 2022, 70, 308. [Google Scholar] [CrossRef]
- Cuadros Sánchez, C.; Egüen, C.S.; Gutierrez-Ezquerro, R.; Giralt-Peret, L.; Fonollosa, A. Central Retinal Vein Occlusion Presumably Associated with Lupus Anticoagulant Induced by SARSCoV-2. Ocul. Immunol. Inflamm. 2022, 30, 2010–2013. [Google Scholar] [CrossRef]
- Vieyra, L.G.; Garduño, C.O.; Martínez, R.R.; Escobar, B.F. Branch retinal vein occlusion on Coats disease during COVID-19 infection: A case report. Oftalmol. Zhurnal 2022, 98, 63–64. [Google Scholar] [CrossRef]
- Pur, D.R.; Catherine Danielle Bursztyn, L.L.; Iordanous, Y. Branch retinal vein occlusion in a healthy young man following mRNA COVID-19 vaccination. Am. J. Ophthalmol. Case Rep. 2022, 26, 101445. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Nagasato, D.; Nakakura, S.; Nagasawa, T.; Wakuda, H.; Kurusu, A.; Mitamura, Y.; Tabuchi, H. Branch retinal vein occlusion post severe acute respiratory syndrome coronavirus 2 vaccination. Taiwan J. Ophthalmol. 2022, 12, 202. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Sun, I.-T. Bilateral Simultaneous Central Retinal Vein Occlusion Secondary to COVID-19: A Case Report. Case Rep Ophthalmol. 2023, 14, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, K.; Hirano, Y.; Esaki, Y.; Yasukawa, T. Central Retinal Vein Occlusion after mRNA COVID-19 Vaccination. Case Rep. Ophthalmol. 2023, 14, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Ong, K.W.; Halim, W.H.M.W.A.; Khialdin, S.M.M.; Yong, M.H.M. Case Report: Branch Retinal Vein Occlusion Post-mRNA SARS-CoV-2 (COVID-19) Vaccination. Optom. Vis. Sci. 2023, 100, 799–803. [Google Scholar] [CrossRef]
- Montesel, A.; Bucolo, C.; Mouvet, V.; Moret, E.; Eandi, C.M. Case Report: Central Retinal Artery Occlusion in a COVID-19 Patient. Front. Pharmacol. 2020, 11, 588384. [Google Scholar] [CrossRef]
- Bapaye, M.M.; Nair, A.G.; Bapaye, C.M.; Shukla, J.J. Simultaneous Bilateral Central Retinal Artery Occlusion Following COVID-19 Infection. Ocul. Immunol. Inflamm. 2021, 29, 671–674. [Google Scholar] [CrossRef]
- Murchison, A.P.; Sweid, A.; Dharia, R.; Theofanis, T.N.; Tjoumakaris, S.I.; Jabbour, P.M.; Bilyk, J.R. Monocular visual loss as the presenting symptom of COVID-19 infection. Clin. Neurol. Neurosurg. 2021, 201, 106440. [Google Scholar] [CrossRef]
- Raj, A.; Kaur, N.; Kaur, N. Cavernous sinus thrombosis with central retinal artery occlusion in COVID-19: A case report and review of literature. Indian J. Ophthalmol. 2021, 69, 1327–1329. [Google Scholar] [CrossRef]
- Sanjay, S.; Srinivasan, P.; Jayadev, C.; Mahendradas, P.; Gupta, A.; Kawali, A.; Shetty, R. Post COVID-19 Ophthalmic Manifestations in an Asian Indian Male. Ocul. Immunol. Inflamm. 2021, 29, 656–661. [Google Scholar] [CrossRef]
- Savastano, M.C.; Culiersi, C.; Savastano, A.; Gambini, G.; Caporossi, T.; Rizzo, S. Focal superior quadrant haemorrhages in post COVID-19 patient: A target for personalized medicine. Eur. J. Ophthalmol. 2021, 32, NP87–NP91. [Google Scholar] [CrossRef] [PubMed]
- Turedi, N.; Onal Gunay, B. Paracentral acute middle maculopathy in the setting of central retinal artery occlusion following COVID-19 diagnosis. Eur. J. Ophthalmol. 2021, 14, NP62–NP66. [Google Scholar] [CrossRef]
- Abdin, A.D.; Gärtner, B.C.; Seitz, B. Central retinal artery occlusion following COVID-19 vaccine administration. Am. J. Ophthalmol. Case Rep. 2022, 26, 101430. [Google Scholar] [CrossRef]
- Chow, S.Y.; Hsu, Y.R.; Fong, V.H. Central retinal artery occlusion after Moderna mRNA-1273 vaccination. J. Formos. Med. Assoc. 2022, 121, 2369–2370. [Google Scholar] [CrossRef]
- Thakar, M.; Bhattacharya, S. Central retinal artery occlusion after vaccination with whole virion inactivated SARSCoV-2 vaccine Covaxin. Indian J. Ophthalmol. 2022, 70, 3716–3718. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, M.R.; Lucena, A.R.V.; Higino, T.M.; Ventura, C.V. Central retinal artery occlusion with cilioretinal artery sparing secondary to COVID-19: Additional ocular complication. Indian J. Ophthalmol. 2023, 71, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Heidarzadeh, H.R.; Abrishami, M.; Shariati, M.M.; Shahri, S.H.G.; Astaneh, M.R.A. Atypical Central Retinal Artery Occlusion following COVID-19 Infection: A Case Report. Case Rep. Ophthalmol. 2023, 14, 405–410. [Google Scholar] [CrossRef]
- Hirosawa, K.; Inomata, T.; Sung, J.; Morooka, Y.; Huang, T.; Akasaki, Y.; Okumura, Y.; Nagino, K.; Omori, K.; Nakao, S. Unilateral branch retinal artery occlusion in association with COVID-19: A case report. Int. J. Ophthalmol. 2024, 17, 777–782. [Google Scholar] [CrossRef]
- Jiang, Z.; Ji, H.; Zhang, H.; Dong, Z.; Dong, J. Branch retinal artery occlusion in a patient with COVID-19 infection: A case report. J. Int. Med. Res. 2024, 52, 03000605241284931. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011); The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Hayreh, S. Central retinal artery occlusion. Indian J. Ophthalmol. 2018, 66, 1684. [Google Scholar] [CrossRef]
- McAllister, I.L. Central retinal vein occlusion: A review: Central retinal vein occlusion. Clin. Exp. Ophthalmol. 2012, 40, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Yasuda, K.; Mimura, T.; Ofusa, A.; Shimura, M. Relationship between retinal blood flow and cytokines in central retinal vein occlusion. BMC Ophthalmol. 2020, 20, 215. [Google Scholar] [CrossRef] [PubMed]
- Seah, I.; Agrawal, R. Can the Coronavirus Disease 2019 (COVID-19) Affect the Eyes? A Review of Coronaviruses and Ocular Implications in Humans and Animals. Ocul. Immunol. Inflamm. 2020, 28, 391–395. [Google Scholar] [CrossRef]
- Singh, S.P.; Pritam, M.; Pandey, B.; Yadav, T.P. Microstructure, pathophysiology, and potential therapeutics of COVID-19: A comprehensive review. J. Med. Virol. 2021, 93, 275–299. [Google Scholar] [CrossRef]
- Zhou, T.; Yuan, Z.; Weng, J.; Pei, D.; Du, X.; He, C.; Lai, P. Challenges and advances in clinical applications of mesenchymal stromal cells. J. Hematol. Oncol. 2021, 14, 24. [Google Scholar] [CrossRef]
- Topcu, A.C.; Ozturk-Altunyurt, G.; Akman, D.; Batirel, A.; Demirhan, R. Acute Limb Ischemia in Hospitalized COVID-19 Patients. Ann. Vasc. Surg. 2021, 74, 88–94. [Google Scholar] [CrossRef]
- Fournier, M.; Faille, D.; Dossier, A.; Mageau, A.; Roland, P.N.; Ajzenberg, N.; Borie, R.; Bouadma, L.; Bunel, V.; Castier, Y.; et al. Arterial Thrombotic Events in Adult Inpatients With COVID-19. Mayo Clin. Proc. 2021, 96, 295–303. [Google Scholar] [CrossRef]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients With COVID-19 in a New York City Health System. JAMA 2020, 324, 799–801. [Google Scholar] [CrossRef]
- Oncul, S.; Afshar-Kharghan, V. The interaction between the complement system and hemostatic factors. Curr. Opin. Hematol. 2020, 27, 341–352. [Google Scholar] [CrossRef]
- Teuwen, L.-A.; Geldhof, V.; Pasut, A.; Carmeliet, P. COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 389–391. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, A.H.; Palaiodimou, L.; Zand, R.; Yaghi, S.; Kamel, H.; Navi, B.B.; Turc, G.; Romoli, M.; Sharma, V.K.; Mavridis, D.; et al. The Impact of SARS-CoV-2 on Stroke Epidemiology and Care: A Meta-Analysis. Ann. Neurol. 2021, 89, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.J.; Smith, C.J.; Roffe, C.; Simister, R.J.; Narayanamoorthi, S.; Marigold, R.; Willmot, M.; Dixit, A.; Hassan, A.; Quinn, T.J.; et al. Characteristics and outcomes of COVID-19 associated stroke: A UK multicentre case-control study. J. Neurol. Neurosurg. Psychiatry 2021, 92, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Bass, D.I.; Meyer, R.M.; Barros, G.; Carroll, K.T.; Walker, M.; D’Oria, M.; Levitt, M.R. The impact of the COVID-19 pandemic on cerebrovascular disease. Semin Vasc. Surg. 2021, 34, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-X.M.; Wei, J.C.-C.; Wang, Y.-H.B.; Bair, H.; Hsu, S.-B.B.; Lin, C.-J. Retinal Vascular Occlusion and COVID-19 Diagnosis: A Multicenter Population-Based Study. Retina 2024, 44, 345–352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Year, Authors | Age | Sex | Type of Occlusion | Eye | Clinical Symptoms | Time Since COVID-19 Infection or SARS-CoV-2 Immunization (days) | Comorbidities | BCVA at Baseline | Interventions | Final BCVA | Follow-up Period |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020, Gaba et al. [8] | 40 | Male | CRVO | OU | DV | 4 (infection) | Hypertension; Obesity | RE 6/9 LE 6/18 | LMWH; Rivaroxaban | RE 6/6 LE 6/12 | 1 week |
| 2020, Insausti-García et al. [9] | 40 | Male | CRVO/ Papillophlebitis | OS | DV | 42 (infection) | None | 20/200 | ASA; Bromfenac; Intravitreal dexamethasone implant | 20/40 | 2 weeks |
| 2020, Rego Lorca et al. [10] | 30 | Female | CRVO | OU | DV, floaters | N/A (infection) | Maturity-onset DM of the young | BE 7/10 | N/A | N/A | N/A |
| 2020, Kapatayes et al. [11] | 59 | Male | CRVO | OD | DV | N/A (infection) | Microscopic colitis | 20/20 | None | 20/20 | N/A |
| 2020, Sheth et al. [12] | 52 | Male | BRVO | OS | DV | 10 (infection) | None | 6/60 | Oral methylprednisolone; Intravitreal anti-VEGF | 6/9 | 1 month |
| 2020, Walinjkar et al. [13] | 17 | Female | CRVO | OD | DV | 22 (infection) | PCOS | 6/24 | Intravitreal anti-VEGF | 6/18 | 1 month |
| 2020, Yahalomi et al. [14] | 33 | Male | CRVO | OS | DV, flashes | 35 (infection) | None | 20/25 | None | 20/20 | Several months |
| 2021, Finn et al. [15] | 32 | Male | CRVO | OD | VF defect | N/A (infection) | None | 20/20 | N/A | N/A | N/A |
| 2021, Raval et al. [16] | 39 | Male | CRVO | OD | DV, floaters | 7 (infection) | None | 20/150 | Intravitreal anti-VEGF | 20/30 | N/A |
| 2021, Venkatesh et al. [17] | 56 | Female | CRVO | OS | DV | N/A (infection) | DM | 6/18 | Low dose ASA | 6/6 | 1 month |
| 2022, Sugihara et al. [7] | 38 | Male | BRVO | OS | DV | 2 (2nd dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | None | 20/25 | Intravitreal anti-VEGF | 20/20 | 7 months |
| 2022, Sonawane et al. [18] | 50 | Male | CRVO | OD | DV | 4 (2nd dose of ChAdOx1 nCoV-19, Covishield, AstraZeneca-Oxford vaccine) | DM | 6/60 | Intravitreal anti-VEGF | N/A | N/A |
| 2022, Sonawane et al. [18] | 43 | Female | CRVO | OD | DV | 3 (2nd dose of ChAdOx1 nCoV-19, Covishield, AstraZeneca-Oxford vaccine) | None | 5/60 | None | N/A | N/A |
| 2022, Cuadros Sánchez et al. [19] | 32 | Male | CRVO | OD | DV, photopsia | 51 (infection) | None | 20/32 | Intravitreal dexamethasone implant | 20/20 | 4 months |
| 2022, Garduño Vieyra et al. [20] | 43 | Male | BRVO | OD | DV | 4 (infection) | Coats disease | 20/400 | Intravitreal anti-VEGF; Periocular triamcinolone; Focal laser treatment | 20/20 | 3 months |
| 2022, Pur et al. [21] | 34 | Male | BRVO | OD | Inferior VF defect, photopsia | 2 (1st dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | None | 20/20 | None | 20/20 | 10 months |
| 2022, Tanaka et al. [22] | 50 | Female | BRVO | OD | DV | 3 (1st dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | Breast cancer (treated with tamoxifen) | 20/25 | Intravitreal anti-VEGF | 20/20 | 2 months |
| 2022, Tanaka et al. [22] | 56 | Female | BRVO | OD | DV | 3 (1st dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | None | 13/20 | Intravitreal anti-VEGF | 20/20 | 2 months |
| 2023, Lin et al. [23] | 48 | Male | CRVO | OU | DV | 14 (infection) | Hypertension; DM type II; CKD stage IV | OU CF | BE Intravitreal anti-VEGF | OU 20/20 | Several months |
| 2023, Ishiguro et al. [24] | 47 | Male | CRVO | OD | DV | 8 h (1st dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | None | 20/200 | Intravitreal anti-VEGF | 20/20 | 10 months |
| 2023, Lee et al. [25] | 41 | Female | BRVO | OD | Central VF defect | 3 (2nd dose of BNT162b2, Comirnaty, Pfizer-BioNTech vaccine) | None | 6/18 | Intravitreal anti-VEGF | 6/6 | 1 month |
| Year, Authors | Age | Sex | Type of Occlusion | Eye | Clinical Symptoms | Time Since COVID-19 Infection or SARS-CoV-2 Immunization (days) | Comorbidities | BCVA at Baseline | Interventions | Final BCVA | Follow-up Period |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020, Acharya et al. [6] | 60 | Male | CRAO | OD | PVL | 12 (infection) | Hypertension; Dyslipidemia; Coronary artery disease; COPD | NLP | N/A | NLP | N/A |
| 2020, Montesel et al. [26] | 59 | Male | CRAO | OS | PVL | 21 (infection) | Hypertension; Hyperuricemia; Heterozygous hemoglobin S (sickle cell trait) | LP | None | CF | 1 month |
| 2021, Bapaye et al. [27] | 42 | Male | CRAO | OU | PVL | 13 (infection) | None | OU LP | ASA; Oral dexamethasone | OU LP | 6 weeks |
| 2021, Murchison et al. [28] | 5th decade | Male | CRAO | OD | PVL | 2 (infection) | Hypertension | HM | LMWH | HM | N/A |
| 2021, Raj et al. [29] | 37 | Male | CRAO | OS | PVL, proptosis, ptosis, ophthalmo-plegia | 14 (infection) | None | NLP | IV steroids; IV antibiotics; IV anticoagulants; Symptomatic care | NLP | N/A |
| 2021, Sanjay et al. [30] | 66 | Male | CRAO | OD | PVL | 10 (infection) | DM type II | 20/2666 | Topical prednisolone; Topical anticholinergic | N/A | N/A |
| 2021, Savastano et al. [31] | 58 | Male | BRAO | OS | None | 40 (infection) | Coronary artery disease; Hypertension; Hyperuricemia | 55/55 | None | 55/55 | 1 week |
| 2021, Turedi et al. [32] | 54 | Male | CRAO | OD | PVL | 14 (infection) | None | CF | Anti-glaucoma eye drops; Hyperbaric oxygen therapy; Ocular massage | CF | 5 days |
| 2022, Abdin et al. [33] | 76 | Female | CRAO | OS | PVL | 2 (1st dose of ChAdOx1-S [recombinant], Vaxzevria, AstraZeneca-Oxford vaccine) | Hypothyroidism | HM | ASA; IV vasodilator; Anti-glaucoma eye drops; Ocular massage | N/A | N/A |
| 2022, Chow et al. [34] | 70 | Male | CRAO | OD | PVL | 5 (1st dose of mRNA-1273, Spikevax, Moderna vaccine) | Hypertension; Dyslipidemia | CF | Clopidogrel; Hyperbaric oxygen therapy | CF | 4 months |
| 2022, Thakar et al. [35] | 44 | Male | CRAO | OS | PVL | 10 (1st dose of BBV152, Covaxin, Bharat Biotech vaccine) | None | LP | None | N/A | N/A |
| 2023, Rv et al. [36] | 68 | Female | CRAO | OS | PVL | N/A (infection) | Hypertension | 20/400 | Anti-glaucoma eye drops; Ocular massage; | CF | 4 months |
| 2023, Heidarzadeh et al. [37] | 44 | Male | CRAO | OS | PVL | 20 (infection) | None | LP | Oral prednisolone; Anti-glaucoma eye drops; Panretinal photocoagulation | NLP | N/A |
| 2024, Kunihiko et al. [38] | 43 | Female | BRAO | OD | DV | 33 (infection) | None | 20/25 | IV vasodilator | N/A | 6 months |
| 2024, Jiang et al. [39] | 76 | Male | BRAO | OS | DV | 12 (infection) | Hypertension | 6/20 | ASA; LMWH; Oral prednisolone; IV vasodilator; Retrobulbar anticholinergic; Anterior chamber puncture; Supplemental oxygen | 20/20 | 12 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzamalis, A.; Foti, M.; Georgiadou, M.; Tsaftaridis, N.; Ziakas, N. COVID-19 Related Retinal Vascular Occlusion: A Systematic Review. J. Clin. Med. 2025, 14, 1183. https://doi.org/10.3390/jcm14041183
Tzamalis A, Foti M, Georgiadou M, Tsaftaridis N, Ziakas N. COVID-19 Related Retinal Vascular Occlusion: A Systematic Review. Journal of Clinical Medicine. 2025; 14(4):1183. https://doi.org/10.3390/jcm14041183
Chicago/Turabian StyleTzamalis, Argyrios, Maria Foti, Maria Georgiadou, Nikolaos Tsaftaridis, and Nikolaos Ziakas. 2025. "COVID-19 Related Retinal Vascular Occlusion: A Systematic Review" Journal of Clinical Medicine 14, no. 4: 1183. https://doi.org/10.3390/jcm14041183
APA StyleTzamalis, A., Foti, M., Georgiadou, M., Tsaftaridis, N., & Ziakas, N. (2025). COVID-19 Related Retinal Vascular Occlusion: A Systematic Review. Journal of Clinical Medicine, 14(4), 1183. https://doi.org/10.3390/jcm14041183