
A Comprehensive Review of Medial Thighplasty: The Role of Liposuction in Reducing Complications and Optimizing Patient Outcomes

 ,
, 
Abstract
1. Introduction
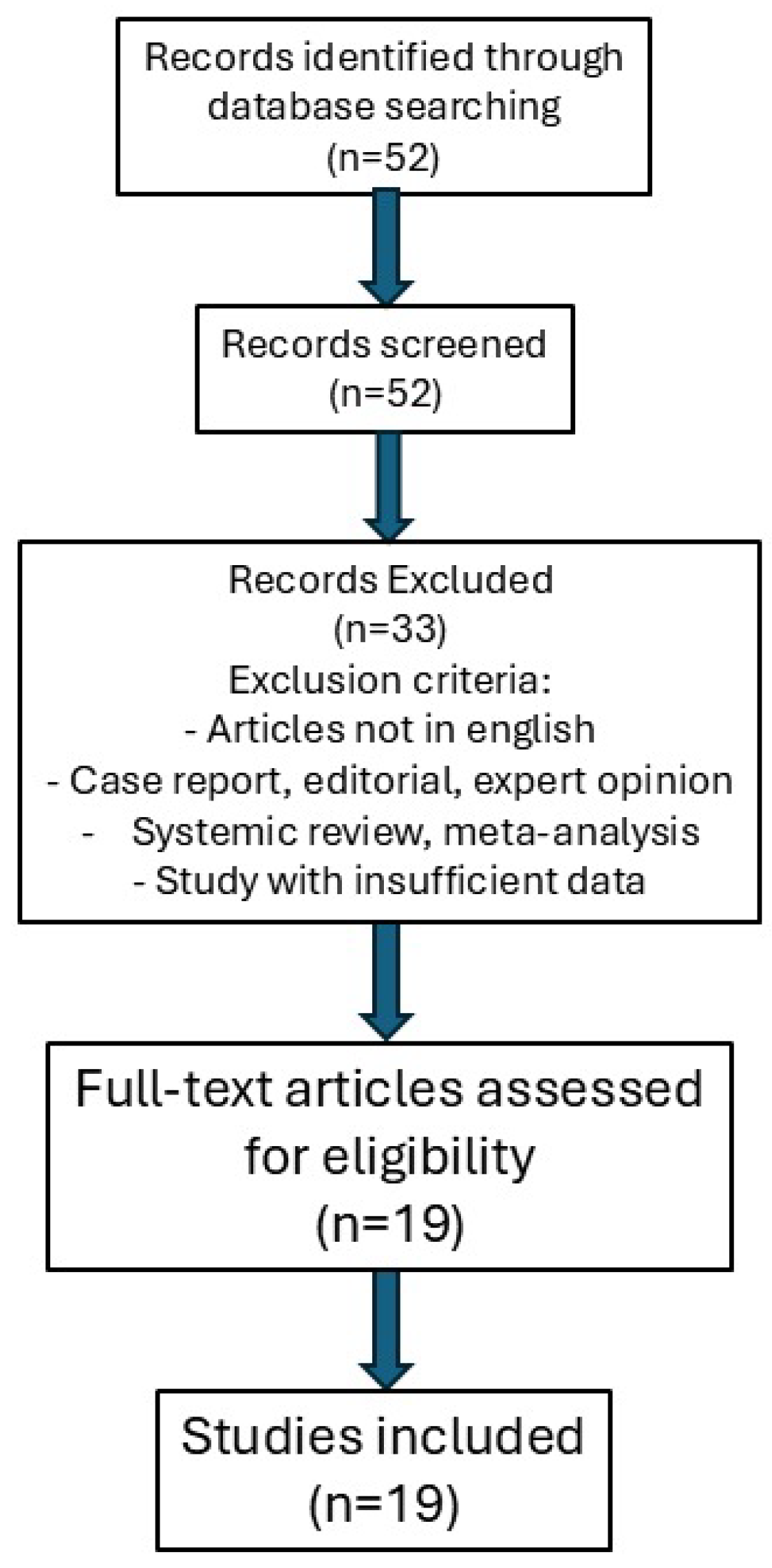
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Inclusion Criteria:
- o
- Original research articles on medial thighplasty, published up to September 2024.
- o
- Studies including patients who underwent medial thighplasty.
- o
- Prospective and retrospective observational studies, including case series.
- o
- Studies evaluating complications and surgical outcomes.
- Exclusion Criteria:
- o
- Articles not written in English.
- o
- Case reports, editorials, expert opinions, systematic reviews, meta-analyses.
- o
- Studies with insufficient or incomplete data on surgical outcomes.
2.3. Study Selection
- Horizontal pattern: This was the first thigh lift technique described by Lewis [28], later improved by Lockwood [16] with fascial anchoring, and further refined by Le Louarn and Pascal [9], who introduced the use of liposuction to minimize wide undermining and reduce complications. This approach involves a horizontal incision along the inguinal crease, extending laterally toward the hip. It is best suited for patients with minimal laxity in the upper thigh, allowing for removal of excess skin and improved contours in the upper inner thigh [9,10,11,12,13,14,16,17].
- Vertical pattern: This method involves a vertical excision of excess tissue from the inguinal crease to or near the knee, often accompanied by a horizontal extension into the inguinal crease to remove excess skin. It is indicated for patients with more extensive laxity, allowing for more skin removal and more complete contouring [2,4,5,9,11,12,13,14,15,16,17,18,19,20,21,22,23].
- Vertical scar: This technique involves an excision that leaves a vertical scar extending from the groin to the knee along the inner thigh [10].
- T-shape scar: This is the classic approach that combines a vertical incision with a horizontal incision in the inguinal fold, forming a “T”. It addresses both vertical and horizontal laxity.
- Short T-shape scar: This variation aims to minimize the horizontal scar length, potentially reducing complications seen with the traditional T-technique [12].
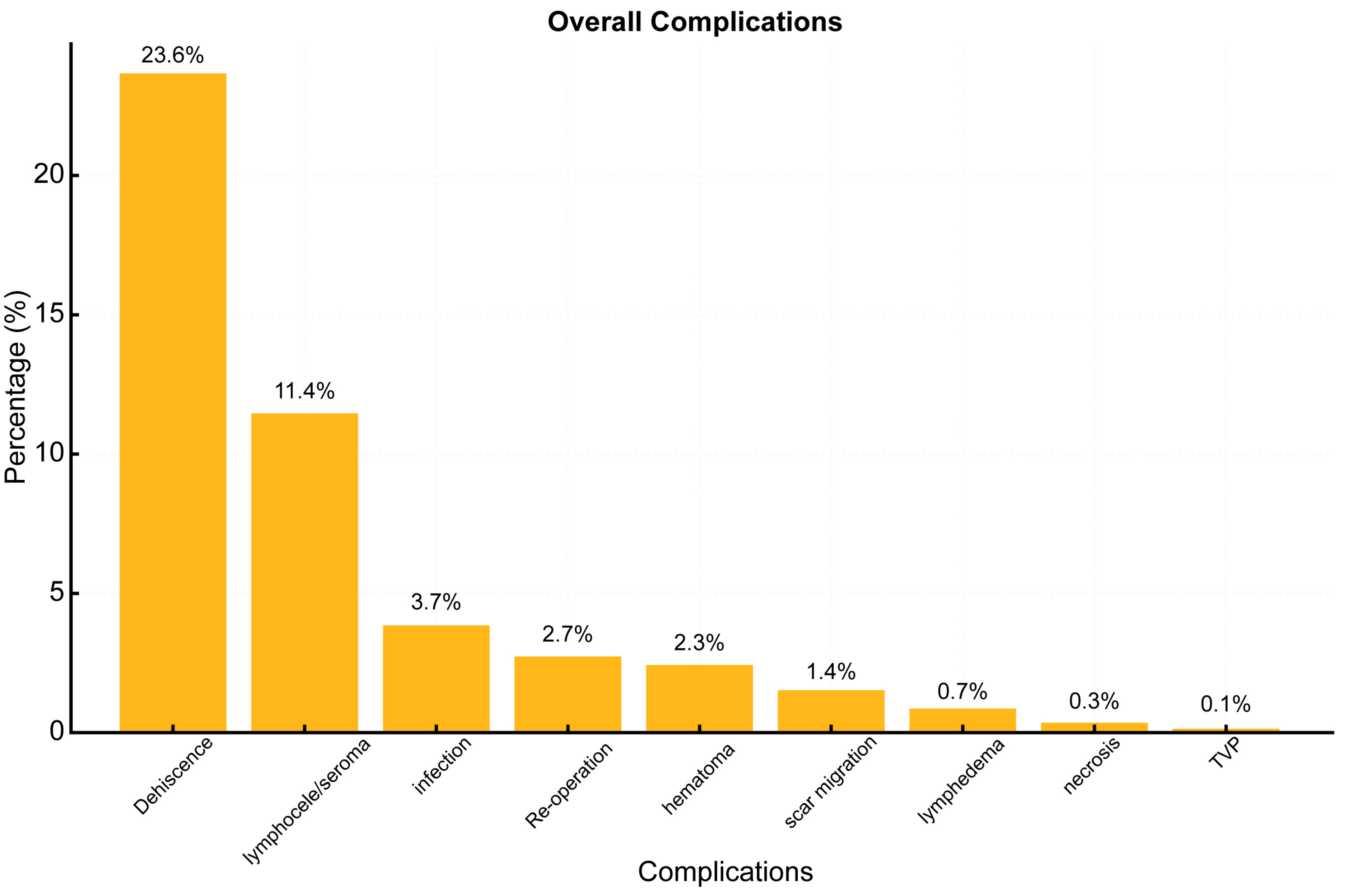
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Ettorre, M.; Bracaglia, R.; Gentileschi, S.; Tambasco, D. Micro- and macroscopic tissue modifications after bariatric surgery: Effects of different procedures-a pilot study. Aesthetic Plast. Surg. 2013, 37, 846–848. [Google Scholar] [CrossRef] [PubMed]
- Legnani, C.; Ventura, A.; Mangiavini, L.; Maffulli, N.; Peretti, G.M. Management of Medial Femorotibial Knee Osteoarthritis in Conjunction with Anterior Cruciate Ligament Deficiency: Technical Note and Literature Review. J. Clin. Med. 2024, 13, 3143. [Google Scholar] [CrossRef] [PubMed]
- Cacciola, G.; Giustra, F.; Bosco, F.; Sabatini, L.; Risitano, S.; De Meo, F.; Braconi, L.; Cavaliere, P.; Massè, A.; Solarino, G. Long-Term Follow-Up of Medial Pivot Total Knee Arthroplasty: A Systematic Review of the Current Evidence. Prosthesis 2023, 5, 622–634. [Google Scholar] [CrossRef]
- D’Ettorre, M.; Tambasco, D.; Mingrone, G.; Bracaglia, R. Predictive value of biochemical and tissue modifications for wound healing in post-bariatric patients. Eur. J. Plast. Surg. 2017, 40, 549–554. [Google Scholar] [CrossRef]
- Susini, P.; Marcaccini, G.; Cuomo, R.; Grimaldi, L.; Nisi, G. Thighs lift in the post-bariatric patient - A systematic review. J. Plast. Reconstr. Aesthet. Surg. 2024, 98, 357–372. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, D.J.; Kruchevsky, D. Interplay of Oblique Flankplasty with Vertical Medial Thighplasty. Clin. Plast. Surg. 2024, 51, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Tambasco, D.; Albanese, R.; Tomaselli, F.; Pinto, V.; Pinelli, M.; De Santis, G. Minimizing Thighplasty Complications: A Combined Approach of J Medial Pattern and Helium-Plasma Assisted Liposculpture. Plast Reconstr Surg. 2025, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Mathes, D.W.; Kenkel, J.M. Current concepts in medial thighplasty. Clin. Plast. Surg. 2008, 35, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Le Louarn, C.; Pascal, J.F. The concentric medial thigh lift. Aesthetic Plast. Surg. 2004, 28, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Labardi, L.; Gentile, P.; Gigliotti, S.; Marianetti, M.; Colicchia, G.M.; Pascali, M.; Brinci, L.; Cervelli, V. Medial thighplasty: Horizontal and vertical procedures after massive weight loss. J. Cutan. Aesthet. Surg. 2012, 5, 20–25. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aboueldahab, A.K. Liposuction-assisted medial thigh lift in obese and non obese patients. J. Cutan. Aesthet. Surg. 2013, 6, 217–225. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gusenoff, J.A.; Coon, D.; Nayar, H.; Kling, R.E.; Rubin, J.P. Medial thigh lift in the massive weight loss population: Outcomes and complications. Plast. Reconstr. Surg. 2015, 135, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.M.; Small, K.; Stark, R.; Constantine, R.S.; Farkas, J.P.; Kenkel, J.M. Personal Evolution in Thighplasty Techniques for Patients Following Massive Weight Loss. Aesthet. Surg. J. 2017, 37, 1124–1135. [Google Scholar] [CrossRef] [PubMed]
- Schwaiger, K.; Russe, E.; Heinrich, K.; Ensat, F.; Steiner, G.; Wechselberger, G.; Hladik, M. Thighplasty: Improving aesthetics through revival of the medial, horizontal procedure: A safe and scar-saving option. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Hunstad, J.P.; Kortesis, B.G.; Knotts, C.D. Avulsion Thighplasty: Technique Overview and 6-Year Experience. Plast. Reconstr. Surg. 2016, 137, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, T.E. Fascial anchoring technique in medial thigh lifts. Plast. Reconstr. Surg. 1988, 82, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, S.; Datta, G.; Bocchiotti, M.A.; Boriani, F.; Obbialero, F.D.; Fraccalvieri, M. Limb contouring after massive weight loss: Functional rather than aesthetic improvement. Obes. Surg. 2009, 19, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Jandali, Z.; Loh, C.Y.; Athanassopoulos, T.; Müller, K. An improved dual approach to post bariatric contouring - Staged liposuction and modified medial thigh lift: A case series. Indian. J. Plast. Surg. 2014, 47, 232–235. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schmidt, M.; Pollhammer, M.S.; Januszyk, M.; Duscher, D.; Huemer, G.M. Concomitant Liposuction Reduces Complications of Vertical Medial Thigh Lift in Massive Weight Loss Patients. Plast. Reconstr. Surg. 2016, 137, 1748–1757. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, V.; Colicchia, G.M.; Cervelli, V. Medial Thigh Contouring After Massive Weight Loss: The Liposuction-Assisted Medial Thigh Lift (LAMeT). J. Cutan. Aesthet. Surg. 2020, 13, 305–313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Di Pietro, V.; Gianfranco, M.C.; Cervelli, V.; Gentile, P. Medial Thigh Contouring in Massive Weight Loss: A Liposuction-Assisted Medial Thigh Lift. World J. Plast. Surg. 2019, 8, 171–180. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Armijo, B.S.; Campbell, C.F.; Rohrich, R.J. Four-step medial thighplasty: Refined and reproducible. Plast Reconstr Surg. 2014, 134, 717e–725e. [Google Scholar] [CrossRef] [PubMed]
- Bertheuil, N.; Duisit, J.; Bekara, F.; Watier, E.; Gandolfi, S.; Bergeat, D. Risk Factors for Complications after J Medial Thighplasty following Massive Weight Loss: A Multivariate Analysis of 94 Consecutive Patients. Plast Reconstr Surg. 2021, 148, 540e–547e. [Google Scholar] [CrossRef] [PubMed]
- Özkaya, Ö.; Yasak, T. Vertical Medial Thigh Lift with the “Anchor L Liposculpture” Technique in Massive Weight Loss Patients: Preliminary results. Aesthetic Plast. Surg. 2022, 46, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Bracaglia, R.; Tambasco, D.; Gentileschi, S.; D’Ettorre, M. L-Shaped Lipothighplasty. Ann. Plast. Surg. 2015, 75, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.L.M.M.; Youngman, K.L.; Packer, R.M.A.; O’Neill, D.G.; Kafarnik, C. A Review of Clinical Outcomes, Owner Understanding and Satisfaction following Medial Canthoplasty in Brachycephalic Dogs in a UK Referral Setting (2016–2021). Animals 2023, 13, 2032. [Google Scholar] [CrossRef]
- Garoosi, K.; Mundra, L.; Jabbari, K.; Winocour, J.; Iorio, M.L.; Mathes, D.W.; Kaoutzanis, C. Comorbid Conditions and Complications in Body Contouring Surgery: A Retrospective Review. Aesthet Surg. J. Open Forum. 2023, 5, ojad080. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mosleh, M.M.; Sohn, M.-J. Optimizing Therapeutic Strategies for Syringomyelia Associated with Tethered Cord Syndrome: A Comprehensive Review. Children 2024, 11, 961. [Google Scholar] [CrossRef]
- Capella, J.F. The vertical medial thigh lift. Clin. Plast. Surg. 2014, 41, 727–743. [Google Scholar] [CrossRef] [PubMed]
- Simone, P.; Carusi, C.; Del Buono, R.; Persichetti, P. Medial thigh lift in post-bariatric patients: Our encouraging experience. J. Plast. Surg. Hand Surg. 2016, 50, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.R., Jr. The thigh lift. J. Int. Coll. Surg. 1957, 27, 330–334. [Google Scholar] [PubMed]
- Triana, L.; Palacios Huatuco, R.M.; Campilgio, G.; Liscano, E. Trends in Surgical and Nonsurgical Aesthetic Procedures: A 14-Year Analysis of the International Society of Aesthetic Plastic Surgery-ISAPS. Aesthetic Plast. Surg. 2024, 48, 4217–4227, Erratum in Aesthetic Plast. Surg. 2024, 48, 4601. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.A.; Chan, L.K.W.; Lee, A.W.K.; Lee, C.H.; Wan, J.; Yi, K.-H. Laser-Assisted Lipolysis Versus Surgical Fat Removal: A Review of Efficacy, Safety, and Patient Satisfaction. Cosmetics 2024, 11, 164. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Author | N° Patient | Year | Country | Demographic Data | Surgical Technique | Follow Up | Complications | Key Points |
|---|---|---|---|---|---|---|---|---|
| The Vertical Medial Thigh Lift Joseph F. Capella, MD [29] | 335 | 2014 | USA | unspecified | Vertical T-shape TL | 12 months | Skin dehiscence Seroma Infection Hematoma Skin necrosis Deep vein thrombosis Pulmonary embolism | Medial thigh lifts that are consistently effective are possible when the vertical and horizontal components of the thigh deformity and their relationship to the lower body are recognized. Our approach to the medial thighs, the correction of lower body deformities before a vertical medial thigh lift with liposuction. |
| The Concentric Medial Thigh Lift C. Le Louarn M.D. [9] | 25 | 2004 | France | unspecified | Horizontal medial TL | unspecified | Dehiscence Scar migration Scar widening Insufficient lift effect | The concentric axes of traction, the new incision pattern, the superficial dissection avoiding any dead space and lymphatic damage, the classic anchoring sutures on nonundermined tissue, and the cutaneous excision on demand address our desire for a more reliable and efficient medial thigh lift. |
| Limb Contouring after Massive Weight Loss: Functional Rather than Aesthetic Improvement S. Bruschi M.D. [17] | 35 | 2009 | Italy | 46 yo | Horizontal/Vertical T-shape TL | 12 months | Hematoma Anaemization Seroma Wound dehiscence Haemorrhage Infection Fistula DTV/TEP Abscess | As the follow-up is at least 1 year, we can state that the satisfaction is durable in addition to being high. No reoperation occurred in the period of time occurred and after it to any of the included patients. Nearly all patients declared a relevant esthetic improvement. |
| Medial Thighplasty: Horizontal and Vertical Procedures after Massive Weight Loss Labardi L M.D. [10] | 45 | 2012 | Italy | 48 yo | 15 Horizontal TL; 15 Vertical TL; 15 Vertical T-shape TL | 60 months | Scar migration Scar widening | Medial thigh lift surgery is free of major complications, if the basic anatomy of this region is understood, in order to preserve important structures such as the great saphenous vein and femoral vessels. The only complication is the presence of extensive and visible scars along the thigh, in the case of vertical procedure, and along the inguinal canal, with a possible distortion of the labia major, in the case of horizontal procedure. |
| Liposuction-assisted Medial Thigh Lift in Obese and Non-Obese Patients Aboueldahab Khalaf Aboueldahab M.D. [11] | 25 | 2013 | Egypt | 25–45 yo | 20 Horizontal TL 5 T shape TL | 12 months | Need for blood transfusion | Liposuction assisted thigh lift improves thigh contour while providing discontinuous thigh undermining. Anchoring of the skin flap to the Colles’ fascia and to the fascia of the adductor muscles reinforces the transverse medial lift and avoids scar descent. |
| Four-Step Medial Thighplasty Bryan S. Armijo, M.D. [22] | 45 | 2014 | USA | 30 to 67 years | Vertical L shape TL | 0.5 months to 9.5 years | Dehiscence Under-correction | The four-step surgical algorithm for medial thighplasty includes: (1) inverted L-shaped anterior markings marked pre-operatively; (2) superwet infiltration of the circumferential thigh; (3) circumferential combined UAL/SAL in an intermediate level except for a key transition to a superficial level in the area to be excised to prevent injury to the saphenous venous system; and (4) pre-designed and patterned skin excision that is rechecked intraoperatively. |
| An Improved Dual Approach to Post Bariatric Contouring—Staged Liposuction and Modified Medial Thigh Lift: A Case Series Zaher Jandali M.D. [18] | 21 | 2014 | India | 38 yo | modified T-shape TL with buried de-epithelialised dermal flap | 6–12 months | Dehischence | The low-seroma rate in this technique is probably due to the reduced of dead space with a buried dermal flap and the combined used to liposuction which generally preserves lymphatic channels. |
| Medial Thigh Lift in the Massive Weight Loss Population: Outcomes and Complications Jeffrey A. Gusenoff, M.D. [12] | 106 | 2015 | USA | 45.1 ± 10.2 yo | 14 Horizontal TL 24 Vertical short T-shape TL 68 Vertical T-shape TL | >70 months | Seroma Dehiscence Bleeding Infection Edema | Complications are highest for the full-length vertical thighplasty (74 percent) and less for the short-scar (67 percent) and horizontal (43 percent) procedures. Age, hypothyroidism, hypertension, and liposuction outside of the area of resection may contribute to postoperative complications. |
| Personal Evolution in Thighplasty Techniques for Patients Following Massive Weight Loss Shelly M. Xie M.D. [13] | 65 | 2017 | USA | 43–46.1 yo | 26 Horizontal TL 39 Vertical T-shape TL | 14.6 months | Hematoma Lymphocele/Seroma Erythema Necrosis Dehiscence Infection | Horizontal vector fixation group had a significant increased use of liposuction intraoperatively and a significant decrease in incidence of lymphocele/seroma and infection postoperatively. Our findings reinforce our theorem: limited dissection of the perineum reduces postoperative sequelae while maintaining equivocal wound dehiscence or necrosis. |
| Risk Factors for Complications after J Medial Thighplasty Following Massive Weight Loss: A Multivariate Analysis of 94 Consecutive Patients Nicolas Bertheuil, M.D., Ph.D. [23] | 94 | 2021 | France | 44 yo | Vertical J-shape TL | 12 months | Surgical revision Hospital readmission Emergency room visit Minor complications were those that could be treated in an outpatient clinic Wound dehiscence | In conclusion, we found that a high body mass index and advanced age were independent risk factors for complications of vertical J medial thighplasty. |
| Concomitant Liposuction Reduces Complications of Vertical Medial Thigh Lift in Massive Weight Loss Patients Manfred Schmidt, M.D. [19] | 59 | 2016 | Austria | 41.5 ± 9.1 yo | Vertical T-shape TL 30 Vertical T-shape TL + liposuction | 36 ± 21 months | Seroma Hematoma Wound dehiscence Wound infection Surgical revision | The combined approach (liposuction + vertical medial thighplasty) has led to a significant reduction of complications (seroma, hematoma, surgical revision). |
| Thighplasty: Improving Aesthetics Through Revival of the Medial, Horizontal Procedure: A Safe and Scar-Saving Option Karl Schwaiger M.D. [14] | 25 | 2017 | Austria | 43 yo | Horizontal TL | 32 months | Hematoma Seroma Wound dehiscence Infection Return to OR | Compared to other thighplasty procedures, we observed fewer complications, which indicates a reduction in postoperative morbidity. Therefore, we estimate that the main reason for employing this procedure is the avoidance of the vertical scar and its associated short- and long-term problems and complications (smaller wound surface, better aesthetic appearance, fewer scar irritation, and pain). |
| Vertical Medial Thigh Lift with the ‘Anchor L Liposculpture’ Technique in Massive Weight Loss Patients: Preliminary results Özay Özkaya M.D. [24] | 33 | 2021 | Turkey | 40.2 ± 10.7 yo | Vertical L-shape TL with dermal flap | 21.9 ± 19.4 months | Hematoma Dehiscence Infection Lymphedema Lymphocele Scar migration | Anchor L Liposculpture technique is an easy, apply and reliable technique aimed better surgical results and lower complication rates. Also, it should be considered that an increased amount of liposuction may lead to an increase the complication rates. |
| L Shaped Lipoplasty Roberto Bracaglia, MD [25] | 16 | 2015 | Italy | 41 yo | Vertical L-shape TL | 24 months | Dehiscence Hematoma Lymphedema Lymphocele Wound infection Skin necrosis Tep/TVP | (1) The excess skin and subcutaneous tissue are concentrated exclusively in the anterior medial thigh region (2) The vertical extent is necessary in all patients with moderate to severe laxity and permits a better definition of the medial profile (3) The anchorage to the fascial system of Colles prevents recurrence of ptosis and reduces the surface forces acting on the skin f laps, preventing further risk of dehiscence and necrosis (4) Previous selective liposuction is a crucial preliminary step to prevent vascular and lymphatic complications and to allow only epidermis and dermis resection of the medial thigh area |
| Medial Thigh Contouring After Massive Weight Loss: The Liposuction-Assisted Medial Thigh Lift (LAMeT) Verdiana Di Pietro M.D. [20] | 54 | 2020 | Italy | 44,16 yo | 25 Vertical T-shape TL 26 LAMet | 12 months | Seroma Hematoma Wound dehiscence Wound infection Surgical revision Vulva deformation Scar migration | The Liposuction-Assisted Medial Thigh Lift (LAMeT) preserves lymphatic and blood vessels and allows a more anatomical resection of the excess skin. Thus, the incidence of postoperative complications is lower, and the patients heal faster. Complications were observed in 35.7% of the patients that underwent the standard technique and in 3.8% patients that underwent the LAMeT. The most frequent complication was seroma. |
| Avulsion Thighplasty: Technique Overview and 6-Year Experience Joseph P. Hunstad, M.D. [15] | 42 | 2015 | USA | 49 yo | 14 Horizontal TL 28 Vertical T-shape TL | 18.3 months | Tep/TVP Hematoma Dehiscence Cellulitis Seroma Lymphedema | Avulsion thighplasty has a low incidence of major complications and minimizes the difficult-to-treat problems of lymphatic origin. It is imperative to counsel patients preoperatively about the high risk of minor complications. |
| Medial Thigh Lift in Post-bariatric Patients: Our Encouraging Experience Pierfranco Simone M.D. [30] | 46 | 2016 | Italy | 42 yo | vertical T + lipo | 12 months | TEP/TVP Wound dehiscence Haematoma Seroma Infection Skin necrosis Lymphoceles Lymphoedema Caudal scar migration Genital distortion Recurrent ptosis | Liposuction with inherent sparing of subcutaneous lymphatics, early mobilisation, and appropriate postoperative management have a pivotal role in reducing complications. |
| Medial Thigh Contouring in Massive Weight Loss: A Liposuction-Assisted Medial Thigh Lift Verdiana Di Pietro M.D. [21] | 24 | 2019 | Italy | 44.16 yo | Vertical T-shape TL | 44 months | Seroma Hematoma Dehiscence Infection Surgical revision | The Liposuction-Assisted Medial Thigh Lift technique preserves the great majority of lymphatics and blood vessels and nerves and allows a more anatomical resection of the excess skin. Thus, it reduces postoperative complications and allows the patient to heal faster. |
| Fascial Anchoring Technique in Medial Thigh Lift Lockwood, M.D. [16] | 18 | 1988 | USA | 35–45 yo | Horizontal TL | 12 months | Infection Hematoma Dehiscence Skin necrosis | Women with very heavy thighs may have an increased risk of recurrence of ptosis. In patients who are marginal candidates for trochanteric liposuction due to decreased skin tone, the medial thigh lift can reduce the upper thigh diameter to an extent that allows a more conservative liposuction of the lateral thigh. |
| Complication | Liposuction (%) | No Liposuction (%) | p-Value |
|---|---|---|---|
| Number of Patients | 849 | 133 | n/a |
| Overall | 36.75 | 70.68 | <0.001 |
| TVP | 0.12 | 0.00 | 1 |
| Re-operation | 2.24 | 3.76 | 0.45 |
| Hematoma | 1.30 | 6.77 | <0.001 |
| Infection | 1.77 | 9.02 | <0.001 |
| Scar migration | 0.71 | 7.52 | <0.001 |
| Dehiscence | 21.20 | 18.05 | 0.47 |
| Necrosis | 0.24 | 0.75 | 0.87 |
| Lymphedema | 0.24 | 0.00 | 1 |
| Lymphocele/seroma | 8.95 | 24.81 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albanese, R.; Blessent, C.G.F.; Tomaselli, F.; De Santis, G.; Pinto, V.; Pinelli, M.; Buccheri, E.M.; Tambasco, D. A Comprehensive Review of Medial Thighplasty: The Role of Liposuction in Reducing Complications and Optimizing Patient Outcomes. J. Clin. Med. 2025, 14, 2426. https://doi.org/10.3390/jcm14072426
Albanese R, Blessent CGF, Tomaselli F, De Santis G, Pinto V, Pinelli M, Buccheri EM, Tambasco D. A Comprehensive Review of Medial Thighplasty: The Role of Liposuction in Reducing Complications and Optimizing Patient Outcomes. Journal of Clinical Medicine. 2025; 14(7):2426. https://doi.org/10.3390/jcm14072426
Chicago/Turabian StyleAlbanese, Roberta, Claudio Gio Francesco Blessent, Federica Tomaselli, Giorgio De Santis, Valentina Pinto, Massimo Pinelli, Ernesto Maria Buccheri, and Damiano Tambasco. 2025. "A Comprehensive Review of Medial Thighplasty: The Role of Liposuction in Reducing Complications and Optimizing Patient Outcomes" Journal of Clinical Medicine 14, no. 7: 2426. https://doi.org/10.3390/jcm14072426
APA StyleAlbanese, R., Blessent, C. G. F., Tomaselli, F., De Santis, G., Pinto, V., Pinelli, M., Buccheri, E. M., & Tambasco, D. (2025). A Comprehensive Review of Medial Thighplasty: The Role of Liposuction in Reducing Complications and Optimizing Patient Outcomes. Journal of Clinical Medicine, 14(7), 2426. https://doi.org/10.3390/jcm14072426