
Pain and Tooth Movement During Orthodontic Leveling and Alignment—A Questionnaire-Based Study

 ,
,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Adjustment
2.2. Ethical Approval of the Survey and Administration of the Survey
2.3. Statistical Analysis
3. Results
3.1. Sample Size Adjustment
3.2. Demographic Characteristics of the Respondents
3.2.1. Age
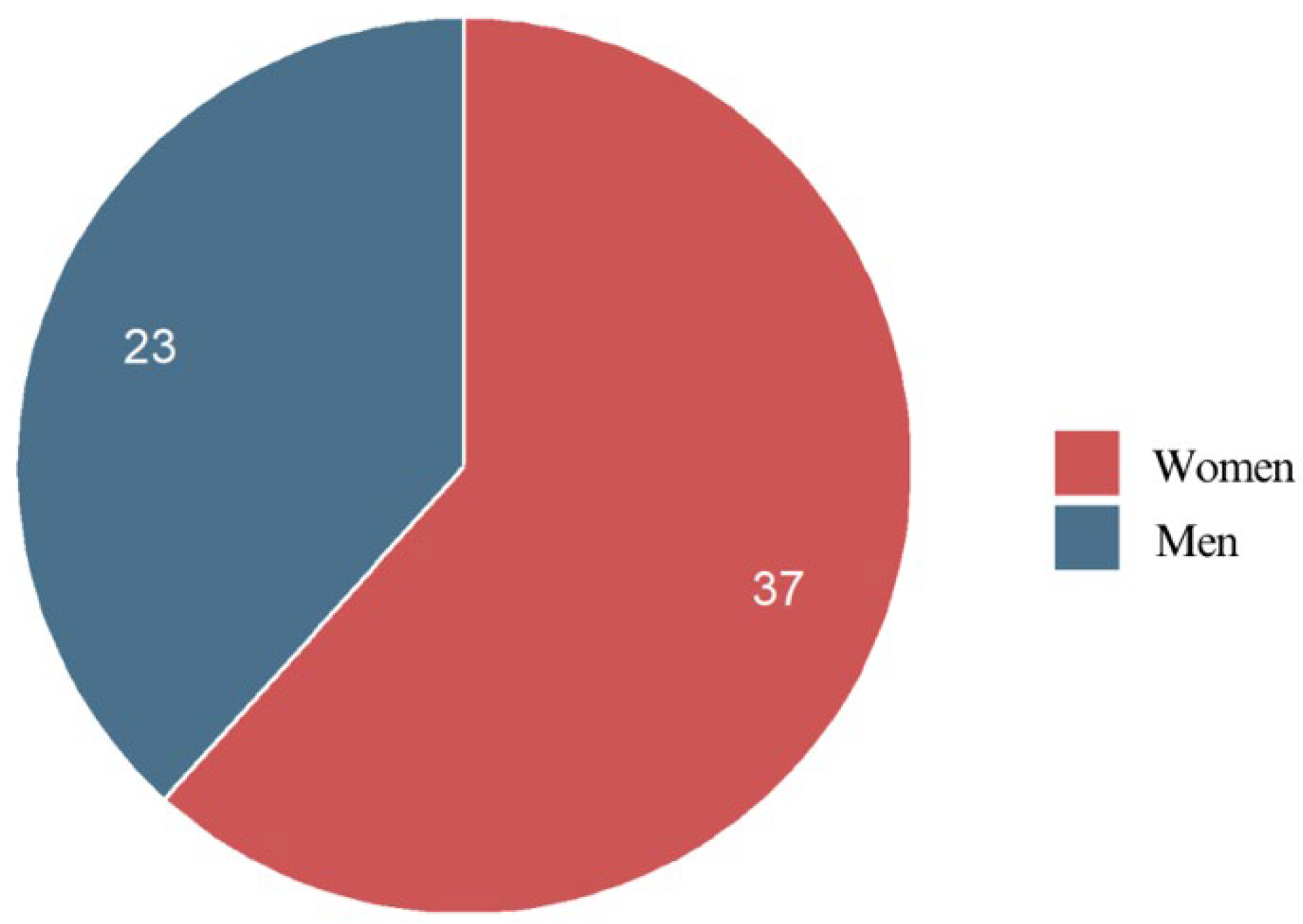
3.2.2. Gender
3.2.3. Place of Residence
3.2.4. Educational Level
3.3. Orthodontic Treatment Details
3.3.1. Duration of Orthodontic Treatment
3.3.2. Braces Placement
3.4. Pain Experience
3.4.1. Maximum Pain Level
3.4.2. Pain Onset
3.4.3. Pain Intensity Spike
3.4.4. Pain Characteristics
3.4.5. Impact of External Stimuli
3.4.6. Common Pain Triggers
3.4.7. Tooth Pain Patterns
3.4.8. Impact of Gender on Pain
3.4.9. Impact of Age on Pain
3.4.10. Impact of Place of Residence on Pain
3.4.11. Impact of Simultaneous vs. Nonsimultaneous Treatment on Pain
3.4.12. Relationship Between Treatment Time and Pain Intensity
3.4.13. Impact of External Stimuli on Pain
3.4.14. Impact of Educational Level on Pain
3.4.15. Relationship Between Educational Level and Pain Medication Use
3.4.16. Relationship Between Educational Level and Tooth Movement Perception
3.5. Pain Management
3.5.1. Medication Usage
3.5.2. Pain Medication Preferences
3.5.3. Impact of Gender on Medication Usage
3.5.4. Impact of Medication Usage on Pain Level
3.6. Tooth Movement Perception
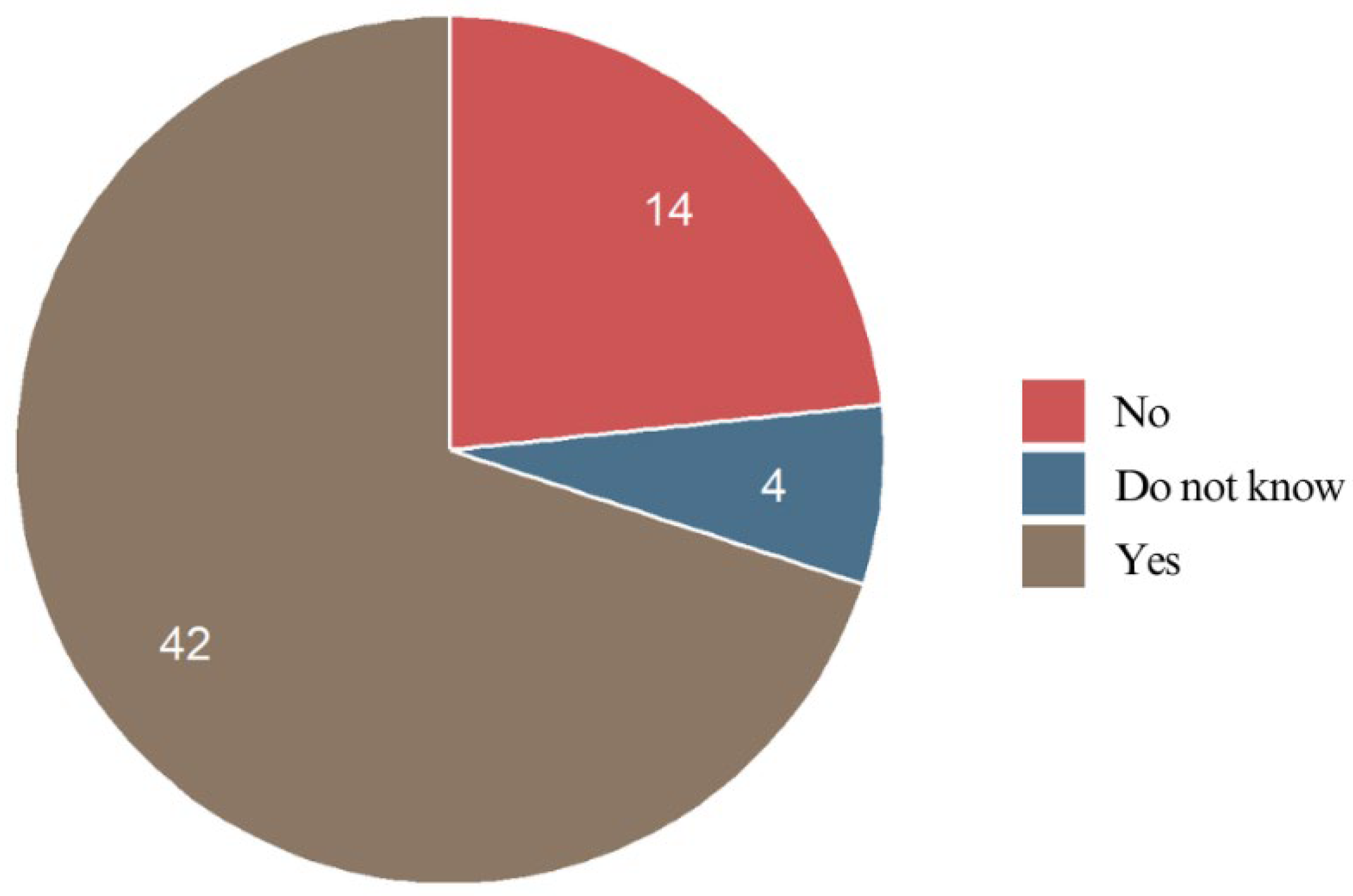
3.6.1. Perception of Immediate Tooth Movement
3.6.2. Teeth Most Affected by Initial Tooth Movement
3.6.3. Impact of Age on Tooth Movement Perception
3.6.4. Relationship Between Tooth Movement Perception and Most Painful Teeth
3.6.5. Relationship Between Braces Placement and Tooth Movement Perception
3.7. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PDL | Periodontal Ligament |
| VAS | Visual Analogue Scale |
| SD | Standard Deviation |
| rho | Spearman’s Rank Correlation Coefficient |
| S | Sum of Squared Differences |
| N | Sample Size |
| mm | Millimeters |
References
- Krishnan, V.; Davidovitch, Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 469.e1–469.e32. [Google Scholar] [CrossRef]
- Meeran, N. Biological response at the cellular level within the periodontal ligament on application of orthodontic force—An update. J. Orthod. Sci. 2012, 1, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Sergl, H.G.; Klages, U.; Zentner, A. Pain and discomfort during orthodontic treatment: Causative factors and effects on compliance. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Yan, X.; Zhao, R.; Shan, Y.; Chen, Y.; Jian, F.; Long, H.; Lai, W. Comparison of pain perception, anxiety, and impacts on oral health-related quality of life between patients receiving clear aligners and fixed appliances during the initial stage of orthodontic treatment. Eur. J. Orthod. 2020, 43, 353–359. [Google Scholar] [CrossRef]
- Li, Q.; Du, Y.; Yang, K. Comparison of pain intensity and impacts on oral health-related quality of life between orthodontic patients treated with clear aligners and fixed appliances: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 920. [Google Scholar] [CrossRef]
- Salgado, K.R.; Normando, D.; Brandão, G.A.M. Is catastrophising associated with pain perception in early phase of orthodontic treatment? A cohort study. J. Oral Rehabil. 2022, 49, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Sew Hoy, W.H. Genetic Factors Associated with Orthodontic Pain in Children and Adolescents: A Pilot Study. Ph.D. Thesis, University of Otago, Dunedin, New Zealand, 2017. [Google Scholar]
- Jones, M.; Chan, C. The Pain and Discomfort Experienced During Orthodntic Treatment: A randomized controlled clinical trial of two intial aligning arch wires. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Bergius, M.; Kiliaridis, S.; Berggren, U. Pain in orthodontics: A review and discussion of the literature. J. Orofac. Orthop. Der Kieferorthopadie 2000, 61, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Toyama, N.; Ono, T.; Ono, T.; Nakashima, T. The interleukin-6 signal regulates orthodontic tooth movement and pain. Biochem. Biophys. Res. Commun. 2023, 684, 149068. [Google Scholar] [CrossRef] [PubMed]
- Inauen, D.S.; Papadopoulou, A.K.; Eliades, T.; Papageorgiou, S.N. Pain profile during orthodontic levelling and alignment with fixed appliances reported in randomized trials: A systematic review with meta-analyses. Clin. Oral Investig. 2023, 27, 1851–1868. [Google Scholar] [CrossRef] [PubMed]
- Calculating the Number of Respondents You Need. Available online: https://help.surveymonkey.com/en/surveymonkey/solutions/calculating-respondents/ (accessed on 6 January 2025).
- Akaike, H. Information Theory and an Extension of the Maximum Likelihood Principle. In Breakthroughs in Statistics; Kotz, S., Johnson, N.L., Eds.; Springer: New York, NY, USA, 1992; Volume 1, pp. 610–624. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://www.R-project.org/ (accessed on 30 March 2025).
- Maltha, J.C.; Kuijpers-Jagtman, A.M. Mechanobiology of orthodontic tooth movement: An update. J. World Fed. Orthod. 2023, 12, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Shimada, E.; Kanetaka, H.; Hihara, H.; Kanno, A.; Kawashima, R.; Nakasato, N.; Igarashi, K. Effects of pain associated with orthodontic tooth movement on tactile sensation of periodontal ligaments. Clin. Oral Investig. 2023, 28, 36. [Google Scholar] [CrossRef] [PubMed]
- Horinuki, E.; Shinoda, M.; Shimizu, N.; Koshikawa, N.; Kobayashi, M. Orthodontic Force Facilitates Cortical Responses to Periodontal Stimulation. J. Dent. Res. 2015, 94, 1158–1166. [Google Scholar] [CrossRef] [PubMed]
- Kyrkanides, S.; Huang, H.; Faber, R.D. Neurologic Regulation and Orthodontic Tooth Movement. In Frontiers of Oral Biology; Kantarci, A., Will, L., Yen, S., Eds.; S. Karger AG: Berlin, Germany, 2016; Volume 18, pp. 64–74. ISBN 978-3-318-05479-8. [Google Scholar]
- Sfeatcu, R.; Balgiu, B.A.; Mihai, C.; Petre, A.; Pantea, M.; Tribus, L. Gender Differences in Oral Health: Self-Reported Attitudes, Values, Behaviours and Literacy among Romanian Adults. J. Pers. Med. 2022, 12, 1603. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C. Orthodontic tooth movement: The biology and clinical implications. Kaohsiung J. Med. Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Lander, J.; Fowler-Kerry, S.; Hargreaves, A. Gender Effects in Pain Perception. Percept. Mot. Ski. 1989, 68, 1088–1090. [Google Scholar] [CrossRef]
- Miller, C.; Newton, S.E. Pain Perception and Expression: The Influence of Gender, Personal Self-Efficacy, and Lifespan Socialization. Pain Manag. Nurs. 2006, 7, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Lautenbacher, S.; Peters, J.H.; Heesen, M.; Scheel, J.; Kunz, M. Age changes in pain perception: A systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci. Biobehav. Rev. 2017, 75, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Mehuys, E.; Crombez, G.; Paemeleire, K.; Adriaens, E.; Van Hees, T.; Demarche, S.; Christiaens, T.; Van Bortel, L.; Van Tongelen, I.; Remon, J.-P.; et al. Self-Medication With Over-the-Counter Analgesics: A Survey of Patient Characteristics and Concerns About Pain Medication. J. Pain 2019, 20, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Olteanu, C.D.; Bucur, S.-M.; Chibelean, M.; Bud, E.S.; Păcurar, M.; Feștilă, D.G. Pain Perception during Orthodontic Treatment with Fixed Appliances. Appl. Sci. 2022, 12, 6389. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Response | Number | Proportion (%) |
|---|---|---|
| Upper incisors | 35 | 58.3 |
| Upper premolars and molars | 29 | 48.3 |
| Lower incisors | 17 | 28.3 |
| Lower premolars and molars | 10 | 16.7 |
| Upper canines | 10 | 16.7 |
| Lower canines | 5 | 8.3 |
| Estimate | S.D. | t.stat | p | |
|---|---|---|---|---|
| (Intercept) | 45.92 | 6.411 | 7.162 | <0.001 |
| Gender/male | −9.295 | 6.375 | −1.458 | 0.151 |
| Age group/25–34 | −13.05 | 6.413 | −2.035 | 0.047 * |
| Age group/35–50 | 12.25 | 8.957 | 1.368 | 0.177 |
| Chronic diseases | 13.46 | 7.156 | 1.881 | 0.065 |
| Medication usage | 18.62 | 6.997 | 2.661 | 0.010 * |
| R2 | Adjusted R2 | F [5, 54] | p | |
| 0.2957 | 0.2305 | 4.5 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prajwos, E.; Jedliński, M.; Król, M.; Kaczmarek, M.; Grabarczyk, A.; Kaźmierczak, P.; Janiszewska-Olszowska, J. Pain and Tooth Movement During Orthodontic Leveling and Alignment—A Questionnaire-Based Study. J. Clin. Med. 2025, 14, 2524. https://doi.org/10.3390/jcm14072524
Prajwos E, Jedliński M, Król M, Kaczmarek M, Grabarczyk A, Kaźmierczak P, Janiszewska-Olszowska J. Pain and Tooth Movement During Orthodontic Leveling and Alignment—A Questionnaire-Based Study. Journal of Clinical Medicine. 2025; 14(7):2524. https://doi.org/10.3390/jcm14072524
Chicago/Turabian StylePrajwos, Eryk, Maciej Jedliński, Małgorzata Król, Michał Kaczmarek, Alicja Grabarczyk, Patrycja Kaźmierczak, and Joanna Janiszewska-Olszowska. 2025. "Pain and Tooth Movement During Orthodontic Leveling and Alignment—A Questionnaire-Based Study" Journal of Clinical Medicine 14, no. 7: 2524. https://doi.org/10.3390/jcm14072524
APA StylePrajwos, E., Jedliński, M., Król, M., Kaczmarek, M., Grabarczyk, A., Kaźmierczak, P., & Janiszewska-Olszowska, J. (2025). Pain and Tooth Movement During Orthodontic Leveling and Alignment—A Questionnaire-Based Study. Journal of Clinical Medicine, 14(7), 2524. https://doi.org/10.3390/jcm14072524