
Trauma Burden Affected People with Multiple Sclerosis During SARS-CoV-2 Pandemic

 , , ,
, , , 
Abstract
1. Introduction
2. Methods
2.1. Study Population and Inclusion Criteria
2.2. Data Acquisition
2.2.1. Baseline Data
2.2.2. Follow-Up Data During the SARS-CoV-2 Pandemic
2.3. Statistics
3. Results
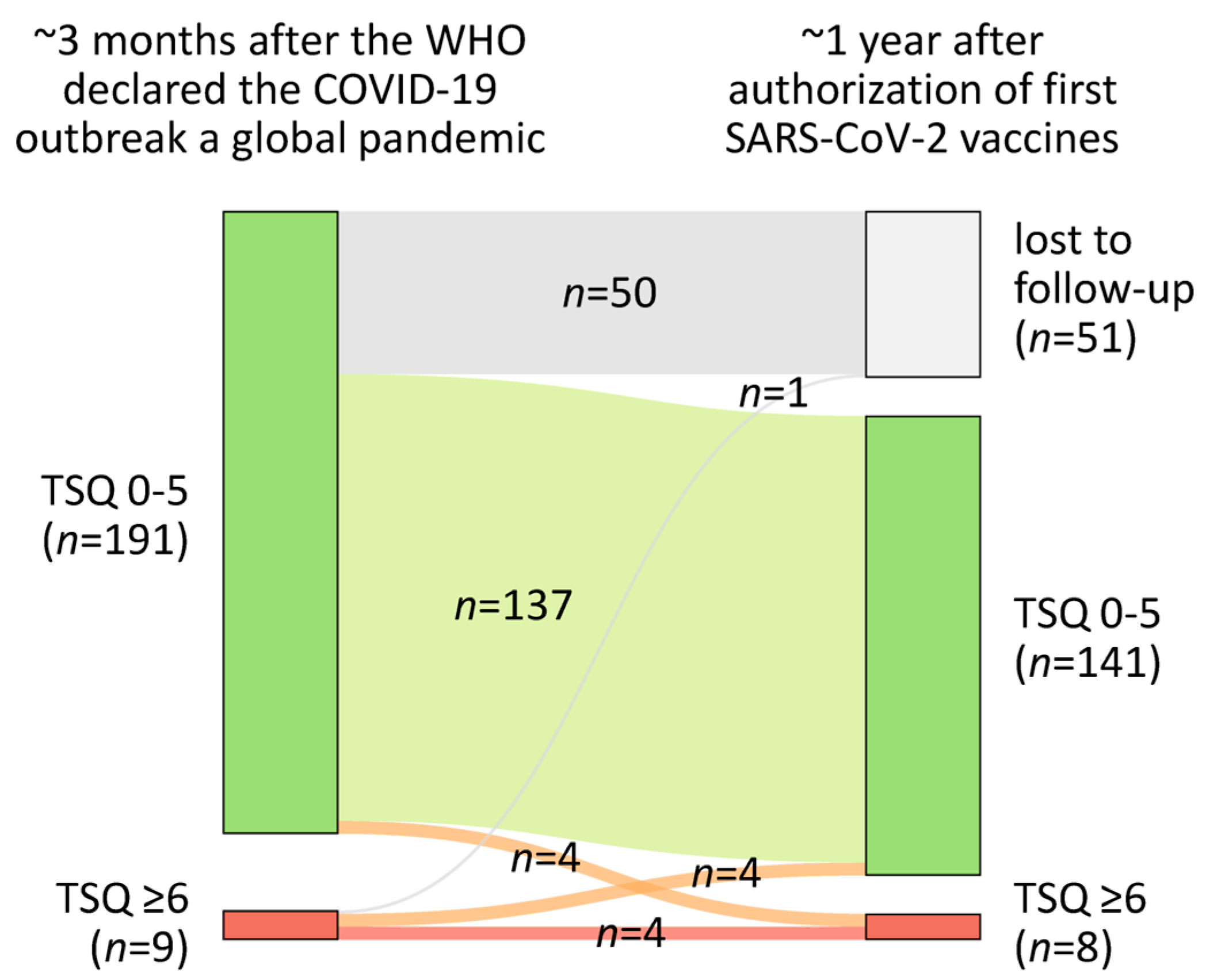
3.1. Prevalence of Probable PTSD During the SARS-CoV-2 Pandemic in Patients with MS
3.2. Demographic and Clinical Comparison of MS Patients with and Without Probable PTSD
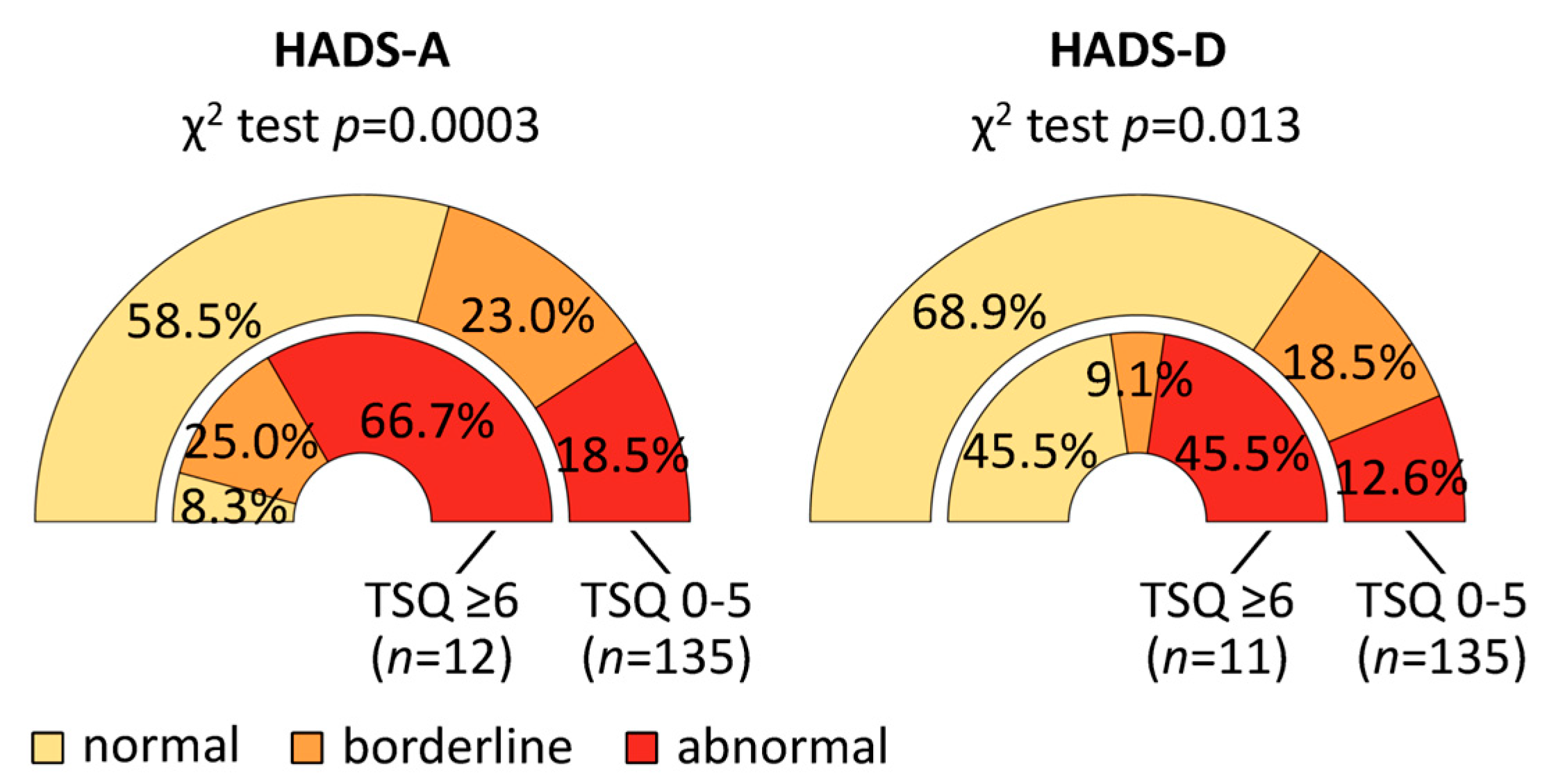
3.3. Probable PTSD in Association with Personality Characteristics, Symptoms of Anxiety and Depression and Mental, Physical, and Social Burden
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Kleber, R.J. Trauma and Public Mental Health: A Focused Review. Front. Psychiatry 2019, 10, 451. [Google Scholar] [CrossRef]
- Benjet, C.; Bromet, E.; Karam, E.G.; Kessler, R.C.; McLaughlin, K.A.; Ruscio, A.M.; Shahly, V.; Stein, D.J.; Petukhova, M.; Hill, E.; et al. The epidemiology of traumatic event exposure worldwide: Results from the World Mental Health Survey Consortium. Psychol. Med. 2016, 46, 327–343. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, D.G.; Resnick, H.S.; Milanak, M.E.; Miller, M.W.; Keyes, K.M.; Friedman, M.J. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J. Trauma. Stress. 2013, 26, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Koenen, K.C.; Ratanatharathorn, A.; Ng, L.; McLaughlin, K.A.; Bromet, E.J.; Stein, D.J.; Karam, E.G.; Meron Ruscio, A.; Benjet, C.; Scott, K.; et al. Posttraumatic stress disorder in the World Mental Health Surveys. Psychol. Med. 2017, 47, 2260–2274. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, J.W. Posttraumatische Belastungsstörung (PTBS), MSD Manual Profi-Ausgabe. 2023. Available online: https://www.msdmanuals.com/de-de/profi/psychiatrische-erkrankungen/anst-und-stressbezogene-erkrankungen/posttraumatische-belastungsstörung-ptbs (accessed on 5 February 2025).
- Bisson, J.I.; Cosgrove, S.; Lewis, C.; Robert, N.P. Post-traumatic stress disorder. BMJ 2015, 351, h6161. [Google Scholar] [CrossRef]
- Kessler, R.C. Posttraumatic stress disorder: The burden to the individual and to society. J. Clin. Psychiatry 2000, 61 (Suppl. S5), 4–12. [Google Scholar]
- Roberts, A.L.; Gilman, S.E.; Breslau, J.; Breslau, N.; Koenen, K.C. Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychol. Med. 2011, 41, 71–83. [Google Scholar] [CrossRef]
- Kubzansky, L.D.; Koenen, K.C.; Spiro, A.; Vokonas, P.S.; Sparrow, D. Prospective study of posttraumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch. Gen. Psychiatry 2007, 64, 109–116. [Google Scholar] [CrossRef]
- Miller, M.W.; Sadeh, N. Traumatic stress, oxidative stress and post-traumatic stress disorder: Neurodegeneration and the accelerated-aging hypothesis. Mol. Psychiatry 2014, 19, 1156–1162. [Google Scholar] [CrossRef]
- Jacob, L.; Haro, J.M.; Koyanagi, A. Post-traumatic stress symptoms are associated with physical multimorbidity: Findings from the Adult Psychiatric Morbidity Survey 2007. J. Affect. Disord. 2018, 232, 385–392. [Google Scholar] [CrossRef]
- Garjani, A.; Hunter, R.; Law, G.R.; Middleton, R.M.; Tuite-Dalton, K.A.; Dobson, R.; Ford, D.V.; Hughes, S.; Pearson, O.R.; Rog, D.; et al. Mental health of people with multiple sclerosis during the COVID-19 outbreak: A prospective cohort and cross-sectional case-control study of the UK MS Register. Mult. Scler. 2022, 28, 1060–1071. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Number of COVID-19 Cases Reported to WHO (Cumulative Total)|WHO COVID-19 Dashboard. 2025. Available online: https://data.who.int/dashboards/covid19/cases (accessed on 11 April 2025).
- World Health Organization. Number of COVID-19 Deaths Reported to WHO (Cumulative Total)|WHO COVID-19 Dashboard. 2025. Available online: https://data.who.int/dashboards/covid19/deaths (accessed on 11 April 2025).
- Alirezaei, M.; Eskandarieh, S.; Sahraian, M.A.; Naser Moghadasi, A. Depression, anxiety, and fear of COVID-19 in patients with multiple sclerosis in pandemic era: A cross-sectional study. Neurol. Sci. 2022, 43, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Alschuler, K.N.; Roberts, M.K.; Herring, T.E.; Ehde, D.M. Distress and risk perception in people living with multiple sclerosis during the early phase of the COVID-19 pandemic. Mult. Scler. Relat. Disord. 2021, 47, 102618. [Google Scholar] [CrossRef]
- Bonavita, S.; Sparaco, M.; Russo, A.; Borriello, G.; Lavorgna, L. Perceived stress and social support in a large population of people with multiple sclerosis recruited online through the COVID-19 pandemic. Eur. J. Neurol. 2021, 28, 3396–3402. [Google Scholar] [CrossRef]
- Sparaco, M.; Miele, G.; Lavorgna, L.; Abbadessa, G.; Bonavita, S. Association between relapses, stress, and depression in people with multiple sclerosis during the COVID-19 pandemic. Neurol. Sci. 2022, 43, 2935–2942. [Google Scholar] [CrossRef]
- Wilski, M.; Koper, M.; Gabryelski, J.; Brola, W.; Tasiemski, T. Mental Health Status of People with Multiple Sclerosis during the COVID-19 Pandemic. J. Clin. Med. 2022, 11, 576. [Google Scholar] [CrossRef]
- Zarghami, A.; Hussain, M.A.; Campbell, J.A.; Ezegbe, C.; van der Mei, I.; Taylor, B.V.; Claflin, S.B. Psychological impacts of COVID-19 pandemic on individuals living with multiple sclerosis: A rapid systematic review. Mult. Scler. Relat. Disord. 2022, 59, 103562. [Google Scholar] [CrossRef]
- Ghaderi, S.; Berg-Hansen, P.; Bakken, I.J.; Magnus, P.; Trogstad, L.; Håberg, S.E. Hospitalization following influenza infection and pandemic vaccination in multiple sclerosis patients: A nationwide population-based registry study from Norway. Eur. J. Epidemiol. 2020, 35, 355–362. [Google Scholar] [CrossRef]
- Lechner-Scott, J.; Waubant, E.; Levy, M.; Hawkes, C.; Giovannoni, G. Is multiple sclerosis a risk factor for infections? Mult. Scler. Relat. Disord. 2020, 41, 102184. [Google Scholar] [CrossRef]
- Pawlitzki, M.; Zettl, U.K.; Ruck, T.; Rolfes, L.; Hartung, H.-P.; Meuth, S.G. Merits and culprits of immunotherapies for neurological diseases in times of COVID-19. EBioMedicine 2020, 56, 102822. [Google Scholar] [CrossRef] [PubMed]
- Persson, R.; Lee, S.; Yood, M.U.; Wagner, U.C.M.; Minton, N.; Niemcryk, S.; Lindholm, A.; Evans, A.; Jick, S. Infections in patients diagnosed with multiple sclerosis: A multi-database study. Mult. Scler. Relat. Disord. 2020, 41, 101982. [Google Scholar] [CrossRef]
- Yuan, S.; Xiong, Y.; Larsson, S.C. An atlas on risk factors for multiple sclerosis: A Mendelian randomization study. J. Neurol. 2021, 268, 114–124. [Google Scholar] [CrossRef] [PubMed]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Zettl, U.K.; Stüve, O.; Patejdl, R. Immune-mediated CNS diseases: A review on nosological classification and clinical features. Autoimmun. Rev. 2012, 11, 167–173. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; Van Der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Filippi, M.; Bar-Or, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, A.M. Multiple sclerosis. Nat. Rev. Dis. Primers 2018, 4, 43. [Google Scholar] [CrossRef]
- Rommer, P.S.; Eichstädt, K.; Ellenberger, D.; Flachenecker, P.; Friede, T.; Haas, J.; Kleinschnitz, C.; Pöhlau, D.; Rienhoff, O.; Stahmann, A.; et al. Symptomatology and symptomatic treatment in multiple sclerosis: Results from a nationwide MS registry. Mult. Scler. 2019, 25, 1641–1652. [Google Scholar] [CrossRef]
- Qian, Z.; Li, Y.; Guan, Z.; Guo, P.; Zheng, K.; Du, Y.; Yin, S.; Chen, B.; Wang, H.; Jiang, J.; et al. Global, regional, and national burden of multiple sclerosis from 1990 to 2019: Findings of global burden of disease study 2019. Front. Public Health 2023, 11, 1073278. [Google Scholar] [CrossRef]
- Heidler, F.; Bopp, T.; Schwab, M.; Hoffmann, F.; Schild, H.; Kannler, M.; Pletz, M.; Zettl, U.K. Infections and multiple sclerosis. Fortschr. Neurol. Psychiatr. 2024. online ahead of print. [Google Scholar] [CrossRef]
- Nelson, R.E.; Xie, Y.; DuVall, S.L.; Butler, J.; Kamauu, A.W.C.; Knippenberg, K.; Schuerch, M.; Foskett, N.; LaFleur, J. Multiple Sclerosis and Risk of Infection-Related Hospitalization and Death in US Veterans. Int. J. MS Care 2015, 17, 221–230. [Google Scholar] [CrossRef]
- Wijnands, J.M.; Kingwell, E.; Zhu, F.; Zhao, Y.; Fisk, J.D.; Evans, C.; Marrie, R.A.; Tremlett, H. Infection-related health care utilization among people with and without multiple sclerosis. Mult. Scler. 2017, 23, 1506–1516. [Google Scholar] [CrossRef]
- Capkun, G.; Dahlke, F.; Lahoz, R.; Nordstrom, B.; Tilson, H.H.; Cutter, G.; Bischof, D.; Moore, A.; Simeone, J.; Fraeman, K.; et al. Mortality and comorbidities in patients with multiple sclerosis compared with a population without multiple sclerosis: An observational study using the US Department of Defense administrative claims database. Mult. Scler. Relat. Disord. 2015, 4, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Loebermann, M.; Winkelmann, A.; Hartung, H.-P.; Hengel, H.; Reisinger, E.C.; Zettl, U.K. Vaccination against infection in patients with multiple sclerosis. Nat. Rev. Neurol. 2012, 8, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Luna, G.; Alping, P.; Burman, J.; Fink, K.; Fogdell-Hahn, A.; Gunnarsson, M.; Hillert, J.; Langer-Gould, A.; Lycke, J.; Nilsson, P.; et al. Infection Risks Among Patients With Multiple Sclerosis Treated With Fingolimod, Natalizumab, Rituximab, and Injectable Therapies. JAMA Neurol. 2020, 77, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Moiola, L.; Rommer, P.S.; Zettl, U.K. Prevention and management of adverse effects of disease modifying treatments in multiple sclerosis. Curr. Opin. Neurol. 2020, 33, 286–294. [Google Scholar] [CrossRef]
- Rommer, P.S.; Zettl, U.K. Managing the side effects of multiple sclerosis therapy: Pharmacotherapy options for patients. Expert. Opin. Pharmacother. 2018, 19, 483–498. [Google Scholar] [CrossRef]
- Winkelmann, A.; Loebermann, M.; Reisinger, E.C.; Hartung, H.-P.; Zettl, U.K. Disease-modifying therapies and infectious risks in multiple sclerosis. Nat. Rev. Neurol. 2016, 12, 217–233. [Google Scholar] [CrossRef]
- Achiron, A.; Dolev, M.; Menascu, S.; Zohar, D.-N.; Dreyer-Alster, S.; Miron, S.; Shirbint, E.; Magalashvili, D.; Flechter, S.; Givon, U.; et al. COVID-19 vaccination in patients with multiple sclerosis: What we have learnt by February 2021. Mult. Scler. 2021, 27, 864–870. [Google Scholar] [CrossRef]
- Moss, B.P.; Mahajan, K.R.; Bermel, R.A.; Hellisz, K.; Hua, L.H.; Hudec, T.; Husak, S.; McGinley, M.P.; Ontaneda, D.; Wang, Z.; et al. Multiple sclerosis management during the COVID-19 pandemic. Mult. Scler. 2020, 26, 1163–1171. [Google Scholar] [CrossRef]
- Ostacoli, L.; Carletto, S.; Borghi, M.; Cavallo, M.; Rocci, E.; Zuffranieri, M.; Malucchi, S.; Bertolotto, A.; Zennaro, A.; Furlan, P.M.; et al. Prevalence and significant determinants of post-traumatic stress disorder in a large sample of patients with multiple sclerosis. J. Clin. Psychol. Med. Settings 2013, 20, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Carletto, S.; Borghi, M.P.; Scavelli, F.M.; Francone, D.P.; Perucchini, M.L.M.; Cavallo, M.; Pagnini, F.; Bertolotto, A.; Oliva, F.; Ostacoli, L. Prevalence of Posttraumatic Stress Disorder in Patients With Multiple Sclerosis. J. Nerv. Ment. Dis. 2018, 206, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Zanghì, A.; D’Amico, E.; Luca, M.; Ciaorella, M.; Basile, L.; Patti, F. Mental health status of relapsing-remitting multiple sclerosis Italian patients returning to work soon after the easing of lockdown during COVID-19 pandemic: A monocentric experience. Mult. Scler. Relat. Disord. 2020, 46, 102561. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Kanning, U.P. NEO-Fünf-Faktoren-Inventar nach Costa und McCrae (NEO-FFI). Z. Arb. Organ. 2009, 53, 194–198. [Google Scholar] [CrossRef]
- Costa, P.; McCrae, R. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1992. [Google Scholar]
- Costa, P.; McCrae, R. NEO PI-R Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1992. [Google Scholar]
- Streckenbach, B.; Baldt, J.; Heidler, F.; Frahm, N.; Langhorst, S.E.; Mashhadiakbar, P.; Burian, K.; Zettl, U.K.; Richter, J. General vaccination willingness and current vaccination status in relation to clinical and psychological variables in patients with multiple sclerosis. Vaccine 2022, 40, 3236–3243. [Google Scholar] [CrossRef]
- Schwartz, E.S.; Chapman, B.P.; Duberstein, P.R.; Weinstock-Guttman, B.; Benedict, R.H.B. The NEO-FFI in Multiple Sclerosis: Internal consistency, factorial validity, and correspondence between self and informant reports. Assessment 2011, 18, 39–49. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef]
- Brändström, S.; Richter, J.; Nylander, P.-O. Further development of the Temperament and Character Inventory. Psychol. Rep. 2003, 93, 995–1002. [Google Scholar] [CrossRef]
- Fossati, A.; Cloninger, C.R.; Villa, D.; Borroni, S.; Grazioli, F.; Giarolli, L.; Battaglia, M.; Maffei, C. Reliability and validity of the Italian version of the Temperament and Character Inventory-Revised in an outpatient sample. Compr. Psychiatry 2007, 48, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Eisemann, M.; Richter, G. Zur deutschsprachigen Version des Temperament- und Charakterinventars. Z. Klin. Psychol. Psychother. 2000, 29, 117–126. [Google Scholar] [CrossRef]
- Goncalves, D.M.; Cloninger, C.R. Validation and normative studies of the Brazilian Portuguese and American versions of the Temperament and Character Inventory—Revised (TCI-R). J. Affect. Disord. 2010, 124, 126–133. [Google Scholar] [CrossRef]
- Pais-Ribeiro, J.L.; Martins da Silva, A.; Vilhena, E.; Moreira, I.; Santos, E.; Mendonça, D. The hospital anxiety and depression scale, in patients with multiple sclerosis. Neuropsychiatr. Dis. Treat. 2018, 14, 3193–3197. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef]
- Marrie, R.A.; Zhang, L.; Lix, L.M.; Graff, L.A.; Walker, J.R.; Fisk, J.D.; Patten, S.B.; Hitchon, C.A.; Bolton, J.M.; Sareen, J.; et al. The validity and reliability of screening measures for depression and anxiety disorders in multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 20, 9–15. [Google Scholar] [CrossRef]
- Walters, J.T.R.; Bisson, J.I.; Shepherd, J.P. Predicting post-traumatic stress disorder: Validation of the Trauma Screening Questionnaire in victims of assault. Psychol. Med. 2007, 37, 143–150. [Google Scholar] [CrossRef]
- Brewin, C.R. Systematic review of screening instruments for adults at risk of PTSD. J. Trauma. Stress. 2005, 18, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Brewin, C.R.; Rose, S.; Andrews, B.; Green, J.; Tata, P.; McEvedy, C.; Turner, S.; Foa, E.B. Brief screening instrument for post-traumatic stress disorder. Br. J. Psychiatry 2002, 181, 158–162. [Google Scholar] [CrossRef]
- Hofmann, A.; Seidler, G.H.; Micka, R.; Hueg, A. TSF (Trauma Screening Fragebogen). 2002. Available online: http://www.emdr-europe.institute/web2/tsf_tsqs_neu_.pdf (accessed on 5 February 2025).
- Galea, S.; Brewin, C.R.; Gruber, M.; Jones, R.T.; King, D.W.; King, L.A.; McNally, R.J.; Ursano, R.J.; Petukhova, M.; Kessler, R.C. Exposure to hurricane-related stressors and mental illness after Hurricane Katrina. Arch. Gen. Psychiatry 2007, 64, 1427–1434. [Google Scholar] [CrossRef]
- Irizar, P.; Stevelink, S.A.; Pernet, D.; Gage, S.H.; Greenberg, N.; Wessely, S.; Goodwin, L.; Fear, N.T. Probable post-traumatic stress disorder and harmful alcohol use among male members of the British Police Forces and the British Armed Forces: A comparative study. Eur. J. Psychotraumatol. 2021, 12, 1891734. [Google Scholar] [CrossRef] [PubMed]
- Houben-Wilke, S.; Goërtz, Y.M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.; van Herck, M.; Burtin, C.; Posthuma, R.; Franssen, F.M.; et al. The Impact of Long COVID-19 on Mental Health: Observational 6-Month Follow-Up Study. JMIR Ment. Health 2022, 9, e33704. [Google Scholar] [CrossRef] [PubMed]
- Knipscheer, J.; Sleijpen, M.; Frank, L.; de Graaf, R.; Kleber, R.; Have, M.T.; Dückers, M. Prevalence of Potentially Traumatic Events, Other Life Events and Subsequent Reactions Indicative for Posttraumatic Stress Disorder in the Netherlands: A General Population Study Based on the Trauma Screening Questionnaire. Int. J. Environ. Res. Public. Health 2020, 17, 1725. [Google Scholar] [CrossRef]
- Jones, G.A.L.; Colville, G.A.; Ramnarayan, P.; Woolfall, K.; Heward, Y.; Morrison, R.; Savage, A.; Fraser, J.; Griksaitis, M.J.; Inwald, D.P. Psychological impact of working in paediatric intensive care. A UK-wide prevalence study. Arch. Dis. Child. 2020, 105, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Bußgeldkatalog. Ausgangssperre Wegen Corona Bundesweit Einheitlich Geregelt. 2021. Available online: https://www.bussgeldkatalog.org/ausgangssperre-corona (accessed on 5 February 2025).
- Breslau, N.; Chilcoat, H.D.; Kessler, R.C.; Peterson, E.L.; Lucia, V.C. Vulnerability to assaultive violence: Further specification of the sex difference in post-traumatic stress disorder. Psychol. Med. 1999, 29, 813–821. [Google Scholar] [CrossRef]
- Gureje, O.; Lasebikan, V.O.; Kola, L.; Makanjuola, V.A. Lifetime and 12-month prevalence of mental disorders in the Nigerian Survey of Mental Health and Well-Being. Br. J. Psychiatry 2006, 188, 465–471. [Google Scholar] [CrossRef]
- Hepp, U.; Gamma, A.; Milos, G.; Eich, D.; Ajdacic–Gross, V.; Rössler, W.; Angst, J.; Schnyder, U. Prevalence of exposure to potentially traumatic events and PTSD. The Zurich Cohort Study. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 151–158. [Google Scholar] [CrossRef]
- Heir, T.; Bonsaksen, T.; Grimholt, T.; Ekeberg, Ø.; Skogstad, L.; Lerdal, A.; Schou-Bredal, I. Serious life events and post-traumatic stress disorder in the Norwegian population. BJPsych Open 2019, 5, e82. [Google Scholar] [CrossRef]
- Olff, M.; Primasari, I.; Qing, Y.; Coimbra, B.M.; Hovnanyan, A.; Grace, E.; Williamson, R.E.; Hoeboer, C.M. Mental health responses to COVID-19 around the world. Eur. J. Psychotraumatol. 2021, 12, 1929754. [Google Scholar] [CrossRef]
- Lotzin, A.; Krause, L.; Acquarini, E.; Ajdukovic, D.; Anastassiou-Hadjicharalambous, X.; Ardino, V.; Bondjers, K.; Böttche, M.; Dragan, M.; Figueiredo-Braga, M.; et al. Risk and protective factors for posttraumatic stress disorder in trauma-exposed individuals during the COVID-19 pandemic—Findings from a pan-European study. Eur. J. Psychotraumatol. 2022, 13, 2138099. [Google Scholar] [CrossRef]
- Olff, M. Sex and gender differences in post-traumatic stress disorder: An update. Eur. J. Psychotraumatol. 2017, 8 (Suppl. S4), 1351204. [Google Scholar] [CrossRef]
- Yehuda, R.; Hoge, C.W.; McFarlane, A.C.; Vermetten, E.; Lanius, R.A.; Nievergelt, C.M.; Hobfoll, S.E.; Koenen, K.C.; Neylan, T.C.; Hyman, S.E. Post-traumatic stress disorder. Nat. Rev. Dis. Primers 2015, 1, 15057. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- de Vries, G.-J.; Olff, M. The lifetime prevalence of traumatic events and posttraumatic stress disorder in the Netherlands. J. Trauma. Stress. 2009, 22, 259–267. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.T.V.M.; Komproe, I.H.; Van Ommeren, M.; El Masri, M.; Araya, M.; Khaled, N.; van de Put, W.; Somasundaram, D. Lifetime events and posttraumatic stress disorder in 4 postconflict settings. JAMA 2001, 286, 555–562. [Google Scholar] [CrossRef]
- Hong, S.; Kim, H.; Park, M.K. Impact of COVID-19 on post-traumatic stress symptoms in the general population: An integrative review. Int. J. Ment. Health Nurs. 2021, 30, 834–846. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Lee, S.H.; Shin, H.-S.; Park, H.Y.; Kim, J.L.; Lee, J.J.; Lee, H.; Won, S.-D.; Han, W. Depression as a Mediator of Chronic Fatigue and Post-Traumatic Stress Symptoms in Middle East Respiratory Syndrome Survivors. Psychiatry Investig. 2019, 16, 59–64. [Google Scholar] [CrossRef]
- Bah, A.J.; James, P.B.; Bah, N.; Sesay, A.B.; Sevalie, S.; Kanu, J.S. Prevalence of anxiety, depression and post-traumatic stress disorder among Ebola survivors in northern Sierra Leone: A cross-sectional study. BMC Public Health 2020, 20, 1391. [Google Scholar] [CrossRef]
- D’Cruz, R.F.; Waller, M.D.; Perrin, F.; Periselneris, J.; Norton, S.; Smith, L.-J.; Patrick, T.; Walder, D.; Heitmann, A.; Lee, K.; et al. Chest radiography is a poor predictor of respiratory symptoms and functional impairment in survivors of severe COVID-19 pneumonia. ERJ Open Res. 2021, 7, 00655–2020. [Google Scholar] [CrossRef]
- Kumar, S.; Bansal, A.; Takia, L.; Prasad, S.; Saini, M.; Chetal, P.; Nallasamy, K.; Angurana, S.K.; Malhi, P.; Jayashree, M. Psychosocial issues among paediatric health-care workers posted in intensive care unit during COVID-19 pandemic: A questionnaire-based survey (Psy-Co-19 survey). J. Paediatr. Child Health 2023, 59, 1082–1088. [Google Scholar] [CrossRef]
- Chen, R.; Sun, C.; Chen, J.; Jen, H.; Kang, X.L.; Kao, C.; Chou, K. A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2021, 30, 102–116. [Google Scholar] [CrossRef]
- Braude, P.; McCarthy, K.; Strawbridge, R.; Short, R.; Verduri, A.; Vilches-Moraga, A.; Hewitt, J.; Carter, B. Frailty is associated with poor mental health 1 year after hospitalisation with COVID-19. J. Affect. Disord. 2022, 310, 377–383. [Google Scholar] [CrossRef]
- Nur, M.I.; Al-Mamun, F.; Yasmin, F.; Mohiuddin, M.S.; Kaggwa, M.M.; Sikder, T.; Mamun, M.A. Psychological benefits of the COVID-19 vaccination: A Bangladeshi comparative study. Health Sci. Rep. 2023, 6, e1346. [Google Scholar] [CrossRef] [PubMed]
- Moghadasi, A.N.; Mirmosayyeb, O.; Barzegar, M.; Sahraian, M.A.; Ghajarzadeh, M. The prevalence of COVID-19 infection in patients with multiple sclerosis (MS): A systematic review and meta-analysis. Neurol. Sci. 2021, 42, 3093–3099. [Google Scholar] [CrossRef] [PubMed]
- Lunkenheimer, F.; Garatva, P.; Steubl, L.; Baumeister, H. Prevalence and incidence of post-traumatic stress disorder and symptoms in people with chronic somatic diseases: A systematic review and meta-analysis. Front. Psychiatry 2023, 14, 1107144. [Google Scholar] [CrossRef] [PubMed]
- Siqveland, J.; Hussain, A.; Lindstrøm, J.C.; Ruud, T.; Hauff, E. Prevalence of Posttraumatic Stress Disorder in Persons with Chronic Pain: A Meta-analysis. Front. Psychiatry 2017, 8, 164. [Google Scholar] [CrossRef]
- Fishbain, D.A.; Pulikal, A.; Lewis, J.E.; Gao, J. Chronic Pain Types Differ in Their Reported Prevalence of Post -Traumatic Stress Disorder (PTSD) and There Is Consistent Evidence That Chronic Pain Is Associated with PTSD: An Evidence-Based Structured Systematic Review. Pain. Med. 2017, 18, 711–735. [Google Scholar] [CrossRef]
- Pepi, C.; Mercier, M.; Salimbene, L.; Galati, C.; Specchio, N.; de Palma, L. Post-Traumatic Stress-Disorder in Epilepsy: Meta-analysis of current evidence. Epilepsy Behav. 2024, 157, 109833. [Google Scholar] [CrossRef]
- Peres, D.S.; Rodrigues, P.; Viero, F.T.; Frare, J.M.; Kudsi, S.Q.; Meira, G.M.; Trevisan, G. Prevalence of depression and anxiety in the different clinical forms of multiple sclerosis and associations with disability: A systematic review and meta-analysis. Brain Behav. Immun. Health 2022, 24, 100484. [Google Scholar] [CrossRef]
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Patten, S.B.; Beck, C.A.; Williams, J.V.A.; Barbui, C.; Metz, L.M. Major depression in multiple sclerosis: A population-based perspective. Neurology 2003, 61, 1524–1527. [Google Scholar] [CrossRef] [PubMed]
- Dalos, N.P.; Rabins, P.V.; Brooks, B.R.; O’Donnell, P. Disease activity and emotional state in multiple sclerosis. Ann. Neurol. 1983, 13, 573–577. [Google Scholar] [CrossRef]
- Schubert, D.S.; Foliart, R.H. Increased depression in multiple sclerosis patients. A meta-analysis. Psychosomatics 1993, 34, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Kishore, J.; Vatsa, R.; Singh, J.; Kumari, M.; Kumar, T.; Bandgar, S. Psychological Impact on Maxillofacial Trauma Patients—An Observational Study. J. Med. Life 2020, 13, 458–462. [Google Scholar] [CrossRef]
- Dekkers, A.M.M.; Olff, M.; Näring, G.W.B. Identifying persons at risk for PTSD after trauma with TSQ in the Netherlands. Community Ment. Health J. 2010, 46, 20–25. [Google Scholar] [CrossRef]
- Kuiper, H.; van Leeuwen, C.C.M.; Kopsky, D.J.; Stolwijk-Swüste, J.M.; Post, M.W.M. Post-traumatic stress disorder symptoms and pain intensity in persons with spinal cord injury. Spinal Cord 2021, 59, 328–335. [Google Scholar] [CrossRef]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M.Á. Quality of life in adults with multiple sclerosis: A systematic review. BMJ Open 2020, 10, e041249. [Google Scholar] [CrossRef]
- Bremner, J.D.; Elzinga, B.; Schmahl, C.; Vermetten, E. Structural and functional plasticity of the human brain in posttraumatic stress disorder. Prog. Brain Res. 2008, 167, 171–186. [Google Scholar] [CrossRef]
- Longinetti, E.; Frisell, T.; Englund, S.; Reutfors, J.; Fang, F.; Piehl, F. Risk of depression in multiple sclerosis across disease-modifying therapies. Mult. Scler. 2022, 28, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Zettl, U.K.; Rommer, P.S.; Aktas, O.; Wagner, T.; Richter, J.; Oschmann, P.; Cepek, L.; Elias-Hamp, B.; Gehring, K.; Chan, A.; et al. Interferon beta-1a sc at 25 years: A mainstay in the treatment of multiple sclerosis over the period of one generation. Expert. Rev. Clin. Immunol. 2023, 19, 1343–1359. [Google Scholar] [CrossRef]
- Hanna, M.; Strober, L.B. Anxiety and depression in Multiple Sclerosis (MS): Antecedents, consequences, and differential impact on well-being and quality of life. Mult. Scler. Relat. Disord. 2020, 44, 102261. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. A pandemic of social isolation? World Psychiatry 2021, 20, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Irarrazaval, M.; Norambuena, P.; Montenegro, C.; Toro-Devia, O.; Vargas, B.; Caqueo-Urízar, A. Public Policy Responses to Address the Mental Health Consequences of the COVID-19 Pandemic: Evidence From Chile. Front. Public Health 2021, 9, 590335. [Google Scholar] [CrossRef] [PubMed]
- van der Velden, P.G.; Contino, C.; Das, M.; van Loon, P.; Bosmans, M.W.G. Anxiety and depression symptoms, and lack of emotional support among the general population before and during the COVID-19 pandemic. A prospective national study on prevalence and risk factors. J. Affect. Disord. 2020, 277, 540–548. [Google Scholar] [CrossRef]
- Copeland, W.E.; Angold, A.; Shanahan, L.; Costello, E.J. Longitudinal patterns of anxiety from childhood to adulthood: The Great Smoky Mountains Study. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 21–33. [Google Scholar] [CrossRef]
- Ormel, J.; Raven, D.; van Oort, F.; Hartman, C.A.; Reijneveld, S.A.; Veenstra, R.; Vollebergh, W.A.M.; Buitelaar, J.; Verhulst, F.C.; Oldehinkel, A.J. Mental health in Dutch adolescents: A TRAILS report on prevalence, severity, age of onset, continuity and co-morbidity of DSM disorders. Psychol. Med. 2015, 45, 345–360. [Google Scholar] [CrossRef]
- Brewin, C.R.; Fuchkan, N.; Huntley, Z.; Scragg, P. Diagnostic accuracy of the Trauma Screening Questionnaire after the 2005 London bombings. J. Trauma. Stress 2010, 23, 393–398. [Google Scholar] [CrossRef]
- Mouthaan, J.; Sijbrandij, M.; Reitsma, J.B.; Gersons, B.P.R.; Olff, M. Comparing screening instruments to predict posttraumatic stress disorder. PLoS ONE 2014, 9, e97183. [Google Scholar] [CrossRef]
- Rooney, E.A.; Hallauer, C.J.; Xie, H.; Shih, C.-H.; Rapport, D.; Elhai, J.D.; Wang, X. Longitudinal PTSD symptom trajectories: Relative contributions of state anxiety, depression, and emotion dysregulation. J. Affect. Disord. 2022, 308, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Hustache, S.; Moro, M.-R.; Roptin, J.; Souza, R.; Gansou, G.M.; Mbemba, A.; Roederer, T.; Grais, R.F.; Gaboulaud, V.; Baubet, T. Evaluation of psychological support for victims of sexual violence in a conflict setting: Results from Brazzaville, Congo. Int. J. Ment. Health Syst. 2009, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Pine, D.S.; Holmes, E.A.; Reif, A. Anxiety disorders. Lancet 2021, 397, 914–927. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A.; Cohen, J.; Stuve, O.; Trojano, M.; Sørensen, P.S.; Reingold, S.; Cutter, G.; Reider, N. A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: Overview. Mult. Scler. 2015, 21, 263–281. [Google Scholar] [CrossRef]
- Hapke, U.; Schumann, A.; Rumpf, H.-J.; John, U.; Meyer, C. Post-traumatic stress disorder: The role of trauma, pre-existing psychiatric disorders, and gender. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 299–306. [Google Scholar] [CrossRef]
- Lassemo, E.; Sandanger, I.; Nygård, J.F.; Sørgaard, K.W. The epidemiology of post-traumatic stress disorder in Norway: Trauma characteristics and pre-existing psychiatric disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 11–19. [Google Scholar] [CrossRef]
- Fernandez, C.A.; Vicente, B.; Marshall, B.D.L.; Koenen, K.C.; Arheart, K.L.; Kohn, R.; Saldivia, S.; Buka, S.L. Longitudinal course of disaster-related PTSD among a prospective sample of adult Chilean natural disaster survivors. Int. J. Epidemiol. 2017, 46, 440–452. [Google Scholar] [CrossRef]
- Quarantini, L.C.; Netto, L.R.; Andrade-Nascimento, M.; Almeida, A.G.-D.; Sampaio, A.S.; Miranda-Scippa, A.; Bressan, R.A.; Koenen, K.C. Comorbid mood and anxiety disorders in victims of violence with posttraumatic stress disorder. Braz. J. Psychiatry 2009, 31 (Suppl. S2), S66–S76. [Google Scholar] [CrossRef]
- Giummarra, M.J.; Lennox, A.; Dali, G.; Costa, B.; Gabbe, B.J. Early psychological interventions for posttraumatic stress, depression and anxiety after traumatic injury: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 62, 11–36. [Google Scholar] [CrossRef]
- Kelber, M.S.; Smolenski, D.J.; Boyd, C.; Shank, L.M.; Bellanti, D.M.; Milligan, T.; Edwards-Stewart, A.; Libretto, S.; Parisi, K.; Morgan, M.A.; et al. Evidence-based telehealth interventions for posttraumatic stress disorder, depression, and anxiety: A systematic review and meta-analysis. J. Telemed. Telecare 2024, 22, 1357633X231224491. [Google Scholar] [CrossRef]
- Young, K.S.; Purves, K.L.; Hübel, C.; Davies, M.R.; Thompson, K.N.; Bristow, S.; Krebs, G.; Danese, A.; Hirsch, C.; Parsons, C.E.; et al. Depression, anxiety and PTSD symptoms before and during the COVID-19 pandemic in the UK. Psychol. Med. 2023, 53, 5428–5441. [Google Scholar] [CrossRef]
- Fernandes, A.; Ferreira, S.; Moreira, P.; Machado-Sousa, M.; Couto, B.; Raposo-Lima, C.; Costa, P.; Morgado, P.; Picó-Pérez, M. Stress, anxiety, and depression trajectories during the “first wave” of the COVID-19 pandemic: What drives resilient, adaptive and maladaptive responses in the Portuguese population? Front. Public Health 2024, 12, 1333997. [Google Scholar] [CrossRef] [PubMed]
- Amor, S.; Baker, D.; Khoury, S.J.; Schmierer, K.; Giovanonni, G. SARS-CoV-2 and Multiple Sclerosis: Not All Immune Depleting DMTs are Equal or Bad. Ann. Neurol. 2020, 87, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, N.; Ashtari, F.; Bastami, E.A.; Ghaderi, K.; Hosseini, S.M.; Naeini, M.K.; Rajabi, F.; Adibi, I. Fear and anxiety in patients with multiple sclerosis during COVID-19 pandemic; report of an Iranian population. Mult. Scler. Relat. Disord. 2021, 50, 102798. [Google Scholar] [CrossRef] [PubMed]
- Engel, C.; Greim, B.; Zettl, U.K. Diagnostics of cognitive dysfunctions in multiple sclerosis. J. Neurol. 2007, 254 (Suppl. S2), II30–II34. [Google Scholar] [CrossRef]
- Fischer, M.; Köhler, W.; Faiss, J.H.; Hoffmann, F.; Kunkel, A.; Sailer, M.; Schwab, M.; Zettl, U.K.; Bublak, P. A smart peek: Processing of rapid visual displays is disturbed in newly diagnosed, cognitively intact MS patients and refers to cognitive performance and disease progression in late stages. J. Neurol. Sci. 2019, 401, 118–124. [Google Scholar] [CrossRef]
- Greim, B.; Benecke, R.; Zettl, U.K. Qualitative and quantitative assessment of fatigue in multiple sclerosis (MS). J. Neurol. 2007, 254 (Suppl. 2), II58–II64. [Google Scholar] [CrossRef]
- Patejdl, R.; Penner, I.K.; Noack, T.K.; Zettl, U.K. Multiple sclerosis and fatigue: A review on the contribution of inflammation and immune-mediated neurodegeneration. Autoimmun. Rev. 2016, 15, 210–220. [Google Scholar] [CrossRef]
- Patejdl, R.; Zettl, U.K. The pathophysiology of motor fatigue and fatigability in multiple sclerosis. Front. Neurol. 2022, 13, 891415. [Google Scholar] [CrossRef]
- Nin, V.M.E.L.; Willmund, G.D.; Jungmann, S.M.; Asmundson, G.J.G.; Piefke, M. Mental health during the COVID-19 pandemic: Stress and strain profiles in the German population. Front. Public Health 2023, 11, 990407. [Google Scholar] [CrossRef]
- Schneider, T.R.; Rench, T.A.; Lyons, J.B.; Riffle, R.R. The influence of neuroticism, extraversion and openness on stress responses. Stress. Health 2012, 28, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Zhang, B.; Cao, M.; Roberts, B.W. The Stressful Personality: A Meta-Analytical Review of the Relation Between Personality and Stress. Pers. Soc. Psychol. Rev. 2023, 27, 128–194. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Guo, Z.; Zhu, X.; Liu, X.; Guo, Y. The interplay of personality traits, anxiety, and depression in Chinese college students: A network analysis. Front. Public Health 2023, 11, 1204285. [Google Scholar] [CrossRef]
- Reijnen, A.; Geuze, E.; Gorter, R.; Vermetten, E. Development of Self-Directedness and Cooperativeness in Relation to Post-Traumatic Stress Disorder Symptom Trajectories After Military Deployment. Chronic Stress 2018, 2, 2470547018803511. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- Leekoff, M.; Culpepper, W.; Jin, S.; Lee-Wilk, T.; Wallin, M. Impact of comorbid post traumatic stress disorder on multiple sclerosis in military veterans: A population-based cohort study. Mult. Scler. 2022, 28, 1257–1266. [Google Scholar] [CrossRef]
- Al-Ameri, M.; Mansour, M.; Al-Habahbeh, S.; Weshah, F.; Ennab, W.; Gammoh, O. Symptoms of PTSD and depression in newly diagnosed people with multiple sclerosis during the outbreak Oct.7th war on Gaza: A case-control study from Jordan. Mult. Scler. Relat. Disord. 2025, 93, 106206. [Google Scholar] [CrossRef]
- Ogle, C.M.; Siegler, I.C.; Beckham, J.C.; Rubin, D.C. Neuroticism Increases PTSD Symptom Severity by Amplifying the Emotionality, Rehearsal, and Centrality of Trauma Memories. J. Pers. 2017, 85, 702–715. [Google Scholar] [CrossRef]
- Brown, N.; Wojtalik, J.A.; Turkel, M.; Vuper, T.; Strasshofer, D.; Sheline, Y.I.; Bruce, S.E. Neuroticism and Its Associated Brain Activation in Women with PTSD. J. Interpers. Violence 2020, 35, 341–363. [Google Scholar] [CrossRef]
- Benedict, R.H.; Schwartz, C.E.S.; Duberstein, P.; Healy, B.; Hoogs, M.M.; Bergsland, N.; Dwyer, M.G.; Weinstock-Guttman, B.; Zivadinov, R. Influence of personality on the relationship between gray matter volume and neuropsychiatric symptoms in multiple sclerosis. Psychosom. Med. 2013, 75, 253–261. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Wojcik, C.; Wilding, G.E.; Pol, J.; Dwyer, M.G.; Weinstock-Guttman, B.; Zivadinov, R.; Benedict, R.H. Trait Conscientiousness predicts rate of longitudinal SDMT decline in multiple sclerosis. Mult. Scler. 2020, 26, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Incerti, C.C.; Magistrale, G.; Argento, O.; Pisani, V.; Di Battista, G.; Ferraro, E.; Caltagirone, C.; Benedict, R.H.; Nocentini, U. Occupational stress and personality traits in multiple sclerosis: A preliminary study. Mult. Scler. Relat. Disord. 2015, 4, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Benjet, C.; Bromet, E.J.; Cardoso, G.; Degenhardt, L.; de Girolamo, G.; Dinolova, R.V.; Ferry, F.; et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur. J. Psychotraumatol. 2017, 8 (Suppl. S5), 1353383. [Google Scholar] [CrossRef] [PubMed]
- Breslau, N.; Chilcoat, H.D.; Kessler, R.C.; Davis, G.C. Previous exposure to trauma and PTSD effects of subsequent trauma: Results from the Detroit Area Survey of Trauma. Am. J. Psychiatry 1999, 156, 902–907. [Google Scholar] [CrossRef]
- da Silva, H.C.; Vilete, L.; Coutinho, E.S.F.; Luz, M.P.; Mendlowicz, M.; Portela, C.M.; Figueira, I.; Ventura, P.; Mari, J.d.J.; Quintana, M.I.; et al. The role of childhood cumulative trauma in the risk of lifetime PTSD: An epidemiological study. Psychiatry Res. 2024, 336, 115887. [Google Scholar] [CrossRef]
- Gould, F.; Harvey, P.D.; Hodgins, G.; Jones, M.T.; Michopoulos, V.; Maples-Keller, J.; Rothbaum, B.O.; Rothbaum, A.O.; Ressler, K.J.; Nemeroff, C.B. Prior trauma-related experiences predict the development of posttraumatic stress disorder after a new traumatic event. Depress. Anxiety 2021, 38, 40–47. [Google Scholar] [CrossRef]
- Gluck, R.L.; Hartzell, G.E.; Dixon, H.D.; Michopoulos, V.; Powers, A.; Stevens, J.S.; Fani, N.; Carter, S.; Schwartz, A.C.; Jovanovic, T.; et al. Trauma exposure and stress-related disorders in a large, urban, predominantly African-American, female sample. Arch. Womens Ment. Health 2021, 24, 893–901. [Google Scholar] [CrossRef]
- Holmes, S.C.; Callinan, L.; Facemire, V.C.; Williams, M.T.; Ciarleglio, M.M.; Smith, M.V. Material hardship is associated with posttraumatic stress disorder symptoms among low-income Black women. J. Trauma. Stress. 2021, 34, 905–916. [Google Scholar] [CrossRef]
- Lu, W.; Dimick, M.K.; Fiksenbaum, L.M.; Timmins, V.; Mitchell, R.H.; Zou, Y.; Goldstein, B.I. Clinical correlates of socioeconomic status in adolescent bipolar disorder. Compr. Psychiatry 2020, 101, 152186. [Google Scholar] [CrossRef]
- Karampampa, K.; Gustavsson, A.; Miltenburger, C.; Eckert, B. Treatment experience, burden and unmet needs (TRIBUNE) in MS study: Results from five European countries. Mult. Scler. 2012, 18 (Suppl. S2), 7–15. [Google Scholar] [CrossRef]
- Karampampa, K.; Gustavsson, A.; Miltenburger, C.; Kindundu, C.M.; Selchen, D.H. Treatment experience, burden, and unmet needs (TRIBUNE) in multiple sclerosis: The costs and utilities of MS patients in Canada. J. Popul. Ther. Clin. Pharmacol. 2012, 19, e11–e25. [Google Scholar]
- Aljaberi, M.A.; Lee, K.-H.; Alareqe, N.A.; Qasem, M.A.; Alsalahi, A.; Abdallah, A.M.; Noman, S.; Al-Tammemi, A.B.; Ibrahim, M.I.M.; Lin, C.-Y. Rasch Modeling and Multilevel Confirmatory Factor Analysis for the Usability of the Impact of Event Scale-Revised (IES-R) during the COVID-19 Pandemic. Healthcare 2022, 10, 1858. [Google Scholar] [CrossRef] [PubMed]
- Rash, C.J.; Coffey, S.F.; Baschnagel, J.S.; Drobes, D.J.; Saladin, M.E. Psychometric properties of the IES-R in traumatized substance dependent individuals with and without PTSD. Addict. Behav. 2008, 33, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Sveen, J.; Bondjers, K.; Willebrand, M. Psychometric properties of the PTSD Checklist for DSM-5: A pilot study. Eur. J. Psychotraumatol. 2016, 7, 30165. [Google Scholar] [CrossRef] [PubMed]
- Monschein, T.; Hartung, H.-P.; Zrzavy, T.; Barnett, M.; Boxberger, N.; Berger, T.; Chataway, J.; Bar-Or, A.; Rommer, P.S.; Zettl, U.K. Vaccination and multiple sclerosis in the era of the COVID-19 pandemic. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1033–1043. [Google Scholar] [CrossRef]
- Winkelmann, A.; Loebermann, M.; Barnett, M.; Hartung, H.-P.; Zettl, U.K. Vaccination and immunotherapies in neuroimmunological diseases. Nat. Rev. Neurol. 2022, 18, 289–306. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 149) | Probable PTSD (n = 12) | No Probable PTSD (n = 137) | p |
|---|---|---|---|---|
| Sex, n (%) | 0.540 Fi | |||
| Men | 53 (35.6) | 3 (25.0) | 50 (36.5) | |
| Women | 96 (64.4) | 9 (75.0) | 87 (63.5) | |
| Age (years), median (range) | 51 (20–74) | 48 (29–57) | 51 (20–74) | 0.184 U |
| School years, median (range) | 10 (8–14) | 10 (10–14) | 10 (8–13) | 0.875 U |
| Employment, n (%) | 74 (49.7) | 5 (41.7) | 69 (50.4) | 0.765 Fi |
| EDSS score, median (range) | 3.5 (0.0–8.5) | 3.75 (1.0–6.5) | 3.5 (0.0–8.5) | 0.578 U |
| Disease duration (years), median (range) | 10 (0–37) | 10 (1–31) | 10 (0–37) | 0.756 U |
| Disease course, n (%) | 0.344 Fi | |||
| Relapsing MS | 103 (69.1) | 10 (83.3) | 93 (67.9) | |
| Progressive MS | 46 (30.9) | 2 (16.7) | 44 (32.1) | |
| Number of comorbidities, n (%) | 0.340 Chi | |||
| 0 | 39 (26.2) | 2 (16.7) | 37 (27.0) | |
| 1 | 28 (18.8) | 1 (8.3) | 27 (19.7) | |
| ≥2 | 82 (55.0) | 9 (75.0) | 73 (53.3) | |
| Psychiatric comorbidities, n (%) | 25 (16.8) | 8 (66.7) | 17 (12.4) | <0.001Fi |
| Anxiety disorder *1 | 5 (3.4) | 2 (16.7) | 3 (2.2) | 0.052 Fi |
| Depression *1 | 23 (15.4) | 7 (58.3) | 16 (11.7) | <0.001Fi |
| Drugs in total, median (range) | 5 (0–16) | 8 (2–12) | 5 (0–16) | 0.113 U |
| Polypharmacy (use of ≥5 drugs), n (%) | 77 (51.7) | 8 (66.7) | 69 (50.4) | 0.371 Fi |
| Use of DMT, n (%) | 117 (78.5) | 8 (66.7) | 109 (79.6) | 0.288 Fi |
| Alemtuzumab | 1 (0.7) | 0 (0.0) | 1 (0.7) | 1.000 Fi |
| Azathioprine | 1 (0.7) | 0 (0.0) | 1 (0.7) | 1.000 Fi |
| Cladribine | 2 (1.3) | 0 (0.0) | 2 (1.5) | 1.000 Fi |
| Dimethyl fumarate | 10 (6.7) | 2 (16.7) | 8 (5.8) | 0.132 Fi |
| Fingolimod | 13 (8.7) | 1 (8.3) | 12 (8.8) | 1.000 Fi |
| Glatiramer actetate | 13 (8.7) | 1 (8.3) | 12 (8.8) | 1.000 Fi |
| Glucocorticosteroid pulse therapy | 16 (10.7) | 0 (0.0) | 16 (11.7) | 0.364 Fi |
| Interferon beta | 19 (12.8) | 1 (8.3) | 18 (13.1) | 1.000 Fi |
| Intravenous immunoglobulin | 1 (0.7) | 0 (0.0) | 1 (0.7) | 1.000 Fi |
| Mitoxantrone | 3 (2.0) | 0 (0.0) | 3 (2.2) | 1.000 Fi |
| Natalizumab | 15 (10.1) | 1 (8.3) | 14 (10.2) | 1.000 Fi |
| Ocrelizumab | 11 (7.4) | 1 (8.3) | 10 (7.3) | 1.000 Fi |
| Teriflunomide | 12 (8.1) | 1 (8.3) | 11 (8.0) | 1.000 Fi |
| Ever smoked, n (%) *2 | 57 (51.4) | 6 (100.0) | 51 (48.6) | 0.027 Fi |
| Willingness regarding recommended standard vaccinations, n (%) | 112 (75.2) | 7 (58.3) | 105 (76.6) | 0.173 Fi |
| MS relapses within the last 3 months prior to the surveys | 19 (12.8) | 3 (25.0) | 16 (11.7) | 0.183 Fi |
| MS progression within the last 3 months prior to the surveys *3 | 48 (32.7) | 7 (58.3) | 41 (30.4) | 0.059 Fi |
| Burden | Total (n = 149) | Probable PTSD (n = 12) | No Probable PTSD (n = 137) | p Fi |
|---|---|---|---|---|
| ~3 months after the COVID-19 outbreak was declared a global pandemic | ||||
| Severe or very severe mental burden | 44 (29.5) | 10 (83.3) | 34 (24.8) | <0.001 |
| Severe or very severe physical burden | 42 (28.2) | 8 (66.7) | 34 (24.8) | 0.004 |
| Severe or very severe social burden | 45 (30.2) | 7 (58.3) | 38 (27.7) | 0.045 |
| ~1 year after the authorization of first SARS-CoV-2 vaccines | ||||
| Severe or very severe mental burden | 38 (25.5) | 10 (83.3) | 28 (20.4) | <0.001 |
| Severe or very severe physical burden | 44 (29.5) | 8 (66.7) | 36 (26.3) | 0.006 |
| Severe or very severe social burden | 35 (23.5) | 8 (66.7) | 27 (19.7) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heidler, F.; Hecker, M.; Frahm, N.; Baldt, J.; Streckenbach, B.; Meißner, J.; Burian, K.; Langhorst, S.E.; Mashhadiakbar, P.; Richter, J.; et al. Trauma Burden Affected People with Multiple Sclerosis During SARS-CoV-2 Pandemic. J. Clin. Med. 2025, 14, 2665. https://doi.org/10.3390/jcm14082665
Heidler F, Hecker M, Frahm N, Baldt J, Streckenbach B, Meißner J, Burian K, Langhorst SE, Mashhadiakbar P, Richter J, et al. Trauma Burden Affected People with Multiple Sclerosis During SARS-CoV-2 Pandemic. Journal of Clinical Medicine. 2025; 14(8):2665. https://doi.org/10.3390/jcm14082665
Chicago/Turabian StyleHeidler, Felicita, Michael Hecker, Niklas Frahm, Julia Baldt, Barbara Streckenbach, Janina Meißner, Katja Burian, Silvan Elias Langhorst, Pegah Mashhadiakbar, Jörg Richter, and et al. 2025. "Trauma Burden Affected People with Multiple Sclerosis During SARS-CoV-2 Pandemic" Journal of Clinical Medicine 14, no. 8: 2665. https://doi.org/10.3390/jcm14082665
APA StyleHeidler, F., Hecker, M., Frahm, N., Baldt, J., Streckenbach, B., Meißner, J., Burian, K., Langhorst, S. E., Mashhadiakbar, P., Richter, J., & Zettl, U. K. (2025). Trauma Burden Affected People with Multiple Sclerosis During SARS-CoV-2 Pandemic. Journal of Clinical Medicine, 14(8), 2665. https://doi.org/10.3390/jcm14082665