Abstract
Background/Objectives: Mitral regurgitation (MR) is the most common left heart valve disease, but its exact prevalence remains uncertain. To estimate the prevalence of MR we conducted a systematic review and meta-analysis of population-based studies. Methods: We searched the Medline/PubMed, Embase, and Scopus databases, in January 2023, for studies reporting or allowing for the calculation of the prevalence of moderate-to-severe MR in the general population. Eligible studies included those using echocardiography or primary care databases from countries with universal healthcare. Studies where echocardiography was performed for medical indications were excluded. Random-effects meta-analysis was used to calculate the pooled estimates. Subgroup and meta-regression analyses were employed to investigate the reasons for heterogeneity. Mixed-model multivariable meta-regression was used to estimate age- and sex-specific prevalence. Results: After screening 13,847 records, we identified 20 eligible studies (22 study populations) including 6,036,691 individuals. The global prevalence of moderate-to-severe MR was 0.67% (95% CI, 0.33−1.11). Prevalence increased greatly with age, and it was estimated to be approximately 0.63% (0.25–1.16) at age 50, 2.85% (1.96–3.90) at 70, and 6.45% (4.17–9.16) by 90 years. North America showed the largest crude prevalence (1.11%; 0.52−1.88), followed by Europe (0.60%; 0.34−0.92), Asia (0.24%; 0.00−0.92), and Africa (0.16%; 0.03−0.37). Differences in prevalence by geographic region and ethnic group were primarily attributable to population age. Prevalence did not differ by sex, study year, or diagnostic criteria. Conclusions: Moderate-to-severe MR is a prevalent condition, particularly among elderly people. With rising life expectancy worldwide, ensuring universal access to interventions will be vital to reduce morbidity and mortality.
1. Introduction
Mitral regurgitation (MR), the backward blood flow from the left ventricle into the left atrium during systole, is the most common left heart valve disease worldwide [1,2]. While mild MR is often seen in healthy individuals, moderate-to-severe MR affects an estimated 2.5 million people in the United States [3]. Clinically significant MR is associated with a high risk of heart failure following diagnosis and markedly increased morbidity and mortality [1].
The main therapeutic options for MR, when it reaches a degree of severity, are surgical, either through mitral valve replacement or repair [4]. Advances in surgical techniques, risk stratification, and patient outcome tracking have greatly improved prognosis when timely diagnosis occurs, allowing many patients to reach life expectancies similar to those without the condition [5]. However, MR remains underdiagnosed and undertreated, resulting in poor survival outcomes for many patients [6]. As population aging continues, MR prevalence is expected to rise, underscoring its importance as a major public health concern [3]. This challenge is compounded by the lack of comprehensive, population-based data on the global burden of MR. Most available epidemiologic studies focus primarily on Western countries and often rely on older data [3,7,8,9]. To effectively allocate resources and guide healthcare investments in specialized diagnostic and treatment services for patients with MR, clinicians and policy makers require updated evidence regarding the burden of moderate-to-severe MR in the general population. Such data are essential for informed decision-making about health system spending and prioritizing interventions, including strategies to improve general awareness around the condition.
We conducted a systematic review and meta-analysis of population-based studies to assess the global prevalence of moderate-to-severe MR in the general adult population with the aim of quantifying the global burden of this condition by age, sex, and across geographic areas.
2. Methods
This work is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [10]. The protocol was registered with PROSPERO (CRD42023448216).
2.1. Search Strategy
We systematically searched for population-based studies reporting the prevalence of MR in the Medline/PubMed, Embase, and Scopus databases from inception to 17 January 2023. Key search terms included “mitral regurgitation” OR “mitral disease” OR “mitral insufficiency” OR (“mitral valve” AND “regurgitation”) combined with “prevalence” OR “incidence” OR “epidemiology” OR “surveillance” OR “survey”. We used the appropriate MeSH terms, truncated terms, variants, and acronyms. The search algorithms are reported in Appendix S1. We excluded editorials, congress abstracts, and studies not conducted in humans. We screened the reference lists of relevant systematic or narrative reviews to identify additional articles. We also consulted with field experts to gather additional evidence. No language restrictions were imposed.
2.2. Selection Criteria
We considered as eligible cross-sectional or longitudinal studies collecting data with a well-specified sampling frame, including population samples of adults at the national, subnational, or community level of reporting, or allowing for the calculation of the prevalence of moderate-to-severe MR. Studies using Doppler echocardiography for diagnosis were considered the most appropriate to answer our research question. Given the broad temporal span of the included studies, we considered studies with slight variations in diagnostic criteria for the identification of our target condition (Supplementary Table S1). A brief discussion of the temporal evolution of the definition and assessment methods of moderate-to-severe MR is given in Appendix S2 [11,12,13,14,15,16].
Also, we considered eligible studies using primary care databases conducted in countries with universal healthcare coverage or countries where at least 80% of the population was publicly insured. To be considered eligible, such studies should have used the International Classification of Diseases (ICD) or other well-defined classification systems, allowing the accurate identification of MR.
We excluded studies that did not include a representative sample of the general adult population, particularly those with an increased or reduced likelihood of presenting with MR. More in detail, echocardiographic studies were excluded if participants were selected based on symptoms, suspected valvular diseases, or any medical indication suggesting the need for diagnostic evaluation. Studies conducted explicitly on elderly people were still retained if diagnostic procedures or study inclusion were not prompted by symptoms or established medical conditions. These studies were excluded from the primary analysis to avoid introducing heterogeneity that could inflate uncertainty in our global estimate, as they represented a distinct subgroup with higher expected prevalence. Nevertheless, these were retained for meta-regression analysis to inform age- and sex-specific prevalence estimates. Studies focusing on individuals <18 years old were considered ineligible.
Four authors (G.F., A.S., M.N.C., and A.H.) independently screened the titles and abstracts, excluding irrelevant studies. Articles identified as potentially eligible were read in full and critically appraised for inclusion. Disagreements were resolved by consensus with the assistance of the senior authors (S.B. and D.P.).
2.3. Data Extraction
Two authors (G.F. and A.S.) independently extracted data using a predefined extraction form. The following data were extracted from each study: first author name, publication title and year, study period, study design, country, predominant ethnicity, method/criteria used for identifying MR, mean age and age range, proportion of males, number of participants, and number of cases with MR. Any stratified data by age, sex, or ethnic group was also extracted from the articles’ main texts and supplementary materials. If the mean study age was not specified, we derived it from the age-stratified data. If ethnicity was not specified, we assessed whether the study population likely reflected the country’s demographics and assumed that participants belonged predominantly to the most represented country’s ethnic group.
2.4. Quality Assessment
A quality assessment of the included studies was performed independently in duplicate, using a modified version of the Joanna Briggs Institute Prevalence Critical Appraisal Tool [17].
2.5. Statistical Analysis
Confidence intervals (CI) for prevalence in each individual study were calculated using the exact binomial method (Clopper–Pearson). The double arcsine transformation was applied prior to data synthesis to prevent variance instability [18]. This transformation does not require continuity correction in the case of studies with zero cases. To allow interpretability, the pooled prevalence was back-transformed on the normal scale using the inverse Freeman–Tukey transformation [19].
The pooled prevalence was estimated by random-effects meta-analysis. The random-effects model was chosen over the fixed-effects model as it accounts for both chance variations and true differences in prevalence across studies. Studies were weighted using the inverse variance method. The restricted maximum-likelihood method was used for estimating τ-squared. Statistical heterogeneity across studies was assessed with the Cochran’s Q-test [20], with a conservative 0.10 level of significance. Heterogeneity was further assessed using the I-squared statistic. This was interpreted as follows: 0–40%, not important; 30–60%, moderate; 50–90%, substantial; and 75–100%, considerable heterogeneity [21]. The small-study effect was assessed visually with a funnel plot and using the Egger regression asymmetry test.
Subgroup and meta-regression analyses were conducted to explore potential sources of heterogeneity. Subgroup meta-analyses were performed by geographic area (i.e., continent), ethnicity of participants, method/criteria used for identifying MR, and study size. The subgroup analysis by identification criteria was used to establish the appropriateness of pooling echocardiographic studies with large registry-based databases with a differential diagnostic standard. We assessed whether subgroups were associated with significantly different estimates using a test of interaction [22].
Univariable and multivariable mixed-effects meta-regression analyses were performed for the relevant continuous moderators as follows: mean age, proportion of males, and study year (midpoint of the study period). Bubble plots illustrated the independent associations between each moderator and the prevalence of moderate-to-severe MR, with study-specific effect sizes on the y-axis and moderator values on the x-axis. Marker sizes reflected study precision, and each graph included the (marginal) multivariable meta-regression lines with 95% CIs. To allow interpretability, graphs were plotted on the normal scale after applying the inverse Freeman–Tukey double arcsine transformation, using the harmonic mean of sample sizes [19].
We also obtained the (marginal) estimates for the moderate-to-severe prevalence of MR at crescent values of age from the multivariable meta-regression model considering the proportion of males and the study publication year kept at the weighted means. Similarly, we derived sex- and sex-and-age-specific estimates. Analyses and data visualization were performed using the R statistical software version 4.4.2, packages meta and metafor (R Core Team, https://www.r-project.org/). For all tests, except for heterogeneity, we considered a 2-tailed p < 0.05 as statistically significant.
3. Results
The systematic search identified 13,847 unique records. After screening the abstracts and reviewing the full texts, 20 studies covering 22 study populations were deemed eligible for inclusion (Figure 1) [3,8,9,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. The primary reason for exclusion was the absence or unclear definition of moderate-to-severe MR prevalence data (N = 230), followed by the lack of representation of the general population, such as echocardiography studies where the diagnostic assessment was clearly medically indicated (N = 30).
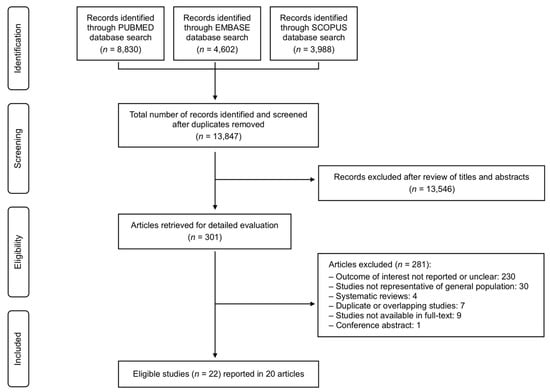
Figure 1.
Summary of the evidence search and selection process (flowchart).
The included studies comprised a combined sample of 6,036,691 individuals (median 2369; IQR 455–4728). Study characteristics are presented in Table 1, with a more detailed description of the method/criteria used for identifying MR provided in Supplementary Table S1. Quality assessment for each study is reported in Supplementary Table S2. Publication years ranged from 1989 to 2021, while study years ranged from 1988 to 2017. On average, there was a 6.7-year (95% CI, 4.7–8.6) delay between the period covered by each study and its publication. Most studies contributed data from North America (eight studies, nine study populations) [3,23−27,34,35] and Europe (eight studies) [8,9,28−32,37], followed by Asia (four studies) [30,33,36,39] and Africa (one study) [38]. The United States (eight studies, nine study populations) [3,23−27,34,35] and the United Kingdom (UK, four studies) [8,9,32,37] were the most frequently represented countries. Eighteen studies determined the diagnosis of MR using Doppler echocardiography [3,8,23−36,38,39], while two comprehensive record-linkage studies conducted in the UK identified cases through the relevant diagnostic codes [9,37]. The weighted mean age across all study populations was 44.9 years, with mean age per study ranging from 20 to 90 years old. Among the 5,916,298 individuals from six study populations that reported sex-specific data, 2,662,092 (45.0%) were females. All studies either reported or allowed for the derivation of the proportion of males.

Table 1.
Study characteristics for the study populations included (N = 22).
Data Synthesis
Five studies focused explicitly on elderly people and showed the mean age of participants above 70 years [8,29,31,32,39]; therefore, our analysis for the general adult population was conducted on 15 studies including 17 study populations (N = 6,029,659) [3,9,23−28,30,33−38].
The pooled global prevalence of moderate-to-severe MR was 0.67% (95% CI, 0.33−1.11; Figure 2). We noted considerable heterogeneity in this analysis (τ2 = 0.002; I2 = 98.6%; p < 0.001). No evidence of small-study effect highlighted by funnel plot asymmetry was observed (Supplementary Figure S1; PEgger = 0.14). We investigated reasons for heterogeneity in subgroup and meta-regression analyses (Table 2 and Table 3).
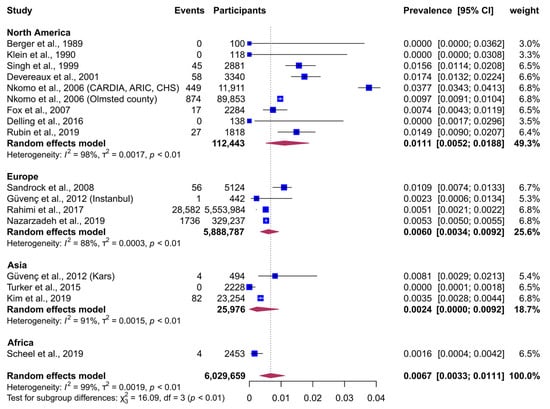
Figure 2.
Random-effects meta-analysis of the prevalence of moderate-to-severe mitral regurgitation, grouped by geographic continent [3,9,23,24,25,26,27,28,30,33,34,35,36,37,38]. Abbreviation: CI, Confidence Interval.
Table 2.
Subgroup meta-analysis of the prevalence of moderate-to-severe mitral regurgitation in adults by the pertinent categorical moderators (N = 17). 1.
Table 3.
Univariable and multivariable mixed-effects meta-regression analysis investigating the association of mean age, proportion of males, and study year, with prevalence of moderate-to-severe mitral regurgitation.
Subgroup analyses suggested a significant geographic disparity in the prevalence of moderate-to-severe MR (Figure 2, Table 2, p = 0.001). North America showed the largest prevalence (1.11%, 95% CI, 0.52−1.88), followed by Europe (0.60%; 0.34−0.92), Asia (0.24%; 0.00−0.92), and Africa (0.16%; 0.03−0.37). Similarly, prevalence differed significantly by ethnic group (Table 2, Supplementary Figure S2, p < 0.001), with the only study conducted on American Indian individuals showing the largest estimates [26], followed by the Hispanic [35], White [3,8,9,23−25,28−34,37], Black [27,38], and Asian ethnic groups [36,39]. When grouped by method/criteria used for identifying MR, there was no significant difference in prevalence (p = 0.18) between studies using Doppler echocardiography (0.69%, 95% CI, 0.31–1.21) [3,8,23−36,38,39] and record-linkage studies using ICD-10 codes and having confirmed most cases by echocardiography (0.52%, 95% CI, 0.51–0.52) [9,37]. Additionally, no significant difference was observed by study size.
Meta-regression analyses comprised all studies, including those performed on elderly populations, and considered age- and sex-stratified estimates whenever available. Age was the only significant moderator of heterogeneity across studies (Table 3; p < 0.001). Although age alone explained a large proportion of the variability in prevalence across studies (R-squared = 47.2%), there was still a significant amount of residual heterogeneity (τ2 = 0.005, SE = 0.001; χ2 = 4976; p < 0.001). The analyses did not show any significant temporal trend or statistically significant difference by sex in the prevalence of moderate-to-severe MR (Table 3).
Based on the results of multivariable meta-regression analysis, the estimated global prevalence of moderate-to-severe MR was approximately 0.08% (95% CI, 0.00–0.50) at 40 years of age, increasing to 0.63% (95% CI, 0.25–1.16) at age 50, 1.56% (95% CI, 1.01–2.22) at 60, 2.85% (95% CI, 1.96–3.90) at 70, 4.48% (95% CI, 3.00–6.23) at 80, and reaching 6.45% (95% CI, 4.17–9.16) by 90 years. The estimated global prevalence by sex was 0.55% (95% CI, 0.05–1.41) in females and 0.63% (95% CI, 0.06–1.61) in males. Although sex did not significantly alter the estimates, we present age-specific, sex-specific, and age-and-sex-specific prevalence estimates in Table 4 for illustrative purposes.
Table 4.
Age- and sex-specific estimates of the global prevalence of moderate-to-severe mitral regurgitation. 1
Figure 3 presents bubble plots showing the adjusted association of age, proportion of males, and study year with the prevalence of moderate-to-severe MR. The meta-regression lines in these graphs depict the “marginal” relationship between each continuous predictor and prevalence, holding all other moderators constant at their weighted mean values. Bubble plots of the univariable meta-regression results for each continuous moderator are shown in Supplementary Figures S3−S5.
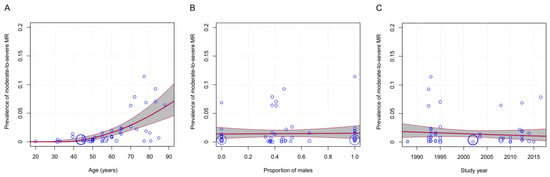
Figure 3.
Bubble plots from multivariable meta-regression analysis, illustrating the independent associations of the mean age (A), proportion of males (B), and study year (C), with the prevalence of moderate-to-severe mitral regurgitation. The study-specific effect size is displayed on the y-axis and the moderator of interest on the x-axis. The size of the markers is proportional to the size of each study. The graphs are accompanied by the (marginal) multivariable meta-regression lines in red and the respective 95% confidence intervals in gray. The bubble representing the study by van Bemmel et al. (2010) [29] is omitted to enhance visual clarity, though its data were fully incorporated into the analysis.
Sensitivity meta-regression analyses, incorporating either the study continent or participant ethnicity into the multivariable model, showed no significant deviation from the main model’s findings (see Supplementary Tables S3 and S4).
4. Discussion
This systematic review and meta-analysis of population-based studies estimated the global prevalence of moderate-to-severe MR in the general adult population. Age was identified as the primary factor influencing MR prevalence across societies. While crude prevalence varied by geographic region and ethnicity, these differences were largely attributable to age distribution. This is the first meta-analysis to present global, population-based, age- and sex-specific estimates of clinically significant MR.
Our findings should be compared with those of Yadgir et al., who used Bayesian modeling in the Global Burden of Disease Study 2017 [40]. They estimated the prevalence of degenerative mitral valve diseases at approximately 0.2%, slightly lower but within the lower bound of our confidence interval. Unlike our analysis, which primarily relied on echocardiographic studies conducted in non-medically indicated general populations, Yadgir et al. utilized diverse direct and indirect data sources, with echocardiographic studies forming a minority [40]. In regions with limited healthcare access, such as non-Western settings, reliance on administrative data, clinical records, and other indirect data sources may underreport subclinical cases. Conversely, population-based echocardiographic studies are better at capturing the true burden of disease, identifying cases that might otherwise go undiagnosed, even in developing countries. Detection bias, particularly due to disparities in healthcare access, might explain the modest difference between our findings and those of Yadgir et al. [40].
We observed geographic differences, with higher prevalence estimates in North America and Europe compared to Asia and Africa, along with significant variations by ethnicity. However, these disparities were no longer significant after accounting for age. This contrasts with Yadgir et al. [40], where estimates differed across regions with varying levels of development, even after age standardization. We believe that both sets of results are valuable but require different interpretations. Yadgir’s results, influenced by diverse data sources and healthcare access disparities, likely reflect the “visible” burden of disease. In contrast, our estimates aim to approximate the “true” burden, including undiagnosed cases in resource-limited settings, despite the inherent uncertainties.
We found no significant sex differences in MR prevalence, consistent with the complex interplay of sex-specific risk factors for primary and secondary MR [41]. Primary MR tends to affect females more [42], while secondary MR is likely more common in males due to increased smoking and alcohol use [43,44]. Conversely, obesity—a key factor for secondary MR—is more prevalent among females [45], and hypertension rates are similar between sexes [46]. Although there are other biological factors specific to each sex [41], the balance across modifiable risk factors likely accounts for a similar global MR prevalence observed between males and females. This aligns with the findings of Yousuf et al., who attributed the higher crude MR prevalence in females to their longer life expectancy [40]. However, regional disparities in risk factor distribution and genetic predisposition to MR [47] may still contribute to sex-based differences in certain populations.
This study has several strengths. We pre-registered our protocol and conducted a robust systematic search across three major scientific databases. Four investigators independently performed the search, with data extractions completed in duplicate. By including studies with a wide age range, we enhanced the generalizability of our findings to the general adult population. Notably, this is the first meta-analysis to report population-based, age- and sex-specific global prevalence estimates for moderate-to-severe MR.
We primarily included studies using Doppler echocardiography, the gold standard for diagnosing MR, along with two high-quality record-linkage studies from the UK that identified cases using relevant diagnostic codes. These studies were included under the assumption that all clinically significant MR cases would be captured in a high-income country with universal healthcare like the UK. Although not all cases in these studies were directly confirmed by Doppler echocardiography, an analysis restricted solely to echocardiographic studies yielded prevalence estimates closely aligned with our main results.
We carefully excluded studies where imaging or inclusion was based on medical indications, such as symptoms or concurrent conditions, to minimize selection bias that could inflate prevalence estimates. However, this strict exclusion resulted in a smaller pool of eligible studies, reducing statistical power for most subgroup analyses and limiting geographic coverage. Although data from four continents were included, the 22 study populations covered only nine countries, with limited representation from Asia and Africa and no data from South America and Oceania. More specifically, the majority of the studies were conducted in North America and Europe, representing approximately 6 million people, whereas the rest of the global population is represented by only 28,000 individuals. The Asian studies were confined to Korea and Turkey, and the one African study was conducted in Uganda; in both analyses these countries cannot be considered representative of their respective continents. As a result, these findings did not allow for reliable estimates of MR prevalence in Asia or Africa. This gap highlights the urgent need for additional, well-designed research in these regions.
Another limitation was the substantial statistical heterogeneity, leading to large confidence intervals and imprecise prevalence estimates, which is a common issue in the meta-analyses of prevalence studies [48,49,50]. While age explained about half of the heterogeneity, a significant portion remained unexplained. Variations in diagnostic tools, imaging techniques, and disease severity definitions—reflecting healthcare development differences across regions and time periods—may have contributed to this. Some heterogeneity may also be due to genuine differences in prevalence, potentially linked to unmeasured genetic or environmental factors specific to certain populations. Additionally, many primary studies had a significant delay between data collection and publication, and while our search was comprehensive, we could not identify more recent prevalence data. This limitation reflects gaps in primary data availability rather than flaws in the current synthesis.
5. Conclusions
Our study found that clinically significant MR is common, particularly among elderly people, with a non-linear association between age and prevalence. The scarcity of recent data, especially from certain regions, underscores the need for updated, high-quality epidemiological studies to better capture the global burden of MR. Advances in diagnostic techniques and increasing life expectancy make recent data crucial for assessing trends and potential changes in prevalence. This gap highlights the possibility that current data may underestimate MR prevalence in certain areas or populations. With the strong link between MR and age, countries experiencing rising life expectancy are likely to face an increasing MR burden. Preparing healthcare systems for the growing demand for diagnosis and treatment and improving universal access to interventions will be key to reducing morbidity and mortality, particularly in aging populations.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm14082749/s1, Appendix S1. Search algorithms; Appendix S2. Temporal evolution of the definition and assessment methods of moderate-to-severe MR; Supplementary Table S1. Methods and criteria used for identifying mitral regurgitation; Supplementary Table S2. Quality assessment of the included studies; Supplementary Table S3. Sensitivity multivariable mixed-effects meta-regression analysis reporting the independent association of mean age, proportion of males, study year, and continent with the prevalence of moderate-to-severe mitral regurgitation; Supplementary Table S4. Sensitivity multivariable mixed-effects meta-regression analysis reporting the independent association of mean age, proportion of males, study year, and predominant ethnicity with the prevalence of moderate-to-severe mitral regurgitation; Supplementary Figure S1. Funnel plot of the prevalence of moderate-to-severe mitral regurgitation in adults (N = 17). Supplementary Figure S2. Subgroup analysis of the prevalence of moderate-to-severe mitral regurgitation in adults by the predominant ethnicity of the participants (N = 17); Supplementary Figure S3. Bubble plot from univariable meta-regression analysis, illustrating the association of the mean age with the prevalence of moderate-to-severe mitral regurgitation; Supplementary Figure S4. Bubble plot from univariable meta-regression analysis, illustrating the association of proportion of males with the prevalence of moderate-to-severe mitral regurgitation; Supplementary Figure S5. Bubble plot from the univariable meta-regression analysis, illustrating the association of study year with the prevalence of moderate-to-severe mitral regurgitation.
Author Contributions
Conceptualization, A.S., S.B., and D.P.; formal analysis, G.F., S.B., and D.P.; data curation, all authors; writing—original draft preparation, G.F. and D.P.; writing—review and editing, all authors; supervision, S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially supported by “Ricerca Corrente” funding from the Italian Ministry of Health, granted to the IRCCS Humanitas Research Hospital.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available upon request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | Confidence Interval |
| ICD | International Classification of Diseases |
| MR | Mitral Regurgitation |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| UK | United Kingdom |
References
- Dziadzko, V.; Clavel, M.A.; Dziadzko, M.; Medina-Inojosa, J.R.; Michelena, H.; Maalouf, J.; Nkomo, V.; Thapa, P.; Enriquez-Sarano, M. Outcome and undertreatment of mitral regurgitation: A community cohort study. Lancet 2018, 391, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Akins, C.W.; Vahanian, A. Mitral regurgitation. Lancet 2009, 373, 1382–1394. [Google Scholar] [CrossRef] [PubMed]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: Executive summary. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Enriquez-Sarano, M.; Avierinos, J.F.; Messika-Zeitoun, D.; Detaint, D.; Capps, M.; Nkomo, V.; Scott, C.; Schaff, H.V.; Tajik, A.J. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N. Engl. J. Med. 2005, 352, 875–883. [Google Scholar] [CrossRef]
- Del Forno, B.; De Bonis, M.; Agricola, E.; Melillo, F.; Schiavi, D.; Castiglioni, A.; Montorfano, M.; Alfieri, O. Mitral valve regurgitation: A disease with a wide spectrum of therapeutic options. Nat. Rev. Cardiol. 2020, 17, 807–827. [Google Scholar] [CrossRef]
- von Kappelgaard, L.; Gislason, G.; Davidsen, M.; Zwisler, A.D.; Juel, K. Temporal trends and socioeconomic differences in the incidence of left-sided valvular heart disease in Denmark. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 608–615. [Google Scholar] [CrossRef]
- d’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef]
- Rahimi, K.; Mohseni, H.; Otto, C.M.; Conrad, N.; Tran, J.; Nazarzadeh, M.; Woodward, M.; Dwyer, T.; MacMahon, S. Elevated blood pressure and risk of mitral regurgitation: A longitudinal cohort study of 5.5 million United Kingdom adults. PLoS Med. 2017, 14, e1002404. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Kraft, C.D.; Levine, R.A.; Nihoyannopoulos, P.; Otto, C.M.; Quinones, M.A.; Rakowski, H.; et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and doppler echocardiography. J. Am. Soc. Echocardiogr. 2003, 16, 777–802. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Moura, L.; Pierard, L.A.; Agricola, E.; Popescu, B.A.; Tribouilloy, C.; Hagendorff, A.; Monin, J.L.; Badano, L.; Zamorano, J.L.; et al. Recommendations for the assessment of valvular regurgitation. Part 2: Mitral and tricuspid regurgitation (native and prosthetic valves). Eur. Heart J. Cardiovasc. Imaging 2013, 14, 612–621. [Google Scholar]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for noninvasive evaluation of native valvular regurgitation: A report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L.; Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the assessment of valvular regurgitation. Part 1: Aortic and pulmonary regurgitation (native and prosthetic valves). Eur. Heart J. Cardiovasc Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and incidence data. Int. J. Evid.-Based Healthcare 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Freeman, M.F.; Tukey, J.W. Transformations related to the angular and the square root. Ann. Math. Stat. 1950, 21, 607–611. [Google Scholar] [CrossRef]
- Miller, J.J. The inverse of the Freeman-Tukey double arcsine transformation. Am. Stat. 1978, 32, 138. [Google Scholar]
- Cochran, W.G. The comparison of percentages in matched samples. Biometrika 1950, 37, 256–266. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Interaction revisited: The difference between two estimates. BMJ 2003, 326, 219. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.; Hecht, S.R.; Van Tosh, A.; Lingam, U. Pulsed and continuous wave Doppler echocardiographic assessment of valvular regurgitation in normal subjects. J. Am. Coll. Cardiol. 1989, 13, 1540–1545. [Google Scholar] [CrossRef]
- Klein, A.L.; Burstow, D.J.; Tajik, A.J.; Zachariah, P.K.; Taliercio, C.P.; Taylor, C.L.; Bailey, K.R.; Seward, J.B. Age-related prevalence of valvular regurgitation in normal subjects: A comprehensive color flow examination of 118 volunteers. J. Am. Soc. Echocardiogr. 1990, 3, 54–63. [Google Scholar] [CrossRef]
- Singh, J.P.; Evans, J.C.; Levy, D.; Larson, M.G.; Larson, M.G.; Freed, L.A.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am. J. Cardiol. 1999, 83, 897–902. [Google Scholar] [CrossRef]
- Devereux, R.B.; Jones, E.C.; Roman, M.J.; Howard, B.V.; Fabsitz, R.R.; Liu, J.E.; Palmieri, V.; Welty, T.K.; Lee, E.T. Prevalence and correlates of mitral valve prolapse in a population-based sample of American Indians: The Strong Heart Study. Am. J. Med. 2001, 111, 679–685. [Google Scholar] [CrossRef]
- Fox, E.R.; Wilson, R.S.; Penman, A.D.; King, J.J.; Towery, J.G.; Butler, K.R.; McMullan, M.R.; Skelton, T.N.; Mosley, T.H.; Taylor, H.A. Epidemiology of pure valvular regurgitation in the large middle-aged African American cohort of the Atherosclerosis Risk in Communities study. Am. Heart J. 2007, 154, 1229–1234. [Google Scholar] [CrossRef]
- Sandrock, M.; Schmidt-Trucksäss, A.; Schmitz, D.; Niess, A.; Dickhuth, H.H. Influence of physiologic cardiac hypertrophy on the prevalence of heart valve regurgitation. J. Ultrasound Med. 2008, 27, 85–93. [Google Scholar] [CrossRef]
- van Bemmel, T.; Delgado, V.; Bax, J.J.; Gussekloo, J.; Blauw, G.J.; Westendorp, R.G.; Holman, E.R. Impact of valvular heart disease on activities of daily living of nonagenarians: The Leiden 85-plus study a population based study. BMC Geriatr. 2010, 10, 17. [Google Scholar] [CrossRef]
- Güvenç, T.S.; Canga, Y.; Karabağ, Y.; Ozen, K.; Balcı, B. Prevalence of mitral valve prolapse in residents living at moderately high altitude. Wilderness Environ. Med. 2012, 23, 300–306. [Google Scholar] [CrossRef]
- Vaes, B.; Rezzoug, N.; Pasquet, A.; Wallemacq, P.; Van Pottelbergh, G.; Matheï, C.; Vanoverschelde, J.L.; Degryse, J. The prevalence of cardiac dysfunction and the correlation with poor functioning among the very elderly. Int. J. Cardiol. 2012, 155, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, F.; Collerton, J.; Kingston, A.; Kenny, A.; Davies, K.; Jagger, C.; Robinson, L.; Kirkwood, T.B.; Keavney, B. Prevalence of left ventricular dysfunction in a UK community sample of very old people: The Newcastle 85+ study. Heart 2012, 98, 1418–1423. [Google Scholar] [CrossRef] [PubMed]
- Turker, Y.; Turker, Y.; Baltaci, D.; Basar, C.; Akkaya, M.; Ozhan, H.; Melen Investigators. The prevalence and clinical characteristics of mitral valve prolapse in a large population-based epidemiologic study: The MELEN study. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2208–2212. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Delling, F.N.; Rong, J.; Larson, M.G.; Lehman, B.; Fuller, D.; Osypiuk, E.; Stantchev, P.; Hackman, B.; Manning, W.J.; Benjamin, E.J.; et al. Evolution of mitral valve prolapse: Insights from the Framingham Heart Study. Circulation 2016, 133, 1688–1695. [Google Scholar] [CrossRef]
- Rubin, J.; Aggarwal, S.R.; Swett, K.R.; Kirtane, A.J.; Kodali, S.K.; Nazif, T.M.; Pu, M.; Dadhania, R.; Kaplan, R.C.; Rodriguez, C.J. Burden of valvular heart diseases in hispanic/latino individuals in the United States: The Echocardiographic Study of Latinos. Mayo Clin. Proc. 2019, 94, 1488–1498. [Google Scholar] [CrossRef]
- Kim, M.S.; Cho, S.J.; Park, S.J.; Cho, S.W.; Choi, S.H.; Kim, H.S.; Carriere, K.; Kim, E.K.; Chang, S.A.; Lee, S.C.; et al. Frequency and clinical associating factors of valvular heart disease in asymptomatic Korean adults. Sci. Rep. 2019, 9, 16741. [Google Scholar] [CrossRef]
- Nazarzadeh, M.; Pinho-Gomes, A.C.; Smith Byrne, K.; Canoy, D.; Raimondi, F.; Ayala Solares, J.R.; Otto, C.M.; Rahimi, K. Systolic blood pressure and risk of valvular heart disease: A mendelian randomization study. JAMA Cardiol. 2019, 4, 788–795. [Google Scholar] [CrossRef]
- Scheel, A.; Ssinabulya, I.; Aliku, T.; Bradley-Hewitt, T.; Clauss, A.; Clauss, S.; Crawford, L.; DeWyer, A.; Donofrio, M.T.; Jacobs, M.; et al. Community study to uncover the full spectrum of rheumatic heart disease in Uganda. Heart 2019, 105, 60–66. [Google Scholar] [CrossRef]
- He, S.; Deng, H.; Jiang, J.; Liu, F.; Liao, H.; Xue, Y.; Zheng, M.; Li, H.; Wu, S. The evolving epidemiology of elderly with degenerative valvular heart disease: The Guangzhou (China) Heart Study. Biomed. Res. Int. 2021, 2021, 9982569. [Google Scholar] [CrossRef]
- Yadgir, S.; Johnson, C.O.; Aboyans, V.; Adebayo, O.M.; Adedoyin, R.A.; Afarideh, M.; Alahdab, F.; Alashi, A.; Alipour, V.; Arabloo, J.; et al. Global, regional, and national burden of calcific aortic valve and degenerative mitral valve diseases, 1990-2017. Circulation 2020, 141, 1670–1680. [Google Scholar] [CrossRef]
- Hahn, R.T.; Clavel, M.A.; Mascherbauer, J.; Mick, S.L.; Asgar, A.W.; Douglas, P.S. Sex-related factors in valvular heart disease: JACC focus seminar 5/7. J. Am. Coll. Cardiol. 2022, 79, 1506–1518. [Google Scholar] [CrossRef] [PubMed]
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical outcome of mitral-valve prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 2024, 403, 1027–1050. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Delling, F.N.; Vasan, R.S. Epidemiology and pathophysiology of mitral valve prolapse: New insights into disease progression, genetics, and molecular basis. Circulation 2014, 129, 2158–2170. [Google Scholar] [CrossRef]
- Mata, D.A.; Ramos, M.A.; Bansal, N.; Khan, R.; Guille, C.; Di Angelantonio, E.; Sen, S. Prevalence of depression and depressive symptoms among resident physicians: A systematic review and meta-analysis. JAMA 2015, 314, 2373–2383. [Google Scholar] [CrossRef]
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global prevalence and incidence of tinnitus: A systematic review and meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef]
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.A. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).