Abstract
Background/Objectives: Chronic obstructive pulmonary disease (COPD) patients are at heightened risk of severe COVID-19 due to underlying respiratory impairment, systemic inflammation, and immune dysregulation. This review explores the hematological changes that occur in COPD patients with COVID-19 and their implications for disease progression, prognosis, and clinical management. Methods: We conducted a comprehensive analysis of recent peer-reviewed studies from medical databases including Clarivate Analytics, PubMed, and Google Scholar. Results: Hematological alterations, such as lymphopenia, elevated neutrophil-to-lymphocyte ratio (NLR), increased D-dimer and fibrinogen levels, inflammatory anemia, and erythrocyte dysfunction, are commonly observed in COPD patients with COVID-19. These changes are linked to immune suppression, hyperinflammation, oxidative stress, and thromboembolic complications. Conclusions: Hematological biomarkers are valuable tools for early risk assessments and guiding treatment strategies in this high-risk population. The regular monitoring of D-dimer, fibrinogen, and NLR is advisable. Prophylactic anticoagulation and immunomodulatory therapies, such as corticosteroids and IL-6 and IL-1 inhibitors, may improve clinical outcomes. Further clinical studies are needed to validate personalized approaches and explore antioxidant-based interventions.
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung disease marked by chronic respiratory symptoms, such as dyspnea, cough, sputum production, and exacerbations, caused by airway (e.g., bronchitis and bronchiolitis) and/or alveolar (e.g., emphysema) abnormalities that lead to persistent, often progressive, airflow obstruction [1]. The disease is primarily caused by long-term exposure to harmful particles and gases, with cigarette smoking being the leading risk factor. In 2016, an estimated 251 million cases of COPD were recorded globally, according to the Global Burden of Disease (GBD) study [2]. The Burden of Obstructive Lung Disease initiative and Global Burden of Disease collaborators have led efforts to estimate global COPD burden, reporting between 212 and 384 million cases from 2010 to 2019 based on spirometry data refined through risk factor modeling [3]. Additionally, projections from the World Health Organization (WHO) suggest that by 2030, COPD will rank as the third leading cause of death worldwide [4].
The pathogenesis of COPD involves an imbalance between proteases and antiproteases, oxidative stress, and chronic inflammation, which contribute to airway remodeling, mucus hypersecretion, and lung parenchymal destruction [5]. COPD is a major global health issue, ranking as the third leading cause of death worldwide, with an increasing burden in low- and middle-income countries [2].
Patients with COPD are at a significantly higher risk of developing severe COVID-19 infections. Pre-existing respiratory impairment and chronic inflammation in COPD patients create a favorable environment for viral infections, leading to increased disease severity and complications [6]. The presence of COPD has been associated with higher rates of hospitalization, intensive care unit (ICU) admissions, and mortality in COVID-19 patients [7]. The heightened vulnerability in COPD patients is attributed to factors such as reduced mucociliary clearance, altered immune responses, and increased expression of angiotensin-converting enzyme 2 (ACE2) receptors in the lungs, which facilitate SARS-CoV-2 entry [8].
The COVID-19 pandemic, with an estimated global excess mortality of 14.9 million in 2020 and 2021 according to WHO, has had a profound impact not only on human health but also across various fields, including epidemiology, pharmaceutical innovation, behavioral sciences, and healthcare system management [9]. It possess a greater risk of severe illness and death in individuals with underlying comorbidities, such as cardiovascular disease, diabetes, and chronic respiratory conditions. These comorbidities, along with factors like advanced age, severe lymphopenia, elevated CRP, and D-dimer levels above 1 μg/L, are strongly associated with a poor prognosis and increased mortality rates [10].
Hematological alterations play a crucial role in predicting COVID-19 severity in COPD patients. Parameters such as lymphopenia, elevated neutrophil-to-lymphocyte ratio (NLR), increased levels of C-reactive protein (CRP), and thrombocytopenia have been identified as markers of disease progression and poor outcomes [11]. In COPD patients, systemic inflammation is already elevated, which may exacerbate the hyperinflammatory state induced by COVID-19, leading to cytokine storms and severe respiratory failure [12]. Understanding these hematological changes is essential for early risk stratification, timely intervention, and improved clinical management of COPD patients with COVID-19.
The aim of this review is to investigate the hematological changes that occur in patients with COPD who are infected with COVID-19 and to explore how these changes influence disease progression, clinical outcomes, and therapeutic strategies. The review seeks to highlight the pathophysiological overlap between the two conditions, particularly in terms of immune dysregulation, coagulation abnormalities, and oxidative stress, and to evaluate the clinical utility of hematological biomarkers for risk stratification and management.
2. Methodology
This review is based on a comprehensive analysis of peer-reviewed studies published between January 2020 and December 2023, which were retrieved from databases including Clarivate Analytics, PubMed, and Google Scholar. Studies were selected based on their relevance to hematological abnormalities in COPD and COVID-19, particularly those addressing markers such as lymphopenia, NLR, D-dimer, fibrinogen, and indicators of oxidative stress. Both clinical and mechanistic research was included, focusing on inflammatory and coagulopathic pathways, erythropoietic dysfunction, and prognostic implications.
3. Shared Mechanisms Between COPD and COVID-19
3.1. Chronic Inflammation and Cytokine Storms
Chronic inflammation is a key pathological feature of both COPD and severe COVID-19, leading to dysregulated immune responses and systemic complications (Table 1). The interplay between chronic inflammation and hematological disturbances highlights the need for targeted anti-inflammatory and anticoagulant strategies in COPD patients at risk of severe COVID-19 complications. Understanding these mechanisms can aid in the development of personalized treatment approaches to mitigate disease progression and improve patient outcomes.

Table 1.
Chronic inflammation and cytokine storms in COPD and severe COVID-19.
Table 1 summarizes the key inflammatory mediators and immune mechanisms involved in the cytokine storm observed in both COPD and severe COVID-19, highlighting their overlapping pathophysiological pathways.
3.2. Hypoxia and Oxidative Stress
COPD and severe COVID-19 are both characterized by hypoxia and oxidative stress, which contribute to systemic complications beyond lung pathology. Chronic hypoxia triggers adaptive and maladaptive responses in hematopoiesis and coagulation [13], while oxidative stress results in cellular damage and inflammation [14].
Both hypoxia and oxidative stress play a central role in the systemic complications of COPD and severe COVID-19, particularly in hematopoietic changes, immune dysregulation, and coagulation abnormalities. Understanding these mechanisms highlights the need for therapeutic strategies that target hypoxia-induced inflammation and oxidative damage, such as antioxidant therapies, oxygen supplementation, and anti-inflammatory treatments.
3.2.1. Hypoxia-Induced Hematological and Coagulation Alterations in COPD and Severe COVID-19
Chronic hypoxia plays a critical role in hematopoiesis, inflammation, and coagulation dysfunction, significantly affecting disease progression in both COPD and severe COVID-19. The body’s response to persistent oxygen deprivation leads to a cascade of adaptive and maladaptive mechanisms, influencing erythropoiesis, leukocyte activity, and thrombotic risk.
Hypoxia acts as a primary stimulus for erythropoiesis, triggering the release of erythropoietin (EPO) from the kidneys to promote red blood cell (RBC) production in an effort to enhance oxygen transport, which is regulated by hypoxia-inducible factors (HIFs) [15]. In COPD, prolonged hypoxia can lead to secondary polycythemia [16], characterized by increased hematocrit levels, which may contribute to blood hyperviscosity, increased cardiovascular burden, and a higher risk of thrombotic events [17,18,19]. acute COPD exacerbations are linked to increased systemic inflammation, which promotes platelet activation, endothelial dysfunction, enhanced coagulation, and impaired fibrinolysis, as indicated by elevated platelet–monocyte complexes (PMCs), monocyte Mac-1 expression, Bon Willebrand factor (VWF), and thrombin generation, while prolonged clot lysis time and platelet hyperreactivity at admission are associated with a higher risk of relapse [20].
However, in severe COVID-19, erythropoiesis appears to be dysregulated, often leading to anemia instead of polycythemia [21]. In a study of 179 infected patients, 20.3% had a positive Coombs test (mainly IgG), though no cases of autoimmune hemolysis were found; Coombs-positive patients had more severe anemia, required more transfusions and intensive care, and showed an inflammatory anemia pattern with elevated hepcidin and ferritin but inappropriately low EPO and erythroferrone, with iron metabolism markers correlating with disease severity [22]. Consequently, while COPD patients frequently experience elevated RBC counts [23], COVID-19 patients may present with normocytic or microcytic anemia [24,25], contributing to worsened oxygen transport and disease severity.
In addition to altering RBC production, hypoxia significantly influences leukocyte function, leading to a state of chronic inflammation. Low oxygen availability enhances the release of pro-inflammatory cytokines, particularly IL-6, TNF-α, and IL-8, which promote neutrophil activation and immune cell recruitment [26]. This exaggerated inflammatory response contributes to the systemic inflammation observed in COPD and plays a role in the cytokine storm characteristic of severe COVID-19 [27].
A central regulator of this process is hypoxia-inducible factor 1-alpha (HIF-1α), a transcription factor that becomes stabilized under hypoxic conditions, leading to the upregulation of inflammatory pathways [28] by activating EGFR/PI3K/AKT pathway [29]. HIF-1α activation not only amplifies neutrophil-driven inflammation but also impairs immune resolution, resulting in sustained tissue damage and increased susceptibility to exacerbations in COPD and multi-organ failure in COVID-19 [30,31,32].
Chronic hypoxia is a well-established driver of hypercoagulability [33], predisposing patients to an increased risk of deep vein thrombosis [34,35], pulmonary embolism [36,37], and microvascular thrombosis [38,39]. This prothrombotic state is primarily mediated by
- -
- Platelet activation and aggregation, leading to enhanced clot formation [40];
- -
- Elevated fibrinogen levels, which contribute to increased blood viscosity [40];
- -
- The upregulation of tissue factor (TF), a key initiator of the extrinsic coagulation cascade [41].
In COPD, chronic inflammation and endothelial dysfunction promote a hypercoagulable state, increasing the risk of cardiovascular events and stroke [42]. Similarly, in severe COVID-19, these mechanisms are further exacerbated by a viral infection, leading to the development of COVID-19-associated coagulopathy, which is strongly linked to higher mortality rates [43]. The presence of elevated D-dimer levels, along with increased fibrinogen and platelet activation, serves as a critical marker of thrombotic complications in both diseases [44].
3.2.2. Increased Production of Reactive Oxygen Species (ROS) and Their Impact on Blood Cells
Oxidative stress occurs when there is an imbalance between reactive oxygen species (ROS) production and the body’s antioxidant defense, leading to cellular and tissue damage. In both COPD and severe COVID-19, excessive ROS generation plays a crucial role in disease progression, contributing to systemic inflammation, hematological alterations, and vascular dysfunction [45,46].
Several biological processes contribute to increased ROS production, further amplifying inflammation and tissue injury. Chronic hypoxia and inflammation lead to excessive mitochondrial ROS production, exacerbating oxidative stress and impairing cellular function [47]. During inflammatory responses, neutrophils generate superoxide radicals (O2−), hydrogen peroxide (H2O2), and hydroxyl radicals (OH−), which contribute to tissue destruction and immune dysregulation [48]. ROS reduce the availability of endothelial nitric oxide (NO), leading to vasoconstriction, impaired blood flow, and increased thrombotic risk [49].
ROS directly affect blood cell function and survival, playing a key role in hematological disturbances observed in COPD and COVID-19. Oxidative stress damages RBC membranes, leading to reduced lifespan, hemolysis, and anemia, worsening oxygen transport [50,51,52]. ROS hyperactivate neutrophils and macrophages, intensifying inflammatory responses and immune dysregulation [53,54,55]. Moreover, ROS promote platelet activation and aggregation, increasing the risk of thrombosis, microvascular injury, and multi-organ dysfunction [56,57].
The pathological effects of excessive ROS production have severe consequences in both COPD and COVID-19. In COPD, chronic oxidative stress accelerates lung tissue damage, systemic inflammation, and cardiovascular complications, leading to disease progression and frequent exacerbations [58]. In severe COVID-19, heightened ROS production is strongly associated with endothelial dysfunction, hyperinflammation (cytokine storm), and increased mortality risk [55].
Both hypoxia and oxidative stress play a central role in the systemic complications of COPD and severe COVID-19, particularly in hematopoietic changes, immune dysregulation, and coagulation abnormalities (Table 2). Understanding these mechanisms highlights the need for therapeutic strategies that target hypoxia-induced inflammation and oxidative damage, such as antioxidant therapies, oxygen supplementation, and anti-inflammatory treatments.
Table 2.
Biomarkers of hypoxia and oxidative stress in COPD and severe COVID-19.
4. Hematological Changes in COPD Patients with COVID-19
Patients suffering from COPD and COVID-19 often exhibit significant hematological changes, reflecting the complex interplay between chronic inflammation, immune dysregulation, and hypercoagulability [83]. These hematological alterations contribute to disease severity, a poor prognosis, and increased risk of complications.
4.1. Lymphopenia and Impaired Immune Responses
Lymphopenia is a common hematological abnormality observed in COPD patients infected with SARS-CoV-2 [84]. This reduction in lymphocytes, particularly CD4+ and CD8+ T cells, impairs the host’s ability to mount an effective antiviral immune response [85,86]. CD4+ T cells play a crucial role in orchestrating adaptive immunity by activating B cells and cytotoxic T cells, while CD8+ T cells are essential for the direct elimination of virus-infected cells [87]. The depletion of these immune cells weakens the body’s defense mechanisms, allowing for uncontrolled viral replication and prolonged infection [88].
Another critical marker of immune dysfunction in COPD patients with COVID-19 is an increased NLR. A high NLR is indicative of an exaggerated inflammatory response and has been established as a reliable prognostic marker for severe disease progression and mortality [89]. The combination of lymphopenia and elevated neutrophil counts promotes systemic inflammation, tissue damage, and multi-organ failure, exacerbating the already compromised pulmonary function in COPD patients [90].
4.2. Coagulopathy and Thromboembolic Risk
Coagulopathy is a significant concern in COPD patients with COVID-19 due to the heightened inflammatory state and endothelial dysfunction associated with both conditions. Elevated levels of D-dimer, fibrinogen, and vWF have been reported in these patients, reflecting an increased propensity for thrombotic complications. D-dimer, a fibrin degradation product, serves as a biomarker of hypercoagulability and is frequently elevated in severe COVID-19 cases, correlating with a higher risk of adverse outcomes [91].
One of the most concerning thromboembolic complications in COPD patients with COVID-19 is pulmonary embolism (PE) [92]. The chronic hypoxia and systemic inflammation present in COPD contribute to a prothrombotic environment, which, when compounded by COVID-19, significantly increases the risk of PE [83]. Furthermore, the presence of disseminated intravascular coagulation has been observed in critically ill COVID-19 patients, manifesting as widespread microvascular thrombosis and the consumption of clotting factors, leading to life-threatening hemorrhagic complications [93]. These hematological alterations necessitate close monitoring and early intervention with anticoagulant therapy to mitigate thrombotic risks.
4.3. Inflammatory Anemia and Erythrocyte Dysfunction
Chronic hypoxia in COPD patients leads to compensatory erythropoiesis, often resulting in secondary polycythemia. However, in the context of COVID-19, systemic inflammation disrupts normal erythropoiesis, leading to inflammatory anemia (also known as anemia of chronic disease) [94,95,96]. Pro-inflammatory cytokines such as IL-6 and TNF-α interfere with iron metabolism by increasing hepcidin levels, which inhibits iron absorption and sequestration, thus impairing hemoglobin synthesis [97].
Additionally, erythrocyte dysfunction is a notable concern in COPD patients with COVID-19. Oxidative stress and systemic inflammation contribute to altered erythrocyte membrane properties, reducing their deformability and increasing their susceptibility to hemolysis [98]. This leads to impaired oxygen delivery to tissues, further exacerbating hypoxia and worsening disease outcomes [99]. The combination of chronic hypoxia, inflammation-driven iron deficiency, and erythrocyte dysfunction highlights the complex hematological challenges faced by COPD patients during COVID-19 infection [100,101].
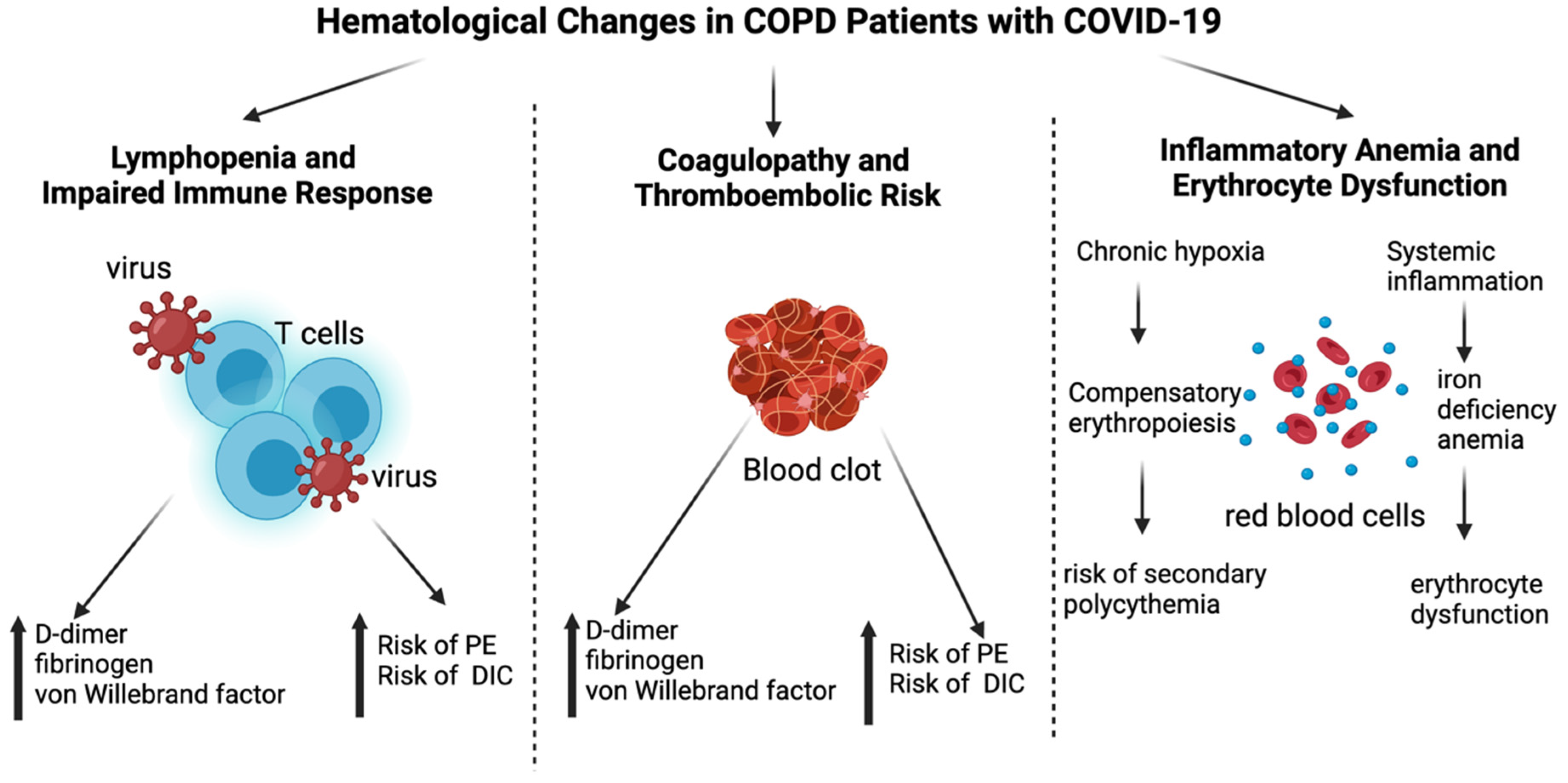
Figure 1 highlights the hematological changes in COPD patients with COVID-19, focusing on three main aspects: lymphopenia and impaired immune response, coagulopathy and thromboembolic risk, as well as inflammatory anemia and erythrocyte dysfunction, each contributing to disease severity and patient prognosis.
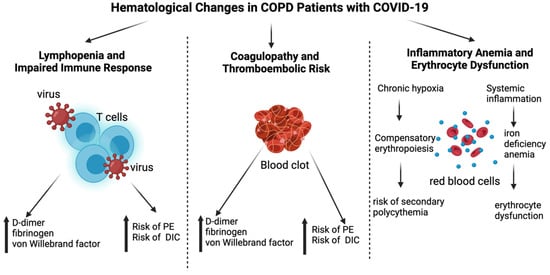
Figure 1.
Hematological changes in COPD patients with COVID-19. This figure illustrates the key hematological changes observed in COPD patients with COVID-19. The three main categories included are as follows: 1. Lymphopenia and Impaired Immune Response—Characterized by a reduction in CD4+ and CD8+ T cells, leading to weakened antiviral defense, and an increased neutrophil-to-lymphocyte ratio (NLR), which serves as a prognostic marker; 2. Coagulopathy and Thromboembolic Risk—Marked by elevated D-dimer, fibrinogen, and von Willebrand factor levels, increasing the risk of pulmonary embolism (PE) and disseminated intravascular coagulation (DIC); 3. Inflammatory Anemia and Erythrocyte Dysfunction—Chronic hypoxia induces compensatory erythropoiesis, increasing the risk of secondary polycythemia, while systemic inflammation contributes to iron deficiency anemia and erythrocyte dysfunction. Arrows indicate relationships between the central concept and its specific pathological mechanisms. Created with Biorender.com.
5. Clinical Implications and Therapeutic Strategies
5.1. Monitoring Hematological Markers
The management of COPD patients infected with COVID-19 necessitates the diligent monitoring of hematological markers, which act as crucial prognostic indicators. Among these markers, D-dimer, fibrinogen, and the neutrophil-to-lymphocyte ratio (NLR) are particularly significant in assessing disease severity and predicting adverse outcomes [102].
The role of hematological markers in prognosis is significant in various medical conditions. Elevated D-dimer levels are strongly associated with an increased risk of thrombotic complications, particularly in COVID-19 patients, and can serve as an early indicator of coagulopathy [103]. High fibrinogen levels reflect an ongoing inflammatory response and a heightened risk of clot formation, both of which are crucial concerns in COPD patients with COVID-19 [104]. Additionally, a high neutrophil-to-lymphocyte ratio (NLR) is indicative of an exaggerated inflammatory response and is correlated with worse clinical outcomes in COVID-19 [105].
Given the prognostic significance of these hematological markers, screening algorithms for COPD patients with COVID-19 should incorporate routine monitoring of D-dimer, fibrinogen, and NLR. The early identification of abnormalities in these markers can help clinicians stratify patients based on risk levels and tailor interventions accordingly.
The table below outlines essential hematological monitoring strategies used in the clinical management of COPD patients with COVID-19, emphasizing their diagnostic and prognostic value, along with associated benefits and limitations (Table 3).
Table 3.
Key hematological monitoring strategies in COPD patients with COVID-19.
In clinical practice, hematological monitoring should begin at hospital admission for all COPD patients diagnosed with COVID-19. For hospitalized patients, D-dimer, fibrinogen, and NLR should be assessed on admission [114]. Suggested thresholds to consider therapeutic escalation include:
- D-dimer > 1.0 µg/mL, which is associated with increased thrombotic risk and may justify the initiation or intensification of anticoagulation;
- NLR > 7, which is predictive of severe disease progression and a poor prognosis;
- Fibrinogen > 4 g/L, which is indicative of high inflammatory burden.
These values should be interpreted along with clinical status, oxygenation levels, and imaging findings. Individualized management strategies based on dynamic changes in these markers can support timely intervention and improved outcomes.
5.2. Anticoagulation Therapy in COPD and COVID-19
Prophylactic anticoagulation plays a crucial role in preventing thromboembolic complications, particularly in patients with COPD and COVID-19, who are already prone to clot formation due to their compromised respiratory and circulatory systems. Given these risks, prophylactic anticoagulation is strongly recommended as a preventative measure to reduce morbidity and mortality in affected patients [115].
The primary benefits of prophylactic anticoagulation include the prevention of deep vein thrombosis (DVT) and pulmonary embolism (PE), which are common complications in severe COVID-19 cases, often leading to worsened respiratory function and increased mortality rates [116]. By inhibiting excessive clotting, anticoagulation significantly reduces the likelihood of these life-threatening events. Another key benefit is the reduction in mortality and morbidity. Patients receiving anticoagulation therapy show lower rates of thrombotic complications, ultimately improving their overall prognosis. By preventing clot formation, these therapies contribute to better systemic oxygenation and reduced strain on the cardiovascular system, thereby enhancing recovery outcomes.
Several anticoagulants are available for prophylactic use, each with specific advantages and considerations for patients with COPD and COVID-19.
Low-molecular-weight heparin (LMWH) is a class of anticoagulants and is often the preferred choice due to its predictable pharmacokinetics and lower risk of bleeding compared to unfractionated heparin [117]. LMWH is administered via subcutaneous injection and does not require frequent laboratory monitoring, making it a practical option for hospitalized and critically ill patients.
Direct oral anticoagulants (DOACs) are anticoagulants which offer an alternative to LMWH and are particularly useful for long-term management. However, their use requires careful dose adjustments in patients with renal impairment, which is a common comorbidity in individuals with COPD [118]. While DOACs provide convenience through oral administration, their safety profile necessitates close monitoring, especially in those with fluctuating renal function [119]. Studies have shown that direct oral anticoagulants (DOACs), such as apixaban, rivaroxaban, dabigatran, and edoxaban, offer superior efficacy and safety compared to traditional oral anticoagulant (OAC) therapies, including vitamin K antagonists (VKAs), in patients with pulmonary disease [120].
Additional clinical considerations should be given to COPD patients with coexisting COVID-19 and renal impairment. Renal dysfunction can significantly alter the pharmacokinetics of anticoagulants, particularly DOACs, increasing the risk of bleeding or subtherapeutic dosing. In this context, the regular monitoring of renal function (e.g., serum creatinine and eGFR) is essential to guide dose adjustments or the choice of anticoagulant type [121].
Although DOACs and LMWH are generally preferred, vitamin K antagonists (VKAs) such as warfarin remain in use for certain patient populations, particularly those with mechanical heart valves, antiphospholipid syndrome, or severe renal impairment, where DOACs may be contraindicated. VKAs require regular INR monitoring but may be a practical option in settings where other anticoagulants are not available or are cost-prohibitive [122].
Table 4 presents a comparative summary of anticoagulant options commonly used in COPD patients with COVID-19, detailing their mechanisms of action, clinical benefits, and associated risks to support individualized treatment decisions.
Table 4.
Comparative overview of anticoagulant therapies in COPD patients with COVID-19.
In conclusion, prophylactic anticoagulation is a critical intervention in managing patients with COPD and COVID-19. By mitigating the risks associated with thromboembolic events, these treatments contribute significantly to improving patient outcomes, reducing complications, and ultimately enhancing survival rates in this vulnerable population. Further research and clinical guidelines will continue to refine the best practices for anticoagulation strategies, ensuring optimal care for high-risk patients.
5.3. Immunomodulators and Anti-Inflammatory Therapy
Inflammatory responses play a crucial role in the pathophysiology of COVID-19-associated respiratory deterioration, particularly in COPD patients who already have compromised pulmonary function. Immunomodulatory therapies aim to control cytokine storms and excessive inflammation [129].
Corticosteroids, such as dexamethasone, are widely used in COVID-19 management due to their ability to reduce lung inflammation and lower mortality in severe cases. Their benefits include reducing cytokine-mediated lung damage, improving oxygenation, and decreasing the need for mechanical ventilation [130]. However, they also carry certain risks, such as immune suppression, which can increase susceptibility to secondary infections and worsen COPD exacerbations [131].
Severe COVID-19 can lead to a cytokine storm, which exacerbates lung injury. Monoclonal antibodies such as Tocilizumab (IL-6 inhibitor) and Anakinra (IL-1 receptor antagonist) have been investigated for their role in mitigating excessive immune responses [132].
Another emerging strategy involves specialized pro-resolving mediators (SPMs), such as resolvins, protectins, and maresins, which actively promote the resolution phase of inflammation without inducing immunosuppression [133]. SPMs have shown potential in preclinical models for reducing cytokine-driven damage and restoring immune homeostasis [133], which could be particularly beneficial in COPD patients with COVID-19 experiencing excessive inflammatory responses.
Table 5 outlines key immunomodulatory agents used in COPD patients with COVID-19, focusing on their mechanisms of action, therapeutic benefits, and potential risks, with a particular emphasis on cytokine-targeted strategies.
Table 5.
Overview of immunomodulatory therapies in the management of COPD patients with COVID-19.
In addition to acute management, attention must be given to the long-term consequences of SARS-CoV-2 infection in COPD patients. Recent studies have highlighted that individuals with COPD are particularly prone to developing post-COVID-19 syndrome, often characterized by persistent fatigue, dyspnea, and neuropsychiatric symptoms. In a cohort study conducted in Romania, symptoms such as fatigue (36%), cough (26%), and myalgia (23%) were observed up to six months post-infection, especially in those with pre-existing respiratory conditions and comorbidities [139]. These findings underscore the importance of integrated post-discharge care and tailored rehabilitation for COPD patients recovering from COVID-19.
6. Conclusions
Patients with chronic obstructive pulmonary disease (COPD) represent a high-risk population during the COVID-19 pandemic due to their underlying chronic inflammation, persistent hypoxia, and immune dysregulation. The presence of SARS-CoV-2 infection further exacerbates these conditions by triggering an intense systemic inflammatory response, which is closely associated with significant hematological changes.
Common hematological abnormalities in COPD patients with COVID-19, such as lymphopenia, elevated NLR, increased levels of D-dimer and fibrinogen, inflammatory anemia, and erythrocyte dysfunction, have been strongly correlated with disease severity, a poor prognosis, and a higher risk of thromboembolic complications. These alterations serve not only as reflections of disease progression but also as important prognostic markers that can guide early clinical intervention.
Chronic hypoxia and oxidative stress, which are hallmark features of both COPD and severe COVID-19, amplify inflammatory and thrombotic responses through mechanisms that involve HIFs and the excessive production of reactive oxygen species (ROS). These processes contribute to systemic damage, cellular dysfunction, and vascular complications that significantly impact patient outcomes.
From a clinical perspective, the continuous monitoring of hematological markers, particularly D-dimer, fibrinogen, and NLR, is crucial for timely risk stratification and therapeutic decision-making. Prophylactic anticoagulation-tailored anti-inflammatory therapies and immunomodulators have emerged as key strategies in managing these patients, and their use should be personalized based on individual hematological profiles and comorbid conditions.
Future research should focus on evaluating the efficacy and safety of anticoagulants and immunomodulatory treatments specifically in COPD patients with COVID-19. Additionally, clinical guidelines should emphasize personalized approaches that integrate hematological assessments as core components of care. Investigating the therapeutic potential of antioxidant strategies and targeted interventions to reduce oxidative stress may further improve clinical outcomes in this vulnerable population.
Author Contributions
Conceptualization, G.M. and C.C.; methodology, G.M.; writing—original draft preparation, G.M., G.N. and C.C.; writing—review and editing, G.M. and C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Meng, Y.; Ji, Q.; Zhang, A.; Zhan, Y. Trends in the prevalence and incidence of chronic obstructive pulmonary disease among adults aged ≥50 years in the United States, 2000–2020. Chronic Dis. Transl. Med. 2024, 10, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Boers, E.; Barrett, M.; Su, J.G.; Benjafield, A.V.; Sinha, S.; Kaye, L.; Zar, H.J.; Vuong, V.; Tellez, D.; Gondalia, R.; et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Netw. Open 2023, 6, e2346598. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I.; NIHR RESPIRE Global Respiratory Health Unit. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]
- Al Wachami, N.; Guennouni, M.; Iderdar, Y.; Boumendil, K.; Arraji, M.; Mourajid, Y.; Bouchachi, F.Z.; Barkaoui, M.; Louerdi, M.L.; Hilali, A.; et al. Estimating the global prevalence of chronic obstructive pulmonary disease (COPD): A systematic review and meta-analysis. BMC Public Health 2024, 24, 297. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M. Chronic obstructive pulmonary disease is associated with severe coronavirus disease 2019 (COVID-19). Respir. Med. 2020, 167, 105941. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Alghamdi, S.M.; Almehmadi, M.; Alqahtani, A.S.; Quaderi, S.; Mandal, S.; Hurst, J.R. Prevalence, Severity and Mortality associated with COPD and Smoking in patients with COVID-19: A Rapid Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0233147. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.; Alghamdi, R.; Guallart, I.; Bergamini, M.; Yu, P.; Froum, S.; Cho, S.-C. Patient-Related Risk Factors for Maxillary Sinus Augmentation Procedures: A Systematic Literature Review. Int. J. Periodontics Restor. Dent. 2021, 41, e121–e128. [Google Scholar] [CrossRef]
- Ashmore, P.; Sherwood, E. An overview of COVID-19 global epidemiology and discussion of potential drivers of variable global pandemic impacts. J. Antimicrob. Chemother. 2023, 78 (Suppl. S2), ii2–ii11. [Google Scholar] [CrossRef]
- Marginean, C.M.; Popescu, M.; Vasile, C.M.; Cioboata, R.; Mitrut, P.; Popescu, I.A.S.; Biciusca, V.; Docea, A.O.; Mitrut, R.; Marginean, I.C.; et al. Challenges in the Differential Diagnosis of COVID-19 Pneumonia: A Pictorial Review. Diagnostics 2022, 12, 2823. [Google Scholar] [CrossRef]
- Zeng, Y.; Cai, S.; Chen, Y.; Duan, J.; Zhao, Y.; Li, X.; Ma, L.; Liu, Q.; Zhu, Y.; Chen, M.; et al. Current Status of the Treatment of COPD in China: A Multicenter Prospective Observational Study. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 3227–3237. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, L.M.; Luppi, F.; Beghé, B.; Rabe, K.F. Complex chronic comorbidities of COPD. Eur. Respir. J. 2008, 31, 204–212. [Google Scholar] [CrossRef]
- Alvarez-Martins, I.; Remédio, L.; Matias, I.; Diogo, L.N.; Monteiro, E.C.; Dias, S. The impact of chronic intermittent hypoxia on hematopoiesis and the bone marrow microenvironment. Pflüg. Arch.-Eur. J. Physiol. 2016, 468, 919–932. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, K.; Anand, K.; Palanisamy, S.; Anathy, V. Editorial: Oxidative stress related to cellular metabolism in lung health and diseases. Front. Pharmacol. 2022, 13, 1015423. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Regulation of Erythropoiesis by the Hypoxia-Inducible Factor Pathway: Effects of Genetic and Pharmacological Perturbations. Annu. Rev. Med. 2023, 74, 307–319. [Google Scholar] [CrossRef]
- Zhang, J.; DeMeo, D.L.; Silverman, E.K.; Make, B.J.; Wade, R.C.; Wells, J.M.; Cho, M.H.; Hobbs, B.D. Secondary polycythemia in chronic obstructive pulmonary disease: Prevalence and risk factors. BMC Pulm. Med. 2021, 21, 235. [Google Scholar] [CrossRef]
- Patel, A.R.; Hurst, J.R. Extrapulmonary comorbidities in chronic obstructive pulmonary disease: State of the art. Expert Rev. Respir. Med. 2011, 5, 647–662. [Google Scholar] [CrossRef]
- Santos, S.; Manito, N.; Sánchez-Covisa, J.; Hernández, I.; Corregidor, C.; Escudero, L.; Rhodes, K.; Nordon, C. Risk of severe cardiovascular events following COPD exacerbations: Results from the EXACOS-CV study in Spain. Rev. Esp. Cardiol. 2025, 78, 138–150. [Google Scholar] [CrossRef]
- Morgan, A.; Herrett, E.; De Stavola, B.; Smeeth, L.; Quint, J. COPD disease severity and the risk of venous thromboembolic events: A matched case-control study. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 899. [Google Scholar] [CrossRef]
- Van Der Vorm, L.N.; Li, L.; Huskens, D.; Hulstein, J.J.J.; Roest, M.; De Groot, P.G.; Ten Cate, H.; De Laat, B.; Remijn, J.A.; Simons, S.O. Acute exacerbations of COPD are associated with a prothrombotic state through platelet-monocyte complexes, endothelial activation and increased thrombin generation. Respir. Med. 2020, 171, 106094. [Google Scholar] [CrossRef]
- Hanson, A.L.; Mulè, M.P.; Ruffieux, H.; Mescia, F.; Bergamaschi, L.; Pelly, V.S.; Turner, L.; Kotagiri, P.; Cambridge Institute of Therapeutic Immunology and Infectious Disease–National Institute for Health Research (CITIID–NIHR) COVID BioResource Collaboration; Göttgens, B.; et al. Iron dysregulation and inflammatory stress erythropoiesis associates with long-term outcome of COVID-19. Nat. Immunol. 2024, 25, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, L.; Pirotte, M.; Lebeau, A.; Ernst, M.; Fillet, M.; Devey, A.; Schmitt, J.; Cobraiville, G.; Binsfeld, M.; Gofflot, S.; et al. Alterations of erythropoiesis in COVID-19 patients: Prevalence of positive Coombs tests and iron metabolism. Ther. Adv. Hematol. 2023, 14, 20406207231199836. [Google Scholar] [CrossRef]
- Saad, E.; Maamoun, B.; Nimer, A. Increased Red Blood Cell Distribution Predicts Severity of Chronic Obstructive Pulmonary Disease Exacerbation. J. Pers. Med. 2023, 13, 843. [Google Scholar] [CrossRef]
- Elemam, N.M.; Talaat, I.M.; Bayoumi, F.A.; Zein, D.; Georgy, R.; Altamimi, A.; Alkhayyal, N.; Habbal, A.; Al Ali, F.; ElKhider, A.; et al. Peripheral blood cell anomalies in COVID-19 patients in the United Arab Emirates: A single-centered study. Front. Med. 2022, 9, 1072427. [Google Scholar] [CrossRef] [PubMed]
- Chandran, N.; Sigamani, K.; Khadeja Bi, A. Hematological Profile in COVID-19 Infection Among Patients in a Tertiary Care Hospital in Tamil Nadu, South India. Cureus 2022, 14, e30731. [Google Scholar] [CrossRef]
- Hacievliyagil, S.S.; Gunen, H.; Mutlu, L.C.; Karabulut, A.B.; Temel, İ. Association between cytokines in induced sputum and severity of chronic obstructive pulmonary disease. Respir. Med. 2006, 100, 846–854. [Google Scholar] [CrossRef]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.-R.; Wang, A.-L.; Li, Y.-Q. Hypoxia-inducible factor 1-alpha is a driving mechanism linking chronic obstructive pulmonary disease to lung cancer. Front. Oncol. 2022, 12, 984525. [Google Scholar] [CrossRef]
- Zhang, H.-X.; Yang, J.-J.; Zhang, S.-A.; Zhang, S.-M.; Wang, J.-X.; Xu, Z.-Y.; Lin, R.-Y. HIF-1α promotes inflammatory response of chronic obstructive pulmonary disease by activating EGFR/PI3K/AKT pathway. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 6077–6084. [Google Scholar]
- Walmsley, S.R.; Print, C.; Farahi, N.; Peyssonnaux, C.; Johnson, R.S.; Cramer, T.; Sobolewski, A.; Condliffe, A.M.; Cowburn, A.S.; Johnson, N.; et al. Hypoxia-induced neutrophil survival is mediated by HIF-1α–dependent NF-κB activity. J. Exp. Med. 2005, 201, 105–115. [Google Scholar] [CrossRef]
- Serebrovska, Z.O.; Chong, E.Y.; Serebrovska, T.V.; Tumanovska, L.V.; Xi, L. Hypoxia, HIF-1α, and COVID-19: From pathogenic factors to potential therapeutic targets. Acta Pharmacol. Sin. 2020, 41, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Jahani, M.; Dokaneheifard, S.; Mansouri, K. Hypoxia: A key feature of COVID-19 launching activation of HIF-1 and cytokine storm. J. Inflamm. Lond. Engl. 2020, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Zhao, Y.-Y.; Evans, C.E. The stimulation of thrombosis by hypoxia. Thromb. Res. 2019, 181, 77–83. [Google Scholar] [CrossRef]
- Ninivaggi, M.; de Laat, M.; Lancé, M.M.D.; Kicken, C.H.; Pelkmans, L.; Bloemen, S.; Dirks, M.L.; van Loon, L.J.C.; Govers-Riemslag, J.W.P.; Lindhout, T.; et al. Hypoxia Induces a Prothrombotic State Independently of the Physical Activity. PLoS ONE 2015, 10, e0141797. [Google Scholar] [CrossRef]
- Malone, P.C.; Agutter, P.S. Deep venous thrombosis: The valve cusp hypoxia thesis and its incompatibility with modern orthodoxy. Med. Hypotheses 2016, 86, 60–66. [Google Scholar] [CrossRef]
- Goldhaber, S.Z.; Elliott, C.G. Acute Pulmonary Embolism: Part I: Epidemiology, Pathophysiology, and Diagnosis. Circulation 2003, 108, 2726–2729. [Google Scholar] [CrossRef]
- Subramanian, M.; Ramadurai, S.; Arthur, P.; Gopalan, S. Hypoxia as an independent predictor of adverse outcomes in pulmonary embolism. Asian Cardiovasc. Thorac. Ann. 2018, 26, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, Y.; Yamashita, A.; Iwakiri, T.; Sugita, C.; Okuyama, N.; Kitamura, K.; Asada, Y. Vascular wall hypoxia promotes arterial thrombus formation via augmentation of vascular thrombogenicity. Thromb. Haemost. 2015, 114, 158–172. [Google Scholar] [CrossRef]
- Jones, D.T.; Macdonald, J.H.; Sandoo, A.; Oliver, S.J.; Rossetti, G.M. The deleterious effects of acute hypoxia and large vessel endothelial function. Exp. Physiol. 2021, 106, 1699–1709. [Google Scholar] [CrossRef]
- Delaney, C.; Davizon-Castillo, P.; Allawzi, A.; Posey, J.; Gandjeva, A.; Neeves, K.; Tuder, R.M.; Di Paola, J.; Stenmark, K.R.; Nozik, E.S. Platelet activation contributes to hypoxia-induced inflammation. Am. J. Physiol. Lung Cell. Mol. Physiol. 2021, 320, L413–L421. [Google Scholar] [CrossRef]
- Bhagat, S.; Biswas, I.; Ahmed, R.; Khan, G.A. Hypoxia induced up-regulation of tissue factor is mediated through extracellular RNA activated Toll-like receptor 3-activated protein 1 signalling. Blood Cells. Mol. Dis. 2020, 84, 102459. [Google Scholar] [CrossRef]
- Ding, C.; Wang, R.; Gong, X.; Yuan, Y. Stroke risk of COPD patients and death risk of COPD patients following a stroke: A systematic review and meta-analysis. Medicine 2023, 102, e35502. [Google Scholar] [CrossRef] [PubMed]
- Conway, E.M.; Mackman, N.; Warren, R.Q.; Wolberg, A.S.; Mosnier, L.O.; Campbell, R.A.; Gralinski, L.E.; Rondina, M.T.; Van De Veerdonk, F.L.; Hoffmeister, K.M.; et al. Understanding COVID-19-associated coagulopathy. Nat. Rev. Immunol. 2022, 22, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Patolia, S.; Looby, M.; Bade, N.; Khangoora, V.; King, C.S. Association of D-dimer and Fibrinogen With Hypercoagulability in COVID-19 Requiring Extracorporeal Membrane Oxygenation. J. Intensive Care Med. 2021, 36, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Boukhenouna, S.; Wilson, M.A.; Bahmed, K.; Kosmider, B. Reactive Oxygen Species in Chronic Obstructive Pulmonary Disease. Oxid. Med. Cell. Longev. 2018, 2018, 5730395. [Google Scholar] [CrossRef]
- Xie, J.; Yuan, C.; Yang, S.; Ma, Z.; Li, W.; Mao, L.; Jiao, P.; Liu, W. The role of reactive oxygen species in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection-induced cell death. Cell. Mol. Biol. Lett. 2024, 29, 138. [Google Scholar] [CrossRef]
- Wang, H.; Song, T.-Y.; Reyes-García, J.; Wang, Y.-X. Hypoxia-Induced Mitochondrial ROS and Function in Pulmonary Arterial Endothelial Cells. Cells 2024, 13, 1807. [Google Scholar] [CrossRef]
- Afzal, S.; Abdul Manap, A.S.; Attiq, A.; Albokhadaim, I.; Kandeel, M.; Alhojaily, S.M. From imbalance to impairment: The central role of reactive oxygen species in oxidative stress-induced disorders and therapeutic exploration. Front. Pharmacol. 2023, 14, 1269581. [Google Scholar] [CrossRef]
- Janaszak-Jasiecka, A.; Siekierzycka, A.; Płoska, A.; Dobrucki, I.T.; Kalinowski, L. Endothelial Dysfunction Driven by Hypoxia-The Influence of Oxygen Deficiency on NO Bioavailability. Biomolecules 2021, 11, 982. [Google Scholar] [CrossRef]
- Yang, Q.; Chen, D.; Li, C.; Liu, R.; Wang, X. Mechanism of hypoxia-induced damage to the mechanical property in human erythrocytes-band 3 phosphorylation and sulfhydryl oxidation of membrane proteins. Front. Physiol. 2024, 15, 1399154. [Google Scholar] [CrossRef]
- Tariq, S.; Ismail, D.; Thapa, M.; Goriparthi, L.; Pradeep, R.; Khalid, K.; Cooper, A.C.; Jean-Charles, G. Chronic Obstructive Pulmonary Disease and Its Effect on Red Blood Cell Indices. Cureus 2023, 15, e36100. [Google Scholar] [CrossRef] [PubMed]
- Mullen, E.; Bergin, S.; Healy, G.; Quinn, J.; Glavey, S.; Murphy, P.T. Red blood cells from COVID-19 patients suffer from increased oxidative stress and may have increased lactate influx. Blood Res. 2022, 57, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Oxidative Stress in Chronic Obstructive Pulmonary Disease. Antioxidants 2022, 11, 965. [Google Scholar] [CrossRef]
- Finicelli, M.; Digilio, F.A.; Galderisi, U.; Peluso, G. The Emerging Role of Macrophages in Chronic Obstructive Pulmonary Disease: The Potential Impact of Oxidative Stress and Extracellular Vesicle on Macrophage Polarization and Function. Antioxidants 2022, 11, 464. [Google Scholar] [CrossRef]
- Georgieva, E.; Ananiev, J.; Yovchev, Y.; Arabadzhiev, G.; Abrashev, H.; Abrasheva, D.; Atanasov, V.; Kostandieva, R.; Mitev, M.; Petkova-Parlapanska, K.; et al. COVID-19 Complications: Oxidative Stress, Inflammation, and Mitochondrial and Endothelial Dysfunction. Int. J. Mol. Sci. 2023, 24, 14876. [Google Scholar] [CrossRef] [PubMed]
- Mallah, H.; Ball, S.; Sekhon, J.; Parmar, K.; Nugent, K. Platelets in chronic obstructive pulmonary disease: An update on pathophysiology and implications for antiplatelet therapy. Respir. Med. 2020, 171, 106098. [Google Scholar] [CrossRef]
- Yang, M. Redox stress in COVID-19: Implications for hematologic disorders. Best Pract. Res. Clin. Haematol. 2022, 35, 101373. [Google Scholar] [CrossRef]
- Jo, Y.S. Long-Term Outcome of Chronic Obstructive Pulmonary Disease: A Review. Tuberc. Respir. Dis. 2022, 85, 289–301. [Google Scholar] [CrossRef]
- El-Korashy, R.I.; Amin, Y.M.; Moussa, H.A.; Badawy, I.; Bakr, S.M. Study the relationship of erythropoietin and chronic obstructive pulmonary disease. Egypt. J. Chest Dis. Tuberc. 2012, 61, 53–57. [Google Scholar] [CrossRef]
- Soliz, J.; Schneider-Gasser, E.M.; Arias-Reyes, C.; Aliaga-Raduan, F.; Poma-Machicao, L.; Zubieta-Calleja, G.; Furuya, W.I.; Trevizan-Baú, P.; Dhingra, R.R.; Dutschmann, M. Coping with hypoxemia: Could erythropoietin (EPO) be an adjuvant treatment of COVID-19? Respir. Physiol. Neurobiol. 2020, 279, 103476. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Weissenborn, K.; Begemann, M.; Busch, M.; Vieta, E.; Miskowiak, K.W. Erythropoietin as candidate for supportive treatment of severe COVID-19. Mol. Med. 2020, 26, 58. [Google Scholar] [CrossRef]
- Thapa, K.B.; Paudel, A.; Dhital, S.; Shrestha, A.; Ojha, L.; Shrestha, A. Polycythemia among Patients with Chronic Obstructive Pulmonary Disease Admitted to the Department of Medicine in a Tertiary Care Center: A Descriptive Cross-sectional Study. JNMA J. Nepal Med. Assoc. 2023, 61, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Ayako, R.M.; Patel, K.; Ndede, I.; Nordgren, J.; Larrson, M.; Mining, S.K. Inflammatory, Hematological, and Biochemical Biomarkers in COVID-19 Patients. Immun. Inflamm. Dis. 2024, 12, e70078. [Google Scholar] [CrossRef] [PubMed]
- Deng, R.; Ma, X.; Zhang, H.; Chen, J.; Liu, M.; Chen, L.; Xu, H. Role of HIF-1α in hypercoagulable state of COPD in rats. Arch. Biochem. Biophys. 2024, 753, 109903. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Liu, W.; Li, X.; Zhao, P.; Shereen, M.A.; Zhu, C.; Huang, S.; Liu, S.; Yu, X.; Yue, M.; et al. HIF-1α promotes SARS-CoV-2 infection and aggravates inflammatory responses to COVID-19. Signal Transduct. Target. Ther. 2021, 6, 308. [Google Scholar] [CrossRef]
- Moulaeian, M.; Ferdousmakan, S.; Banihashemi, S.; Homayounfar, S.; Pasupulla, A.P.; Malekzadegan, Y. Reactive oxygen species induced by SARS-CoV-2 infection can induce EMT in solid tumors: Potential role of COVID-19 in chemo-resistance and metastasis. Heliyon 2024, 10, e40297. [Google Scholar] [CrossRef]
- Voskresenska, N.; Voicehovska, J.; Vojcehovska, A.; Orlikovs, G.; Skesters, A. Malondialdehyde level in chronic obstructive pulmonary disease exacerbations. In 52 Monitoring Airway Disease; European Respiratory Society: Lausanne, Switzerland, 2015; p. OA2920. [Google Scholar]
- Mehri, F.; Rahbar, A.H.; Ghane, E.T.; Souri, B.; Esfahani, M. Changes in oxidative markers in COVID-19 patients. Arch. Med. Res. 2021, 52, 843–849. [Google Scholar] [CrossRef]
- Bowler, R.P.; Hokanson, J.; Taylor, M.; Levy, S.; Canaham, E.M.; Regan, E.; Wheeler, C.; Nicks, M.; Chan, E.; Crapo, J.D. Extracellular superoxide dismutase (EC-SOD) as a protective factor for risk of chronic obstructive pulmonary disease. Eur. Respir. Rev. 2006, 15, 200–201. [Google Scholar] [CrossRef]
- Chu, J.; Hua, L.; Liu, X.; Xiong, H.; Jiang, F.; Zhou, W.; Wang, L.; Xue, G. Superoxide dismutase alterations in COVID-19: Implications for disease severity and mortality prediction in the context of omicron variant infection. Front. Immunol. 2024, 15, 1362102. [Google Scholar] [CrossRef]
- Silvagno, F.; Vernone, A.; Pescarmona, G.P. The Role of Glutathione in Protecting against the Severe Inflammatory Response Triggered by COVID-19. Antioxidants 2020, 9, 624. [Google Scholar] [CrossRef]
- Guloyan, V.; Oganesian, B.; Baghdasaryan, N.; Yeh, C.; Singh, M.; Guilford, F.; Ting, Y.-S.; Venketaraman, V. Glutathione Supplementation as an Adjunctive Therapy in COVID-19. Antioxidants 2020, 9, 914. [Google Scholar] [CrossRef] [PubMed]
- Satała, J.; Woźniak, A.; Fabiś, M.; Gorzelak-Pabiś, P.; Pawlos, A.; Fabiś, J.; Broncel, M.; Woźniak, E. Severe COVID-19 classified by simple covid risk index is associated with higher levels of advanced oxidation protein products and 8-hydroxy 2 deoxyguanosine. Epidemiol. Infect. 2023, 151, e140. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; González-Rivero, A.F.; Pérez-Cejas, A.; Cáceres, J.J.; Perez, A.; Ramos-Gómez, L.; Solé-Violán, J.; Ramos, J.A.M.Y.; Ojeda, N.; et al. DNA and RNA Oxidative Damage and Mortality of Patients With COVID-19. Am. J. Med. Sci. 2021, 361, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, J.; Janson, C.; Bröms, K.; Hårdstedt, M.; Högman, M.; Lisspers, K.; Palm, A.; Ställberg, B.; Malinovschi, A. CRP, Fibrinogen, White Blood Cells, and Blood Cell Indices as Prognostic Biomarkers of Future COPD Exacerbation Frequency: The TIE Cohort Study. J. Clin. Med. 2024, 13, 3855. [Google Scholar] [CrossRef]
- Rahaghi, F.N.; Pistenmaa, C.L. Hypercoagulation in COPD: The clot thickens. ERJ Open Res. 2021, 7, 00534–02021. [Google Scholar] [CrossRef]
- Higham, A.; Mathioudakis, A.; Vestbo, J.; Singh, D. COVID-19 and COPD: A narrative review of the basic science and clinical outcomes. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2020, 29, 200199. [Google Scholar] [CrossRef]
- Hilda, F.; Liana, P.; Nurtjahyo, A.; Hudari, H.; Sari, N.P.; Umar, T.P.; Amin, C.A.; Afifah, A.R. D-Dimer as a Sensitive Biomarker of Survival Rate in Patients with COVID-19. Eurasian J. Med. 2022, 54, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Hafez, W.; Nasa, P.; Khairy, A.; Jose, M.; Abdelshakour, M.; Ahmed, S.; Abdulaal, F.; Nair, N.; Ahmad, M.; Rashid, V.J.; et al. Interleukin-6 and the determinants of severe COVID-19: A retrospective cohort study. Medicine 2023, 102, e36037. [Google Scholar] [CrossRef]
- Shekhawat, J.; Gauba, K.; Gupta, S.; Purohit, P.; Mitra, P.; Garg, M.; Misra, S.; Sharma, P.; Banerjee, M. Interleukin-6 Perpetrator of the COVID-19 Cytokine Storm. Indian J. Clin. Biochem. IJCB 2021, 36, 440–450. [Google Scholar] [CrossRef]
- Lodge, K.M.; Vassallo, A.; Liu, B.; Long, M.; Tong, Z.; Newby, P.R.; Agha-Jaffar, D.; Paschalaki, K.; Green, C.E.; Belchamber, K.B.R.; et al. Hypoxia Increases the Potential for Neutrophil-mediated Endothelial Damage in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2022, 205, 903–916. [Google Scholar] [CrossRef]
- Teo, A.; Chan, L.L.Y.; Cheung, C.; Chia, P.Y.; Ong, S.W.X.; Fong, S.W.; Ng, L.F.P.; Renia, L.; Lye, D.C.; Young, B.E.; et al. Myeloperoxidase inhibition may protect against endothelial glycocalyx shedding induced by COVID-19 plasma. Commun. Med. 2023, 3, 62. [Google Scholar] [CrossRef] [PubMed]
- Awatade, N.T.; Wark, P.A.B.; Chan, A.S.L.; Mamun, S.M.A.A.; Mohd Esa, N.Y.; Matsunaga, K.; Rhee, C.K.; Hansbro, P.M.; Sohal, S.S.; On Behalf of The Asian Pacific Society of Respirology Apsr Copd Assembly. The Complex Association between COPD and COVID-19. J. Clin. Med. 2023, 12, 3791. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Pothast, C.R.; Dijkland, R.C.; Thaler, M.; Hagedoorn, R.S.; Kester, M.G.D.; Wouters, A.K.; Hiemstra, P.S.; van Hemert, M.J.; Gras, S.; Falkenburg, J.H.F.; et al. SARS-CoV-2-specific CD4+ and CD8+ T cell responses can originate from cross-reactive CMV-specific T cells. eLife 2022, 11, e82050. [Google Scholar] [CrossRef]
- Kervevan, J.; Chakrabarti, L.A. Role of CD4+ T Cells in the Control of Viral Infections: Recent Advances and Open Questions. Int. J. Mol. Sci. 2021, 22, 523. [Google Scholar] [CrossRef]
- Sun, Y.; Luo, B.; Liu, Y.; Wu, Y.; Chen, Y. Immune damage mechanisms of COVID-19 and novel strategies in prevention and control of epidemic. Front. Immunol. 2023, 14, 1130398. [Google Scholar] [CrossRef]
- Lian, J.; Jin, C.; Hao, S.; Zhang, X.; Yang, M.; Jin, X.; Lu, Y.; Hu, J.; Zhang, S.; Zheng, L.; et al. High neutrophil-to-lymphocyte ratio associated with progression to critical illness in older patients with COVID-19: A multicenter retrospective study. Aging 2020, 12, 13849–13859. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Negri, S.; Carru, C.; Zinellu, A. Neutrophil to lymphocyte ratio and clinical outcomes in COPD: Recent evidence and future perspectives. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2018, 27, 170113. [Google Scholar] [CrossRef]
- Grobler, C.; Maphumulo, S.C.; Grobbelaar, L.M.; Bredenkamp, J.C.; Laubscher, G.J.; Lourens, P.J.; Steenkamp, J.; Kell, D.B.; Pretorius, E. COVID-19: The Rollercoaster of Fibrin(Ogen), D-Dimer, Von Willebrand Factor, P-Selectin and Their Interactions with Endothelial Cells, Platelets and Erythrocytes. Int. J. Mol. Sci. 2020, 21, 5168. [Google Scholar] [CrossRef]
- Singh, D.; Mathioudakis, A.G.; Higham, A. Chronic obstructive pulmonary disease and COVID-19: Interrelationships. Curr. Opin. Pulm. Med. 2022, 28, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef] [PubMed]
- Alisamir, M.; Ebrahimi, M.; Rahim, F. Anemia in chronic obstructive pulmonary disease: A systematic review. Respir. Investig. 2022, 60, 510–521. [Google Scholar] [CrossRef]
- Tao, Z.; Xu, J.; Chen, W.; Yang, Z.; Xu, X.; Liu, L.; Chen, R.; Xie, J.; Liu, M.; Wu, J.; et al. Anemia is associated with severe illness in COVID-19: A retrospective cohort study. J. Med. Virol. 2021, 93, 1478–1488. [Google Scholar] [CrossRef]
- Benoit, J.L.; Benoit, S.W.; de Oliveira, M.H.S.; Lippi, G.; Henry, B.M. Anemia and COVID-19: A prospective perspective. J. Med. Virol. 2021, 93, 708–711. [Google Scholar] [CrossRef] [PubMed]
- Wessling-Resnick, M. Iron homeostasis and the inflammatory response. Annu. Rev. Nutr. 2010, 30, 105–122. [Google Scholar] [CrossRef]
- Mendonça, M.M.; da Cruz, K.R.; Pinheiro, D.d.S.; Moraes, G.C.A.; Ferreira, P.M.; Ferreira-Neto, M.L.; da Silva, E.S.; Gonçalves, R.V.; Pedrino, G.R.; Fajemiroye, J.O.; et al. Dysregulation in erythrocyte dynamics caused by SARS-CoV-2 infection: Possible role in shuffling the homeostatic puzzle during COVID-19. Hematol. Transfus. Cell Ther. 2022, 44, 235–245. [Google Scholar] [CrossRef]
- Kent, B.D.; Mitchell, P.D.; McNicholas, W.T. Hypoxemia in patients with COPD: Cause, effects, and disease progression. Int. J. Chronic Obstr. Pulm. Dis. 2011, 6, 199–208. [Google Scholar]
- Cavezzi, A.; Troiani, E.; Corrao, S. COVID-19: Hemoglobin, Iron, and Hypoxia beyond Inflammation. A Narrative Review. Clin. Pract. 2020, 10, 1271. [Google Scholar] [CrossRef]
- Hardang, I.M.; Søyseth, V.; Kononova, N.; Hagve, T.-A.; Einvik, G. COPD: Iron Deficiency and Clinical Characteristics in Patients With and Without Chronic Respiratory Failure. Chronic Obstr. Pulm. Dis. J. COPD Found. 2024, 11, 261–269. [Google Scholar] [CrossRef]
- Şan, İ.; Gemcioğlu, E.; Davutoğlu, M.; Çatalbaş, R.; Karabuğa, B.; Kaptan, E.; Erden, A.; Küçükşahin, O.; Ateş, İ.; Karaahmetoğlu, S.; et al. Which hematological markers have predictive value as early indicators of severe COVID-19 cases in the emergency department? Turk. J. Med. Sci. 2021, 51, 2810–2821. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Sui, J.; Noubouossie, D.F.; Gandotra, S.; Cao, L. Elevated Plasma Fibrinogen Is Associated With Excessive Inflammation and Disease Severity in COVID-19 Patients. Front. Cell. Infect. Microbiol. 2021, 11, 734005. [Google Scholar] [CrossRef]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.M.; Bory, O.M.; Diehl, J.-L.; Mareau, A.; Gendron, N.; Jannot, A.-S.; Chocron, R. Daily Monitoring of D-Dimer Allows Outcomes Prediction in COVID-19. TH Open 2022, 06, e21–e25. [Google Scholar] [CrossRef]
- Patil, S.; Khule, S.; Toshniwal, S. Role of D-Dimer in assessing severity, monitoring, and predicating outcome in COVID-19 pneumonia: A single center study. Glob. J. Health Sci. Res. 2023, 1, 31–37. [Google Scholar] [CrossRef]
- Beidollahkhani, S.; Fayedeh, F.; Shoja, A.; Hassan Nejad, E.; Hoseinpour, M.; Fazlpour, F.; Payandeh, A.; Pezeshki Rad, M.; Moodi Ghalibaf, A. d-dimer as a biomarker for COVID-19-associated pulmonary thromboembolism: A narrative review from molecular pathways to the imaging findings. Egypt. J. Bronchol. 2023, 17, 44. [Google Scholar] [CrossRef]
- Kornblith, L.Z.; Sadhanandhan, B.; Arun, S.; Long, R.; Johnson, A.J.; Noll, J.; Ramchand, C.N.; Olynyk, J.K.; Farrell, D.H. γ′ fibrinogen levels as a biomarker of COVID-19 respiratory disease severity. Blood Cells. Mol. Dis. 2023, 101, 102746. [Google Scholar] [CrossRef]
- Long, W.; Yang, J.; Li, Z.; Li, J.; Chen, S.; Chen, D.; Wang, S.; Li, Q.; Hu, D.; Huang, J.; et al. Abnormal Fibrinogen Level as a Prognostic Indicator in Coronavirus Disease Patients: A Retrospective Cohort Study. Front. Med. 2021, 8, 687220. [Google Scholar] [CrossRef]
- Toori, K.U.; Qureshi, M.A.; Chaudhry, A.; Safdar, M.F. Neutrophil to lymphocyte ratio (NLR) in COVID-19: A cheap prognostic marker in a resource constraint setting. Pak. J. Med. Sci. 2021, 37, 1435–1439. [Google Scholar] [CrossRef]
- Ribeiro Carvalho, C.R.; Lamas, C.D.A.; Visani De Luna, L.A.; Chate, R.C.; Salge, J.M.; Yamada Sawamura, M.V.; Toufen, C.; Garcia, M.L.; Scudeller, P.G.; Nomura, C.H.; et al. Post-COVID-19 respiratory sequelae two years after hospitalization: An ambidirectional study. Lancet Reg. Health-Am. 2024, 33, 100733. [Google Scholar] [CrossRef] [PubMed]
- Asperges, E.; Albi, G.; Zuccaro, V.; Sambo, M.; Pieri, T.C.; Calia, M.; Colaneri, M.; Maiocchi, L.; Melazzini, F.; Lasagna, A.; et al. Dynamic NLR and PLR in Predicting COVID-19 Severity: A Retrospective Cohort Study. Infect. Dis. Ther. 2023, 12, 1625–1640. [Google Scholar] [CrossRef] [PubMed]
- Gemicioglu, B.; Uzun, H.; Borekci, S.; Karaali, R.; Kurugoglu, S.; Atukeren, P.; Sirolu, S.; Durmus, S.; Dirican, A.; Kuskucu, M.A.; et al. Focusing on Asthma and Chronic Obstructive Pulmonary Disease with COVID-19. J. Infect. Dev. Ctries. 2021, 15, 1415–1425. [Google Scholar] [CrossRef]
- Labbé, V.; Contou, D.; Heming, N.; Megarbane, B.; Razazi, K.; Boissier, F.; Ait-Oufella, H.; Turpin, M.; Carreira, S.; Robert, A.; et al. Effects of Standard-Dose Prophylactic, High-Dose Prophylactic, and Therapeutic Anticoagulation in Patients With Hypoxemic COVID-19 Pneumonia: The ANTICOVID Randomized Clinical Trial. JAMA Intern. Med. 2023, 183, 520. [Google Scholar] [CrossRef]
- Kaptein, F.H.J.; Stals, M.a.M.; Huisman, M.V.; Klok, F.A. Prophylaxis and treatment of COVID-19 related venous thromboembolism. Postgrad. Med. 2021, 133 (Suppl. S1), 27–35. [Google Scholar] [CrossRef] [PubMed]
- Pereyra, D.; Heber, S.; Schrottmaier, W.C.; Santol, J.; Pirabe, A.; Schmuckenschlager, A.; Kammerer, K.; Ammon, D.; Sorz, T.; Fritsch, F.; et al. Low-molecular-weight heparin use in coronavirus disease 2019 is associated with curtailed viral persistence: A retrospective multicentre observational study. Cardiovasc. Res. 2021, 117, 2807–2820. [Google Scholar] [CrossRef]
- Roguljić, H.; Arambašić, J.; Ninčević, V.; Kuna, L.; Šesto, I.; Tabll, A.; Smolić, R.; Včev, A.; Primorac, D.; Wu, G.Y.; et al. The role of direct oral anticoagulants in the era of COVID-19: Are antiviral therapy and pharmacogenetics limiting factors? Croat. Med. J. 2022, 63, 287–294. [Google Scholar] [CrossRef]
- Batra, G.; Modica, A.; Renlund, H.; Larsson, A.; Christersson, C.; Held, C. Oral anticoagulants, time in therapeutic range and renal function over time in real-life patients with atrial fibrillation and chronic kidney disease. Open Heart 2022, 9, e002043. [Google Scholar] [CrossRef]
- Lai, J.; Feng, S.; Xu, S.; Liu, X. Effects of oral anticoagulant therapy in patients with pulmonary diseases. Front. Cardiovasc. Med. 2022, 9, 987652. [Google Scholar] [CrossRef]
- Aursulesei, V.; Costache, I.I. Anticoagulation in chronic kidney disease: From guidelines to clinical practice. Clin. Cardiol. 2019, 42, 774–782. [Google Scholar] [CrossRef]
- Ballestri, S.; Romagnoli, E.; Arioli, D.; Coluccio, V.; Marrazzo, A.; Athanasiou, A.; Di Girolamo, M.; Cappi, C.; Marietta, M.; Capitelli, M. Risk and Management of Bleeding Complications with Direct Oral Anticoagulants in Patients with Atrial Fibrillation and Venous Thromboembolism: A Narrative Review. Adv. Ther. 2023, 40, 41–66. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.Y.; Ward, S.M. The Anti-Factor Xa Range For Low Molecular Weight Heparin Thromboprophylaxis. Hematol. Rep. 2015, 7, 5844. [Google Scholar] [CrossRef]
- Alsagaff, M.Y.; Mulia, E.P.B.; Maghfirah, I.; Azmi, Y.; Rachmi, D.A.; Yutha, A.; Andira, L.H.; Semedi, B.P. Low molecular weight heparin is associated with better outcomes than unfractionated heparin for thromboprophylaxis in hospitalized COVID-19 patients: A meta-analysis. Eur. Heart J.-Qual. Care Clin. Outcomes 2022, 8, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Wumaier, K.; Li, W.; Chen, N.; Cui, J. Direct oral anticoagulants versus low molecular weight heparins for the treatment of cancer-associated thrombosis: A cost-effectiveness analysis. Thromb. J. 2021, 19, 68. [Google Scholar] [CrossRef] [PubMed]
- Kustos, S.; Fasinu, P. Direct-Acting Oral Anticoagulants and Their Reversal Agents—An Update. Medicines 2019, 6, 103. [Google Scholar] [CrossRef]
- Lutz, J.; Jurk, K.; Schinzel, H. Direct oral anticoagulants in patients with chronic kidney disease: Patient selection and special considerations. Int. J. Nephrol. Renov. Dis. 2017, 10, 135–143. [Google Scholar] [CrossRef]
- Olie, R.H.; Winckers, K.; Rocca, B.; Ten Cate, H. Oral Anticoagulants Beyond Warfarin. Annu. Rev. Pharmacol. Toxicol. 2024, 64, 551–575. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, A.; Tirpude, N.V.; Sharma, S.; Padwad, Y.S.; Kumar, S. Pharmaco-immunomodulatory interventions for averting cytokine storm-linked disease severity in SARS-CoV-2 infection. Inflammopharmacology 2022, 30, 23–49. [Google Scholar] [CrossRef]
- van Paassen, J.; Vos, J.S.; Hoekstra, E.M.; Neumann, K.M.I.; Boot, P.C.; Arbous, S.M. Corticosteroid use in COVID-19 patients: A systematic review and meta-analysis on clinical outcomes. Crit. Care 2020, 24, 696. [Google Scholar] [CrossRef]
- Singanayagam, A.; Glanville, N.; Girkin, J.L.; Ching, Y.M.; Marcellini, A.; Porter, J.D.; Toussaint, M.; Walton, R.P.; Finney, L.J.; Aniscenko, J.; et al. Corticosteroid suppression of antiviral immunity increases bacterial loads and mucus production in COPD exacerbations. Nat. Commun. 2018, 9, 2229. [Google Scholar] [CrossRef]
- Ohadian Moghadam, S. A Review on Currently Available Potential Therapeutic Options for COVID-19. Int. J. Gen. Med. 2020, 13, 443–467. [Google Scholar] [CrossRef] [PubMed]
- Balta, M.G.; Papathanasiou, E.; Christopoulos, P.F. Specialized Pro-Resolving Mediators as Potential Regulators of Inflammatory Macrophage Responses in COVID-19. Front. Immunol. 2021, 12, 632238. [Google Scholar] [CrossRef] [PubMed]
- Bahsoun, A.; Fakih, Y.; Zareef, R.; Bitar, F.; Arabi, M. Corticosteroids in COVID-19: Pros and cons. Front. Med. 2023, 10, 1202504. [Google Scholar] [CrossRef]
- Abidi, E.; El Nekidy, W.S.; Alefishat, E.; Rahman, N.; Petroianu, G.A.; El-Lababidi, R.; Mallat, J. Tocilizumab and COVID-19: Timing of Administration and Efficacy. Front. Pharmacol. 2022, 13, 825749. [Google Scholar] [CrossRef]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, L.; Scherger, S.; Franco-Paredes, C.; Gharamti, A.; Henao-Martinez, A.F. Anakinra authorized to treat severe coronavirus disease 2019; Sepsis breakthrough or time to reflect? Front. Microbiol. 2023, 14, 1250483. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Akinosoglou, K.; Florou, E.; Kouriannidi, E.; Bogosian, A.; Tsachouridou, O.; Syrigos, K.N.; Gatselis, N.; Milionis, H.; Papanikolaou, I.C.; et al. Anakinra efficacy in COVID-19 pneumonia guided by soluble urokinase plasminogen activator receptor: Association with the inflammatory burden of the host. Int. J. Antimicrob. Agents 2025, 65, 107405. [Google Scholar] [CrossRef]
- Cioboata, R.; Nicolosu, D.; Streba, C.T.; Vasile, C.M.; Olteanu, M.; Nemes, A.; Gheorghe, A.; Calarasu, C.; Turcu, A.A. Post-COVID-19 Syndrome Based on Disease Form and Associated Comorbidities. Diagnostics 2022, 12, 2502. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).