Abstract
Background/Objectives: Patients with periodontitis have been found to have higher salivary concentrations of malondialdehyde, a biomarker of lipid hyperoxidation, compared to healthy subjects. However, the association between salivary malondialdehyde levels and periodontitis, independently of other risk factors, has not been analyzed. Therefore, the novel objective of our study was to explore this possible association by performing a logistic regression analysis. Material and Methods: This observational, prospective study was carried out in a private dental practice. Salivary malondialdehyde levels were measured in subjects with periodontitis (characterized by periodontal tissue loss) and in subjects without periodontitis (either periodontally healthy or with localized gingivitis in <30% of sites). A multivariate regression analysis was carried out to determine the factors associated with periodontitis. Variables with a p-value ≤ 0.05 in the comparison between subjects with and without periodontitis were included in the regression analysis. Results: A total of 119 subjects were included, 63 with periodontitis and 56 without (35 periodontally healthy subjects and 21 patients with localized gingivitis). In the multiple binomial regression analysis, salivary malondialdehyde levels > 0.77 nmol/mL were identified as a predictor of periodontitis (p = 0.03), after controlling for age (p < 0.001), diabetes mellitus (p = 0.81), arterial hypertension (p = 0.43), smoking status (never smoked p = 0.08), and cardiovascular disease (p = 0.88). Conclusions: To our knowledge, this is the first study to report that salivary malondialdehyde levels are associated with periodontitis, independently of other known risk factors.
1. Introduction
Periodontitis, a chronic inflammatory disease of the periodontium, represents a significant public health problem due to its widespread global prevalence and economic impact [1,2,3,4]. In periodontitis, different pathophysiological pathways are activated, such as inflammation [2,3,4], oxidation [5,6,7], and programmed cell death [8].
The clinical diagnosis of periodontitis can be interfered with by certain factors such as the pressure applied with the periodontal probe in the crevice, limited mouth openings, and discomfort during the examination [2].
Thus, some salivary biomarkers have been suggested that could help in the diagnosis of periodontitis and the classification of periodontitis severity [2,3,4], although they are not being used in clinical practice. In this respect, different biomarkers in saliva have been found in higher concentrations in patients with periodontitis than in healthy subjects as interleukin (IL)-1β, S100A8, S100A9, S100A12, matrix metalloproteinase (MMP)-8, and hepatocyte growth factor (HGF), colony-stimulating factor-1 (CSF-1) [2], interleukin (IL)-6, tumor necrosis factor-alpha (TNF-alpha), osteoprotegerin [3], and prostaglandin E2 (PGE2) [4], malondialdehyde (MDA), nitric oxide (NO), total oxidant status (TOS), and 8-hydroxy-deoxyguanosine [5].
The increased production of reactive oxygen species (ROS) can induce multiple adverse effects, such as lipid, protein, and nucleic acid oxidation [5,6,7] as well as the activation of programmed cell death [5,6,7]. Periodontal inflammation is associated with high levels of malondialdehyde (a biomarker of lipid hyperoxidation) in saliva.
Malondialdehyde is an end-product that appears during lipid peroxidation, specifically due to phospholipid degradation of the cellular membrane. Due to the action of phospholipase-A2, arachidonic acid is produced. Afterwards, arachidonic acid is attacked by mitochondrial ROS (mainly by hydroxyl radical), forming lipid endoperoxide. Subsequently, due to the spontaneous rupture of lipid endoperoxide, malondialdehyde in the intracellular space is formed. Finally, malondialdehyde is released into the extracellular space and will appear in blood and saliva [6].
A meta-analysis published by Chen et al. in 2019, which included 14 articles and 931 subjects (474 with and 457 without periodontitis), reported higher salivary concentrations of malondialdehyde in subjects with periodontitis than in periodontally healthy subjects in the bivariate analysis [5]. In the meta-analysis published by Mohideen et al. in 2023, which included 10 articles and 763 subjects (393 with and 370 without periodontitis), higher salivary concentrations of malondialdehyde in subjects with periodontitis were reported than in healthy subjects in the bivariate analysis [6]. Those 10 articles and 763 subjects were also included in the meta-analysis published by Chen et al. In 2019 [5]. In addition, no new studies were included in the meta-analysis by Mohideen et al. with respect to the meta-analysis by Chen et al. [5]. In addition, some studies have found an association between malondialdehyde salivary levels and periodontitis severity [9,10,11,12].
Different risk factors have been associated with the development of periodontitis, such as age [13], sex [14], obesity [15], diabetes mellitus [16], systemic lupus erythematosus and rheumatoid arthritis [17], arterial hypertension [18], dental hygiene, consumption of tobacco and alcohol, immunosuppression and oral cancer [19].
However, the potential association of salivary malondialdehyde levels and periodontitis, independent of other risk factors, has not been analyzed. We hypothesize that there is an association between salivary malondialdehyde levels and periodontitis regardless of other risk factors. Therefore, the main and novel objective of our study was to explore this possible association by performing a logistic regression analysis.
As the clinical diagnosis of periodontitis can be interfered with by some factors [2], the use of salivary biomarkers could help in the diagnosis of periodontitis [2,3,4]. Therefore, one secondary objective of this study was to explore the potential role of salivary malondialdehyde levels in the diagnosis of periodontitis, performing a receiver operating characteristic (ROC) analysis.
2. Methods
2.1. Design and Subjects
The Clinical Research Ethics Committee of the Hospital Universitario de Canarias approved the study protocol (CHUC_2023_138). Informed consent was obtained from each subject prior to inclusion in this study.
This prospective and observational study was developed at Clínica Dental Cándido in La Laguna, Tenerife, Spain. This study included subjects with periodontitis (loss of periodontal tissue) and subjects without periodontitis (periodontal health or localized gingivitis in <30% of sites). We used current internationally accepted criteria for the definitions of periodontal health, gingivitis, and periodontitis, and for the classification of periodontitis severity [20]. Subjects younger than 18 years and lactating females were excluded.
2.2. Definitions
Clinical periodontal health was defined as the absence of bleeding on probing or its presence in less than 10% of sites, along with the absence of clinical interproximal attachment loss and bone loss due to periodontitis.
Localized gingivitis was defined as the presence of bleeding in 10–30% of sites, with the absence of clinical interproximal attachment loss and bone loss due to periodontitis.
Periodontitis was defined as the bone loss or clinical interproximal attachment loss. In some cases, tooth loss may have occurred due to periodontitis. The severity of periodontitis was determined based on the following criteria: (1) Clinical interproximal attachment loss: Stage I <3 mm, Stage II 3–4 mm, Stage III or IV ≥5 mm. (2) Radiographic bone loss: Stage I when was coronal third (<15%), Stage II when affecting 15–33%), Stage III or IV when there was extension to the middle or apical third of the root. (3) Tooth loss: Stage I or II when none was, Stage III when ≤4 teeth were lost, Stage IV when ≥5 teeth were lost.
We used periodontal probes PCP 12 of Hu Friedy (Chicago, IL, USA). All the teeth of each subject were probed in 6 surfaces: mesial, central, and distal, both on the vestibular (external) and lingual (internal) surfaces. We used orthopantomography to make a radiological diagnosis.
2.3. Variables Recorded
The following variables were recorded: age, sex, diabetes mellitus, arterial hypertension, cardiovascular disease, hypercholesterolemia, oral cancer, consumption of tobacco, coffee, tea, alcohol and drugs, dental hygiene, body mass index (BMI) (kg/m2), obesity (BMI ≥ 30 kg/m2), immunosuppressive therapy, radiotherapy, chemotherapy, methotrexate, loss of clinical interproximal attachment, radiographic bone loss and tooth loss due to periodontitis.
Samples of unstimulated whole saliva were collected using the technique described by Navazesh [21]. Samples were taken in the morning from 8 to 10 a.m. to avoid possible influences of the circadian rhythm on the concentrations of biomarkers in saliva. Subjects were instructed to fast overnight and refrain from smoking, drinking, or brushing their teeth for 2 h before the session. They rinsed their mouths thoroughly 3 times with 10 mL of deionized water. They were then seated comfortably with their eyes open, heads tilted slightly forward, and rested for 30 min, trying to minimize orofacial movements. Saliva was allowed to accumulate on the floor of the mouth and was collected into a container over a 30 min period, without swallowing. The collected samples were then centrifuged at 3000 rpm for 10 min at 24 °C to remove debris and cells. The supernatant was then pipetted into Eppendorf tubes and stored immediately in a freezer at −80 °C until the analytical determinations were performed.
Some subjects included in this study were previously part of other publications by our research team in which salivary levels of nitrites [22] and uric acid [23] were determined. In the current study, salivary malondialdehyde levels were determined.
2.4. Salivary Malondialdehyde Level Analysis
Salivary malondialdehyde levels were measured using the thiobarbituric acid-reactive substance (TBARS) method described by Kikugawa et al. [24]. To minimize potential interferences, we used the methods described by Hodges et al. [25] and Valenzuela [26]. The samples were run in duplicate. The internal positive control was authentic malondialdehyde as standard (Merck-Millipore Sigma, Madrid, Spain). Each assay included 10 malondialdehyde standards. The assay had a detection limit of 0.079 nmol/mL, an intra-assay coefficient of variation of 1.82%, and an inter-assay coefficient of variation of 4.01%. Salivary malondialdehyde concentrations were expressed in nmol/mL.
2.5. Statistical Methods
Statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA) and LogXact 4.0 (Cytel Software Corporation, Cambridge, MA, USA). Kruskal–Wallis test was used to determine whether there was a possible difference in salivary malondialdehyde concentrations between subject groups.
The comparison between subject groups in categorical variables was carried out using the Chi-square test, while continuous variables were analyzed using the Mann–Whitney U-test. The potential association between salivary malondialdehyde levels and periodontitis severity was evaluated using Spearman’s rho correlation coefficient.
Receiver operating characteristic (ROC) analyses were carried out using the diagnosis of periodontitis and salivary malondialdehyde levels. Sensitivity, specificity, positive and negative likelihood ratios, positive and negative predictive values, and their 95% confidence interval (CI) were reported for the salivary malondialdehyde threshold > 0.77 nmol/mL, selected based on the Youden J index [27].
Multiple binomial logistic regression was used to estimate the association between salivary malondialdehyde levels > 0.77 nmol/mL and periodontitis, adjusting for age, arterial hypertension, and smoking status (never smoked). Variables with a p-value ≤ 0.05 in the comparison between subjects with and without periodontitis were included in the regression analysis.
3. Results
A total of 119 subjects were included, 63 with periodontitis and 56 without (35 periodontally healthy subjects and 21 patients with local gingivitis). Table 1 shows the description of periodontal status and salivary malondialdehyde levels for each periodontal state group.

Table 1.
Description of periodontal state in all subjects of this study.
Patients with periodontitis compared to subjects without periodontitis had a higher prevalence of arterial hypertension (p = 0.001), a higher proportion of never having smoked (p < 0.001), higher malondialdehyde salivary levels (p < 0.001), and were older (p < 0.001). In our cohort, there were no subjects with oral cancer, chemotherapy, drug consumption, or lack of dental hygiene (toothbrushing). There were no significant differences between subjects with and without periodontitis in sex, personal history of diabetes mellitus, cardiovascular disease, hypercholesterolemia, rheumatoid arthritis, systemic lupus erythematosus, immunosuppressive therapy, radiotherapy, methotrexate, body mass index, obesity, or consumption of coffee, tea, or alcohol (Table 2).
Table 2.
Comparisons between subjects with and without periodontitis.
We have found a positive association between salivary malondialdehyde levels and age (rho = 0.27; p = 0.004). However, we have not found significant differences in salivary malondialdehyde levels according to sex (p = 0.96), diabetes mellitus (p = 0.21), arterial hypertension (p = 0.61), rheumatoid arthritis (p = 0.38), systemic lupus erythematosus (p = 0.20), cardiovascular disease (p = 0.95), hypercholesterolemia (p = 0.55), coffee (p = 0.57), never smoker (p = 0.90), tea (p = 0.06), alcohol (p = 0.31), obesity (p = 0.97), immunosuppressive therapy (p = 0.54), radiotherapy (p = 0.43) or methotrexate (p = 0.15).
A significant association was found between salivary malondialdehyde levels and the severity of periodontitis (rho = 0.40; p < 0.001).
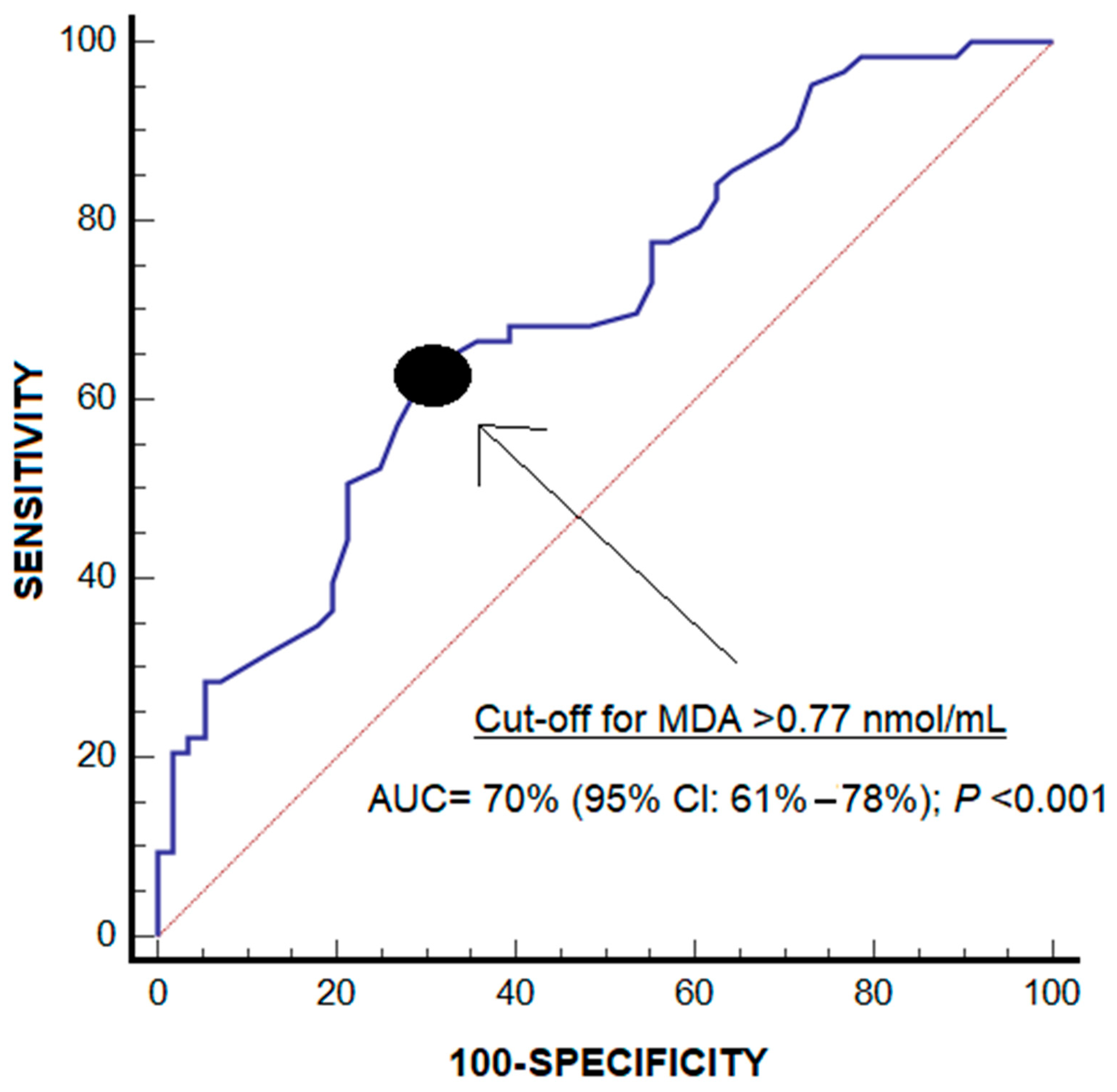
The area under the curve for the diagnosis of periodontitis by salivary malondialdehyde levels was 70% (95% CI = 61–78%; p < 0.001) (Figure 1). The malondialdehyde levels > 0.77 nmol/mL showed a sensitivity of 63% (50–75%), a specificity of 70% (56–81%), a positive likelihood ratio of 2.1 (1.4–3.2), a negative likelihood ratio of 0.5 (0.4–0.8), a positive predictive value of 70% (60–79%) and a negative predictive value of 63% (54–71%) for the diagnosis of periodontitis.
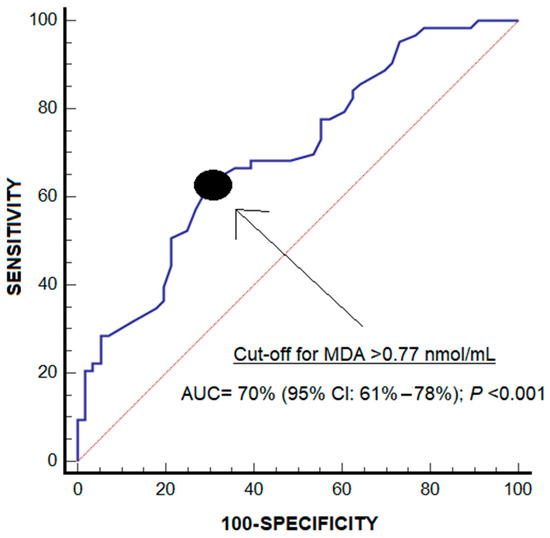
Figure 1.
Receiver operating characteristic analysis using malondialdehyde salivary levels for diagnosis of periodontitis.
In the multiple logistic regression analysis, salivary malondialdehyde levels > 0.77 nmol/mL were associated with periodontitis (p = 0.03), controlling for age, arterial hypertension, and never smoking (Table 3).
Table 3.
Multiple logistic regression analyses to determine factors associated with periodontitis.
4. Discussion
The findings of our study are consistent with the results of other previous studies showing higher salivary malondialdehyde levels in patients with periodontitis than in healthy oral subjects [5,6]. In addition, the novel finding of our study was that there is an association between salivary malondialdehyde levels and periodontitis independently of other known risk factors.
In the meta-analysis by Chen et al. of 2019 (including 14 articles and 931 subjects, 474 with and 457 without periodontitis), higher salivary concentrations of malondialdehyde in subjects with periodontitis than in periodontally healthy subjects were found [5]. In most of the studies included in the meta-analysis by Chen et al. were found higher salivary malondialdehyde levels were found in patients with periodontitis than in healthy controls [28,29,30,31,32,33,34,35,36,37]. However, in a few studies included in that meta-analysis, no significant differences were found in salivary malondialdehyde levels between patients with periodontitis and healthy controls [38,39,40]. In addition, in one study with 19 subjects, lower salivary malondialdehyde levels were found in patients with periodontitis compared to healthy controls [41].
In the meta-analysis by Mohideen et al. in 2023 (including 10 articles and 763 subjects, 393 with and 370 without periodontitis), higher salivary concentrations of malondialdehyde in subjects with periodontitis than in periodontally healthy subjects were found [6]. Those 10 articles were also included in the meta-analysis published by Chen et al., and no new studies were included in the meta-analysis by Chen et al. [5].
In addition, three studies that were not included in any of the meta-analyses also reported higher salivary concentrations of malondialdehyde in subjects with periodontitis than in healthy subjects [42,43,44]. In the study by Altıngöz et al., 120 subjects (60 with periodontitis and 60 healthy subjects) were included [42]. In the study by Gautam et al., 112 subjects (56 with periodontitis and 56 healthy subjects) were included [43]. In the study by Veljovic et al., 50 subjects were included (30 with periodontitis and 20 healthy subjects) [44].
Other variables that were associated with periodontitis in our study were age and never smoking, findings that have also been reported previously [13,19]. However, we found no other variables associated with periodontitis, possibly due to the relatively small sample size of our study.
We have found an association between salivary malondialdehyde levels and age; but we have not found significant differences in salivary malondialdehyde levels according to sex, diabetes mellitus, arterial hypertension, rheumatoid arthritis, systemic lupus erythematosus, cardiovascular disease, hypercholesterolemia, coffee, never smoker, tea, alcohol, obesity, immunosuppressive therapy, radiotherapy or metrotexate. It is possible that other variables that we have not registered could influence salivary malondialdehyde levels. However, the only variable associated with salivary malondialdehyde levels (age) was introduced in the regression analysis, and we found that salivary malondialdehyde and age were independently associated with periodontitis in the multiple logistic regression analysis. Thus, we think that with those findings, the bias risk could have been mitigated. This finding of our study about the positive association between salivary malondialdehyde levels and age has been previously described [45].
Another finding of our study was the positive correlation between salivary malondialdehyde levels and the severity of periodontitis, which was also found in previous studies [9,10,11,12].
All together, these results indicate that alteration of the oxidative state occurs in periodontitis. High salivary malondialdehyde levels found in patients with periodontitis could represent an increase in lipid peroxidation. Increased ROS production may contribute to high salivary malondialdehyde levels found in patients with periodontitis. Those aspects could be related to the periodontal inflammation in periodontitis.
Previous studies by our research team also found that malondialdehyde levels could be used as a biomarker of severity in patients with different diseases such as sepsis [46], traumatic brain injury [47], cerebral infarcts [48] or spontaneous intracerebral hemorrhage [49] and hepatocellular carcinoma undergoing liver transplantation [50]. We carried out this study due to the fact that we found in our previous studies that malondialdehyde levels could be used as a severity biomarker in determined patients, and we hypothesized that there could be an association between salivary malondialdehyde levels and periodontitis regardless of other risk factors.
The administration of agents that modulate the antioxidant and oxidant state could be a promising treatment for patients with severe periodontitis. In fact, treatment with melatonin has been shown to improve periodontal disease in some patients. Besides its antioxidant effects, melatonin also exerts anti-inflammatory and anti-apoptotic properties [51,52,53,54]. A systematic review by Balaji et al. analyzed the use of melatonin in the management of periodontitis, including four studies on topical (orobase cream) and eight with systemic (oral tablet) melatonin administration [53]. All four studies using topical melatonin administration reported improvements in periodontal disease. Only two of eight studies using oral melatonin administration reported periodontal parameters, and improvements in periodontal parameters were reported in those two studies using oral melatonin administration. Some studies also found a reduction in inflammatory biomarkers (C-reactive protein, tumor necrosis factor alpha, interleukin-6) in saliva and blood with the administration of topical and oral melatonin. However, only one study by Zare et al. assessed the oxidative state [54], reporting that oral melatonin reduced serum malondialdehyde levels and increased total antioxidant capacity.
The diagnosis of periodontitis is performed by clinical and radiological examination; however, the determination of salivary malondialdehyde concentrations could help in the diagnosis of periodontitis according to the results of our ROC analysis. The clinical diagnosis of periodontitis can be interfered with by certain factors such as the pressure applied with the periodontal probe in the crevice, limited mouth opening, and discomfort during the exploration [2]. Thus, the use of salivary biomarkers could help in the diagnosis of periodontitis and periodontitis severity classification [2,3,4]. It is considered that an AUC less than 0.7 is sub-optimal performance, from 0.70 to 0.80 is considered good, and a value of 0.80 or above is excellent [55,56]. Thus, the AUC of 0.7 that we found in our study is within the limit to be considered good. However, it would be interesting to conduct more studies to confirm our findings. In addition, assessing salivary malondialdehyde concentrations could help assess the saliva antioxidant status of subjects. The use of mouth creams with antioxidant agents may be suggested for individuals with high salivary malondialdehyde concentrations to help prevent or delay the development of periodontitis or to help prevent or delay its progression to more severe forms or to try to reverse its severity. As is logical, before taking this step, studies with mouth creams with antioxidant agents should first be carried out in animal models and then in humans.
We would like to acknowledge some limitations in our study. First, malondialdehyde levels were not determined in other biological samples (like blood or gingival crevicular fluid). Second, a larger sample size would have allowed us not to include patients with local gingivitis in the category of subjects without periodontitis. Third, we have not calculated the sample size; however, it was sufficient to find an association between salivary malondialdehyde concentrations and periodontitis independently of other risk factors in the regression analysis. Previously, higher salivary concentrations in subjects with periodontitis than in periodontally healthy subjects in the bivariate analysis have been reported [5,6]. However, the independent association of salivary malondialdehyde levels and periodontitis in a regression analysis has not previously been reported. Therefore, the novel objective of our study was to explore this possible association by performing a logistic regression analysis. Thus, the association between salivary malondialdehyde concentrations and periodontitis independently of other risk factors in the regression analysis that we found in our study represents the main novel finding of our study. Despite the limitations of our study, this is the first to report such findings.
5. Conclusions
In conclusion, to our knowledge, this is the first study reporting that salivary malondialdehyde levels are associated with periodontitis, independently of other known risk factors.
Author Contributions
L.L. conceived, designed, and coordinated this study, participated in the acquisition and interpretation of data, and drafted the manuscript. E.H.M., A.D.L.M., A.F.G.-R., M.J.M.G., C.H.M., O.H.M. and C.M.H.P. participated in the acquisition of data. P.A.G. participated in the salivary levels determinations. A.J. participated in the interpretation of data. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Clinical Research Ethics Committee of the Hospital Universitario de Canarias approved the study protocol (CHUC_2023_138, 30 November 2023).
Informed Consent Statement
Informed consent was obtained from each subject prior to inclusion in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
Clínica Dental Cándido (Laguna, Tenerife, Spain) clinic has paid the costs of consumables and reagents for the determinations.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Medrano, A.G.; Martinez-Martinez, R.E.; Soria-Guerra, R.; Portales-Perez, D.; Bach, H.; Martinez-Gutierrez, F. A systematic review of the protein composition of whole saliva in subjects with healthy periodontium compared with chronic periodontitis. PLoS ONE 2023, 18, e0286079. [Google Scholar] [CrossRef]
- Gomes, P.R.; Rocha, M.D.; Lira, J.A.; Coelho, F.A.; Alves, E.H.; Nascimento, H.M.; Oliveira, S.M.; Carmo, R.R.; Araújo, H.T.; Silva, F.R.; et al. Salivary biomarkers present in patients with periodontitis without clinical distinction: Findings from a meta-analysis. Med. Oral Patol. Oral Cir. Bucal. 2023, 28, e457–e466. [Google Scholar] [CrossRef]
- Arroyo, E.; Oliveira-Alves, M.G.; Chamorro-Petronacci, C.M.; Marichalar-Mendia, X.; Bravo-López, S.B.; Blanco-Carrión, J.; Pérez-Sayáns, M. Protein-based salivary biomarkers for the diagnosis of periodontal diseases: Systematic review and meta-analysis. J. Taibah. Univ. Med. Sci. 2022, 18, 737–747. [Google Scholar] [CrossRef]
- Chen, M.; Cai, W.; Zhao, S.; Shi, L.; Chen, Y.; Li, X.; Sun, X.; Mao, Y.; He, B.; Hou, Y.; et al. Oxidante stress-related biomarkers in saliva and gingival crevicular fluid associated with chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 608–622. [Google Scholar] [CrossRef] [PubMed]
- Mohideen, K.; Chandrasekar, K.; Ramsridhar, S.; Rajkumar, C.; Ghosh, S.; Dhungel, S. Assessment of Oxidative Stress by the Estimation of Lipid Peroxidation Marker Malondialdehyde (MDA) in Patients with Chronic Periodontitis: A Systematic Review and Meta-Analysis. Int. J. Dent. 2023, 2023, 6014706. [Google Scholar] [CrossRef] [PubMed]
- Veljovic, T.; Djuric, M.; Mirnic, J.; Gusic, I.; Maletin, A.; Ivic, S.; Stojilkovic, M.; Brkic, S. Effect of Nonsurgical Periodontal Treatment on Salivary and Plasma Superoxide Dismutase Levels of Patients Suffering from Periodontitis. J. Clin. Med. 2023, 12, 6688. [Google Scholar] [CrossRef]
- He, W.; Fu, Y.; Yao, S.; Huang, L. Programmed cell death of periodontal ligament cells. J. Cell. Physiol. 2023, 238, 1768–1787. [Google Scholar] [CrossRef]
- Khalili, J.; Biloklytska, H.F. Salivary malondialdehyde levels in clinically healthy and periodontal diseased individuals. Oral Dis. 2008, 14, 754–760. [Google Scholar] [CrossRef]
- Akhi, R.; Nissinen, A.E.; Wang, C.; Kyrklund, M.; Paju, S.; Mäntylä, P.; Buhlin, K.; Sinisalo, J.; Pussinen, P.J.; Hörkkö, S. Salivary IgA antibody to malondialdehyde-acetaldehyde associates with mild periodontal pocket depth. Oral Dis. 2022, 28, 2285–2293. [Google Scholar] [CrossRef]
- Celecová, V.; Kamodyová, N.; Tóthová, L.; Kúdela, M.; Celec, P. Salivary markers of oxidative stress are related to age and oral health in adult non-smokers. J. Oral Pathol. Med. 2013, 42, 263–266. [Google Scholar] [CrossRef]
- Nanakaly, H.; Nouri Ahmed, S.; Warya Azeez, H. Effect of periodontal therapy on serum and salivary Interleukin-1 beta (IL-1β) and malondialdehyde levels in chronic periodontitis. Cell. Mol. Biol. 2024, 70, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S130–S148. [Google Scholar] [CrossRef] [PubMed]
- Shiau, H.J.; Reynolds, M.A. Sex differences in destructive periodontal disease: A systematic review. J. Periodontol. 2010, 81, 1379–1389. [Google Scholar] [CrossRef]
- Adam, M. Obesity as a risk factor for periodontitis—Does it really matter? Evid. Based Dent. 2023, 24, 48–49. [Google Scholar] [CrossRef] [PubMed]
- Enteghad, S.; Shirban, F.; Nikbakht, M.H.; Bagherniya, M.; Sahebkar, A. Relationship Between Diabetes Mellitus and Periodontal/Peri-Implant Disease: A Contemporaneous Review. Int. Dent. J. 2024, 74, 426–445. [Google Scholar] [CrossRef]
- Tan, P.R.; Lee, A.J.L.; Zhao, J.J.; Chan, Y.H.; Fu, J.H.; Ma, M.; Tay, S.H. Higher odds of periodontitis in systemic lupus erythematosus compared to controls and rheumatoid arthritis: A systematic review, meta-analysis and network meta-analysis. Front. Immunol. 2024, 15, 1356714. [Google Scholar] [CrossRef]
- Tada, A.; Tano, R.; Miura, H. The relationship between tooth loss and hypertension: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 13311. [Google Scholar] [CrossRef]
- Salvi, G.E.; Roccuzzo, A.; Imber, J.C.; Stähli, A.; Klinge, B.; Lang, N.P. Clinical periodontal diagnosis. Periodontol. 2000, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S149–S161. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Hernández Marrero, E.; Abreu González, P.; Lorente Martín, A.D.; González-Rivero, A.F.; Marrero González, M.J.; Hernández Marrero, C.; Hernández Marrero, O.; Jiménez, A.; Hernández Padilla, C.M. Observational prospective study to determine the association and diagnostic utility of salivary nitrites levels in periodontitis. Quintessence Int. 2025, 56, 100–107. [Google Scholar] [PubMed]
- Lorente, L.; Hernández Marrero, E.; Abreu González, P.; Lorente Martín, A.D.; González-Rivero, A.F.; Marrero González, M.J.; Hernández Marrero, C.; Hernández Marrero, O.; Jiménez, A.; Hernández Padilla, C.M. Low Salivary Uric Acid Levels Are Independently Associated with Periodontitis. World. J. Clin. Cases. 2025; in press. [Google Scholar]
- Kikugawa, K.; Kojima, T.; Yamaki, S.; Kosugi, H. Interpretation of the thiobarbituric acid reactivity of rat liver and brain homogenates in the presence of ferric ion and ethylediaminotetraacetic acid. Anal. Biochem. 1992, 202, 249–255. [Google Scholar] [CrossRef]
- Hodges, D.M.; DeLong, J.M.; Forney, C.F.; Prange, R.K. Improving the thiobarbituric acid-reactive-substances assay for estimating lipid peroxidation in plant tissues containing anthocyanin and other interfering compounds. Planta 1999, 207, 604–611. [Google Scholar] [CrossRef]
- Valenzuela, A. The biological significance of malondialdehyde determination in the assessment of tissue oxidative stress. Life Sci. 1991, 48, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Baltacıoğlu, E.; Kehribar, M.A.; Yuva, P.; Alver, A.; Atagün, O.S.; Karabulut, E.; Akalın, F.A. Total oxidant status and bone resorption biomarkers in serum and gingival crevicular fluid of patients with periodontitis. J. Periodontol. 2014, 85, 317–326. [Google Scholar] [CrossRef]
- Trivedi, S.; Lal, N.; Mahdi, A.A.; Mittal, M.; Singh, B.; Pandey, S. Evaluation of antioxidant enzymes activity and malondialdehyde levels in patients with chronic periodontitis and diabetes mellitus. J. Periodontol. 2014, 85, 713–720. [Google Scholar] [CrossRef]
- Trivedi, S.; Lal, N.; Mahdi, A.A.; Singh, B.; Pandey, S. Association of salivary lipid peroxidation levels, antioxidant enzymes, and chronic periodontitis. Int. J. Periodontics Restor. Dent. 2015, 35, e14–e19. [Google Scholar] [CrossRef]
- Canakci, C.F.; Cicek, Y.; Yildirim, A.; Sezer, U.; Canakci, V. Increased levels of 8-hydroxydeoxyguanosine and malondialdehyde and its relationship with antioxidant enzymes in saliva of periodontitis patients. Eur. J. Dent. 2009, 3, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Ngo, L.Q.; Promsudthi, A.; Surarit, R. Salivary Lipid Peroxidation in Patients With Generalized Chronic Periodontitis and Acute Coronary Syndrome. J. Periodontol. 2016, 87, 134–141. [Google Scholar] [CrossRef]
- Akalin, F.A.; Baltacioğlu, E.; Alver, A.; Karabulut, E. Lipid peroxidation levels and total oxidant status in serum, saliva and gingival crevicular fluid in patients with chronic periodontitis. J. Clin. Periodontol. 2007, 34, 558–565. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Ngo, L.Q.; Promsudthi, A.; Surarit, R. Salivary oxidative stress biomarkers in chronic periodontitis and acute coronary syndrome. Clin. Oral Investig. 2017, 21, 2345–2353. [Google Scholar] [CrossRef]
- Önder, C.; Kurgan, Ş.; Altıngöz, S.M.; Bağış, N.; Uyanık, M.; Serdar, M.A.; Kantarcı, A.; Günhan, M. Impact of non-surgical periodontal therapy on saliva and serum levels of markers of oxidative stress. Clin. Oral Investig. 2017, 21, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi-Motamayel, F.; Goodarzi, M.T.; Jamshidi, Z.; Kebriaei, R. Evaluation of Salivary and Serum Antioxidant and Oxidative Stress Statuses in Patients with Chronic Periodontitis: A Case-Control Study. Front. Physiol. 2017, 8, 189. [Google Scholar] [CrossRef]
- Dhotre, P.S.; Suryakar, A.N.; Bhogade, R.B. Oxidative stress in periodontitis: A critical link to cardiovascular disease. Biomed. Res. 2011, 22, 180–184. [Google Scholar]
- Wei, D.; Zhang, X.L.; Wang, Y.Z.; Yang, C.X.; Chen, G. Lipid peroxidation levels, total oxidant status and superoxide dismutase in serum, saliva and gingival crevicular fluid in chronic periodontitis patients before and after periodontal therapy. Aust. Dent. J. 2010, 55, 70–78. [Google Scholar] [CrossRef]
- Miricescu, D.; Totan, A.; Calenic, B.; Mocanu, B.; Didilescu, A.; Mohora, M.; Spinu, T.; Greabu, M. Salivary biomarkers: Relationship between oxidative stress and alveolar bone loss in chronic periodontitis. Acta. Odontol. Scand. 2014, 72, 42–47. [Google Scholar] [CrossRef]
- Guentsch, A.; Preshaw, P.M.; Bremer-Streck, S.; Klinger, G.; Glockmann, E.; Sigusch, B.W. Lipid peroxidation and antioxidant activity in saliva of periodontitis patients: Effect of smoking and periodontal treatment. Clin. Oral Investig. 2008, 12, 345–352. [Google Scholar] [CrossRef]
- Emekli-Alturfan, E.; Yarat, A.; Çalışkan, A.E.; Pisiriciler, R.; Kuru, B.; Noyan, Ü. Determination of storage time of saliva samples obtained from patients with and without chronic periodontitis for the comparison of some biochemical and cytological parameters. J. Clin. Lab. Anal. 2013, 27, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Altıngöz, S.M.; Kurgan, Ş.; Önder, C.; Serdar, M.A.; Ünlütürk, U.; Uyanık, M.; Başkal, N.; Tatakis, D.N.; Günhan, M. Salivary and serum oxidative stress biomarkers and advanced glycation end products in periodontitis patients with or without diabetes: A cross-sectional study. J. Periodontol. 2021, 92, 1274–1285. [Google Scholar] [CrossRef] [PubMed]
- Gautam, A.; Mittal, N.; Mishra, S.P.; Singh, T.B.; Chandra, A. Evaluation of the effect of nonsurgical periodontal therapy on malondialdehyde and 8-hydroxy deoxyguanosine levels in chronic periodontitis. Indian. J. Dent. Res. 2022, 33, 41–45. [Google Scholar] [CrossRef]
- Veljovic, T.; Djuric, M.; Mirnic, J.; Gusic, I.; Maletin, A.; Ramic, B.; Neskovic, I.; Vukoje, K.; Brkic, S. Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis. J. Clin. Med. 2022, 11, 3617. [Google Scholar] [CrossRef]
- Salvolini, E.; Martarelli, D.; Di Giorgio, R.; Mazzanti, L.; Procaccini, M.; Curatola, G. Age-related modifications in human unstimulated whole saliva: A biochemical study. Aging Clin. Exp. Res. 2000, 12, 445–448. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Domínguez-Rodriguez, A.; Labarta, L.; Díaz, C.; Solé-Violán, J.; Ferreres, J.; Cabrera, J.; Igeño, J.C.; et al. Sustained high serum malondialdehyde levels are associated with severity and mortality in septic patients. Crit. Care 2013, 17, R290. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Cáceres, J.J.; Argueso, M.; Solé-Violán, J.; Jiménez, A.; García-Marín, V. Maintained high sustained serum malondialdehyde levels after severe brain trauma injury in non-survivor patients. BMC Res. Notes 2019, 12, 789. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Sabatel, R.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. Non-survivor patients with malignant middle cerebral artery infarction showed persistently high serum malondialdehyde levels. BMC Neurol. 2019, 19, 238. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Sabatel, R.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Riaño-Ruiz, M.; Jiménez, A.; García-Marín, V. Serum Malondialdehyde Levels and Mortality in Patients with Spontaneous Intracerebral Hemorrhage. World Neurosurg. 2018, 113, e542–e547. [Google Scholar] [CrossRef]
- Lorente, L.; Rodriguez, S.T.; Sanz, P.; Abreu-González, P.; Díaz, D.; Moreno, A.M.; Borja, E.; Martín, M.M.; Jiménez, A.; Barrera, M.A. Association between Pre-Transplant Serum Malondialdehyde Levels and Survival One Year after Liver Transplantation for Hepatocellular Carcinoma. Int. J. Mol. Sci. 2016, 17, 500. [Google Scholar] [CrossRef]
- Meenakshi, S.S.; Malaiappan, S. Role of melatonin in periodontal disease—A systematic review. Indian J. Dent. Res. 2020, 31, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.Y.; Li, L.; Zhang, Z.T.; Wu, T.; Lin, S.; Zhang, X.T. Clinical efficacy of melatonin as adjunctive therapy to non-surgical treatment of periodontitis: A systematic review and meta-analysis. Inflammopharmacology 2022, 30, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Mahendra, J.; Fageeh, H.I.; Fageeh, H.N.; Mushtaq, S.; Baeshen, H.A.; Bhandi, S.; Gupta, A.A.; et al. Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review. Materials 2021, 14, 2417. [Google Scholar] [CrossRef]
- Zare Javid, A.; Hosseini, S.A.; Gholinezhad, H.; Moradi, L.; Haghighi-Zadeh, M.H.; Bazyar, H. Antioxidant and Anti-Inflammatory Properties of Melatonin in Patients with Type 2 Diabetes Mellitus with Periodontal Disease Under Non-Surgical Periodontal Therapy: A Double-Blind, Placebo-Controlled Trial. Diabetes Metab. Syndr. Obes. 2020, 13, 753–761. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Sr.; Pencina, M.J.; Massaro, J.M.; Coady, S. Cardiovascular Disease Risk Assessment: Insights from Framingham. Glob. Heart 2013, 8, 11–23. [Google Scholar] [CrossRef]
- Çorbacıoğlu, Ş.K.; Aksel, G. Receiver operating characteristic curve analysis in diagnostic accuracy studies: A guide to interpreting the area under the curve value. Turk. J. Emerg. Med. 2023, 23, 195–198. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).