The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Procedures
2.3. Echocardiography and Cardiac Computed Tomography Analysis
2.4. Definition and Assessment of Endpoints
2.5. Biomarker Assessment
2.6. Statistical Analysis
3. Results
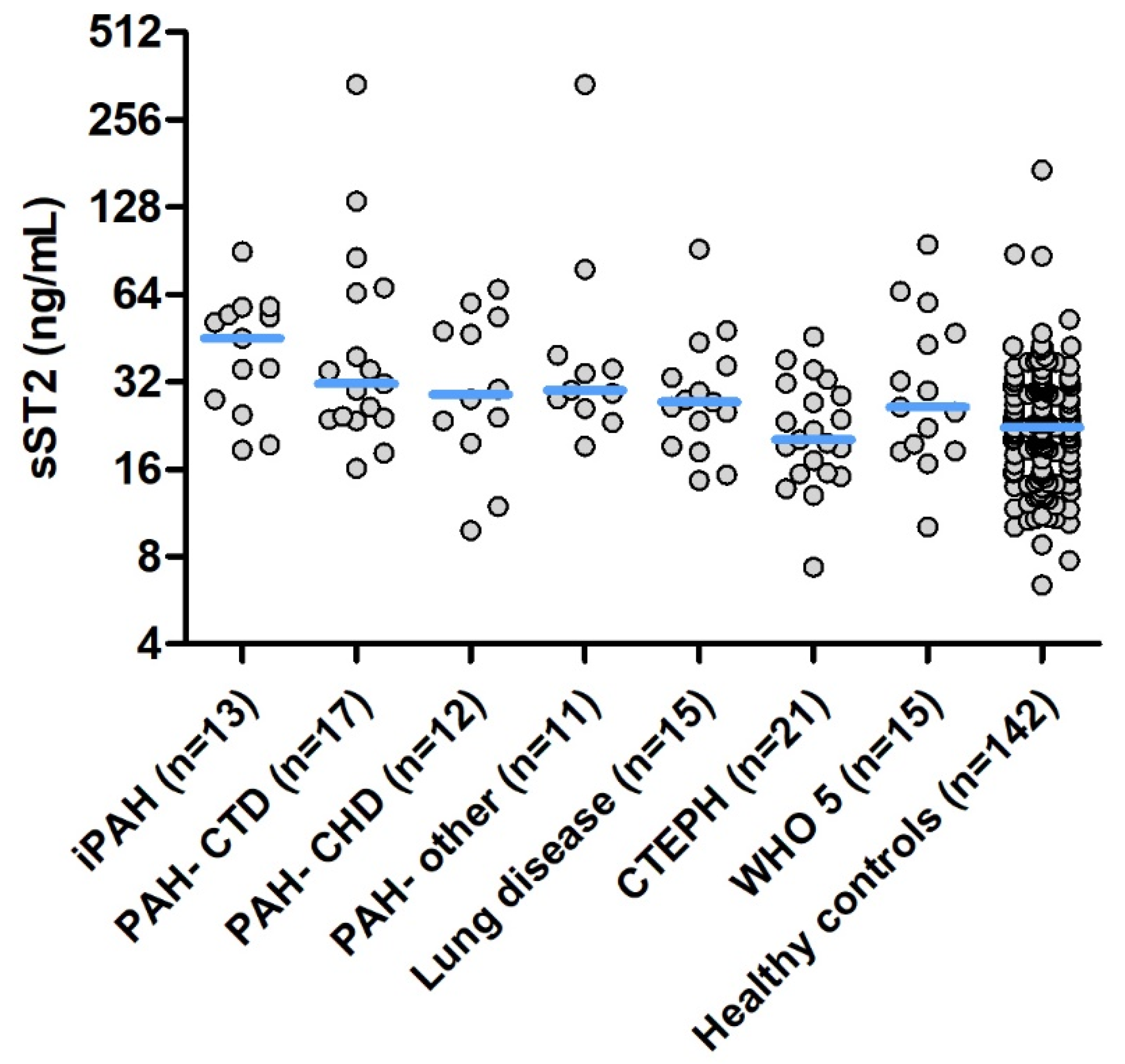
3.1. Baseline Characteristics
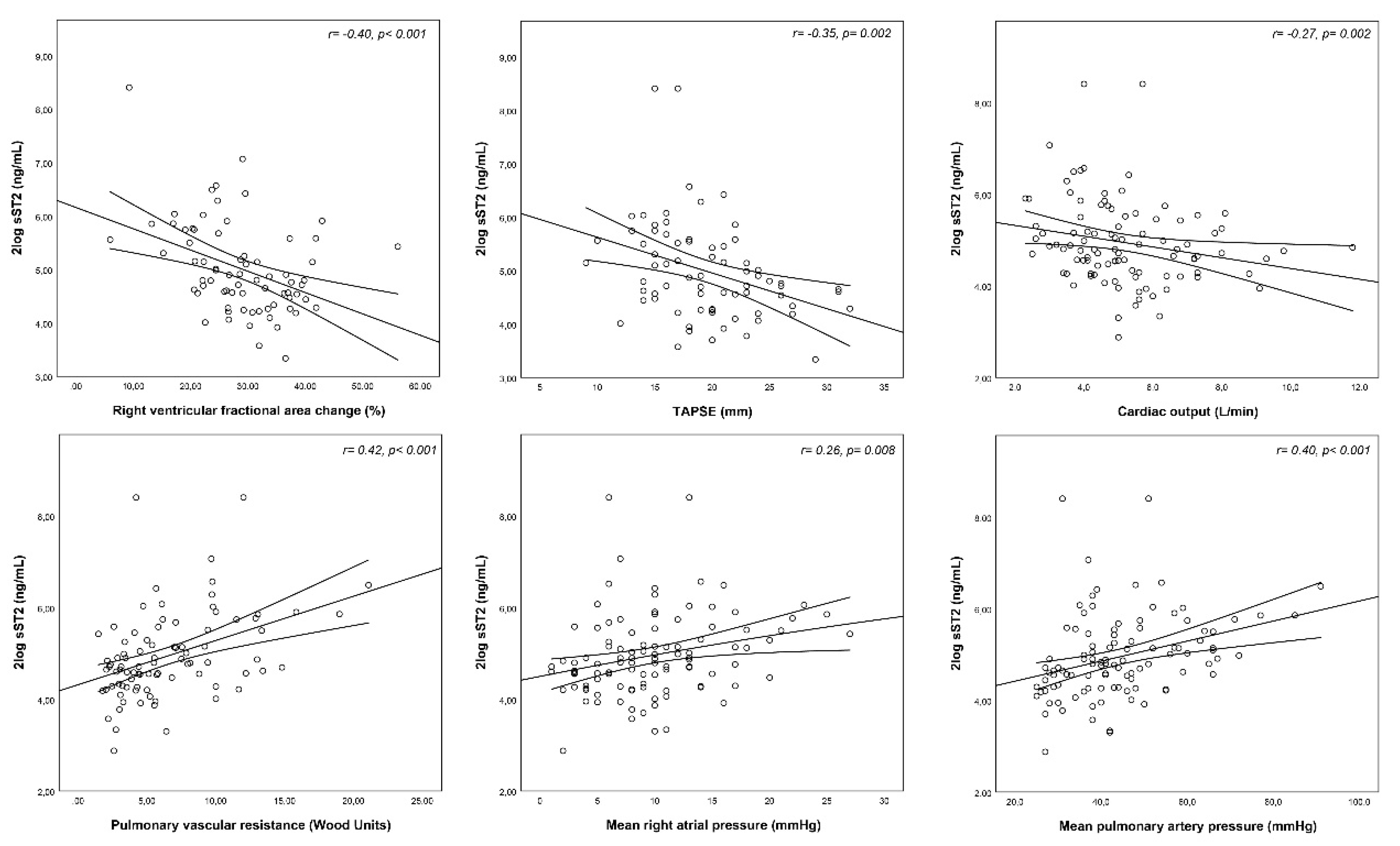
3.2. Correlations between sST2 and Clinical Characteristics
3.3. Follow-Up
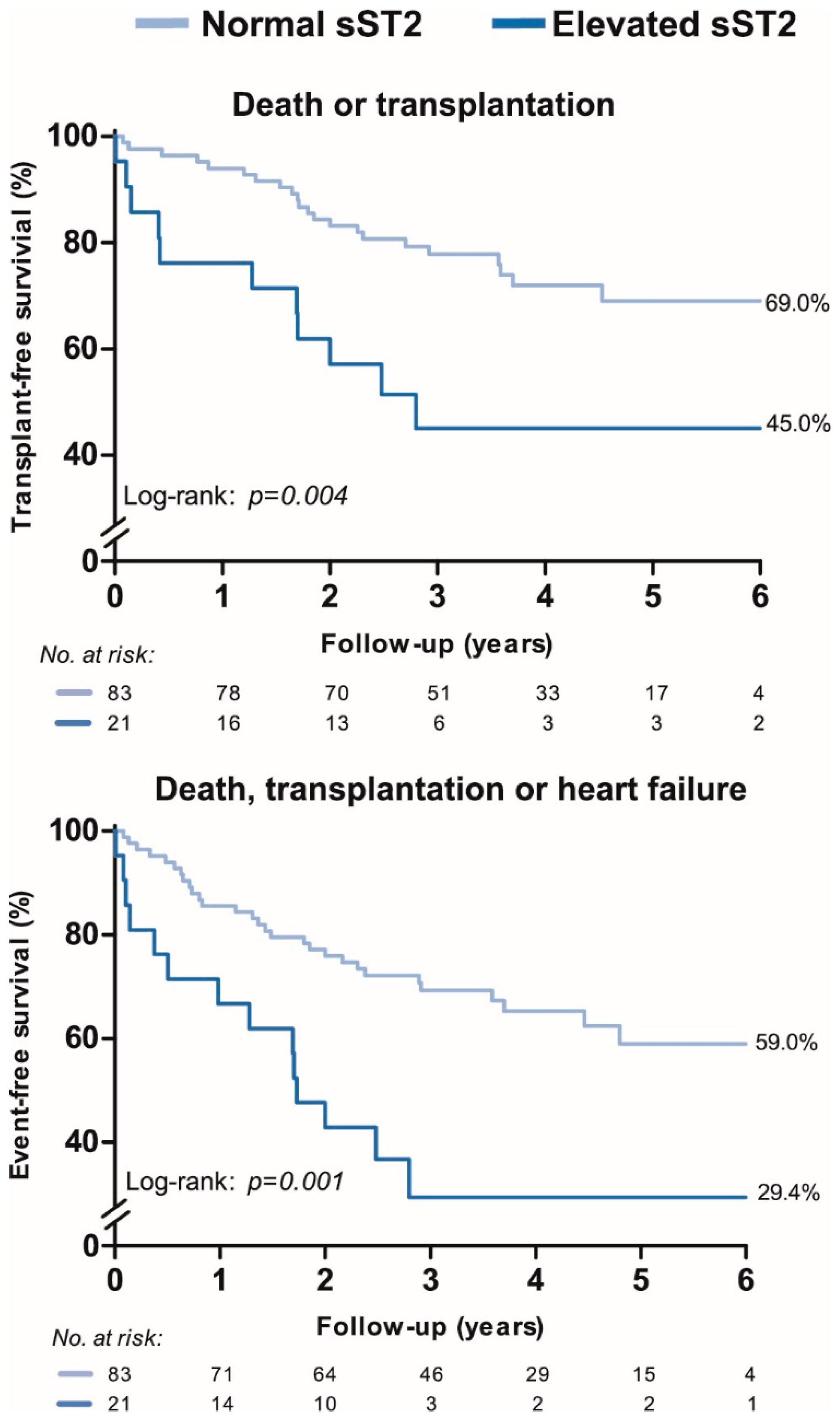
3.4. Associations between ST2 and Clinical Outcomes
4. Discussion
4.1. Previous Studies
4.2. Pathophysiology of sST2 in PH
4.3. sST2 and Etiologic Differences of PH
4.4. Limitations
4.5. Clinical Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Weinberg, E.O.; Shimpo, M.; De Keulenaer, G.W.; MacGillivray, C.; Tominaga, S.; Solomon, S.D.; Rouleau, J.L.; Lee, R.T. Expression and regulation of st2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation 2002, 106, 2961–2966. [Google Scholar] [CrossRef] [PubMed]
- Pei, C.; Barbour, M.; Fairlie-Clarke, K.J.; Allan, D.; Mu, R.; Jiang, H.R. Emerging role of interleukin-33 in autoimmune diseases. Immunology 2014, 141, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Vergaro, G.; Ripoli, A.; Bayes-Genis, A.; Figal, D.A.P.; de Boer, R.A.; Lassus, J.; Mebazaa, A.; Gayat, E.; Breidthardt, T.; et al. Meta-analysis of soluble suppression of tumorigenicity-2 and prognosis in acute heart failure. JACC Heart Fail. 2017, 5, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Vergaro, G.; Passino, C.; Ripoli, A.; Ky, B.; Miller, W.L.; Bayes-Genis, A.; Anand, I.; Januzzi, J.L.; Emdin, M. Prognostic value of soluble suppression of tumorigenicity-2 in chronic heart failure: A meta-analysis. JACC Heart Fail. 2017, 5, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Vonk-Noordegraaf, A.; Haddad, F.; Chin, K.M.; Forfia, P.R.; Kawut, S.M.; Lumens, J.; Naeije, R.; Newman, J.; Oudiz, R.J.; Provencher, S.; et al. Right heart adaptation to pulmonary arterial hypertension: Physiology and pathobiology. J. Am. Coll. Cardiol. 2013, 62, D22–D33. [Google Scholar] [CrossRef] [PubMed]
- Benza, R.L.; Miller, D.P.; Barst, R.J.; Badesch, D.B.; Frost, A.E.; McGoon, M.D. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the reveal registry. Chest 2012, 142, 448–456. [Google Scholar] [CrossRef]
- Farber, H.W.; Miller, D.P.; Poms, A.D.; Badesch, D.B.; Frost, A.E.; Muros-Le Rouzic, E.; Romero, A.J.; Benton, W.W.; Elliott, C.G.; McGoon, M.D.; et al. Five-year outcomes of patients enrolled in the reveal registry. Chest 2015, 148, 1043–1054. [Google Scholar] [CrossRef] [PubMed]
- Hemnes, A.R.; Humbert, M. Pathobiology of pulmonary arterial hypertension: Understanding the roads less travelled. Eur. Respir. Rev. 2017, 26, 170093. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Perros, F.; Caramori, G.; Meng, C.; Dormuller, P.; Chou, P.C.; Church, C.; Papi, A.; Casolari, P.; Welsh, D.; et al. Nuclear il-33 regulates soluble st2 receptor and il-6 expression in primary human arterial endothelial cells and is decreased in idiopathic pulmonary arterial hypertension. Biochem. Biophys. Res. Commun. 2014, 451, 8–14. [Google Scholar] [CrossRef]
- Carlomagno, G.; Messalli, G.; Melillo, R.M.; Stanziola, A.A.; Visciano, C.; Mercurio, V.; Imbriaco, M.; Ghio, S.; Sofia, M.; Bonaduce, D.; et al. Serum soluble st2 and interleukin-33 levels in patients with pulmonary arterial hypertension. Int. J. Cardiol. 2013, 168, 1545–1547. [Google Scholar] [CrossRef]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 esc/ers guidelines for the diagnosis and treatment of pulmonary hypertension: The joint task force for the diagnosis and treatment of pulmonary hypertension of the european society of cardiology (esc) and the european respiratory society (ers): Endorsed by: Association for european paediatric and congenital cardiology (aepc), international society for heart and lung transplantation (ishlt). Eur. Heart J. 2016, 37, 67–119. [Google Scholar]
- Simonneau, G.; Gatzoulis, M.A.; Adatia, I.; Celermajer, D.; Denton, C.; Ghofrani, A.; Gomez Sanchez, M.A.; Krishna Kumar, R.; Landzberg, M.; Machado, R.F.; et al. Updated clinical classification of pulmonary hypertension. J. Am. Coll. Cardiol. 2013, 62, D34–D41. [Google Scholar] [CrossRef] [PubMed]
- Geenen, L.W.; Baggen, V.J.M.; Koudstaal, T.; Boomars, K.A.; Eindhoven, J.A.; Boersma, E.; Roos-Hesselink, J.W.; van den Bosch, A.E. The prognostic value of various biomarkers in adults with pulmonary hypertension; a multi-biomarker approach. Am. Heart J. 2018, 208, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the american society of echocardiography and the european association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Freed, B.H.; Collins, J.D.; Francois, C.J.; Barker, A.J.; Cuttica, M.J.; Chesler, N.C.; Markl, M.; Shah, S.J. Mr and ct imaging for the evaluation of pulmonary hypertension. JACC Cardiovasc. Imaging 2016, 9, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Menting, M.E.; McGhie, J.S.; Koopman, L.P.; Vletter, W.B.; Helbing, W.A.; van den Bosch, A.E.; Roos-Hesselink, J.W. Normal myocardial strain values using 2d speckle tracking echocardiography in healthy adults aged 20 to 72 years. Echocardiography 2016, 33, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
- Geenen, L.W.; Baggen, V.J.M.; van den Bosch, A.E.; Eindhoven, J.A.; Cuypers, J.; Witsenburg, M.; Boersma, E.; Roos-Hesselink, J.W. Prognostic value of soluble st2 in adults with congenital heart disease. Heart 2019, 105, 999–1006. [Google Scholar] [CrossRef]
- Zheng, Y.G.; Yang, T.; He, J.G.; Chen, G.; Liu, Z.H.; Xiong, C.M.; Gu, Q.; Ni, X.H.; Zhao, Z.H. Plasma soluble st2 levels correlate with disease severity and predict clinical worsening in patients with pulmonary arterial hypertension. Clin. Cardiol. 2014, 37, 365–370. [Google Scholar] [CrossRef]
- Placido, R.; Cortez-Dias, N.; Martins, S.R.; Almeida, A.G.; Calisto, C.; Goncalves, S.; Sadoune, M.; Diogo, A.N.; Mebazaa, A.; Pinto, F.J. Prognostic stratification in pulmonary hypertension: A multi-biomarker approach estratificacao prognostica na hipertensao pulmonar: Valor acrescido da abordagem multibiomarcadores. Rev. Port. Cardiol. 2017, 36, 111–125. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Januzzi, J.L. The biology of st2: The international st2 consensus panel. Am. J. Cardiol. 2015, 115, 3B–7B. [Google Scholar] [CrossRef]
- Sanada, S.; Hakuno, D.; Higgins, L.J.; Schreiter, E.R.; McKenzie, A.N.; Lee, R.T. Il-33 and st2 comprise a critical biomechanically induced and cardioprotective signaling system. J. Clin. Investig. 2007, 117, 1538–1549. [Google Scholar] [CrossRef]
- Farber, H.W.; Loscalzo, J. Pulmonary arterial hypertension. N. Engl. J. Med. 2004, 351, 1655–1665. [Google Scholar] [CrossRef]
- Groth, A.; Vrugt, B.; Brock, M.; Speich, R.; Ulrich, S.; Huber, L.C. Inflammatory cytokines in pulmonary hypertension. Respir. Res. 2014, 15, 47. [Google Scholar] [CrossRef]
- Zabini, D.; Heinemann, A.; Foris, V.; Nagaraj, C.; Nierlich, P.; Balint, Z.; Kwapiszewska, G.; Lang, I.M.; Klepetko, W.; Olschewski, H.; et al. Comprehensive analysis of inflammatory markers in chronic thromboembolic pulmonary hypertension patients. Eur. Respir. J. 2014, 44, 951–962. [Google Scholar] [CrossRef] [Green Version]
- Piper, S.; deCourcey, J.; Sherwood, R.; Amin-Youssef, G.; McDonagh, T. Biologic variability of soluble st2 in patients with stable chronic heart failure and implications for monitoring. Am. J. Cardiol. 2016, 118, 95–98. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Complete Cases (n, %) | All | PAH | PH Lung Disease | CTEPH | WHO 5/mixed | |
|---|---|---|---|---|---|---|
| n = 104 | n = 53 | n = 15 | n = 21 | n = 15 | ||
| Clinical characteristics | ||||||
| Age, years | 104 (100) | 59 (47–69) | 55 (41–66) | 64 (55–72) | 59 (42–73) | 65 (57–70) |
| Sex, women n (%) | 104 (100) | 66 (64) | 35 (66) | 8 (53) | 12 (57) | 11 (73) |
| Body mass index, kg/m² | 104 (100) | 28.1 ± 6.6 | 26.3 ± 5.8 | 30.5 ± 6.3 | 31.4 ± 5.7 | 27.8 ± 8.5 |
| Heart rate, beats/minute | 104 (100) | 80 ± 16 | 80 ± 16 | 81 ± 12 | 75 ± 17 | 85 ± 19 |
| Systolic blood pressure, mmHg | 104 (100) | 127 ± 18 | 122 ± 15 | 125 ± 17 | 131 ± 13 | 133 ± 27 |
| Oxygen saturation <90%, n (%) | 104 (100) | 3 (3) | 2 (4) | 1 (7) | 0 (0) | 0 (0) |
| NYHA class 3/4, n (%) | 104 (100) | 56 (54) | 31 (59) | 8 (53) | 9 (43) | 8 (53) |
| 6-minute walking distance | 89 (86) | 337 ± 139 | 348 ± 147 | 309 ± 115 | 385 ± 130 | 261 ± 122 |
| Electrocardiogram | ||||||
| Sinus rhythm, n(%) | 102 (97) | 90 (87) | 46 (87) | 13 (87) | 18 (86) | 13 (87) |
| QRS duration, ms | 100 (96) | 98 (90–106) | 100 (89–124) | 100 (91–111) | 94 (88–99) | 100 (89–124) |
| Echocardiogram | ||||||
| RA area, cm² | 79 (76) | 27.5 ± 26.2 | 28.0 ± 6.9 | 28.4 ± 8.4 | 24.6 ± 10.0 | 28.2 ± 13.1 |
| RV end diastolic basal dimension, mm | 74 (71) | 51.5 ± 9.6 | 52.7 ± 8.1 | 47.8 ± 4.7 | 51.1 ± 12.1 | 50.2 ± 13.0 |
| RV fractional area change, % | 72 (69) | 28.9 ± 8.6 | 26.7 ± 7.8 | 31.3 ± 6.2 | 33.0 ± 4.3 | 30.7 ± 12.7 |
| TAPSE, mm | 72 (69) | 20 ± 5 | 19 ± 5 | 19 ± 3 | 21 ± 3 | 21 ± 7 |
| LV function, n (%): | 99 (94) | |||||
| Normal | 65 (66) | 32 (63) | 10 (71) | 15 (83) | 8 (53) | |
| Mildly impaired | 29 (30) | 17 (33) | 4 (29) | 3 (17) | 5 (33) | |
| Moderately/ severely impaired | 4 (4) | 2 (4) | 0 (0) | 0 (0) | 2 (14) | |
| LV end diastolic dimension, mm | 80 (77) | 43.2 ± 7.4 | 46.7 ± 5.6 | 46.1 ± 7.3 | 45.5 ± 5.6 | 46.8 ± 8.4 |
| Hemodynamics | ||||||
| mPAP, mmHg | 104 (100) | 42 (35–52) | 46 (39–60) | 37 (32–41) | 37 (30–48) | 42 (34–47) |
| mRAP, mmHg | 104 (100) | 10 ± 5 | 11 ± 6 | 8 ± 4 | 8 ± 5 | 11 ± 6 |
| Capillary wedge pressure, mmHg | 90 (87) | 13 ± 6 | 11 ± 5 | 13 ± 4 | 14 ± 3 | 19 ± 9 |
| Pulmonary vascular resistance, WU | 86 (83) | 5.5 (3.4–9.4) | 7.9 (5.4–12.0) | 4.4 (4.1–5.5) | 3.4 (3.0–5.3) | 4.1 (2.2–6.8) |
| Cardiac output, L/min | 99 (87) | 4.9 (4.0–6.2) | 5.0 (3.9–5.8) | 5.0 (3.9–5.8) | 5.4 (4.9–6.3) | 4.9 (4.0–6.8) |
| Computed tomography | ||||||
| PA diameter, mm | 98 (94) | 34.4 ± 5.4 | 35.3 ± 6.0 | 34.9 ± 4.1 | 34.4 ± 5.1 | 31.1 ± 3.3 |
| PA/AO ratio | 98 (94) | 1.12 ± 0.24 | 1.20 ± 0.26 | 1.03 ± 0.12 | 1.12 ± 0.24 | 0.98 ± 0.13 |
| Laboratory | ||||||
| sST2, ng/mL | 104 (100) | 27.9 (19.6–44.9) | 34.2 (24.1–54.1) | 27.3 (19.2–36.3) | 20.2 (15.5–28.6) | 26.2 (18.5–47.1) |
| NT-proBNP, pmol/L | 104 (100) | 60 (21–226) | 120 (26–280) | 60 (23–216) | 24 (5–36) | 31 (12–282) |
| sST2 | ||
|---|---|---|
| Clinical Characteristics | r | p-Value |
| Age | −0.09 | 0.346 |
| Sex | 0.11 | 0.260 |
| Body mass index | −0.15 | 0.124 |
| Heart rate | 0.28 | 0.005 |
| Systolic blood pressure | −0.21 | 0.036 |
| Oxygen saturation < 90% | 0.08 | 0.417 |
| NYHA class 3/4 | 0.23 | 0.018 |
| 6-minute walking distance | −0.29 | 0.007 |
| Electrocardiogram | ||
| Loss of sinus rhythm | 0.17 | 0.095 |
| QRS Duration | 0.15 | 0.142 |
| Echocardiogram | ||
| Right atrial area | 0.13 | 0.269 |
| RV basal dimension | 0.17 | 0.145 |
| RV fractional area change | −0.40 | <0.001 |
| TAPSE, mm | −0.35 | 0.002 |
| LV end diastolic dimension | −0.23 | 0.044 |
| Hemodynamics | ||
| mPAP | 0.40 | <0.001 |
| mRAP | 0.26 | 0.008 |
| Capillary wedge pressure | −0.11 | 0.314 |
| Pulmonary vascular resistance | 0.42 | <0.001 |
| Cardiac output | −0.27 | 0.007 |
| Computed tomography | ||
| PA diameter | 0.07 | 0.475 |
| PA/AO ratio | 0.08 | 0.426 |
| Laboratory | ||
| NT-proBNP | 0.54 | <0.001 |
| Hazard Ratio * (95%CI) | p-Value | |
|---|---|---|
| Primary endpoint (n = 33) | ||
| sST2 (univariable) | 1.53 (1.12–2.07) | 0.007 |
| Adjusted for: | ||
| Age and sex | 1.59 (1.17–2.16) | 0.003 |
| NT-proBNP | 1.13 (0.75–1.69) | 0.568 |
| Secondary endpoint (n = 43) | ||
| sST2 (univariable) | 1.45 (1.10–1.90) | 0.008 |
| Adjusted for: | ||
| Age and sex | 1.50 (1.15–1.95) | 0.002 |
| NT-proBNP | 1.07 (0.75–1.52) | 0.712 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geenen, L.W.; Baggen, V.J.M.; Kauling, R.M.; Koudstaal, T.; Boomars, K.A.; Boersma, E.; Roos-Hesselink, J.W.; van den Bosch, A.E. The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension. J. Clin. Med. 2019, 8, 1517. https://doi.org/10.3390/jcm8101517
Geenen LW, Baggen VJM, Kauling RM, Koudstaal T, Boomars KA, Boersma E, Roos-Hesselink JW, van den Bosch AE. The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension. Journal of Clinical Medicine. 2019; 8(10):1517. https://doi.org/10.3390/jcm8101517
Chicago/Turabian StyleGeenen, Laurie W., Vivan J. M. Baggen, Robert M. Kauling, Thomas Koudstaal, Karin A. Boomars, Eric Boersma, Jolien W. Roos-Hesselink, and Annemien E. van den Bosch. 2019. "The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension" Journal of Clinical Medicine 8, no. 10: 1517. https://doi.org/10.3390/jcm8101517
APA StyleGeenen, L. W., Baggen, V. J. M., Kauling, R. M., Koudstaal, T., Boomars, K. A., Boersma, E., Roos-Hesselink, J. W., & van den Bosch, A. E. (2019). The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension. Journal of Clinical Medicine, 8(10), 1517. https://doi.org/10.3390/jcm8101517