Abstract
Background: Mycophenolic acid (MPA), a crucial immunosuppressive drug, and plasmapheresis, an effective immunoreduction method, are simultaneously used for the management of various immune-related diseases, including kidney transplantation. While plasmapheresis has been proven efficient in removing many substances from the blood, its effect on MPA plasma levels remains unestablished. Objectives: To evaluate the full pharmacokinetics of MPA by measuring the area under the time–concentration curve (AUC0–12), which is the best indicator for MPA treatment monitoring after each plasmapheresis session, and to compare the AUC0–12 measurements on the day with and on the day without plasmapheresis. Methods: A cross-sectional study was conducted in kidney transplantation recipients who were taking a twice-daily oral dose of mycophenolate mofetil (MMF, Cellcept®) and undergoing plasmapheresis at King Chulalongkorn Memorial Hospital, Bangkok, Thailand, during January 2018 and January 2019. The MPA levels were measured by an enzymatic method (Roche diagnostic®) 0, 1/2, 1, 2, 3, 4, 6, 8, and 12 h after MMF administration, for AUC0–12 calculation on the day with and on the day without plasmapheresis sessions. Plasmapheresis was started within 4 h after administering the oral morning dose of MMF. Our primary outcome was the difference of AUC0–12 between the day with and the day without plasmapheresis. Results: Forty complete AUC measurements included 20 measurements on the plasmapheresis day and other 20 measurements on the day without plasmapheresis in six kidney transplant patients. The mean age of the patients was 56.2 ± 20.7 years. All patients had received 1000 mg/day of MMF for at least 72 h before undergoing 3.5 ± 1.2 plasmapheresis sessions. The mean AUC on the day with plasmapheresis was lower than that on the day without plasmapheresis (28.22 ± 8.21 vs. 36.79 ± 10.29 mg × h/L, p = 0.001), and the percentage of AUC reduction was 19.49 ± 24.83%. This was mainly the result of a decrease in AUC0–4 of MPA (23.96 ± 28.12% reduction). Conclusions: Plasmapheresis significantly reduces the level of full AUC0–12 of MPA. The present study is the first to measure the full AUC0–12 in MPA-treated patients undergoing plasmapheresis. Our study suggests that a supplementary dose of MPA is necessary for patients undergoing plasmapheresis.
1. Introduction
Mycophenolic acid (MPA) is one of the main powerful immunosuppressive drugs widely used for many immunological diseases. There are two MPA compounds available, i.e., mycophenolate mofetil (MMF, Cellcept®) and enteric-coated mycophenolate sodium (EC-MPS, Myfortic®). Both MMF and EC-MPS are similar in terms of efficacy and safety. EC-MPS was developed to improve the side effects of upper gastrointestinal symptoms. The time to reach maximum plasma MPA concentration (tmax) of MMF is usually within 1–2 h after an oral dose, while EC-MPS reveals a median lag time from 0.25 to 1.25 h [1]. After absorption from the gastrointestinal tract, 97 to 99% of MPA, which is the active form, will bind to serum albumin. MPA is converted by uridine diphosphate-glucuronosyltransferase (UGT) into inactive mycophenolic acid glucuronide (MPAG), which is mainly excreted by the renal tubules. MPAG can also be excreted in the biliary tract by multidrug-resistant protein (MRP), which can lead to enterohepatic recycling. [1]
Plasmapheresis is one of the most effective methods utilized for rapid immunoglobulin removal in various immunological diseases. Many proteins and protein-bound substances, including medications, can also be removed during plasmapheresis sessions [2,3]. Substances which are likely to be removed during plasmapheresis have the following characters: (1) high blood concentration, (2) high protein bound, (3) low volume of distribution (Vd), and (4) undergoing high-dose/high-efficiency plasmapheresis [4].
Several immunologically mediated diseases can be treated by MPA together with plasmapheresis, i.e., systemic lupus erythematosus (SLE), lupus nephritis, myasthenia gravis, Guillain–Barré syndrome, psoriatic arthritis, relapsed/refractory thrombotic thrombocytopenic purpura (TTP), severe polymyositis/dermatomyositis, inflammatory bowel disease, pemphigus vulgaris, and kidney transplantation [5,6,7]. Unintentional removal of MPA may result in inadequate immunosuppression and unfavorable outcomes. Of interest, the effect of plasmapheresis on MPA concentration has been studied only in a case series of two patients, one kidney transplant recipient and one patient with myasthenia gravis [8]. MPA removal were measured by considering MPA levels at only two time points—before and after each plasmapheresis session. The MPA removal was calculated on the basis of MPA concentration in plasma effluent. The authors concluded that plasmapheresis of 3 L of plasma did not significantly alter post-plasmapheresis MPA concentration. Currently, there are no available data regarding the effect of plasmapheresis on the area under the concentration–time curve from 0 to 12 h (AUC0–12) of MPA, which is the best indicator of MPA exposure of patients.
The present study was conducted in kidney transplant recipients who were taking stable doses of MMF and had indication for plasmapheresis to examine the effects of plasmapheresis on MPA exposure.
2. Methods
An observational study of patients who were taking MMF (Roche, Basel, Switzerland) in combination with plasmapheresis treatment was conducted in King Chulalongkorn Memorial Hospital, Bangkok, Thailand, during January 2018 and January 2019. The inclusion criteria were kidney transplant recipients older than 18 years, who were under an immunosuppressive regimen of tacrolimus, MMF, low-dose prednisolone and had an indication for plasmapheresis. The dosage of MMF had to be 500 mg orally every 12 h for at least one week. Exclusion criteria were patients with serum albumin concentration lower than 2 g/dL and patients who were coadministered a proton pump inhibitor.
Plasmapheresis sessions were initiated within 4 h after the morning dose of MMF. The plasmapheresis machine was Plasauto EZ®, and the dialyzer was Plasmaflo® with a maximum pore size of 0.3 µm. The total treatment volume was 1.5 plasma volume per session. The blood flow rate was 150 mL/h. The replacement fluid was 5% albumin in the same volume as the treatment volume. The number of sessions required was determined on the basis of the clinical judgment of the attending nephrologists.
Plasmapheresis was performed on an alternate day basis for patients who were prescribed more than one plasmapheresis session.
Patients had to strictly take a stable dose of MMF, i.e., 500 mg orally every 12 h for at least one week, before entering the study. MMF dosage adjustment was not allowed during the study period. Patients were not allowed to have a meal for one hour before and two hours after taking the MMF dose. MPA level was measured by an enzymatic immunoassay method (Roche-diagnostic®). The AUC0–12 was calculated with the trapezoidal rule from the MPA levels at nine time points after the morning dose of MMF (C0, C0.5, C1, C2, C3, C4, C6, C8, and C12) (Figure 1). The full AUC0–12 was measured on the day just before the day patients underwent plasmapheresis and compared with the AUC0–12 of the following day, in which patients received the plasmapheresis treatment. Blood samples were taken via a heparin lock in the arm by using the double-syringe technique.

Figure 1.
Timing of mofetil (MMF) dosage, plasmapheresis sessions, and meal on the day before and on the day with a plasmapheresis session. MPA: mycophenolic acid.
A complete clinical evaluation including vital signs and body weight was performed. The baseline characteristics including age, cause of end-stage renal disease, type of kidney transplantation, time after kidney transplantation, renal function, indications for plasmapheresis, session of plasmapheresis, and plasma volume per session were recorded.
Absolute and relative frequencies were used for qualitative data. Mean and standard deviation were utilized for numerical data. The chi-squared test was used for comparisons between categorical data. Paired-samples t-test was used to compare the AUC0–12 of the day with plasmapheresis and the AUC0–12 of the day without plasmapheresis. Data were analyzed using the SPSS statistic version 22 (IBM; New York, NY, USA).
This study was approved by The Research Ethics Review Committee for Research Involving Human Research Participants, Health Sciences Group, Chulalongkorn University (IRB No.CF 333/61). The study was registered with the Thai Clinical Trials Registry (TCTR20190211001).
3. Results
Six kidney transplant recipients were enrolled, with a total of 20 plasmapheresis sessions. There were 40 AUC0–12 measurements (each AUC consisted of measurements of MPA levels at 9 time points), 20 of which were recorded on the day just before the day patients underwent plasmapheresis, and the other 20 were recorded on the following day, when patients underwent a plasmapheresis session. The mean (±SD) age of the patients was 56.2 ± 20.7 years, and five patients (83.3%) were men (Table 1). At baseline, the mean (±SD) estimated glomerular filtration rate (eGFR) was 49.7 ± 10.9 mL/min/1.73 m2, serum albumin concentration was 3.8 ± 0.4 g/dL, and hemoglobin concentration was 10.3 ± 1.4 g/dL. Indication for plasmapheresis was antibody-mediated rejection (ABMR) for all six patients, who were diagnosed by pathological presentation and donor-specific antibody (DSA) detection. The number of plasmapheresis sessions per patient was 3.5 ± 1.2 (range of 1–4 sessions).

Table 1.
Baseline characteristics of the patients.
The mean of MPA AUC0–12 of the day with plasmapheresis was significantly lower than that of the day without plasmapheresis (28.22 ± 8.21 vs. 36.79 ± 10.29 mg × h/L, p = 0.001) (Figure 2). The percentage reduction of AUC0–12 was 19.49 ± 24.83% (Table 2). The early part of the AUC was affected by plasmapheresis sessions. The AUC0–4 of the day with plasmapheresis was significantly lower than that of the day without plasmapheresis (15.79 ± 6.46 vs. 21.78 ± 5.66 mg × h/L, p < 0.001), while the AUC4–12 was not significantly different between the day with and that without plasmapheresis (12.43 ± 5.02 vs. 15.00 ± 7.56 mg × h/L, p = 0.125).
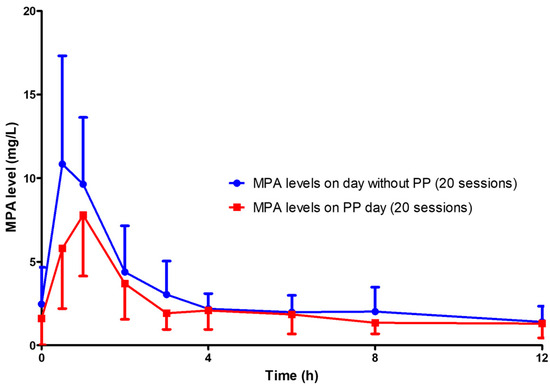
Figure 2.
MPA levels on the day with plasmapheresis (20 sessions) compared with those on the day without plasmapheresis (20 sessions). PP: plasmapheresis.
Table 2.
Comparison of MPA AUCs recorded on days with and without plasmapheresis, from 0 to 12 h, from 0 to 4 h, and from 4 to 12 h.
The reduction of MPA AUC0–12 was detected as early as the first session of plasmapheresis. The MPA AUC0–12 of the day before and of the day of the first session of plasmapheresis were 41.66 ± 10.66 and 32.26 ± 9.42mg × h/L, respectively (p = 0.001) (Table 2 and Figure 3). The percentage reduction of MPA AUC0–12 of the first day of plasmapheresis session was 22.86 ± 6.99%. The AUC0–12 of the day before the second to that of the day of the forth plasmapheresis sessions could be rebounded from the AUC0–12 of the day with plasmapheresis. However, the rebounded AUC0–12 gradually decreased with the number of sessions of plasmapheresis that the patients received (Figure 4). Given that the target therapeutic AUC0–12 of MPA is 30 to 60 mg × h/L for kidney transplantation recipients [9], 17 out of 20 (85%) AUC0–12 measured on the day without plasmapheresis achieved the target therapeutic range, compared with only 9 out of 20 (45%) AUC0–12 measured on the day with plasmapheresis (p = 0.008) (Figure 5).
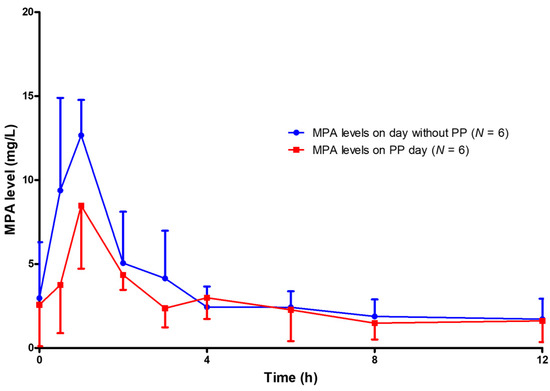
Figure 3.
MPA levels on the day before the first plasmapheresis session (N = 6) compared with MPA levels on the day with the first plasmapheresis session (N = 6).
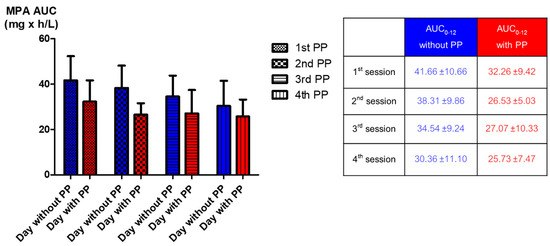
Figure 4.
Comparison of the mean MPA AUC0–12 between the day with and that without plasmapheresis from the first plasmapheresis session to the fourth session.
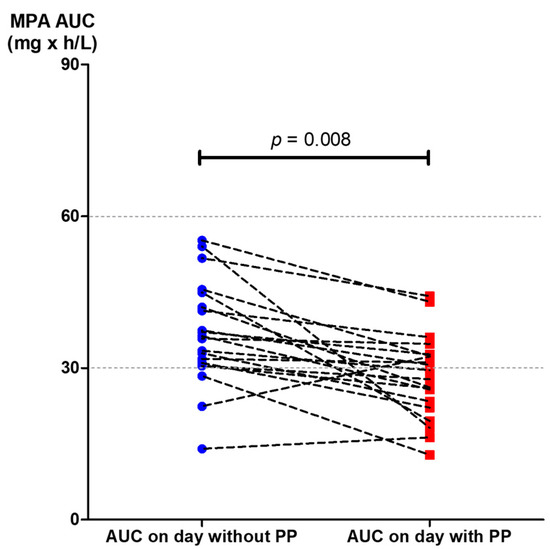
Figure 5.
The MPA AUC0–12 achieved the target level between the day just before a plasmapheresis session (20 measurements) and the following day, when plasmapheresis was administered (20 measurements).
4. Discussion
The present study is the first to demonstrate the effect of plasmapheresis on MPA exposure by using the full MPA AUC0–12. The AUC0–12 of MPA was significantly affected by plasmapheresis. This effect was found starting from the first session of plasmapheresis (Figure 2 and Figure 3). One-fifth of the total AUC0–12 was lowered by plasmapheresis. The component of AUC most affected by plasmapheresis was the early part (AUC0–4). Undergoing plasmapheresis treatment immediately after an oral dose of MMF can lower the MPA peak level, leading to exposure to a subtherapeutic level of MPA. Consecutive sessions of plasmapheresis could increase the risk of underimmunosuppression by lowering the rebound of MPA AUC0–12 (Figure 4).
MMF is one of the major immunosuppressive agents widely used to treat many immunological diseases. Since overimmunosuppression can lead to many side effects and underimmunosuppression can cause unfavorable treatment outcomes, MPA level monitoring has been recommended to maintain MPA concentration at the therapeutic level [9,10]. Plasmapheresis is one of the most effective methods for rapid immunoglobulin G (IgG) reduction [5]. Many high-molecular-weight substances can also be removed during a plasmapheresis session, especially proteins and albumin, which makes albumin replacement necessary. Since 97 to 99% of MPA is protein-bound, MPA should be theoretically removed from patients during plasmapheresis treatment.
The effect of plasmapheresis on MPA plasma level was reported in only two patients who were administered MMF in combination with plasmapheresis [8]. Plasmapheresis sessions were started 4 h after MMF administration, and MPA removal was assessed at only two time points (pre- and post-plasmapheresis) together with MPA concentration in plasma waste. The authors concluded that a plasmapheresis session starting later than 4 h after the administration of an oral MMF dose did not significantly alter MPA concentration. Since serum proteins can be trapped in the dialyzer and bloodline, monitoring of MPA removal by only measuring MPA in plasma waste may not reflect total MPA removal. Our study monitored MPA exposure by full AUC0–12 measurement on the day with a plasmapheresis session as the study arm and on the day without plasmapheresis as the control arm. Alteration in AUC0–12 between the day with and the day without plasmapheresis is the best indicator of the effect of plasmapheresis on MPA plasma levels. The early phase of the full MPA AUC (peak level, AUC0–4) is the one mostly affecting MPA exposure and represents more than 50% of AUC0–12. The plasmapheresis sessions designed in the present study started within one hour after oral administration of an MMF dose which is the most crucial period for determining the effects of plasmapheresis on MPA.
MPA together with plasmapheresis is mainly utilized for the treatment of many immunologic conditions and diseases which require potent immunosuppression, such as kidney transplant rejection, severe lupus nephritis, or relapsed/refractory thrombotic thrombocytopenic purpura. The patients enrolled in the present study were kidney transplant recipients who were taking MMF and experienced antibody-mediated rejection, which is indicated for plasmapheresis treatment. The present study reveals that MPA administration without dosage adjustment during consecutive sessions of plasmapheresis can lead to unexpected underimmunosuppression and may increase the failure rate of treatment. The present study demonstrated that MPA AUC0–12 is reduced by 20% when a plasmapheresis session is started within 4 h after oral administration of MMF (Table 2, Figure 2). The higher the number of consecutive sessions of plasmapheresis performed, the higher the chance of MPA underexposure (Figure 4). We also further examined the role of MMF dose increments in two patients who underwent plasmapheresis and found that increasing the MMF dose from 1000 mg/day to 1250 mg/day can prevent subtherapeutic AUC0–12 during plasmapheresis sessions (unpublished data). An MMF dosage increment of 20% may be required to maintain a therapeutic level of MPA on the day patients undergo plasmapheresis. A further comprehensive study of therapeutic drug monitoring in patients with increased dose of MPA before undergoing plasmapheresis is crucially required. Otherwise, a 4 h delay of the plasmapheresis session after administration of an MMF dose may reduce the effect of plasmapheresis on MPA exposure (Figure 6).
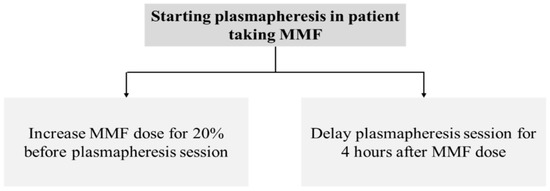
Figure 6.
Recommendations for MMF dose or plasmapheresis adjustment in patient receiving concomitant MMF and plasmapheresis treatment.
The MMF dose used in the present study was relatively low. This is because the target population of patients enrolled in this study were kidney transplant recipients who were in the maintenance phase of immunosuppression. Moreover, a study on Asian patients showed that most of the patients achieved the target MPA level with an MMF dose of 1000 mg/day [11]. Besides conventional plasmapheresis, a study of the effects of others apheresis techniques such as double-filtration plasmapheresis and immunoadsorption, which have different kinetics of protein removal, should be carried out.
5. Conclusions
Plasmapheresis significantly reduces MPA plasma levels, particularly in the early phase after oral administration of an MPA dose. This effect should be addressed when combining MPA administration together with plasmapheresis in a treatment protocol.
Author Contributions
Conceptualization, S.P., N.T. and S.U.; methodology, S.P., N.T. and S.V.; formal analysis, N.T. and K.P. (Krit Pongpirul); investigation, S.P. and S.W.; writing-original draft preparation, S.P. and N.T.; writing-review and editing, N.T., B.S., Y.A., K.T., S.E.-O. and K.P. (Kearkiat Praditpornsilpa); visualization, N.T., supervision, N.T.; project administration, N.T.; funding acquisition, S.P. and N.T.
Funding
This research was funded by Ratchadaphiseksomphot Fund of Chulalongkorn University, grant number RA61/106.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Staatz, C.E.; Tett, S.E. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin. Pharmacokinet. 2007, 46, 13–58. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, R.B.; Liu, C.; Cronin, S.M.; Murphy, B.C.; Cha, R.; Swerdlow, P.; Edward, D.J. Drug Removal by Plasmapheresis: An Evidence-Based Review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2007, 27, 1529–1549. [Google Scholar] [CrossRef] [PubMed]
- Katagri, D.; Mogi, K. Double Filtration Plasmapheresis. In The Concise Manual of Apheresis Therapy; Springer: Heidelberg, Germany, 2014; pp. 57–64. [Google Scholar]
- Ibrahim, R.B.; Balogun, R.A. Medications in Patients Treated with Therapeutic Plasma Exchange: Prescription Dosage, Timing, and Drug Overdose. Semin. Dial. 2012, 25, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Padmanabhan, A.; Aqui, N.; Balogun, R.A.; Delaney, M.; Dunbar, N.M.; Witt, V.; Wu, Y.; Shaz, B.H.; Connelly-Smith, L.; et al. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice-Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Seventh Special Issue. J. Clin. Apher. 2016, 31, 149–338. [Google Scholar] [CrossRef] [PubMed]
- Houssiau, F.A.; D’Cruz, D.; Sangle, S.; Remy, P.; Vasconcelos, C.; Petrovic, R.; Fiehn, C.; Garrido, E.D.R.; Gilboe, I.-M.; Tektonidou, M.; et al. Azathioprine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis: Results from the maintain Nephritis Trial. Ann. Rheum. Dis. 2010, 69, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, H.; Tedesco-Silva, H.; Demirbaş, A.; Vitko, S.; Nashan, B.; Gürkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced Exposure to Calcineurin Inhibitors in Renal Transplantation. New Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, A.Q.; Davies, N.M.; Crow, S.A.; Little, C.; Ojogho, O.N.; Weeks, D.L. Effects of Plasmapheresis on Mycophenolic Acid Concentrations. Transplantation 2011, 91, e3–e4. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, D.R.; Le Meur, Y.; Cantarovich, M.; Tredger, M.J.; Tett, S.E.; Cattaneo, D.; Tönshoff, B.; Holt, D.W.; Chapman, J.; Van Gelder, T.; et al. Consensus Report on Therapeutic Drug Monitoring of Mycophenolic Acid in Solid Organ Transplantation. Clin. J. Am. Soc. Nephrol. 2010, 5, 341–358. [Google Scholar] [CrossRef]
- van Gelder, T.; Hilbrands, L.B.; Vanrenterghem, Y.; Weimar, W.; de Fijter, J.W.; Squifflet, J.P.; Hené, R.J.; Verpooten, G.A.; Navarro, M.T.; Hale, M.D.; et al. A randomized double-blind, multicenter plasma concentration controlled study of the safety and efficacy of oral mycophenolate mofetil for the prevention of acute rejection after kidney transplantation. Transplantation 1999, 68, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Pithukpakorn, M.; Tiwawanwong, T.; Lalerd, Y.; Assawamakin, A.; Premasathian, N.; Tasanarong, A.; Thongnoppakhun, W.; Vongwiwatana, A. Mycophenolic acid AUC in Thai kidney transplant recipients receiving low dose mycophenolate and its association with UGT2B7 polymorphisms. Pharm. Pers. Med. 2014, 7, 379–385. [Google Scholar] [CrossRef][Green Version]






© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).