The Changing Landscape of Acute Kidney Injury in Pregnancy from an Obstetrics Perspective


Abstract
:1. Introduction
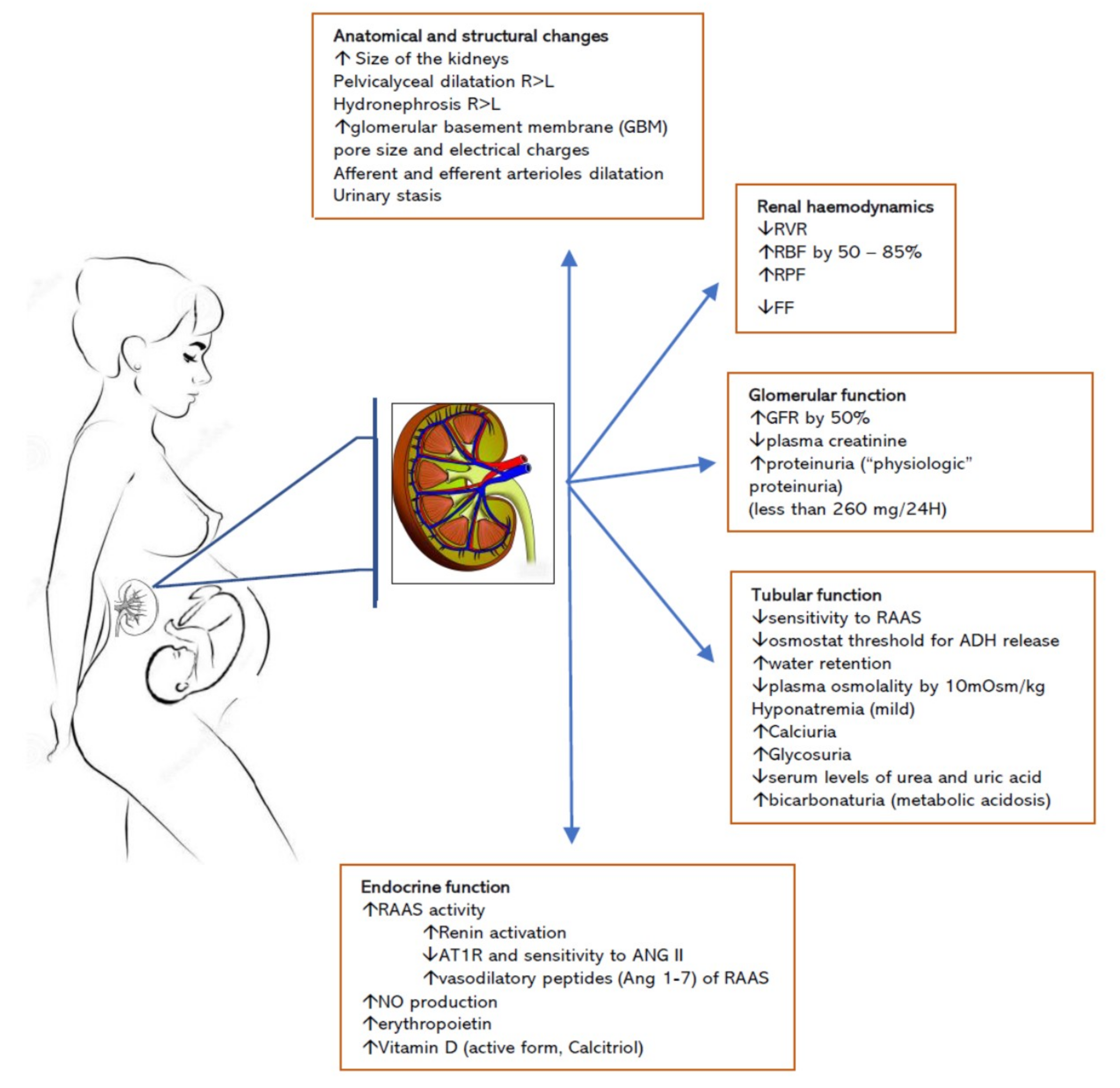
2. Physiological Changes and Kidney Adaptation to Pregnancy
3. The Changing Epidemiological Landscape of Acute Kidney Injury in Pregnancy
4. Challenges in Diagnosis of PR-AKI
5. Principle of Management of PR-AKI
6. Clinical Presentations of PR-AKI
6.1. Bleeding and Hypovolemia
6.2. Infection and Sepsis
6.3. Hypertensive Disorders of Pregnancy
6.4. Haematological/Immune Conditions
7. The Risk of CKD after AKI
8. Conclusions
Author Contributions
Conflicts of Interest
References
- Piccoli, G.B.; Zakharova, E.; Attini, R.; Ibarra Hernandez, M.; Covella, B.; Alrukhaimi, M.; Liu, Z.-H.; Ashuntantang, G.; Orozco Guillen, A.; Cabiddu, G.; et al. Acute Kidney Injury in Pregnancy: The Need for Higher Awareness. A Pragmatic Review Focused on What Could Be Improved in the Prevention and Care of Pregnancy-Related AKI, in the Year Dedicated to Women and Kidney Diseases. J. Clin. Med. 2018, 7, 318. [Google Scholar] [CrossRef]
- Liu, Y.; Ma, X.; Zheng, J.; Liu, X.; Yan, T. Pregnancy outcomes in patients with acute kidney injury during pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2017, 17, 235. [Google Scholar] [CrossRef]
- Covella, B.; Vinturache, A.E.; Cabiddu, G.; Attini, R.; Gesualdo, L.; Versino, E.; Piccoli, G.B. A systematic review and meta-analysis indicates long-term risk of chronic and end-stage kidney disease after preeclampsia. Kidney Int. 2019, 96, 711–727. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Maxia, S.; Lepori, N.; Tuveri, M.; Massidda, M.; Marchi, C.; Mura, S.; et al. Risk of Adverse Pregnancy Outcomes in Women with CKD. J. Am. Soc. Nephrol. 2015, 26, 2011–2022. [Google Scholar] [CrossRef] [Green Version]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Moroni, G.; Giannattasio, M.; Gregorini, G.; Giacchino, F.; Attini, R.; Loi, V.; et al. A best practice position statement on pregnancy in chronic kidney disease: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2016, 29, 277–303. [Google Scholar] [CrossRef]
- Acharya, A.; Santos, J.; Linde, B.; Anis, K. Acute Kidney Injury in Pregnancy—Current Status. Adv. Chronic Kidney Dis. 2013, 20, 215–222. [Google Scholar] [CrossRef]
- Machado, S.; Figueiredo, N.; Borges, A.; Sao Jose Pais, M.; Freitas, L.; Moura, P.; Campos, M. Acute kidney injury in pregnancy: A clinical challenge. J. Nephrol. 2012, 25, 19–30. [Google Scholar] [CrossRef]
- Nwoko, R.; Plećaš, D.; Garovic, V.D. Acute kidney injury in the pregnant patient. Clin. Nephrol. 2012, 78, 478–486. [Google Scholar] [CrossRef]
- Rao, S.; Jim, B. Acute Kidney Injury in Pregnancy: The Changing Landscape for the 21st Century. Kidney Int. Rep. 2018, 3, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.R.; Rolleston, G.L. Kidney length and ureteric dilatation in the puerperium. BJOG Int. J. Obs. Gynaecol. 1971, 78, 55–61. [Google Scholar] [CrossRef]
- Cheung, K.L.; Lafayette, R.A. Renal physiology of pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 209–214. [Google Scholar] [CrossRef]
- Beydoun, S.N. Morphologic Changes in the Renal Tract in Pregnancy. Clin. Obs. Gynecol. 1985, 28, 249–256. [Google Scholar] [CrossRef]
- Faundes, A.; Brícola-Filho, M.; E Silva, J.C.P. Dilatation of the urinary tract during pregnancy: Proposal of a curve of maximal caliceal diameter by gestational age. Am. J. Obs. Gynecol. 1998, 178, 1082–1086. [Google Scholar] [CrossRef]
- Au, K.K.L.; Woo, J.S.K.; Tang, L.C.H.; Liang, S.T. Aetiological Factors in the Genesis of Pregnancy Hydronephrosis. Aust. N. Z. J. Obs. Gynaecol. 1985, 25, 248–251. [Google Scholar] [CrossRef]
- Hytten, F. Blood volume changes in normal pregnancy. Clin. Haematol. 1985, 14, 601–612. [Google Scholar] [CrossRef]
- Chapman, A.B.; Abraham, W.T.; Zamudio, S.; Coffin, C.; Merouani, A.; Young, D.; Johnson, A.; Osorio, F.; Goldberg, C.; Moore, L.G.; et al. Temporal relationships between hormonal and hemodynamic changes in early human pregnancy. Kidney Int. 1998, 54, 2056–2063. [Google Scholar] [CrossRef] [Green Version]
- Odutayo, A.; Hladunewich, M. Obstetric Nephrology: Renal Hemodynamic and Metabolic Physiology in Normal Pregnancy. Clin. J. Am. Soc. Nephrol. 2012, 7, 2073–2080. [Google Scholar] [CrossRef] [Green Version]
- Davison, J.M.; Dunlop, W. Renal hemodynamics and tubular function in normal human pregnancy. Kidney Int. 1980, 18, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Carlin, A.; Alfirevic, Z. Physiological changes of pregnancy and monitoring. Best Pr. Res. Clin. Obs. Gynaecol. 2008, 22, 801–823. [Google Scholar] [CrossRef]
- Blackburn, S.T. Maternal, Fetal & Neonatal Physiology: A Clinical Perspective, 4th ed.; Elsevier: St. Louis, MD, USA, 2013. [Google Scholar]
- Cunningham, F.G. Laboratory values in normal pregnancy. In Protocols for High-Risk Pregnancies: An Evidence-Based Approach, 5th ed.; John, T., Queenan, J., Cha, C.Y.S., Eds.; Blackwell Science Ltd.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Jameson, J.; Fauci, A.; Kasper, D.L.; Hauser, S.L.; Longo, D.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 20th ed.; McGraw Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Wiles, K.; Bramham, K.; Seed, P.T.; Nelson-Piercy, C.; Lightstone, L.; Chappell, L.C. Serum Creatinine in Pregnancy: A Systematic Review. Kidney Int. Rep. 2019, 4, 408–419. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Maynard, S.E.; Kimmel, P.L. Misapplications of Commonly Used Kidney Equations: Renal Physiology in Practice. Clin. J. Am. Soc. Nephrol. 2009, 4, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Lopes van Balen, V.A.; van Gansewinkel, T.A.G.; de Haas, S.; Spaan, J.J.; Ghossein-Doha, C.; van Kuijk, S.M.J.; van Drongelen, J.; Cornelis, T.; Spaanderman, M.E.A. Kidney function during pregnancy: A systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2018. [Google Scholar] [CrossRef]
- Harel, Z.; McArthur, E.; Hladunewich, M.; Dirk, J.S.; Wald, R.; Garg, A.X.; Ray, J.G. Serum Creatinine Levels Before, During, and After Pregnancy Serum Creatinine Levels Before, During, and After Pregnancy Letters. JAMA 2019, 321, 205–207. [Google Scholar] [CrossRef]
- Davison, J.M.; Hytten, F.E. The effect of pregnancy on the renal handling of glucose. BJOG Int. J. Obs. Gynaecol. 1975, 82, 374–381. [Google Scholar] [CrossRef]
- Cornelis, T.; Odutayo, A.; Keunen, J.; Hladunewich, M. The Kidney in Normal Pregnancy and Preeclampsia. Semin. Nephrol. 2011, 31, 4–14. [Google Scholar] [CrossRef]
- Davison, J.M. Kidney function in pregnant women. Am. J. Kidney Dis. 1987, 9, 248–252. [Google Scholar] [CrossRef]
- Brown, M.A.; Sinosich, M.J.; Saunders, D.M.; Eileen, D.M. Gallery Potassium regulation and progesterone-aldosterone interrelationships in human pregnancy: A prospective study. Am. J. Obs. Gynecol. 1986, 155, 349–353. [Google Scholar] [CrossRef]
- Section 2: AKI Definition. Kidney Int. Suppl. 2012, 2, 19–36. [CrossRef] [Green Version]
- Barasch, J.; Zager, R.; Bonventre, J.V. Acute Kidney Injury: A Problem of Definition. Lancet 2017, 389, 779–781. [Google Scholar] [CrossRef]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative Workgroup. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef]
- Makris, K.; Spanou, L. Acute Kidney Injury: Definition, Pathophysiology and Clinical Phenotypes. Clin. Biochem. Rev. 2016, 37, 85–98. [Google Scholar]
- Mehta, R.L.; A Kellum, J.; Shah, S.V.; A Molitoris, B.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Kellum, J.A.L.N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; MacLeod, A.M.; et al. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Tsai, T.-Y.; Chien, H.; Tsai, F.-C.; Pan, H.-C.; Yang, H.-Y.; Lee, S.-Y.; Hsu, H.-H.; Fang, J.-T.; Yang, C.-W.; Chen, Y.-C. Comparison of RIFLE, AKIN, and KDIGO classifications for assessing prognosis of patients on extracorporeal membrane oxygenation. J. Med. Assoc. 2017, 116, 844–851. [Google Scholar] [CrossRef]
- Luo, X.; Jiang, L.; Du, B.; Wen, Y.; Wang, M.; Xi, X. A comparison of different diagnostic criteria of acute kidney injury in critically ill patients. Crit. Care 2014, 18, R144. [Google Scholar] [CrossRef]
- Fujii, T.; Uchino, S.; Takinami, M.; Bellomo, R. Validation of the Kidney Disease Improving Global Outcomes Criteria for AKI and Comparison of Three Criteria in Hospitalized Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Lameire, N.H.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; A Kellum, J.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Van Biesen, W.; et al. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Hou, S.P.C. Acute renal failure in pregnancy. Saudi J. Kidney Dis. Transpl. 1998, 9, 261–266. [Google Scholar]
- Rewa, O.; Bagshaw, S.M. Acute kidney injury—Epidemiology, outcomes and economics. Nat. Rev. Nephrol. 2014, 10, 193–207. [Google Scholar] [CrossRef]
- Sawhney, S.; Fraser, S.D. Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI. Adv. Chronic Kidney Dis. 2017, 24, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Grunfeld, J.P.; Ganeval, D.; Bournerias, F. Acute renal failure in pregnancy. Kidney Int. 1980, 18, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Siribamrungwong, M.; Chinudomwong, P. Relation between acute kidney injury and pregnancy-related factors. J. Acute Dis. 2016, 5, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Piccoli, G.B.; Kooij, I.A.; Attini, R.; Montersino, B.; Fassio, F.; Gerbino, M.; Biolcati, M.; Cabiddu, G.; Versino, E.; Todros, T. A Systematic Review on Materno-Foetal Outcomes in Pregnant Women with IgA Nephropathy: A Case of “Late-Maternal” Preeclampsia? J. Clin. Med. 2018, 7, 212. [Google Scholar] [CrossRef]
- Najar, M.S.; Shah, A.R.; Wani, I.A.; Reshi, A.R.; Banday, K.A.; Bhat, M.A.; Saldanha, C.L. Pregnancy related acute kidney injury: A single center experience from the Kashmir Valley. Indian J. Nephrol. 2008, 18, 159–161. [Google Scholar] [CrossRef]
- Bentata, Y.; Housni, B.; Mimouni, A.; Azzouzi, A.; Abouqal, R. Acute kidney injury related to pregnancy in developing countries: Etiology and risk factors in an intensive care unit. J. Nephrol. 2012, 25, 764–775. [Google Scholar] [CrossRef]
- Ansari, M.R.; Laghari, M.S.; Solangi, K.B. Acute renal failure in pregnancy: One year observational study at Liaquat University Hospital, Hyderabad. J. Pak. Med. Assoc. 2008, 58, 61. [Google Scholar]
- Van Hook, J.W. Acute kidney injury during pregnancy. Clin. Obs. Gynecol. 2014, 57, 851–861. [Google Scholar] [CrossRef]
- Deltombe, C.; Fakhouri, F. Pregnancy-related acute kidney injury in high income countries: Still a critical issue. J. Nephrol. 2017, 30, 767–771. [Google Scholar]
- Sabban, H.; Zakhari, A.; Patenaude, V.; Tulandi, T.; Abenhaim, H.A. Obstetrical and perinatal morbidity and mortality among in-vitro fertilization pregnancies: A population-based study. Arch. Gynecol. Obs. 2017, 296, 107–113. [Google Scholar] [CrossRef]
- Heldal, K.; Lyngdal, P.; Johansen, T.; Kahn, J.; Johansen, T.E.B. Acute renal failure following IVF: Case report. Hum. Reprod. 2005, 20, 2250–2252. [Google Scholar] [CrossRef] [Green Version]
- Khalaf, Y. Ovarian hyperstimulation syndrome and its effect on renal function in a renal transplant patient undergoing IVF treatment: Case report. Hum. Reprod. 2000, 15, 1275–1277. [Google Scholar] [CrossRef] [Green Version]
- Varghese, J.S.M. Ovarian hyperstimulation syndrome causing atypical renal disease. Am. J. Kidney Dis. 2015, 65, A1–A93. [Google Scholar]
- Stratta, P.; Besso, L.; Canavese, C.; Grill, A.; Todros, T.; Benedetto, C.; Hollo, S.; Segoloni, G.P. Is Pregnancy-Related Acute Renal Failure a Disappearing Clinical Entity? Ren. Fail. 1996, 18, 575–584. [Google Scholar] [CrossRef]
- Mehrabadi, A.; Liu, S.; Bartholomew, S.; A Hutcheon, J.; A Magee, L.; Kramer, M.S.; Liston, R.M.; Joseph, K.S. Hypertensive disorders of pregnancy and the recent increase in obstetric acute renal failure in Canada: Population based retrospective cohort study. BMJ 2014, 349, g4731. [Google Scholar] [CrossRef]
- Mehrabadi, A.; Dahhou, M.; Joseph, K.S.; Kramer, M.S. Investigation of a Rise in Obstetric Acute Renal Failure in the United States, 1999–2011. Obs. Gynecol. 2016, 127, 899–906. [Google Scholar] [CrossRef]
- Lunn, M.R.; Obedin-Maliver, J.; Hsu, C.-Y. Increasing Incidence of Acute Kidney Injury: Also a Problem in Pregnancy? Am. J. Kidney Dis. 2015, 65, 650–654. [Google Scholar] [CrossRef]
- Liu, Y.-M.; Bao, H.-D.; Jiang, Z.-Z.; Huang, Y.-J.; Wang, N.-S. Pregnancy-related Acute Kidney Injury and a Review of the Literature in China. Int. Med. 2015, 54, 1695–1703. [Google Scholar] [CrossRef] [Green Version]
- Mahesh, E.; Puri, S.; Varma, V.; Madhyastha, P.R.; Bande, S.; Gurudev, K.C. Pregnancy-related acute kidney injury: An analysis of 165 cases. Indian J. Nephrol. 2017, 27, 113–117. [Google Scholar] [CrossRef]
- Prakash, J.; Pant, P.; Prakash, S.; Sivasankar, M.; Vohra, R.; Doley, P.K.; Pandey, L.K.; Singh, U. Changing picture of acute kidney injury in pregnancy: Study of 259 cases over a period of 33 years. Indian J. Nephrol. 2016, 26, 262–267. [Google Scholar] [CrossRef]
- Arrayhani, M.; El Youbi, R.; Sqalli, T. Pregnancy-related acute kidney injury: Experience of the nephrology unit at the university hospital of Fez, Morocco. ISRN Nephrol. 2013, 2013, 109034. [Google Scholar] [CrossRef]
- Hildebrand, A.M.; Liu, K.; Shariff, S.Z.; Ray, J.G.; Sontrop, J.M.; Clark, W.F.; Hladunewich, M.A.; Garg, A.X. Characteristics and Outcomes of AKI Treated with Dialysis during Pregnancy and the Postpartum Period. J. Am. Soc. Nephrol. 2015, 26, 3085–3091. [Google Scholar] [CrossRef] [Green Version]
- Fakhouri, F.; Vercel, C.; Frémeaux-Bacchi, V. Obstetric Nephrology: AKI and Thrombotic Microangiopathies in Pregnancy. Clin. J. Am. Soc. Nephrol. 2012, 7, 2100–2106. [Google Scholar] [CrossRef] [Green Version]
- Jim, B.; Garovic, V.D. Acute Kidney Injury in Pregnancy. Semin. Nephrol. 2017, 37, 378–385. [Google Scholar] [CrossRef]
- Liu, Y.; Ma, X.; Liu, X.; Yan, T.; Zheng, J. A Systematic Review and Meta-Analysis of Kidney and Pregnancy Outcomes in IgA Nephropathy. Am. J. Nephrol. 2016, 44, 187–193. [Google Scholar] [CrossRef]
- Prakash, J.; Vohra, R.; Wani, I.A.; Murthy, A.S.; Srivastva, P.K.; Tripathi, K.; Pandey, L.K.; Usha Raja, R. Decreasing incidence of renal cortical necrosis in patients with acute renal failure in developing countries: A single-centre experience of 22 years from Eastern India. Nephrol. Dial. Transpl. 2007, 22, 1213–1217. [Google Scholar] [CrossRef]
- Davidson, N.L.; Wolski, P.; Callaway, L.K.; Barrett, H.L.; Fagermo, N.; Lust, K.; Shakhovskoy, R.E. Chronic kidney disease in pregnancy: Maternal and fetal outcomes and progression of kidney disease. Obs. Med. 2015, 8, 92–98. [Google Scholar] [CrossRef]
- Rahman, M.; Shad, F.; Smith, M.C. Acute kidney injury: A guide to diagnosis and management. Am. Fam. Phys. 2012, 86, 631–639. [Google Scholar]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Johnson, E.B.; Krambeck, A.E.; White, W.M.; Hyams, E.; Beddies, J.; Marien, T.; Shah, O.; Matlaga, B.; Pais, V.M. Obstetric Complications of Ureteroscopy During Pregnancy. J. Urol. 2012, 188, 151–154. [Google Scholar] [CrossRef]
- Valovska, M.-T.I.; Pais, V.M., Jr. Contemporary best practice urolithiasis in pregnancy. Adv. Urol. 2018, 10, 127–138. [Google Scholar] [CrossRef] [Green Version]
- Blanco, L.T.; Socarras, M.R.; Montero, R.F.; Diez, E.L.; Calvo, A.O.; Gregorio, S.A.Y.; Ramón Cansino, J.; Antonio Galan, J.; Gómez Rivas, J. Renal colic during pregnancy: Diagnostic and therapeutic aspects. Literature review. Cent. Eur. J. Urol. 2017, 70, 93–100. [Google Scholar]
- Park, J.; Gage, B.F.; Vijayan, A. Use of EPO in Critically Ill Patients with Acute Renal Failure Requiring Renal Replacement Therapy. Am. J. Kidney Dis. 2005, 46, 791–798. [Google Scholar] [CrossRef]
- Powell-Tuck, J.; Crichton, S.; Raimundo, M.; Camporota, L.; Wyncoll, D.; Ostermann, M. Anaemia is not a risk factor for progression of acute kidney injury: A retrospective analysis. Crit. Care 2016, 20, 1411. [Google Scholar] [CrossRef]
- Grams, M.E.; Estrella, M.M.; Coresh, J.; Brower, R.G.; Liu, K.D. Fluid Balance, Diuretic Use, and Mortality in Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2011, 6, 966–973. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Delaney, A.; Haase, M.; A Ghali, W.; Bellomo, R. Loop diuretics in the management of acute renal failure: A systematic review and meta-analysis. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2007, 9, 60. [Google Scholar]
- Ho, K.M.; Sheridan, D.J. Meta-analysis of frusemide to prevent or treat acute renal failure. BMJ 2006, 333, 420. [Google Scholar] [CrossRef]
- Anthony, J.; Schoeman, L.K. Fluid management in pre-eclampsia. Obs. Med. 2013, 6, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P. Updates in hyperkalemia: Outcomes and therapeutic strategies. Rev. Endocr. Metab. Disord. 2017, 18, 41–47. [Google Scholar] [CrossRef]
- Vijayakumar, S.; Butler, J.; Anker, S.D. New treatments for hyperkalaemia: Clinical use in cardiology. Eur. Hear. J. Suppl. 2019, 21, A41–A47. [Google Scholar] [CrossRef]
- Shaman, A.M.; Kowalski, S.R. Hyperphosphatemia Management in Patients with Chronic Kidney Disease. Saudi Pharm. J. 2016, 24, 494–505. [Google Scholar] [CrossRef]
- Hewitt, J.; Uniacke, M.; Hansi, N.K.; Venkat-Raman, G.; McCarthy, K. Sodium bicarbonate supplements for treating acute kidney injury. Cochrane Database Syst. Rev. 2012, 6, Cd009204. [Google Scholar] [CrossRef]
- Druml, W. Nutritional management of acute renal failure. J. Ren. Nutr. 2005, 15, 63–70. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Maggiore, U.; Cabassi, A.; Morabito, S.; Castellano, G.; Regolisti, G. Nutritional Evaluation and Management of AKI Patients. J. Ren. Nutr. 2013, 23, 255–258. [Google Scholar] [CrossRef]
- Tangren, J.; Nadel, M.; Hladunewich, M.A. Pregnancy and End-Stage Renal Disease. Blood Purif. 2018, 45, 194–200. [Google Scholar] [CrossRef]
- Hladunewich, M.; Schatell, D. Intensive dialysis and pregnancy. Hemodial. Int. 2016, 20, 339–348. [Google Scholar] [CrossRef]
- Gopalakrishnan, N.; Dhanapriya, J.; Muthukumar, P.; Sakthirajan, R.; Dineshkumar, T.; Thirumurugan, S.; Balasubramaniyan, T. Acute kidney injury in pregnancy—a single center experience. Ren. Fail. 2015, 37, 1476–1480. [Google Scholar] [CrossRef]
- Prakash, J.; Ganiger, V.C.; Prakash, S.; Iqbal, M.; Kar, D.P.; Singh, U.; Verma, A. Acute kidney injury in pregnancy with special reference to pregnancy-specific disorders: A hospital based study (2014–2016). J. Nephrol. 2018, 31, 79–85. [Google Scholar] [CrossRef]
- Gabra, A. Updates in Management of Hyperemesis Gravidarum. Crit. Care Obs. Gynecol. 2018, 4. [Google Scholar] [CrossRef]
- Hill, J. Acute renal failure in association with severe hyperemesis gravidarum. Obs. Gynecol. 2002, 100, 1119–1121. [Google Scholar]
- Chatwani, A.; Schwartz, R. A severe case of hyperemesis gravidarum. Am. J. Obs. Gynecol. 1982, 143, 964–965. [Google Scholar] [CrossRef]
- Abou Arkoub, R.; Xiao, C.W.; Claman, P.; Clark, E.G. Acute Kidney Injury Due to Ovarian Hyperstimulation Syndrome. Am. J. Kidney Dis. 2019, 73, 416–420. [Google Scholar] [CrossRef]
- Soares, S.R. Etiology of OHSS and use of dopamine agonists. Fertil. Steril. 2012, 97, 517–522. [Google Scholar] [CrossRef]
- Shim, S.M.; Ryu, A.L.; Kim, Y.S. Acute Kidney Injury Arising from Severe Hyperemesis Gravidarum: Case Report with a Review of Literatures. Soonchunhyang Med. Sci. 2015, 21, 28–30. [Google Scholar] [CrossRef]
- Rahman, S.G.R.; Islam, N.; Das, A.; Shaha, A.; Khan, M.; Rahman, M. Pregnancy Related Acute Renal Failure in a Tertiary Care Hospital in Bangladesh. J. Med. 2012, 13, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Hanif, M.O.; Ramphul, K. Acute Renal Tubular Necrosis StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507815/ (accessed on 2 September 2019).
- Dawkins, J.C.; Fletcher, H.M.; Rattray, C.A.; Reid, M.; Gordon-Strachan, G. Acute Pyelonephritis in Pregnancy: A Retrospective Descriptive Hospital Based-Study. ISRN Obs. Gynecol. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.B.; Sheffield, J.S.; McIntire, D.D.; Wendel, G.D., Jr. Acute pyelonephritis in pregnancy. Obstet. Gynecol. 2005, 105, 18–23. [Google Scholar] [CrossRef]
- Tandogdu, Z.; Johansen, T.E.B.; Bartoletti, R.; Wagenlehner, F.; Johansen, T.E.B. Management of the Urologic Sepsis Syndrome. Eur. Urol. Suppl. 2016, 15, 102–111. [Google Scholar] [CrossRef]
- Sqalli, T.H.; Hamzaoui, H.; Guiard, E.; Noel, L.-H.; Fakhouri, F. Severe renal failure in acute bacterial pyelonephritis: Do not forget corticosteroids. Saudi J. Kidney Dis. Transpl. 2010, 21, 118–122. [Google Scholar]
- Prakash, J.; Ganiger, V.C. Acute Kidney Injury in Pregnancy-specific Disorders. Indian J. Nephrol. 2017, 27, 258–270. [Google Scholar] [CrossRef]
- Sahay, M.; Swain, M.; Padua, M. Renal cortical necrosis in tropics. Saudi J. Kidney Dis. Transpl. 2013, 24, 725–730. [Google Scholar] [CrossRef]
- Frimat, M.; Decambron, M.; LeBas, C.; Moktefi, A.; Lemaitre, L.; Gnemmi, V.; Sautenet, B.; Glowacki, F.; Subtil, D.; Jourdain, M.; et al. Renal Cortical Necrosis in Postpartum Hemorrhage: A Case Series. Am. J. Kidney Dis. 2016, 68, 50–57. [Google Scholar] [CrossRef]
- Ali, A.; Ali, M.A.; Ali, M.U. Obstetrical associated renal, cortical necrosis: Uncommon but not rare! J. Ayub. Med. Colleg. 2010, 22, 74–76. [Google Scholar]
- Beji, S.; Hajji, M.; Rais, L.; Kheder, R.; Jebali, H.; Smaoui, W.; Krid, M.; Ben Hamida, F.; Ben Fatma, L.; Zouaghi, M.K. Acute renal cortical necrosis in pregnancy: Clinical course and changing prognosis. Néphrol. Thér. 2017, 13, 550–552. [Google Scholar] [CrossRef]
- Huang, C.-C.; Huang, J.-K. Sepsis-induced acute bilateral renal cortical necrosis. Nephrology 2011, 16, 787. [Google Scholar] [CrossRef]
- Arnold, D.M.; Patriquin, C.J.; Nazy, I. Thrombotic microangiopathies: A general approach to diagnosis and management. CMAJ 2017, 189, E153–E159. [Google Scholar] [CrossRef]
- Stella, C.L.; Dacus, J.; Guzman, E.; Dhillon, P.; Coppage, K.; How, H.; Sibai, B. The diagnostic dilemma of thrombotic thrombocytopenic purpura/hemolytic uremic syndrome in the obstetric triage and emergency department: Lessons from 4 tertiary hospitals. Am. J. Obs. Gynecol. 2009, 200, 381.e1–381.e6. [Google Scholar] [CrossRef]
- Gupta, M.; Feinberg, B.; Burwick, R. Thrombotic microangiopathies of pregnancy: Differential diagnosis. Pregnancy Hypertens. 2018, 12, 29–34. [Google Scholar] [CrossRef]
- Kappler, S.; Ronan-Bentle, S.; Graham, A. Thrombotic microangiopathies (TTP, HUS, HELLP). Emerg. Med. Clin. N. Am. 2014, 32, 649–671. [Google Scholar] [CrossRef]
- Fakhouri, F.; Roumenina, L.; Provot, F.; Sallée, M.; Caillard, S.; Couzi, L.; Essig, M.; Ribes, D.; Dragon-Durey, M.-A.; Bridoux, F.; et al. Pregnancy-Associated Hemolytic Uremic Syndrome Revisited in the Era of Complement Gene Mutations. J. Am. Soc. Nephrol. 2010, 21, 859–867. [Google Scholar] [CrossRef] [Green Version]
- Noris, M.; Caprioli, J.; Bresin, E.; Mossali, C.; Pianetti, G.; Gamba, S.; Daina, E.; Fenili, C.; Castelletti, F.; Sorosina, A.; et al. Relative Role of Genetic Complement Abnormalities in Sporadic and Familial aHUS and Their Impact on Clinical Phenotype. Clin. J. Am. Soc. Nephrol. 2010, 5, 1844–1859. [Google Scholar] [CrossRef]
- Loirat, C.; Frémeaux-Bacchi, V. Atypical hemolytic uremic syndrome. Orphanet. J. Rare Dis. 2011, 6, 1676–1687. [Google Scholar] [CrossRef]
- Wong, E.K.; Goodship, T.H.; Kavanagh, D. Complement therapy in atypical haemolytic uraemic syndrome (aHUS). Mol. Immunol. 2013, 56, 199–212. [Google Scholar] [CrossRef]
- Huerta, A.; Arjona, E.; Rabasco, C.; Cavero, T.; Cao, M.; Manrique, J.; Cabello-Chavez, V.; Suñer, M.; Heras, M.; Fulladosa, X.; et al. A retrospective study of pregnancy-associated atypical hemolytic uremic syndrome. Kidney Int. 2018, 93, 450–459. [Google Scholar] [CrossRef]
- Pereira, B.J.; Barreto, S.; Gentil, T.; Assis, L.S.; Soeiro, E.M.; De Castro, I.; Laranja, S.M. Risk factors for the progression of chronic kidney disease after acute kidney injury. Braz. J. Nephrol. 2017, 39, 239–245. [Google Scholar] [CrossRef]
- Horne, K.L.; Packington, R.; Monaghan, J.; Reilly, T.; Selby, N.M. Three-year outcomes after acute kidney injury: Results of a prospective parallel group cohort study. BMJ Open 2017, 7, e015316. [Google Scholar] [CrossRef]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef]
- McDonald, S.D.; Han, Z.; Walsh, M.W.; Gerstein, H.C.; Devereaux, P.J. Kidney Disease After Preeclampsia: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2010, 55, 1026–1039. [Google Scholar] [CrossRef]
- Ayansina, D.; Black, C.; Hall, S.; Marks, A.; Millar, C.; Prescott, G.; Wilde, K.; Bhattacharya, S. Long term effects of gestational hypertension and pre-eclampsia on kidney function: Record linkage study. Pregnancy Hypertens. 2016, 6, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Tangren, J.S.; Powe, C.E.; Ankers, E.; Ecker, J.; Bramham, K.; Hladunewich, M.A.; Ananth Karumanchi, S.; Thadhani, R. Pregnancy Outcomes after Clinical Recovery from AKI. JASN 2017, 28, 1566–1574. [Google Scholar] [CrossRef]
- Popkov, V.A.; Andrianova, N.V.; Manskikh, V.N.; Silachev, D.N.; Pevzner, I.B.; Zorova, L.D.; Sukhikh, G.T.; Plotnikov, E.Y.; Zorov, D.B. Pregnancy protects the kidney from acute ischemic injury. Sci. Rep. 2018, 8, 14534. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Moroni, G.; Spotti, D.; Giacchino, F.; Attini, R.; Limardo, M.; et al. A best practice position statement on the role of the nephrologist in the prevention and follow-up of preeclampsia: The Italian study group on kidney and pregnancy. J. Nephrol. 2017, 30, 307–317. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| % Change | Pregnant | Postnatal | |||
|---|---|---|---|---|---|
| 1–20 weeks | 20–30 weeks | 30–40 weeks | 1–6 weeks | >6 weeks | |
| Odutayo and Hladunewich [17] | |||||
| GFR | 37.13 | 38.38 | 39.46 | 24.9 | −0.91 |
| ERPF | 41.18 | 29.44 | 10.37 | −5.13 | −7.49 |
| FF | −1.89 | 10.68 | 29.26 | 24.8 | −1.59 |
| Davison and Dunlop [18] | |||||
| GFR | 48.9 | 45.8 | 51.0 | - | - |
| ERPF | 67.8 | 64.9 | 44.1 | - | - |
| FF | −10.9 | −10.9 | 5.8 | - | - |
| Renal Variable | Non-Pregnant Values | Pregnant Values | Values in Pregnancy that Require Further Investigation |
|---|---|---|---|
| Glomerular filtration rate (GFR) (mL/min) | 106–132 | 130–180 | <115 |
| Effective renal plasma flow (ERPF) (mL/min) | 492–696 | 630–1030 | <590 |
| Filtration Fraction (FF) (%) | 16.9–24.7 | 15.4–22.8 | <14.0 |
| Serum Sodium (mEq/L) | 136–146 | 133–148 | <128 |
| Serum Potassium (mEq/L) | 3.5–5.0 | 3.3–5.0 | >5.1 |
| Serum Chloride (mEq/L) | 102–109 | 97–109 | >110 |
| Serum Bicarbonate (mEq/L) | 27–28 | 20–22 | <20 |
| Plasma osmolality (mOsm/kg H2O) | 275–295 | 276–289 | >290 |
| pH (arterial) | 7.35–7.45 | 7.40–7.45 | <7.36; >7.45 |
| Plasma urate (mg/dL) | 4–6 | 2.5–4 | >5.8 |
| Plasma Creatinine (mg/dL, µmol/L) | 0.51–1.02; (45–90) | 0.59–0.87; (52–77) | >0.87 (77) |
| Creatinine clearance (mL/min) | 91–130 | 110–150 | <90 |
| Blood urea nitrogen (mg/dL) | 13 ± 3 | 8.7 ± 1.5 | >14 |
| Urinary glucose (mg/24 h) | 20–100 | >100 | - |
| Urinary protein (mg/24 h) | <100–150 | <250–300 | >300 |
| Urinary amino acids (g/24 h) | - | ≤2 | >2 |
| AKI Classification Systems | |||||
|---|---|---|---|---|---|
| RIFLE Criteria for Classification/Staging AKI | AKIN Criteria for Classification/Staging AKI | ||||
| Stage | GFR Criteria | Urine Output Criteria | Stage | Serum Creatinine Criteria | Urine Output Criteria |
| Risk | Increase in SCr ×1.5 or Decrease in GFR > 25% | UO < 0.5 mL/kg/h × 6 h | Stage 1 | Increase in SCr ≥ 0.3 mg/dL or Increase SCr ≥ 1.5–2.0 × | UO < 0.5 mL/kg/h × 6 h |
| Injury | Increase in SCr ×2.0 or Decrease in GFR >50% | UO < 0.5mL/kg/h × 12 h | Stage 2 | Increase in SCr > 2.0–3.0 × | UO < 0.5 mL/kg/h × 12 h |
| Failure | Increase in SCr × 3.0 or Decrease in GFR >75% or SCr >4.0 mg/dL (acute increase ≥ 0.5 mg/dL) | UO < 0.3mL/kg/h × 24 h or anuria for 12 h | Stage 3 | Increase in SCr > 3 × or Increase of SCr to ≥4.0 mg/dL with an acute increase of at least 0.5 mg/dL | UO < 0.3 mL/kg/h × 24 h or anuria for 12 h |
| Loss | Persistent ARF: Complete loss of kidney function for >4 weeks | Patients who receive renal replacement therapy (RRT) are considered to have met the criteria for stage 3 irrespective of the stage they were in at the time of commencement of RRT. | |||
| ESKD | End-stage kidney disease for >3 months | ||||
| AKI Classification Systems: KDIGO Criteria | ||
|---|---|---|
| Stage | Serum Creatinine Criteria | Urine Output Criteria |
| Stage 1 | Increase in SCr × 1.5–1.9 or Increase in SCr ≥ 0.3 mg/dL | UO < 0.5 mL/kg/h × 6–12 h |
| Stage 2 | SCr ≥ 2.0–2.9 times baseline | UO < 0.5 mL/kg/h ≥ 12 h |
| Stage 3 | Increase SCr ≥ 3.0 × or Increase in SCr to ≥ 4.0 mg/dL or Initiation of renal replacement therapy (RRT) or In patients < 18 years, decrease in eGFR to <35 mL/min per 1.73 m2 | UO < 0.3 mL/kg/h × ≥24 h or Anuria for ≥ 12 h |
| Pre-Renal | Intrinsic Renal | Post-Renal |
|---|---|---|
| Early Pregnancy | ||
| Bleeding—miscarriage | Anticardiolipin antibody syndrome | Renal stones |
| Hyperemesis gravidarum | Sepsis (i.e., septic abortion) | Ureteral obstruction |
| Ovarian hyperstimulation syndrome | Autoimmune disease | |
| Ectopic pregnancy | Glomerulonephritis, interstitial nephritis, lupus nephritis | |
| CKD progression | ||
| Late Pregnancy | ||
| Bleeding—second-trimester miscarriage, placenta praevia, placental abruption | Severe pre-eclampsia, HELLP | Polyhydramnios |
| Acute fatty liver of pregnancy | Multifetal gestation | |
| HUS/TTP | Large uterine fibroids | |
| Pyelonephritis | Ureteral obstruction | |
| Chorioamnionitis | Renal stones | |
| CKD Progression | ||
| Glomerulonephritis, interstitial nephritis, lupus nephritis | ||
| Postpartum | ||
| Bleeding—uterine atonia, uterine rupture, obstetrical trauma (vulvo-vaginal and perineal tears and lacerations) | Severe pre-eclampsia, HELLP | Renal stones |
| HUS | ||
| Puerperal sepsis | ||
| Glomerulonephritis, interstitial nephritis, lupus nephritis | ||
| Nephrotoxic drugs (NSAIDS, antibiotics, proton-pump inhibitors, H2 antagonists) | ||
| CKD Progression |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinturache, A.; Popoola, J.; Watt-Coote, I. The Changing Landscape of Acute Kidney Injury in Pregnancy from an Obstetrics Perspective. J. Clin. Med. 2019, 8, 1396. https://doi.org/10.3390/jcm8091396
Vinturache A, Popoola J, Watt-Coote I. The Changing Landscape of Acute Kidney Injury in Pregnancy from an Obstetrics Perspective. Journal of Clinical Medicine. 2019; 8(9):1396. https://doi.org/10.3390/jcm8091396
Chicago/Turabian StyleVinturache, Angela, Joyce Popoola, and Ingrid Watt-Coote. 2019. "The Changing Landscape of Acute Kidney Injury in Pregnancy from an Obstetrics Perspective" Journal of Clinical Medicine 8, no. 9: 1396. https://doi.org/10.3390/jcm8091396
APA StyleVinturache, A., Popoola, J., & Watt-Coote, I. (2019). The Changing Landscape of Acute Kidney Injury in Pregnancy from an Obstetrics Perspective. Journal of Clinical Medicine, 8(9), 1396. https://doi.org/10.3390/jcm8091396