Incidence of Anaplastic Large Cell Lymphoma and Breast-Implant-Associated Lymphoma—An Analysis of a Certified Tumor Registry over 17 Years


 and
and
Abstract
1. Introduction
2. Materials and Methods
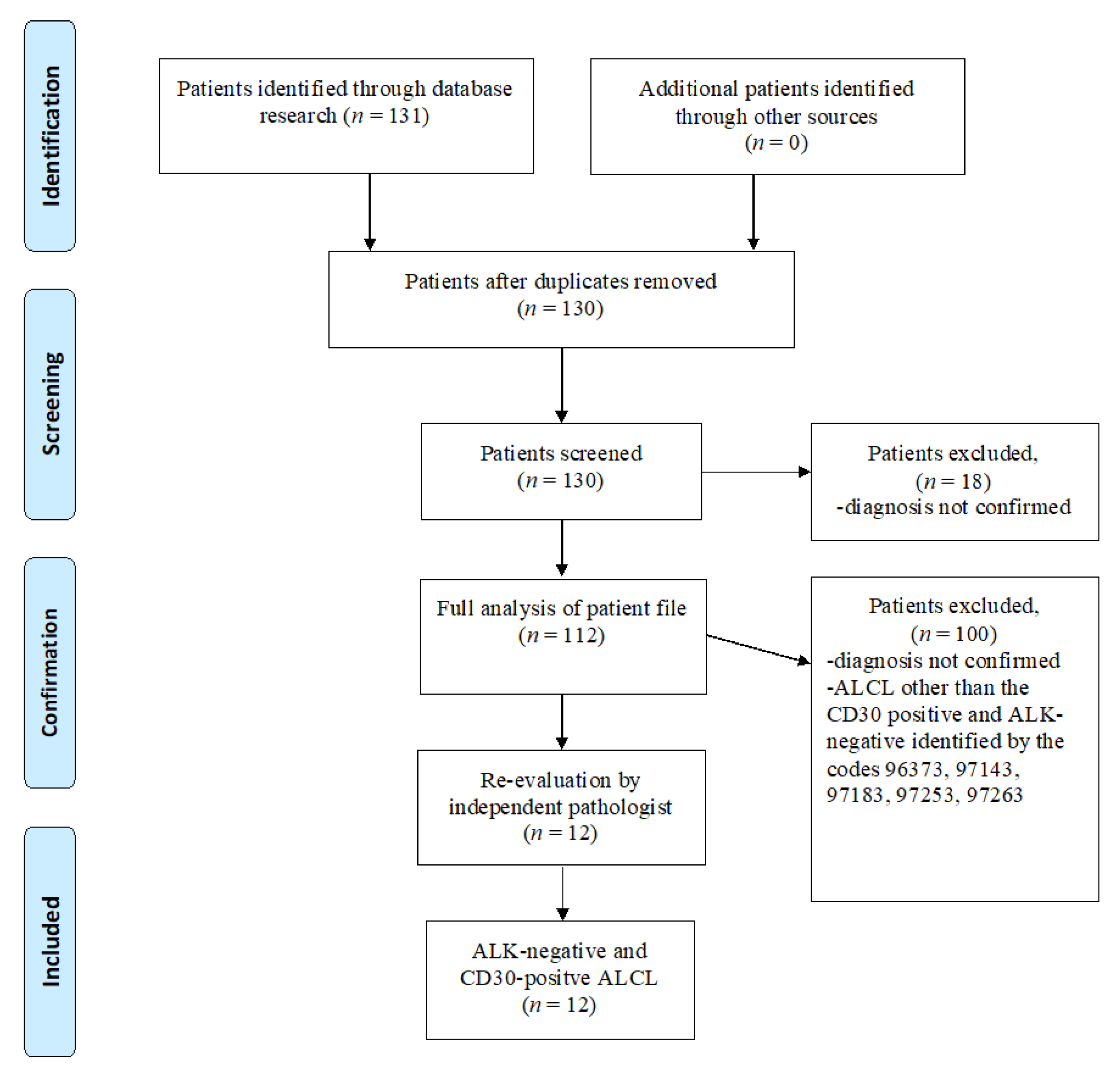
2.1. Study Design
2.2. Data Base and Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Descriptive Data
3.2. Incidence in the Regensburg Data Set
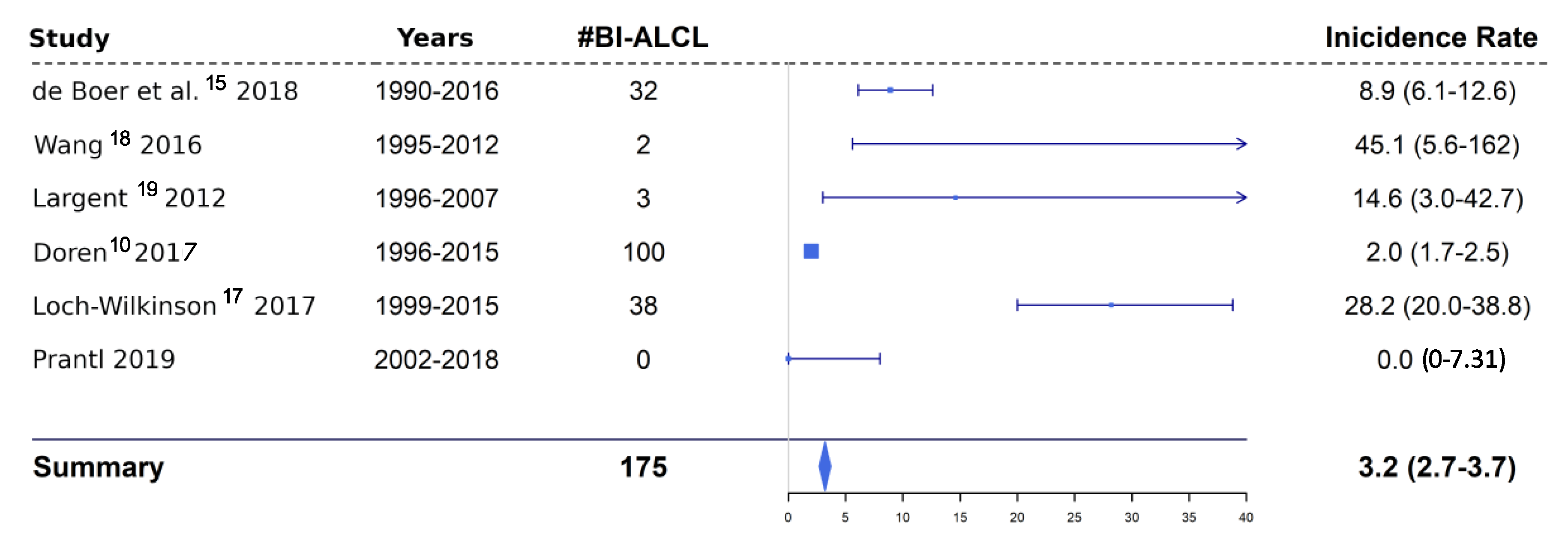
3.3. Incidence in Comparison Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Miranda, R.N.; Medeiros, L.J.; Ferrufino-Schmidt, M.C.; Keech, J.A., Jr.; Brody, G.S.; de Jong, D.; Dogan, A.; Clemens, M.W. Pioneers of Breast Implant-Associated Anaplastic Large Cell Lymphoma: History from Case Report to Global Recognition. Plast. Reconstr. Surg. 2019, 143, 7S–14S. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.J. Silicone breast implants not linked to breast cancer risk. J. Natl. Cancer Inst. 2000, 92, 1714–1715. [Google Scholar] [CrossRef] [PubMed]
- Keech, J.A., Jr.; Creech, B.J. Anaplastic T-cell lymphoma in proximity to a saline-filled breast implant. Plast. Reconstr. Surg. 1997, 100, 554–555. [Google Scholar] [CrossRef] [PubMed]
- Radkani, P.; Joshi, D.; Paramo, J.C.; Mesko, T.W. Primary breast lymphoma: 30 years of experience with diagnosis and treatment at a single medical center. JAMA Surg. 2014, 149, 91–93. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef]
- Collett, D.J.; Rakhorst, H.; Lennox, P.; Magnusson, M.; Cooter, R.; Deva, A.K. Current Risk Estimate of Breast Implant-Associated Anaplastic Large Cell Lymphoma in Textured Breast Implants. Plast. Reconstr. Surg. 2019, 143, 30S–40S. [Google Scholar] [CrossRef]
- Kricheldorff, J.; Fallenberg, E.M.; Solbach, C.; Gerber-Schafer, C.; Rancso, C.; Fritschen, U.V. Breast Implant-Associated Lymphoma. Dtsch. Arztebl. Int. 2018, 115, 628–635. [Google Scholar] [CrossRef]
- Brody, G.S.; Deapen, D.; Taylor, C.R.; Pinter-Brown, L.; House-Lightner, S.R.; Andersen, J.S.; Carlson, G.; Lechner, M.G.; Epstein, A.L. Anaplastic large cell lymphoma occurring in women with breast implants: Analysis of 173 cases. Plast. Reconstr. Surg. 2015, 135, 695–705. [Google Scholar] [CrossRef]
- Miranda, R.N.; Aladily, T.N.; Prince, H.M.; Kanagal-Shamanna, R.; de Jong, D.; Fayad, L.E.; Amin, M.B.; Haideri, N.; Bhagat, G.; Brooks, G.S.; et al. Breast implant-associated anaplastic large-cell lymphoma: Long-term follow-up of 60 patients. J. Clin. Oncol. 2014, 32, 114–120. [Google Scholar] [CrossRef]
- Doren, E.L.; Miranda, R.N.; Selber, J.C.; Garvey, P.B.; Liu, J.; Medeiros, L.J.; Butler, C.E.; Clemens, M.W. U.S. Epidemiology of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Plast. Reconstr. Surg. 2017, 139, 1042–1050. [Google Scholar] [CrossRef]
- Gholam, D.; Bibeau, F.; El Weshi, A.; Bosq, J.; Ribrag, V. Primary breast lymphoma. Leuk. Lymphoma 2003, 44, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Leberfinger, A.N.; Behar, B.J.; Williams, N.C.; Rakszawski, K.L.; Potochny, J.D.; Mackay, D.R.; Ravnic, D.J. Breast Implant-Associated Anaplastic Large Cell Lymphoma: A Systematic Review. JAMA Surg. 2017, 152, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Lortet-Tieulent, J.; Ferlay, J.; Bray, F.; Jemal, A. International Patterns and Trends in Endometrial Cancer Incidence, 1978–2013. J. Natl. Cancer Inst. 2018, 110, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Kinslow, C.J.; Hibshoosh, H.; Guo, H.; Cheng, S.K.; He, C.; Gentry, M.S.; Sun, R.C. Clinical Features, Survival and Prognostic Factors of Glycogen-Rich Clear Cell Carcinoma (GRCC) of the Breast in the U.S. Population. J. Clin. Med. 2019, 8, 246. [Google Scholar] [CrossRef]
- De Boer, M.; van Leeuwen, F.E.; Hauptmann, M.; Overbeek, L.I.H.; de Boer, J.P.; Hijmering, N.J.; Sernee, A.; Klazen, C.A.H.; Lobbes, M.B.I.; van der Hulst, R.; et al. Breast Implants and the Risk of Anaplastic Large-Cell Lymphoma in the Breast. JAMA Oncol. 2018, 4, 335–341. [Google Scholar] [CrossRef]
- De Jong, D.; Vasmel, W.L.; de Boer, J.P.; Verhave, G.; Barbe, E.; Casparie, M.K.; van Leeuwen, F.E. Anaplastic large-cell lymphoma in women with breast implants. JAMA 2008, 300, 2030–2035. [Google Scholar] [CrossRef]
- Loch-Wilkinson, A.; Beath, K.J.; Knight, R.J.W.; Wessels, W.L.F.; Magnusson, M.; Papadopoulos, T.; Connell, T.; Lofts, J.; Locke, M.; Hopper, I.; et al. Breast Implant-Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand: High-Surface-Area Textured Implants Are Associated with Increased Risk. Plast. Reconstr. Surg. 2017, 140, 645–654. [Google Scholar] [CrossRef]
- Wang, S.S.; Deapen, D.; Voutsinas, J.; Lacey, J.V., Jr.; Lu, Y.; Ma, H.; Clarke, C.A.; Weisenburger, D.; Forman, S.J.; Bernstein, L. Breast implants and anaplastic large cell lymphomas among females in the California Teachers Study cohort. Br. J. Haematol. 2016, 174, 480–483. [Google Scholar] [CrossRef]
- Largent, J.; Oefelein, M.; Kaplan, H.M.; Okerson, T.; Boyle, P. Risk of lymphoma in women with breast implants: Analysis of clinical studies. Eur. J. Cancer Prev. 2012, 21, 274–280. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Bavarian Federal Statistical Office. Available online: https://www.statistik.bayern.de/ (accessed on 12 December 2019).
- (StBA), G.F.S.O. Available online: https://www.destatis.de/TablecountryprofileNetherlands (accessed on 15 November 2019).
- Lorthiois, E.; Anderson, K.; Vulpetti, A.; Rogel, O.; Cumin, F.; Ostermann, N.; Steinbacher, S.; Mac Sweeney, A.; Delgado, O.; Liao, S.M.; et al. Discovery of Highly Potent and Selective Small-Molecule Reversible Factor D Inhibitors Demonstrating Alternative Complement Pathway Inhibition in Vivo. J. Med. Chem. 2017, 60, 5717–5735. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.M.; Loyo-Berrios, N.; Qureshi, A.A.; Mullen, E.; Gordillo, G.; Pusic, A.L.; Ashar, B.S.; Sommers, K.; Clemens, M.W. Patient Registry and Outcomes for Breast Implants and Anaplastic Large Cell Lymphoma Etiology and Epidemiology (PROFILE): Initial Report of Findings, 2012–2018. Plast. Reconstr. Surg. 2019, 143, 65S–73S. [Google Scholar] [CrossRef] [PubMed]
- Mendes, J., Jr.; Mendes Maykeh, V.A.; Frascino, L.F.; Zacchi, F.F.S. Gluteal Implant-Associated Anaplastic Large Cell Lymphoma. Plast. Reconstr. Surg. 2019, 144, 610–613. [Google Scholar] [CrossRef]
- Magnusson, M.; Beath, K.; Cooter, R.; Locke, M.; Prince, H.M.; Elder, E.; Deva, A.K. The Epidemiology of Breast Implant-Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand Confirms the Highest Risk for Grade 4 Surface Breast Implants. Plast. Reconstr. Surg. 2019, 143, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Tandon, V.J.; DeLong, M.R.; Ballard, T.N.; Clemens, M.W.; Brandt, K.E.; Kenkel, J.M.; Cederna, P.S. Evolving Trends in Textured Implant Use for Cosmetic Augmentation in the United States. Plast. Reconstr. Surg. 2018, 142, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Kuehlmann, B.; Prantl, L. Breast implants and possible association with ALCL: A retrospective study including a histological analysis of 296 explanted breast tissues and current literature. Clin. Hemorheol. Microcirc. 2016, 63, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Link, B.K.; Altekruse, S.; Romitti, P.A.; Schroeder, M.C. Primary Breast Lymphoma in the United States: 1975–2013. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Cao, Y.B.; Wang, S.S.; Huang, H.Q.; Xu, G.C.; He, Y.J.; Guan, Z.Z.; Lin, T.Y. Primary breast lymphoma—A report of 27 cases with literature review. Ai Zheng 2007, 26, 84–89. [Google Scholar]
- Blombery, P.; Prince, H.M.; Seymour, J.F. Primary Breast Lymphoma-Population-Level Insights into an Infrequent but Increasingly Recognized Subtype of Lymphoma. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Altekruse, S.F.; Kosary, C.L.; Krapcho, M.; Neyman, N.; Aminou, R.; Waldron, W.; Ruhl, J.; Howlader, N.; Tatalovich, Z.; Cho, H.; et al. SEER Cancer Statistics Review, 1975–2007; Table 19.28, Based on November 2009 SEER Data Submission; National Cancer Institute: Bethesda, MD, USA, 2009. Available online: http://seer.cancer.gov/csr/1975_2007/ (accessed on 22 November 2019).
- Blombery, P.; Thompson, E.R.; Prince, H.M. Molecular Drivers of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Plast. Reconstr. Surg. 2019, 143, 59S–64S. [Google Scholar] [CrossRef]
- King, R.L.; Dao, L.N.; McPhail, E.D.; Jaffe, E.S.; Said, J.; Swerdlow, S.H.; Sattler, C.A.; Ketterling, R.P.; Sidhu, J.S.; Hsi, E.D.; et al. Morphologic Features of ALK-negative Anaplastic Large Cell Lymphomas with DUSP22 Rearrangements. Am. J. Surg. Pathol. 2016, 40, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Stuttgen, K.; Croessmann, S.; Fetting, J.; Stearns, V.; Nunes, R.; Connolly, R.M.; Park, B.H. Pathogenic Germline Variants in Patients With Metastatic Breast Cancer. JAMA Oncol. 2019, 5, 1506–1508. [Google Scholar] [CrossRef] [PubMed]
- Devin, J.; Kassambara, A.; Bruyer, A.; Moreaux, J.; Bret, C. Phenotypic Characterization of Diffuse Large B-Cell Lymphoma Cells and Prognostic Impact. J. Clin. Med. 2019, 8, 1074. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.M.; Horwitz, S.M. Association of Breast Implants With Anaplastic Large-Cell Lymphoma. JAMA Oncol. 2018, 4, 341–342. [Google Scholar] [CrossRef]
- Young-Afat, D.A. Risk of Breast Implant-Associated Anaplastic Large Cell Lymphoma. JAMA Oncol. 2018, 4, 1434–1435. [Google Scholar] [CrossRef]
- Roberts, J.M.; Carr, L.W.; Jones, A.; Schilling, A.; Mackay, D.R.; Potochny, J.D. A Prospective Approach to Inform and Treat 1340 Patients at Risk for BIA-ALCL. Plast. Reconstr. Surg. 2019, 144, 46–54. [Google Scholar] [CrossRef]
- Prantl, L.; von Fritschen, U.; Liebau, J.; von Hassel, J.; Baur, E.M.; Vogt, P.M.; Giunta, R.E.; Horch, R.E. Concept for a National Implant Registry to Improve Patient Safety. Handchir. Mikrochir. Plast. Chir. 2016, 48, 320–329. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Year of Diagnosis | 9702/3-ALK-Negativ, CD30-Positive | PTCL: ALK-Positive ALCL, ALCL T and Null Cell Types, ALCL not Specified and without T- and B-Cell Markers, Primary Cutaneous ALCL | C00 to C97 except C44 |
|---|---|---|---|
| 2002 | 0 | 6 | 8031 |
| 2003 | 0 | 6 | 8496 |
| 2004 | 0 | 7 | 9909 |
| 2005 | 0 | 4 | 9889 |
| 2006 | 0 | 5 | 9824 |
| 2007 | 0 | 6 | 10,203 |
| 2008 | 0 | 7 | 10,427 |
| 2009 | 0 | 5 | 10,700 |
| 2010 | 0 | 7 | 10,801 |
| 2011 | 1 | 6 | 10,369 |
| 2012 | 0 | 8 | 10,939 |
| 2013 | 0 | 9 | 11,232 |
| 2014 | 2 | 9 | 11,131 |
| 2015 | 3 | 4 | 11,098 |
| 2016 | 4 | 5 | 11,189 |
| 2017 | 1 | 4 | 10,705 |
| 2018 | 1 | 2 | 5350 |
| Total No. (%) | 12 (0.007) | 100 (0.05) | 170,293 (99.94) |
| ICD-10 | No. of Cases |
|---|---|
| C82 Follicular lymphoma | 4 |
| C83 Non-follicular lymphoma | 15 |
| C84 Mature T/NK-cell lymphomas | 0 |
| C85 Other and unspecified types of non-Hodgkin lymphoma | 2 |
| C50 primary breast cancer | 25,897 |
| Total No. | 25,918 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prantl, L.; Gerken, M.; Zeman, F.; Leitzmann, M.; Koller, M.; Klinkhammer-Schalke, M.; Evert, M.; Kuehlmann, B.; Biermann, N. Incidence of Anaplastic Large Cell Lymphoma and Breast-Implant-Associated Lymphoma—An Analysis of a Certified Tumor Registry over 17 Years. J. Clin. Med. 2020, 9, 1247. https://doi.org/10.3390/jcm9051247
Prantl L, Gerken M, Zeman F, Leitzmann M, Koller M, Klinkhammer-Schalke M, Evert M, Kuehlmann B, Biermann N. Incidence of Anaplastic Large Cell Lymphoma and Breast-Implant-Associated Lymphoma—An Analysis of a Certified Tumor Registry over 17 Years. Journal of Clinical Medicine. 2020; 9(5):1247. https://doi.org/10.3390/jcm9051247
Chicago/Turabian StylePrantl, Lukas, Michael Gerken, Florian Zeman, Michael Leitzmann, Michael Koller, Monika Klinkhammer-Schalke, Matthias Evert, Britta Kuehlmann, and Niklas Biermann. 2020. "Incidence of Anaplastic Large Cell Lymphoma and Breast-Implant-Associated Lymphoma—An Analysis of a Certified Tumor Registry over 17 Years" Journal of Clinical Medicine 9, no. 5: 1247. https://doi.org/10.3390/jcm9051247
APA StylePrantl, L., Gerken, M., Zeman, F., Leitzmann, M., Koller, M., Klinkhammer-Schalke, M., Evert, M., Kuehlmann, B., & Biermann, N. (2020). Incidence of Anaplastic Large Cell Lymphoma and Breast-Implant-Associated Lymphoma—An Analysis of a Certified Tumor Registry over 17 Years. Journal of Clinical Medicine, 9(5), 1247. https://doi.org/10.3390/jcm9051247