Significance of NT-proBNP and High-Sensitivity Troponin in Friedreich Ataxia

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Population
2.2. Neurological Evaluation
2.3. Electrocardiogram (ECG)
2.4. Echocardiography
2.5. Blood Assays
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Population
3.1.1. ECG
3.1.2. Echocardiography
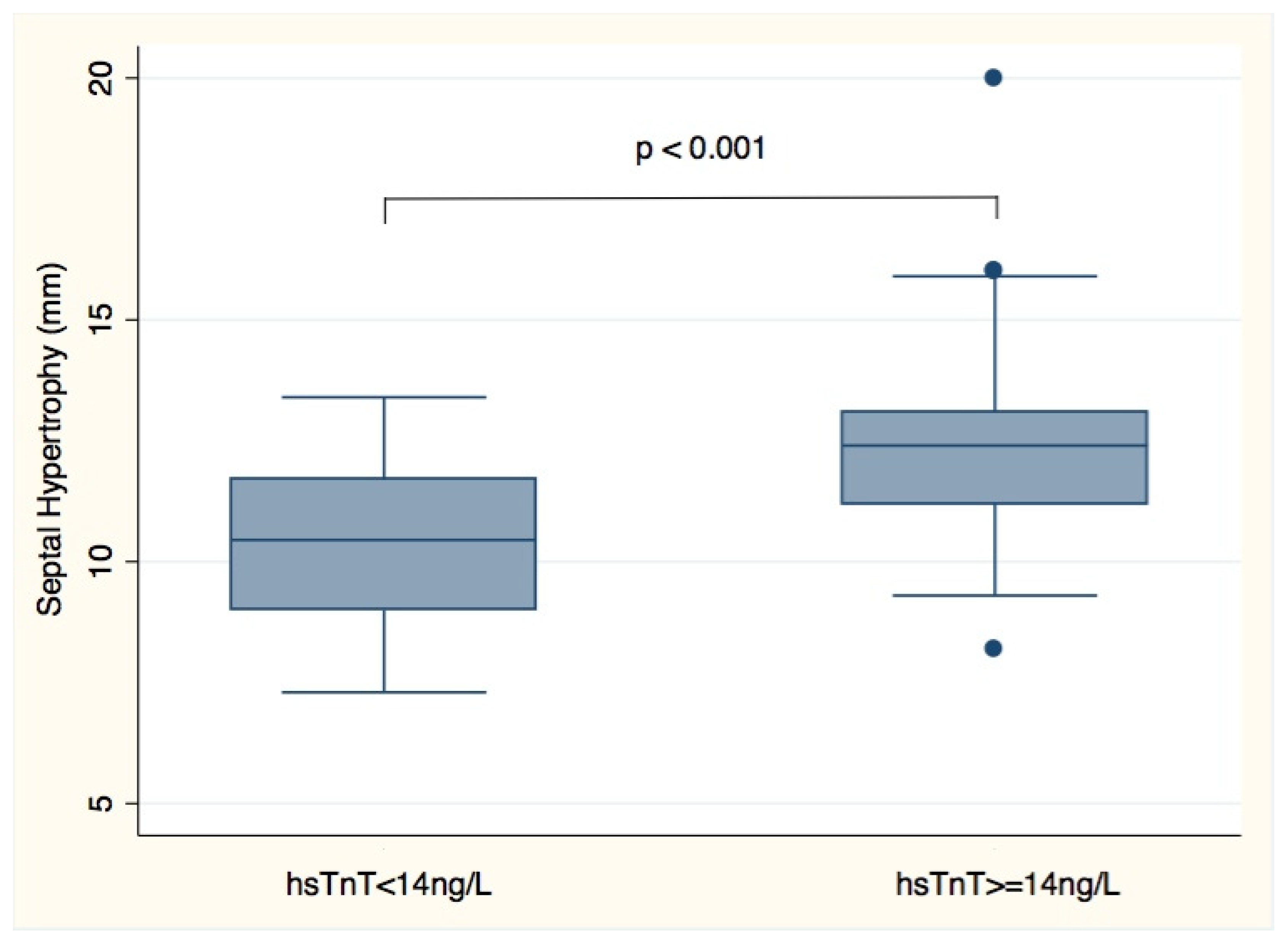
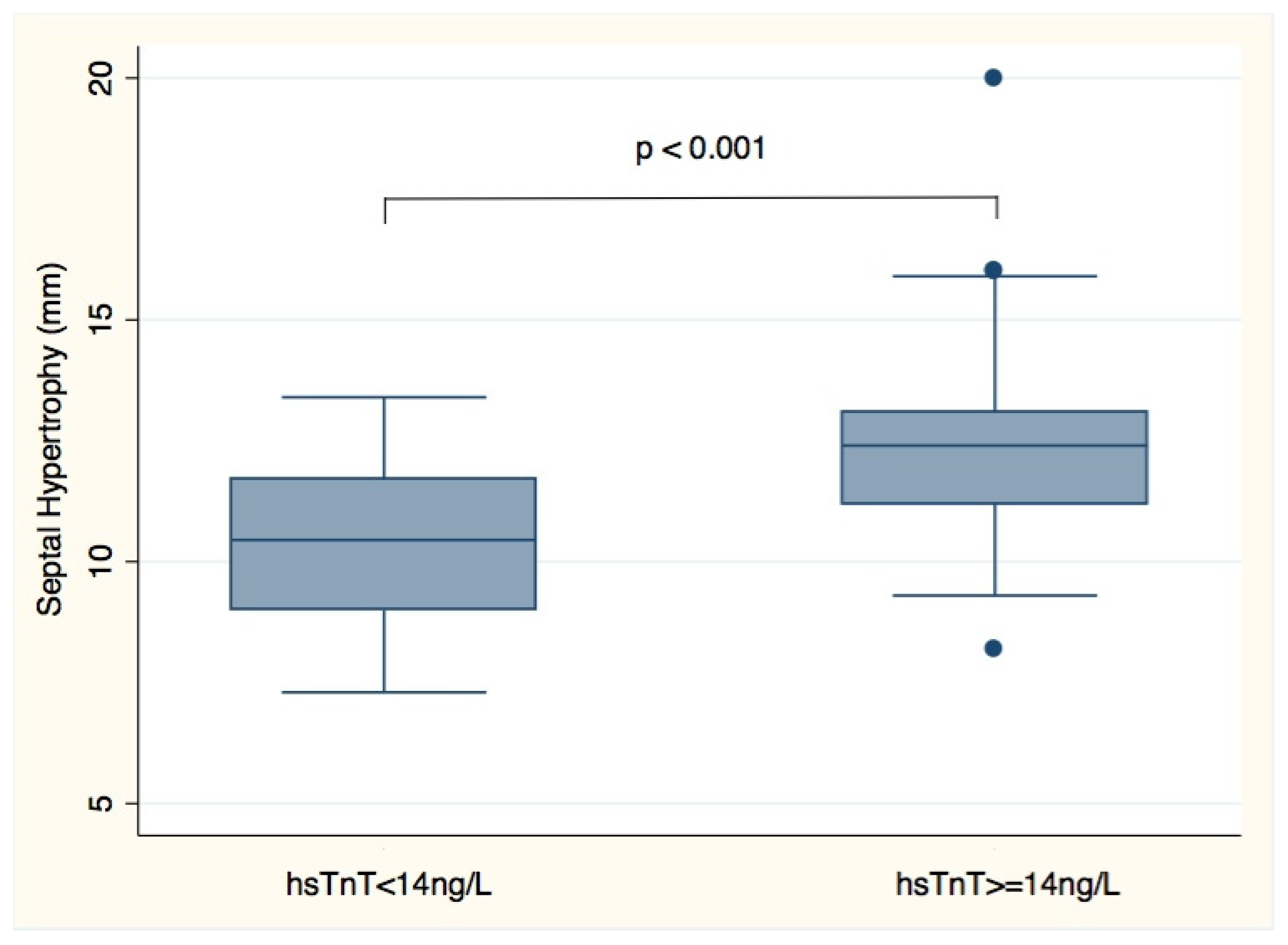
3.1.3. Cardiac Biomarkers
4. Discussion
5. Limits of the Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | angiotensin-converting enzyme |
| ECG | electrocardiogram |
| FA | Friedreich’s ataxia |
| hsTnT | high-sensitivity troponin T |
| LV | left ventricle |
| LVEDD | left ventricular end diastolic diameter |
| LVEF | left ventricular ejection fraction |
| LVESD | left ventricular end systolic diameter |
| NOAC | new oral anticoagulant |
| NT-proBNP | N-Terminal proBrain Natriuretic Peptide |
| PWT | posterior wall thickness |
| RWT | relative wall thickness |
| SWT | septal wall thickness |
| GAA1 | number of GAA (guanine-adenine-adenine) repeats in the shorter allele of the FXN gene |
| GAA2 | trinucleotide number of GAA (guanine-adenine-adenine) repeats in the longer allele of the FXN gene |
References
- Durr, A.; Cossee, M.; Agid, Y.; Campuzano, V.; Mignard, C.; Penet, C.; Mandel, J.-L.; Brice, A.; Koenig, M. Clinical and genetic abnormalities in patients with Friedreich’s ataxia. N. Engl. J. Med. 1996, 335, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Campuzano, V.; Montermini, L.; Molto, M.D.; Pianese, L.; Cossee, M.; Cavalcanti, F.; Monros, E.; Rodius, F.; Duclos, F.; Monticelli, A.; et al. Friedreich’s ataxia: Autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science 1996, 271, 1423–1427. [Google Scholar] [CrossRef] [PubMed]
- Reetz, K.; Dogan, I.; Costa, A.S.; Dafotakis, M.; Fedosov, K.; Giunti, P.; Parkinson, M.H.; Sweeney, M.G.; Mariotti, C.; Panzeri, M.; et al. Biological and clinical characteristics of the European Friedreich’s Ataxia Consortium for Translational Studies (EFACTS) cohort: A cross-sectional analysis of baseline data. Lancet Neurol. 2015, 14, 174–182. [Google Scholar] [CrossRef]
- Reetz, K.; Dogan, I.; Hilgers, R.D.; Giunti, P.; Mariotti, C.; Durr, A.; Boesch, S.; Klopstock, T.; Javier Rodriguez de Rivera, F.; Schöls, L.; et al. Progression characteristics of the European Friedreich’s Ataxia Consortium for Translational Studies (EFACTS): A 2 year cohort study. Lancet Neurol. 2016, 15, 1346–1354. [Google Scholar] [CrossRef]
- Weidemann, F.; Liu, D.; Hu, K.; Florescu, C.; Niemann, M.; Herrmann, S.; Kramer, B.; Klebe, S.; Doppler, K.; Üçeyler, N.; et al. The cardiomyopathy in Friedreich’s ataxia—New biomarker for staging cardiac involvement. Int. J. Cardiol. 2015, 194, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Pousset, F.; Legrand, L.; Monin, M.L.; Ewenczyk, C.; Charles, P.; Komajda, M.; Brice, A.; Pandolfo, M.; Isnard, R.; Tezenas du Montcel, S.; et al. A 22-Year Follow-up Study of Long-term Cardiac Outcome and Predictors of Survival in Friedreich Ataxia. JAMA Neurol. 2015, 72, 1334–1341. [Google Scholar] [CrossRef] [Green Version]
- Tsou, A.Y.; Paulsen, E.K.; Lagedrost, S.J.; Perlman, S.L.; Mathews, K.D.; Wilmot, G.R.; Ravinah, B.; Koeppenij, A.H.; Lynchabcd, D.R. Mortality in Friedreich ataxia. J. Neurol. Sci. 2011, 307, 46–49. [Google Scholar] [CrossRef]
- Latini, R.; Masson, S.; Anand, I.S.; Missov, E.; Carlson, M.; Vago, T.; Angelici, L.; Barlera, S.; Parrinello, G.; Maggioni, A.P.; et al. Prognostic value of very low plasma concentrations of troponin T in patients with stable chronic heart failure. Circulation 2007, 116, 1242–1249. [Google Scholar] [CrossRef] [Green Version]
- Friedman, L.S.; Schadt, K.A.; Regner, S.R.; Mark, G.E.; Lin, K.Y.; Sciascia, T.; Sutton, M.S.J.; Willi, S.; Lynch, D.R. Elevation of serum cardiac troponin I in a cross-sectional cohort of asymptomatic subjects with Friedreich ataxia. Int. J. Cardiol. 2013, 167, 1622–1624. [Google Scholar] [CrossRef]
- Maisel, A.S.; Krishnaswamy, P.; Nowak, R.M.; McCord, J.; Hollander, J.E.; Duc, P.; Omland, T.; Storrow, A.B.; Abraham, W.T.; Wu, A.H.; et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N. Engl. J. Med. 2002, 347, 161–167. [Google Scholar] [CrossRef]
- Coats, C.J.; Gallagher, M.J.; Foley, M.; O’Mahony, C.; Critoph, C.; Gimeno, J.; Dawnay, A.; McKenna, W.J.; Elliott, P.M. Relation between serum N-terminal pro-brain natriuretic peptide and prognosis in patients with hypertrophic cardiomyopathy. Eur. Heart J. 2013, 34, 2529–2537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- York, M.K.; Gupta, D.K.; Reynolds, C.F.; Farber-Eger, E.; Wells, Q.S.; Bachmann, K.N.; Xu, M.; Harrell, F.E., Jr.; Wang, T.J. 1B-Type Natriuretic Peptide Levels and Mortality in Patients with and Without Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Marelli, C.; Figoni, J.; Charles, P.; Anheim, M.; Tchikviladze, M.; Vincitorio, C.M.; Tezenas du Montcel, S.; Brice, A.; Golmard, J.L.; Dürr, A. Annual change in Friedreich’s ataxia evaluated by the Scale for the Assessment and Rating of Ataxia (SARA) is independent of disease severity. Mov. Disord. 2012, 27, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- Foppa, M.; Duncan, B.B.; Rohde, L.E. Echocardiography-based left ventricular mass estimation. How should we define hypertrophy? Cardiovasc. Ultrasound. 2005, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Rivas-Gotz, C.; Manolios, M.; Thohan, V.; Nagueh, S.F. Impact of left ventricular ejection fraction on estimation of left ventricular filling pressures using tissue Doppler and flow propagation velocity. Am. J. Cardiol. 2003, 91, 780–784. [Google Scholar] [CrossRef]
- Henry, W.L.; Gardin, J.M.; Ware, J.H. Echocardiographic measurements in normal subjects from infancy to old age. Circulation 1980, 62, 1054–1061. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.W.; Abdullah, S.M.; Drazner, M.H.; Das, S.R.; Khera, A.; McGuire, D.K.; Wians, F.; Sabatine, M.S.; Morrow, D.A.; de Lemos, J.A. Prevalence and determinants of troponin T elevation in the general population. Circulation 2006, 113, 1958–1965. [Google Scholar] [CrossRef] [Green Version]
- Kubo, T.; Kitaoka, H.; Yamanaka, S.; Hirota, T.; Baba, Y.; Hayashi, K.; Iiyama, T.; Kumagai, N.; Tanioka, K.; Yamasaki, N.; et al. Significance of high-sensitivity cardiac troponin T in hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2013, 62, 1252–1259. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Taniguchi, R.; Nagai, K.; Makiyama, T.; Okada, H.; Yamada, T.; Matsumori, A.; Takatsu, Y. Measurements of cardiac troponin T in patients with hypertrophic cardiomyopathy. Heart 2003, 89, 659–660. [Google Scholar] [CrossRef]
- Jenab, Y.; Pourjafari, M.; Darabi, F.; Boroumand, M.A.; Zoroufian, A.; Jalali, A. Prevalence and determinants of elevated high-sensitivity cardiac troponin T in hypertrophic cardiomyopathy. J. Cardiol. 2014, 63, 140–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeppen, A.H. Friedreich’s ataxia: Pathology, pathogenesis, and molecular genetics. J. Neurol. Sci. 2011, 303, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeppen, A.H.; Ramirez, R.L.; Becker, A.B.; Bjork, S.T.; Levi, S.; Santambrogio, P.; Parsons, P.J.; Kruger, P.C.; Yang, K.X.; Feustel, P.J.; et al. The pathogenesis of cardiomyopathy in Friedreich ataxia. PLoS ONE 2015, 10, e0116396. [Google Scholar] [CrossRef] [PubMed]
- Coats, C.J.; Parisi, V.; Ramos, M.; Janagarajan, K.; O’Mahony, C.; Dawnay, A.; Lachmann, R.H.; Murphy, E.; Mehta, A.; Hughes, D.; et al. Role of serum N-terminal pro-brain natriuretic peptide measurement in diagnosis of cardiac involvement in patients with anderson-fabry disease. Am. J. Cardiol. 2013, 111, 111–117. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Patients (n = 85) Mean ± SD |
|---|---|
| Age (years) | 39 ± 12 |
| Male sex n (%) | 44 (51) |
| Body surface area (m2) | 1.8 ± 1.7 |
| GAA1 pb | 480 ± 300 |
| GAA2 pb (n = 83) | 750 ± 300 |
| Age at onset (years) (n = 83) | 17 ± 10 |
| Age at becoming wheelchair bound (years) (n = 53), | 26 ± 9 |
| Systolic blood pressure (mm Hg) | 117 ± 12 |
| Diastolic blood pressure (mm Hg) | 75 ± 13 |
| Heart rate (beats/min) | 77 ± 13 |
| Septal wall thickness (mm) | 11 ± 2 |
| Posterior wall thickness (mm) | 10 ± 2 |
| Relative wall thickness (RWT) > 0.42, n (%) | 60 (71%) |
| Left ventricular diastolic diameter (mm) | 45 ± 5 |
| Left ventricular systolic diameter (mm) (n = 82) | 27 ± 6 |
| Left ventricular ejection fraction (%) | 64 ± 6 |
| Left ventricular mass index (g/m2) | 98 ± 24 |
| Trans mitral E wave (cm/s) (n = 84) | 70 ± 10 |
| Trans mitral A wave (cm/s) (n = 81), | 60 ± 20 |
| Trans mitral E/A ratio (n = 81) | 1.3 ± 0.6 |
| Lateral E/E’ ratio (n = 84) | 6.2 ± 2.2 |
| Left atrial area (cm2) (n = 83) | 17 ± 5 |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95%IC) | p | OR (95%IC) | p | |
| Age | 0.96 (0.92–1.00) | 0.05 * | - | NS |
| Male sex | 0.88 (0.33–2.34) | 0.79 | ||
| Body surface area | 0.40 (0.02–7.08) | 0.36 | ||
| GAA1 | 1.47 (0.67–3.18) | 0.29 | ||
| GAA2 | 1.32 (0.69–2.55) | 0.72 | ||
| Heart rate | 1.02 (0.98–1.06) | 0.31 | ||
| NT-proBNP plasma level ≥ 125 ng/L | 2.34 (0.63–8.61) | 0.20 | ||
| Septal wall thickness | 1.79 (1.27–2.53) | <0.001 * | 1.79 (1.27–2.53) | <0.001 |
| Posterior wall thickness | 1.38 (1.01–1.88) | 0.04 * | - | NS |
| Relative wall thickness (RWT) > 0.42 | 2.64 (0.83–8.34) | 0.1 | - | |
| LV diastolic diameter | 0.99 (0.9–1.09) | 0.66 | ||
| LV systolic diameter | 1.06 (0.97–1.15) | 0.19 | ||
| LVejection fraction | 0.91 (0.84–1.00) | 0.17 | ||
| LV mass index | 1.04 (1.01–1.08) | <0.001 * | - | NS |
| Trans mitral E wave | 0.1 (0.001–6.06) | 0.59 | ||
| Trans mitral A wave | 0.32 (0.01–6.84) | 0.53 | ||
| E/A ratio | 1.27 (0.58–2.77) | 0.6 | ||
| Lateral E/E’ ratio | 1.1 (0.86–1.51) | 0.5 | ||
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95%IC) | p | OR (95%IC) | p | |
| Age | 0.99 (0.94–1.04) | 0.72 | ||
| Male sex | 2.42 (0.67–8.76) | 0.17 | ||
| Body surface area | 1.34 (0.03–48.7) | 0.87 | ||
| GAA1 | 4.10 (1.25–13.38] | 0.02 * | - | NS |
| GAA2 | 1.95 (0.84–4.53) | 0.12 | ||
| Heart rate | 1.00 (0.96–1.05) | 0.79 | ||
| Septal wall thickness | 1.41 (1.06–1.89) | 0.02 * | - | NS |
| Posterior wall thickness | 1.14(0.78–1.66) | 0.49 | ||
| Relative wall thickness (RWT) > 0.42 | 5.38 (0.65–44.19) | 0.11 | ||
| LV diastolic diameter | 0.99 (0.88–1.12) | 0.95 | ||
| LV systolic diameter | 1.05 (0.94–1.17) | 0.34 | ||
| LV ejection fraction | 0.88 (0.80–0.98) | 0.02 * | - | NS |
| LV mass index | 1.02 (0.99–1.04) | 0.11 | ||
| Trans mitral E wave | 0.20 (0.01–30) | 0.53 | ||
| Trans mitral A wave | 0.01 (0.00–0.37) | 0.02 * | - | NS |
| E/A ratio | 3.46 (1.30–9.19) | 0.01 * | 3.48 (1.28–9.48) | 0.01 |
| Lateral E/E’ ratio | 1.47 (1.06–2.02) | 0.02 * | 1.64 (1.13–2.40) | 0.01 |
| Left atrial area | 1.20 (1.05–1.36) | 0.006 * | - | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legrand, L.; Maupain, C.; Monin, M.-L.; Ewenczyk, C.; Isnard, R.; Alkouri, R.; Durr, A.; Pousset, F. Significance of NT-proBNP and High-Sensitivity Troponin in Friedreich Ataxia. J. Clin. Med. 2020, 9, 1630. https://doi.org/10.3390/jcm9061630
Legrand L, Maupain C, Monin M-L, Ewenczyk C, Isnard R, Alkouri R, Durr A, Pousset F. Significance of NT-proBNP and High-Sensitivity Troponin in Friedreich Ataxia. Journal of Clinical Medicine. 2020; 9(6):1630. https://doi.org/10.3390/jcm9061630
Chicago/Turabian StyleLegrand, Lise, Carole Maupain, Marie-Lorraine Monin, Claire Ewenczyk, Richard Isnard, Rana Alkouri, Alexandra Durr, and Francoise Pousset. 2020. "Significance of NT-proBNP and High-Sensitivity Troponin in Friedreich Ataxia" Journal of Clinical Medicine 9, no. 6: 1630. https://doi.org/10.3390/jcm9061630
APA StyleLegrand, L., Maupain, C., Monin, M.-L., Ewenczyk, C., Isnard, R., Alkouri, R., Durr, A., & Pousset, F. (2020). Significance of NT-proBNP and High-Sensitivity Troponin in Friedreich Ataxia. Journal of Clinical Medicine, 9(6), 1630. https://doi.org/10.3390/jcm9061630