Deterioration of Retinal Blood Flow Parameters in Branch Retinal Vein Occlusion Measured by Doppler Optical Coherence Tomography Flowmeter

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Inclusion/Exclusion Criteria and Diagnosis of BRVO
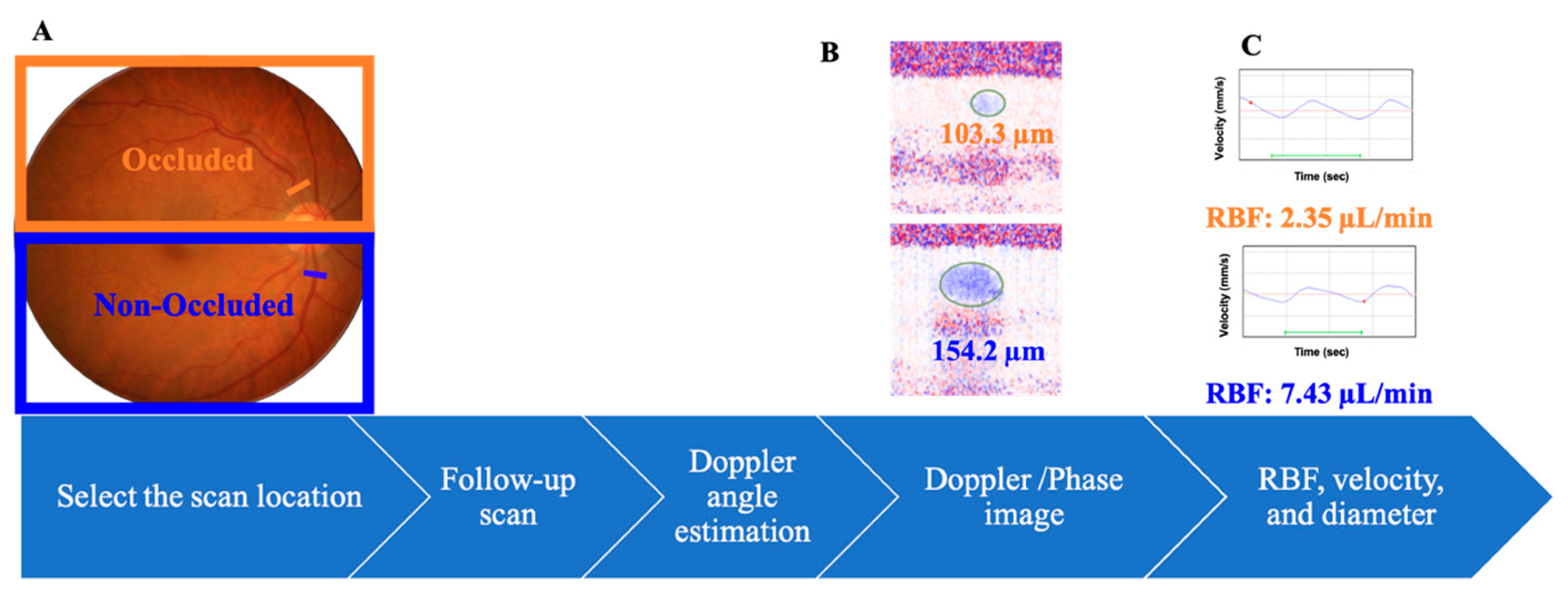
2.2. Doppler Optical Coherence Tomography
2.3. Study Protocol
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. RBF Parameters of DOCT Flowmeter
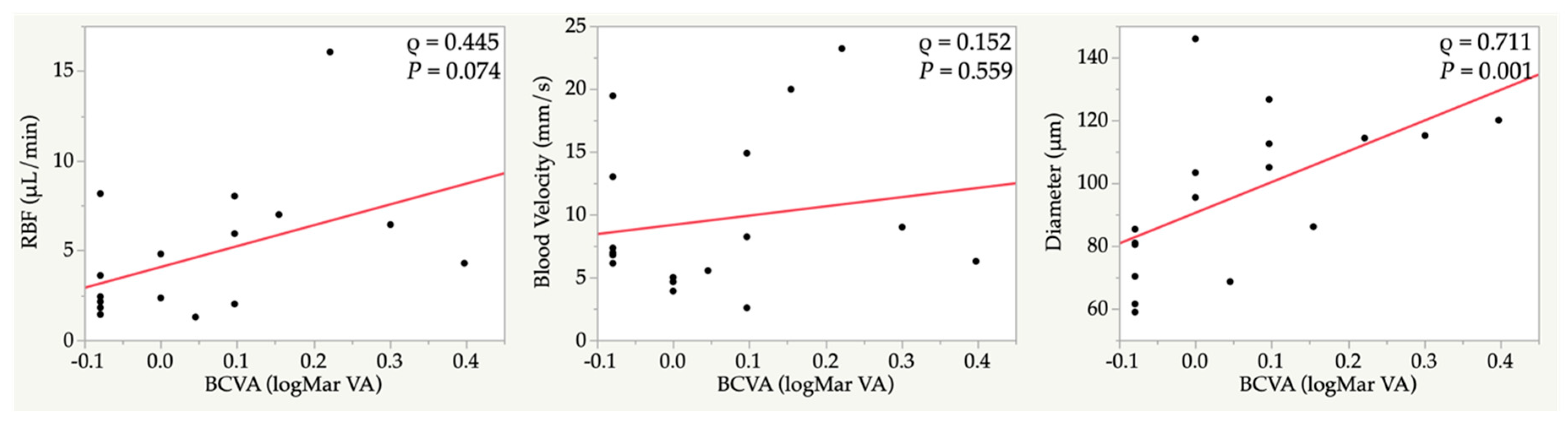
3.3. Correlations between Retinal Blood Flow and the Ocular Parameters in the Occluded Vein
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Browning, D.J. Retinal Vein Occlusions: Evidence-Based Management; Springer: New York, NY, USA, 2012. [Google Scholar]
- Hayreh, S.S.; Zimmerman, M.B. Branch retinal vein occlusion: Natural history of visual outcome. JAMA Ophthalmol. 2014, 132, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Shilling, J.S.; Jones, C.A. Retinal branch vein occlusion: A study of argon laser photocoagulation in the treatment of macular oedema. Br. J. Ophthalmol. 1984, 68, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Pulido, J.S.; Flaxel, C.J.; Adelman, R.A.; Hyman, L.; Folk, J.C.; Olsen, T.W. Retinal vein occlusions preferred practice pattern((R)) guidelines. Ophthalmology 2016, 123, 182–208. [Google Scholar] [CrossRef] [PubMed]
- Tadayoni, R.; Waldstein, S.M.; Boscia, F.; Gerding, H.; Gekkieva, M.; Barnes, E.; Das Gupta, A.; Wenzel, A.; Pearce, I. Sustained benefits of ranibizumab with or without laser in branch retinal vein occlusion: 24-month results of the BRIGHTER study. Ophthalmology 2017, 124, 1778–1787. [Google Scholar] [CrossRef] [PubMed]
- Avila, C.P., Jr.; Bartsch, D.U.; Bitner, D.G.; Cheng, L.; Mueller, A.J.; Karavellas, M.P.; Freeman, W.R. Retinal blood flow measurements in branch retinal vein occlusion using scanning laser Doppler flowmetry. Am. J. Ophthalmol. 1998, 126, 683–690. [Google Scholar] [CrossRef]
- Noma, H.; Funatsu, H.; Sakata, K.; Harino, S.; Nagaoka, T.; Mimura, T.; Sone, T.; Hori, S. Macular microcirculation and macular oedema in branch retinal vein occlusion. Br. J. Ophthalmol. 2009, 93, 630–633. [Google Scholar] [CrossRef] [PubMed]
- Horio, N.; Horiguchi, M. Effect of arteriovenous sheathotomy on retinal blood flow and macular edema in patients with branch retinal vein occlusion. Am. J. Ophthalmol. 2005, 139, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, T.; Sogawa, K.; Yoshida, A. Changes in retinal blood flow in patients with macular edema secondary to branch retinal vein occlusion before and after intravitreal injection of bevacizumab. Retin. (Phila. Pa.) 2014, 34, 2037–2043. [Google Scholar] [CrossRef] [PubMed]
- Tani, T.; Song, Y.S.; Yoshioka, T.; Omae, T.; Ishibazawa, A.; Akiba, M.; Yoshida, A. Repeatability and Reproducibility of Retinal Blood Flow Measurement Using a Doppler Optical Coherence Tomography Flowmeter in Healthy Subjects. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2891–2898. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Tani, T.; Omae, T.; Ishibazawa, A.; Yoshioka, T.; Takahashi, K.; Akiba, M.; Yoshida, A. Retinal blood flow reduction after panretinal photocoagulation in Type 2 diabetes mellitus: Doppler optical coherence tomography flowmeter pilot study. PLoS ONE 2018, 13, e0207288. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, T.; Tani, T.; Song, Y.S.; Yoshioka, T.; Ishibazawa, A.; Nakabayashi, S.; Akiba, M.; Yoshida, A. Evaluation of Retinal Circulation Using Segmental-Scanning Doppler Optical Coherence Tomography in Anesthetized Cats. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2936–2941. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, T.; Song, Y.; Kawai, M.; Tani, T.; Takahashi, K.; Ishiko, S.; Lavinsky, F.; Wollstein, G.; Ishikawa, H.; Schuman, J.S.; et al. Retinal blood flow reduction in normal-tension glaucoma with single-hemifield damage by Doppler optical coherence tomography. Br. J. Ophthalmol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Leitgeb, R.A.; Werkmeister, R.M.; Blatter, C.; Schmetterer, L. Doppler optical coherence tomography. Prog. Retin. Eye Res. 2014, 41, 26–43. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Funatsu, H.; Harino, S.; Nagaoka, T.; Mimura, T.; Hori, S. Influence of macular microcirculation and retinal thickness on visual acuity in patients with branch retinal vein occlusion and macular edema. Jpn. J. Ophthalmol. 2010, 54, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.; Kriechbaum, K.; Prager, F.; Benesch, T.; Georgopoulos, M.; Zlabinger, G.J.; Schmidt-Erfurth, U. Intraocular concentrations of growth factors and cytokines in retinal vein occlusion and the effect of therapy with bevacizumab. Investig. Ophthalmol. Vis. Sci. 2009, 50, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Funatsu, H.; Yamasaki, M.; Tsukamoto, H.; Mimura, T.; Sone, T.; Jian, K.; Sakamoto, I.; Nakano, K.; Yamashita, H.; et al. Pathogenesis of macular edema with branch retinal vein occlusion and intraocular levels of vascular endothelial growth factor and interleukin-6. Am. J. Ophthalmol. 2005, 140, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Lee, S.; Son, Y. Effects of two different doses of intravitreal bevacizumab on subfoveal choroidal thickness and retinal vessel diameter in branch retinal vein occlusion. Int. J. Ophthalmol. 2016, 9, 999–1005. [Google Scholar] [PubMed]
- Su, E.N.; Cringle, S.J.; McAllister, I.L.; Yu, D.Y. An experimental study of VEGF induced changes in vasoactivity in pig retinal arterioles and the influence of an anti-VEGF agent. BMC Ophthalmol. 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| BRVO Eye (n = 17) | Fellow Eye (n = 17) | p Value * | |
|---|---|---|---|
| Age (years) | 63.1 ± 10.8 | - | |
| Male (n = 9) | 65.6 ± 12.0 | ||
| Female (n = 8) | 60.3 ± 9.3 | ||
| Occluded location (superior/inferior) | 8/9 | - | |
| Male (n = 9) | 4/5 | - | |
| Female (n = 8) | 4/4 | - | |
| BCVA at the initial visit (logMAR) | 0.26 ± 0.34 | −0.08 ± 0.05 | <0.001 |
| BCVA (logMAR) | 0.06 ± 0.15 | −0.09 ± 0.03 | <0.001 |
| Refractive errors | −0.07 ± 2.45 | −0.37 ± 2.12 | 0.71 |
| IOP (mmHg) | 14.9 ± 2.3 | 14.7 ± 2.1 | 0.747 |
| MOPP (mmHg) | 58.2 ± 8.7 | 58.4 ± 8.5 | 0.968 |
| CMT at the initial visit (µm) | 439.5 ± 120.0 | 243.2 ± 19.7 | <0.001 |
| CMT (µm) | 259.0 ± 40.3 | 244.7 ± 18.5 | 0.193 |
| Total number of anti-VEGF injections | 1.9 ± 1.6 | - | |
| MBP (mmHg) | 102.2 ± 13.3 | - | |
| HR (bpm) | 79.0 ± 15.0 | ||
| Time from the initial visit (month) | 37.6 ± 32.8 | ||
| Time from the last anti-VEGF injection (month) | 28.2 ± 21.6 | ||
| Parameters | Occluded Vein in BRVO Eye (n = 17) | Non-Occluded Vein in BRVO Eye (n = 17) | Veins in Fellow Eye(n = 17) | p Value * | ||
|---|---|---|---|---|---|---|
| Occluded vs. Non-Occluded | Occluded vs. Fellow eye | Non-Occluded vs. Fellow eye | ||||
| RBF (µL/min) | 4.7 ± 3.7 | 10.3 ± 5.1 | 8.6 ± 4.0 | 0.001 | 0.013 | 0.828 |
| Blood Velocity (mm/s) | 9.6 ± 5.3 | 12.3 ± 5.0 | 11.7 ± 5.3 | 0.105 | 0.353 | 0.999 |
| Diameter (µm) | 95.9 ± 24.7 | 127.9 ± 23.7 | 116.4 ± 13.9 | 0.003 | 0.022 | 0.317 |
| Time from the Initial Visit | Time from the Last Anti-VEGF Injection | Number of Anti-VEGF Injections | ||||
|---|---|---|---|---|---|---|
| ρ | p Value | ρ | p Value | ρ | p Value | |
| RBF (µL/min) | −0.158 | 0.545 | −0.188 | 0.470 | 0.268 | 0.298 |
| Blood Velocity (mm/s) | 0.286 | 0.266 | 0.211 | 0.416 | 0.046 | 0.862 |
| Diameter (µm) | −0.467 | 0.059 | −0.393 | 0.119 | 0.279 | 0.278 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, K.; Song, Y.; Sogawa, K.; Yoshioka, T.; Tani, T.; Ishiko, S.; Yoshida, A. Deterioration of Retinal Blood Flow Parameters in Branch Retinal Vein Occlusion Measured by Doppler Optical Coherence Tomography Flowmeter. J. Clin. Med. 2020, 9, 1847. https://doi.org/10.3390/jcm9061847
Takahashi K, Song Y, Sogawa K, Yoshioka T, Tani T, Ishiko S, Yoshida A. Deterioration of Retinal Blood Flow Parameters in Branch Retinal Vein Occlusion Measured by Doppler Optical Coherence Tomography Flowmeter. Journal of Clinical Medicine. 2020; 9(6):1847. https://doi.org/10.3390/jcm9061847
Chicago/Turabian StyleTakahashi, Kengo, Youngseok Song, Kenji Sogawa, Takafumi Yoshioka, Tomofumi Tani, Satoshi Ishiko, and Akitoshi Yoshida. 2020. "Deterioration of Retinal Blood Flow Parameters in Branch Retinal Vein Occlusion Measured by Doppler Optical Coherence Tomography Flowmeter" Journal of Clinical Medicine 9, no. 6: 1847. https://doi.org/10.3390/jcm9061847
APA StyleTakahashi, K., Song, Y., Sogawa, K., Yoshioka, T., Tani, T., Ishiko, S., & Yoshida, A. (2020). Deterioration of Retinal Blood Flow Parameters in Branch Retinal Vein Occlusion Measured by Doppler Optical Coherence Tomography Flowmeter. Journal of Clinical Medicine, 9(6), 1847. https://doi.org/10.3390/jcm9061847