
WGCAMNet: Wasserstein Generative Adversarial Network Augmented and Custom Attention Mechanism Based Deep Neural Network for Enhanced Brain Tumor Detection and Classification

 , , , and
, , , and 
Abstract
1. Introduction
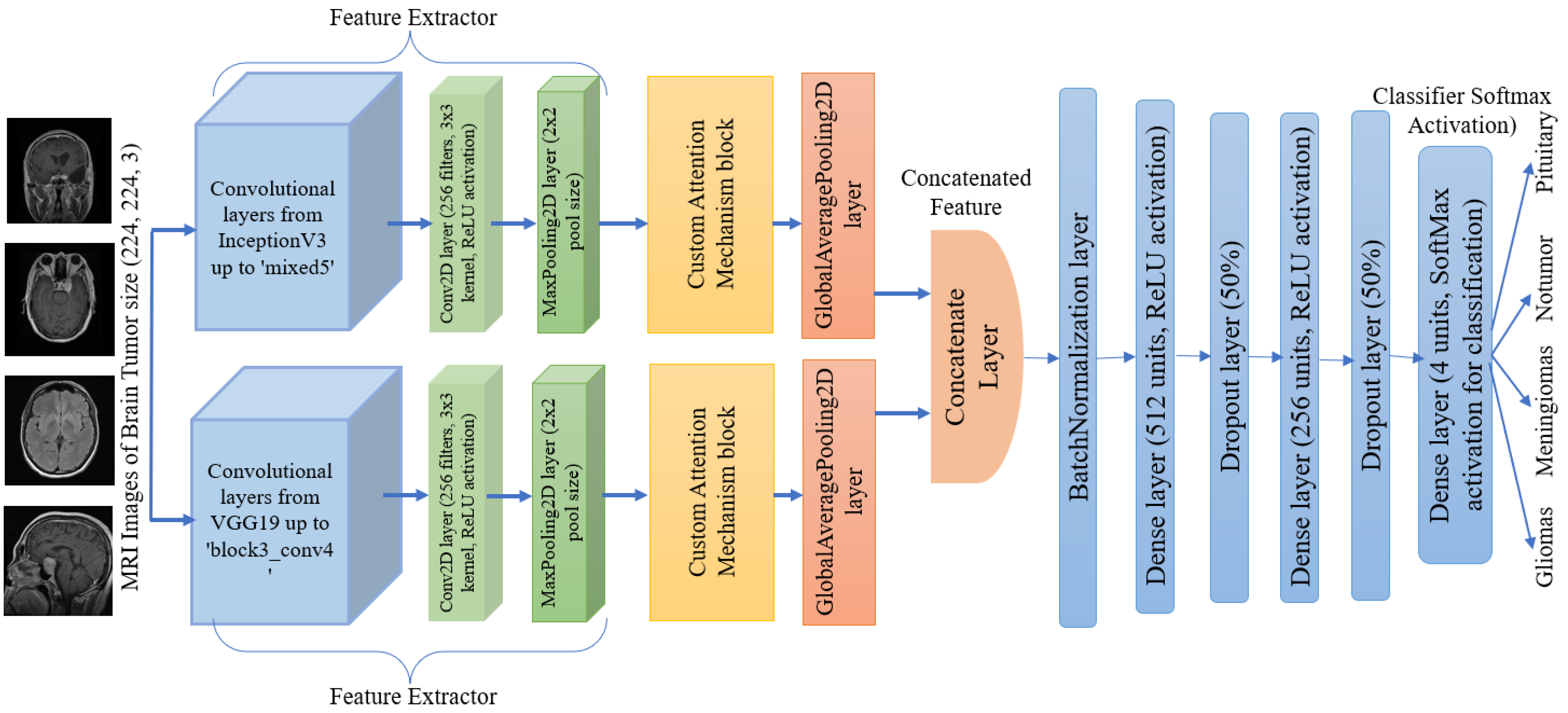
- A new deep learning framework for brain tumor detection and classification has been proposed, in which modified VGG19 and Inception v3 architectures, custom attention mechanism in the feature extraction along with classification layers are implemented.
- In the data preprocessing, images in the dataset have been balanced and augmented using Wasserstein Generative Adversarial Network (WGAN) to generate synthetic images, and a Gaussian filter has also been used for the noise reduction and enhancement of the quality of MRI images.
- After training the proposed model, the performance evaluation metrics have shown excellent results which will be very promising with the comparison of the existing models for brain tumor detection and classification.
- The model’s explainability through t-SNE plots shows distinct tumor clusters and Grad-CAM highlights crucial areas in MRI scans.
2. Related Works
2.1. Convolutional Neural Network (CNN)-Based Methods
2.2. Hybrid Models
2.3. Lightweight Models
3. Materials and Methods
3.1. Dataset
3.2. Data Loading and Preparation
- Standard Normalization:where is the mean and is the standard deviation of the pixel values. This helps in faster convergence during training by ensuring the data distribution is centered and scaled properly.
- Min-Max Normalization:where min and max are the minimum and maximum pixel values in the image, scales the pixel values to the range [0, 1], which helps in reducing the impact of outliers and ensures the data falls within a specific range, making it easier for the model to learn.
- GAN Normalization:modifies the values of pixels to the range [−1, 1]. This is particularly beneficial for Generative Adversarial Networks (GANs), because they perform better when the data is normalized to this range, resulting in more reliable and efficient training.
3.3. WGAN for Data Augmentation
3.4. Proposed Classifier Model
3.5. Training and Evaluation
4. Results
4.1. Experimental Setup
4.2. Data Filtering Impact
4.3. Data Augmentation Results
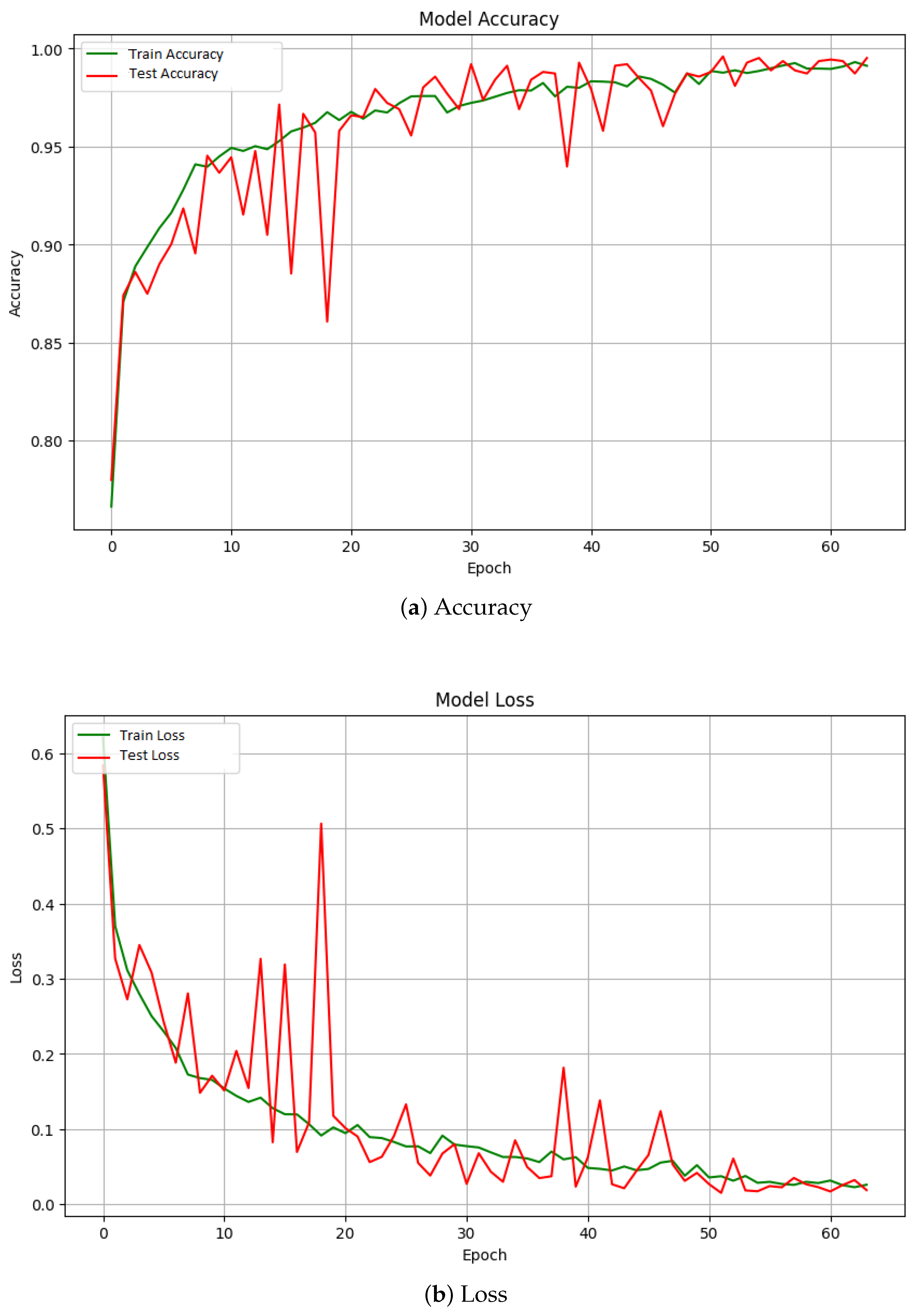
4.4. Classifier Performance
- Loss: 0.0153
- Accuracy: 0.9961
- Precision: 0.9960
- Recall: 0.9960
- AUC: 0.9999
4.5. Confusion Matrix and Visualization
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2011–2015. Neuro-Oncology 2018, 20, iv1–iv86. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016. Neuro-Oncology 2019, 21, v1–v100. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Jung, K.W.; Yoo, H.; Park, S.; Lee, S.H. Epidemiology of primary brain and central nervous system tumors in Korea. J. Korean Neurosurg. Soc. 2010, 48, 145. [Google Scholar] [CrossRef] [PubMed]
- Chandana, S.R.; Movva, S.; Arora, M.; Singh, T. Primary brain tumors in adults. Am. Fam. Physician 2008, 77, 1423–1430. [Google Scholar] [PubMed]
- Castro, M.G.; Cowen, R.; Williamson, I.K.; David, A.; Jimenez-Dalmaroni, M.J.; Yuan, X.; Bigliari, A.; Williams, J.C.; Hu, J.; Lowenstein, P.R. Current and future strategies for the treatment of malignant brain tumors. Pharmacol. Ther. 2003, 98, 71–108. [Google Scholar] [CrossRef]
- Erickson, B.J.; Korfiatis, P.; Akkus, Z.; Kline, T.L. Machine learning for medical imaging. Radiographics 2017, 37, 505–515. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H.I. Deep learning in medical image analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Sundaram, B. Deep learning at chest radiography: Automated classification of pulmonary tuberculosis by using convolutional neural networks. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.I.; Toscano, E. An extensive investigation into the use of machine learning tools and deep neural networks for the recognition of skin cancer: Challenges, future directions, and a comprehensive review. Symmetry 2024, 16, 366. [Google Scholar] [CrossRef]
- Hossain, T.; Shishir, F.S.; Ashraf, M.; Al Nasim, M.D.A.; Shah, F.M. Brain tumor detection using convolutional neural network. In Proceedings of the 2019 1st International Conference on Advances in Science, Engineering and Robotics Technology (ICASERT), Dhaka, Bangladesh, 3–5 May 2019; pp. 1–6. [Google Scholar]
- Khan, M.S.I.; Rahman, A.; Debnath, T.; Karim, M.R.; Nasir, M.K.; Band, S.S.; Mosavi, A.; Dehzangi, I. Accurate brain tumor detection using deep convolutional neural network. Comput. Struct. Biotechnol. J. 2022, 20, 4733–4745. [Google Scholar] [CrossRef]
- Shah, H.A.; Saeed, F.; Yun, S.; Park, J.H.; Paul, A.; Kang, J.M. A robust approach for brain tumor detection in magnetic resonance images using finetuned efficientnet. IEEE Access 2022, 10, 65426–65438. [Google Scholar] [CrossRef]
- Saeedi, S.; Rezayi, S.; Keshavarz, H.; Niakan Kalhori, S.R. MRI-based brain tumor detection using convolutional deep learning methods and chosen machine learning techniques. BMC Med. Inform. Decis. Mak. 2023, 23, 16. [Google Scholar] [CrossRef]
- Aggarwal, M.; Tiwari, A.K.; Sarathi, M.P.; Bijalwan, A. An early detection and segmentation of brain tumor using deep neural network. Bmc Med. Inform. Decis. Mak. 2023, 23, 78. [Google Scholar] [CrossRef]
- Khaliki, M.Z.; Başarslan, M.S. Brain tumor detection from images and comparison with transfer learning methods and 3-layer CNN. Sci. Rep. 2024, 14, 2664. [Google Scholar] [CrossRef]
- Alsubai, S.; Khan, H.U.; Alqahtani, A.; Sha, M.; Abbas, S.; Mohammad, U.G. Ensemble deep learning for brain tumor detection. Front. Comput. Neurosci. 2022, 16, 1005617. [Google Scholar] [CrossRef] [PubMed]
- Mahum, R.; Sharaf, M.; Hassan, H.; Liang, L.; Huang, B. A robust brain tumor detector using BiLSTM and Mayfly optimization and multi-level thresholding. Biomedicines 2023, 11, 1715. [Google Scholar] [CrossRef] [PubMed]
- Sailunaz, K.; Bestepe, D.; Alhajj, S.; Özyer, T.; Rokne, J.; Alhajj, R. Brain tumor detection and segmentation: Interactive framework with a visual interface and feedback facility for dynamically improved accuracy and trust. PLoS ONE 2023, 18, e0284418. [Google Scholar] [CrossRef] [PubMed]
- Asiri, A.A.; Shaf, A.; Ali, T.; Aamir, M.; Irfan, M.; Alqahtani, S.; Mehdar, K.M.; Halawani, H.T.; Alghamdi, A.H.; Alshamrani, A.F.A.; et al. Brain tumor detection and classification using fine-tuned CNN with ResNet50 and U-Net model: A study on TCGA-LGG and TCIA dataset for MRI applications. Life 2023, 13, 1449. [Google Scholar] [CrossRef] [PubMed]
- Saad, G.; Suliman, A.; Bitar, L.; Bshara, S. Developing a hybrid algorithm to detect brain tumors from MRI images. Egypt. J. Radiol. Nucl. Med. 2023, 54, 14. [Google Scholar] [CrossRef]
- Anantharajan, S.; Gunasekaran, S.; Subramanian, T.; Venkatesh, R. MRI brain tumor detection using deep learning and machine learning approaches. Meas. Sens. 2024, 31, 101026. [Google Scholar] [CrossRef]
- Mahmud, M.I.; Mamun, M.; Abdelgawad, A. A deep analysis of brain tumor detection from MR images using deep learning networks. Algorithms 2023, 16, 176. [Google Scholar] [CrossRef]
- Hammad, M.; ElAffendi, M.; Ateya, A.A.; Abd El-Latif, A.A. Efficient brain tumor detection with lightweight end-to-end deep learning model. Cancers 2023, 15, 2837. [Google Scholar] [CrossRef]
- Ghauri, M.S.; Wang, J.Y.; Reddy, A.J.; Shabbir, T.; Tabaie, E.; Siddiqi, J. Brain tumor recognition using artificial intelligence neural-networks (BRAIN): A cost-effective clean-energy platform. Neuroglia 2024, 5, 105–118. [Google Scholar] [CrossRef]
- Chaki, J.; Wozniak, M. Brain Tumor MRI Dataset. IEEE Dataport. 2023. Available online: https://ieee-dataport.org/documents/brain-tumor-mri-dataset (accessed on 20 July 2024).
- Podder, P.; Alam, F.B.; Mondal, M.R.H.; Hasan, M.J.; Rohan, A.; Bharati, S. Rethinking densely connected convolutional networks for diagnosing infectious diseases. Computers 2023, 12, 95. [Google Scholar] [CrossRef]
- Alam, F.B.; Podder, P.; Mondal, M.R.H. RVCNet: A hybrid deep neural network framework for the diagnosis of lung diseases. PLoS ONE 2023, 18, e0293125. [Google Scholar] [CrossRef] [PubMed]
- Chaki, J.; Woźniak, M. Brain Tumor Categorization and Retrieval Using Deep Brain Incep Res Architecture Based Reinforcement Learning Network. IEEE Access 2023, 11, 130584–130600. [Google Scholar] [CrossRef]
- Arumugam, M.; Thiyagarajan, A.; Adhi, L.; Alagar, S. Crossover Smell Agent Optimized Multilayer Perceptron for Precise Brain Tumor Classification on MRI Images. Expert Syst. Appl. 2024, 238, 121453. [Google Scholar] [CrossRef]
- Amarnath, A.; Al Bataineh, A.; Hansen, J.A. Transfer-Learning Approach for Enhanced Brain Tumor Classification in MRI Imaging. BioMedInformatics 2024, 4, 1745–1756. [Google Scholar] [CrossRef]
- Vu, H.A. Integrating Preprocessing Methods and Convolutional Neural Networks for Effective Tumor Detection in Medical Imaging. arXiv 2024, arXiv:2402.16221. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Methods | Performance Metrics |
|---|---|---|
| Hossain et al. [16] | Fuzzy C-Means clustering, traditional classifiers (SVM, KNN, MLP, etc.), CNN | CNN accuracy: 97.87% |
| Khan et al. [17] | 23-layer CNN, transfer learning with VGG16 | Accuracy: 97.8% (binary), 100% (multiclass) |
| Shah et al. [18] | Fine-tuned EfficientNet-B0, data augmentation, image enhancement | Accuracy: 98.87% |
| Saeedi et al. [19] | 2D CNN, convolutional auto-encoder, traditional ML methods (MLP, KNN, etc.) | 2D CNN Accuracy: 96.47%, Auto-encoder Accuracy: 95.63%, AUC: 0.99, Recall: 95% |
| Aggarwal et al. [20] | Improved ResNet for segmentation | >10% improvement in accuracy, recall, F1-score |
| Khaliki et al. [21] | CNN, Inception-V3, EfficientNetB4, VGG19, transfer learning | Best accuracy: 98% (VGG16), F-score: 97%, AUC: 99%, Recall: 98%, Precision: 98% |
| Alsubai et al. [22] | Hybrid CNN-LSTM, data preprocessing, CNN feature extraction | Accuracy: 99.1%, Precision: 98.8%, Recall: 98.9%, F1-score: 99.0% |
| Mahum et al. [23] | Mayfly optimization, ResNet-V2, BiLSTM | High accuracy, precision, recall, F1 score, AUC |
| Sailunaz et al. [24] | CNN, U-Net, U-Net++ for 2D and 3D MRI segmentation | Accuracy and Dice scores above 90% |
| Asiri et al. [25] | Fine-tuned CNN with ResNet50, U-Net for segmentation | IoU: 0.91, DSC: 0.95, SI: 0.95 |
| Saad et al. [26] | Hybrid algorithm for brain tumor detection, CAD | Detection accuracy: 96.6% |
| Anantharajan et al. [27] | Ensemble Deep Neural SVM, Fuzzy C-means, GLCM | Accuracy: 97.93%, Sensitivity: 92%, Specificity: 98% |
| Mahmud et al. [28] | CNN architecture compared with ResNet-50, VGG16, Inception V3 | Accuracy: 93.3%, AUC: 98.43%, Recall: 91.19%, Loss: 0.25 |
| Hammad et al. [29] | CNN-based model for IoMT applications, lightweight design | Accuracy: 99.48% (binary), 96.86% (multi-class) |
| Ghauri et al. [30] | Clean-energy cloud-based DL platform, multi-layer CNN | Precision: 96.8% |
| Type of Brain Tumor | Training Set | Testing Set |
|---|---|---|
| Glioma | 1321 | 300 |
| Meningioma | 1339 | 306 |
| No tumor | 1595 | 405 |
| Pituitary | 1457 | 300 |
| Total | 5712 | 1270 |
| Metric | Equation | Notes |
|---|---|---|
| Accuracy | TP: True Positives | |
| Precision | TN: True Negatives | |
| Recall (Sensitivity) | FP: False Positives | |
| F1 Score | FN: False Negatives |
| Augmentation Method | Loss | Accuracy | Precision | Recall | AUC |
|---|---|---|---|---|---|
| No Augmentation | 0.1889 | 93.12% | 0.9348 | 0.9304 | 0.9923 |
| Traditional Augmentation | 0.1666 | 95.50% | 0.9561 | 0.9525 | 0.9936 |
| WGAN Augmentation | 0.0153 | 99.60% | 0.9960 | 0.9960 | 0.9999 |
| Fold | Accuracy | Loss | Precision | Recall | AUC |
|---|---|---|---|---|---|
| Fold 1 | 0.9920 | 0.0375 | 0.9910 | 0.9905 | 0.9990 |
| Fold 2 | 0.9875 | 0.0405 | 0.9860 | 0.9880 | 0.9980 |
| Fold 3 | 0.9905 | 0.0380 | 0.9880 | 0.9920 | 0.9996 |
| Fold 4 | 0.9915 | 0.0380 | 0.9900 | 0.9890 | 0.9998 |
| Fold 5 | 0.9890 | 0.0395 | 0.9885 | 0.9875 | 0.9995 |
| Average | 0.9902 | 0.0389 | 0.9889 | 0.9894 | 0.9996 |
| Reference | Dataset | Preprocessing Method | Model Architecture | Performance Metrics |
|---|---|---|---|---|
| Chaki et al. [34] | [31] | Fuzzy Inference System | Deep Brain INCEP Res Architecture 2.0 Based Reinforcement Learning Network | Accuracy: 97.5% |
| Arumugam et al. [35] | [31] | Cropping and denoising by Gaussian filter | CNN with Multi Layer Perception | Accuracy: 98.5%, Sensitivity: 98.6%, Specificity: 98.4% |
| Amarnath et al. [36] | [31] | Traditional Augmentation | ResNet50 | Accuracy: 87.9%, F1 Score: 79.6% |
| Amarnath et al. [36] | [31] | Traditional Augmentation | Xception | Accuracy: 98.1%, F1 Score: 98.1% |
| Amarnath et al. [36] | [31] | Traditional Augmentation | EfficientNetV2-S | Accuracy: 96.1%, F1 Score: 96.2% |
| Amarnath et al. [36] | [31] | Traditional Augmentation | ResNet152V2 | Accuracy: 78.5%, F1 Score: 79.9% |
| Amarnath et al. [36] | [31] | Traditional Augmentation | VGG16 | Accuracy: 76.8%, F1 Score: 77.5% |
| Vu et al. [37] | [31] | Smoothing with a Kernel, Bilateral Filtering, Gray scale conversion and Traditional Augmentation | Modified ResNet50 | Accuracy: 75% |
| Proposed Model | [31] | WGAN and Gaussian Filter | WGCAMNet | Accuracy: 99.61%, Precision: 99.60%, Recall: 99.60%, AUC: 99.99%, Loss: 0.0153 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, F.B.; Fahim, T.A.; Asef, M.; Hossain, M.A.; Dewan, M.A.A. WGCAMNet: Wasserstein Generative Adversarial Network Augmented and Custom Attention Mechanism Based Deep Neural Network for Enhanced Brain Tumor Detection and Classification. Information 2024, 15, 560. https://doi.org/10.3390/info15090560
Alam FB, Fahim TA, Asef M, Hossain MA, Dewan MAA. WGCAMNet: Wasserstein Generative Adversarial Network Augmented and Custom Attention Mechanism Based Deep Neural Network for Enhanced Brain Tumor Detection and Classification. Information. 2024; 15(9):560. https://doi.org/10.3390/info15090560
Chicago/Turabian StyleAlam, Fatema Binte, Tahasin Ahmed Fahim, Md Asef, Md Azad Hossain, and M. Ali Akber Dewan. 2024. "WGCAMNet: Wasserstein Generative Adversarial Network Augmented and Custom Attention Mechanism Based Deep Neural Network for Enhanced Brain Tumor Detection and Classification" Information 15, no. 9: 560. https://doi.org/10.3390/info15090560
APA StyleAlam, F. B., Fahim, T. A., Asef, M., Hossain, M. A., & Dewan, M. A. A. (2024). WGCAMNet: Wasserstein Generative Adversarial Network Augmented and Custom Attention Mechanism Based Deep Neural Network for Enhanced Brain Tumor Detection and Classification. Information, 15(9), 560. https://doi.org/10.3390/info15090560