
Effect of Bergenin on Human Gingival Fibroblast Response on Zirconia Implant Surfaces: An In Vitro Study




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation
Complete Media Preparation
2.2. Cell Culture
2.2.1. Cell Morphology and Attachment
2.2.2. Cell Proliferation
2.2.3. Cell Migration
2.3. Statistical Analysis
3. Results
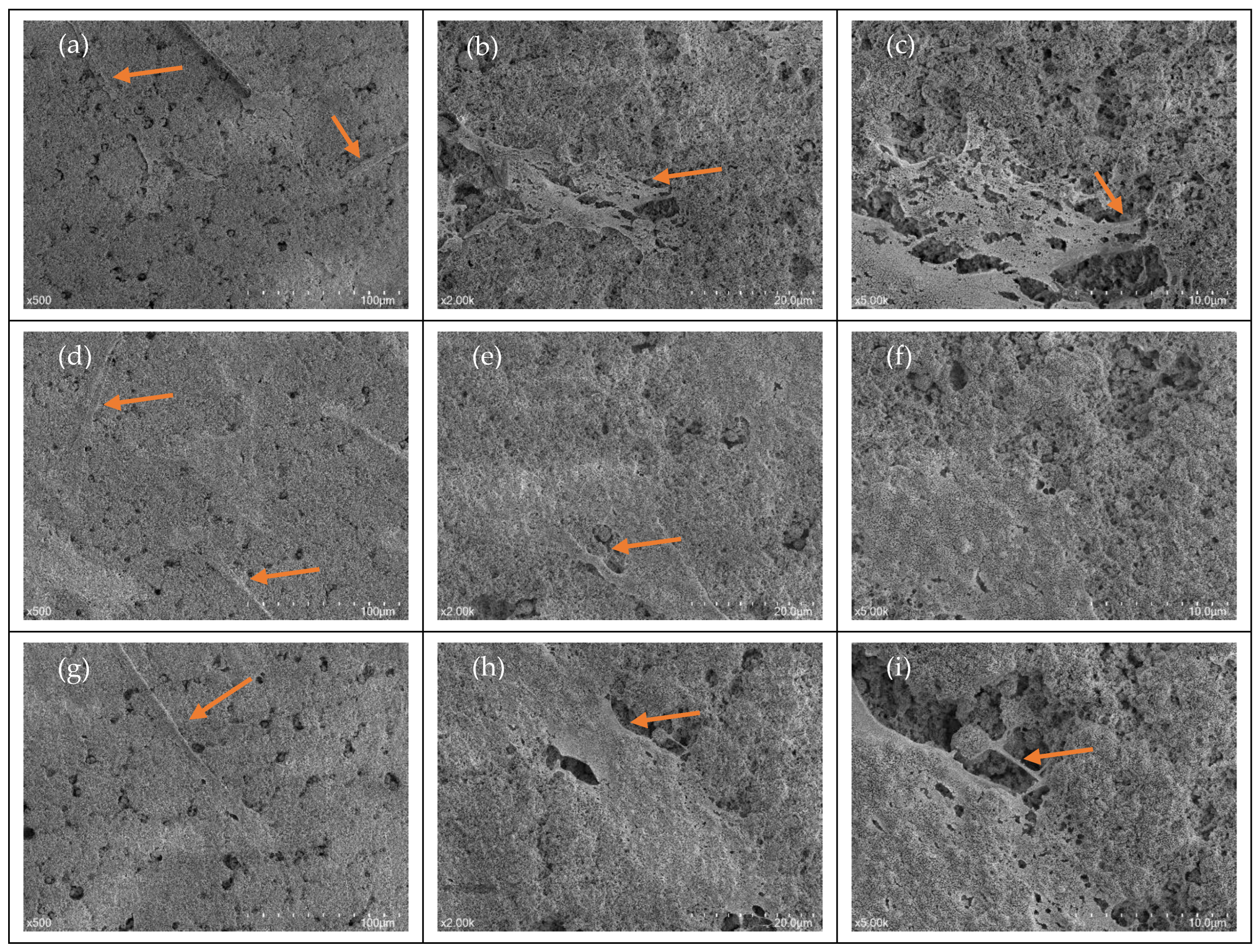
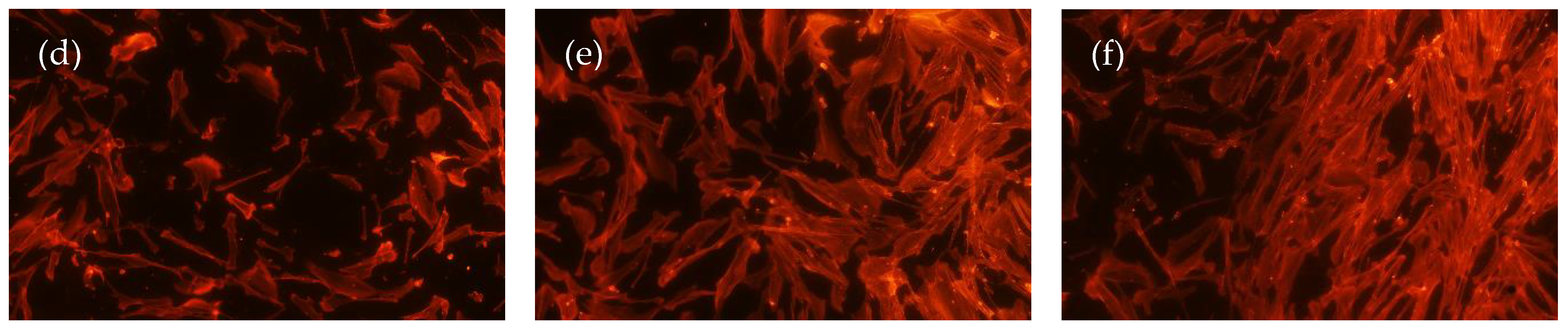
3.1. Cellular Morphology
Cellular Attachment
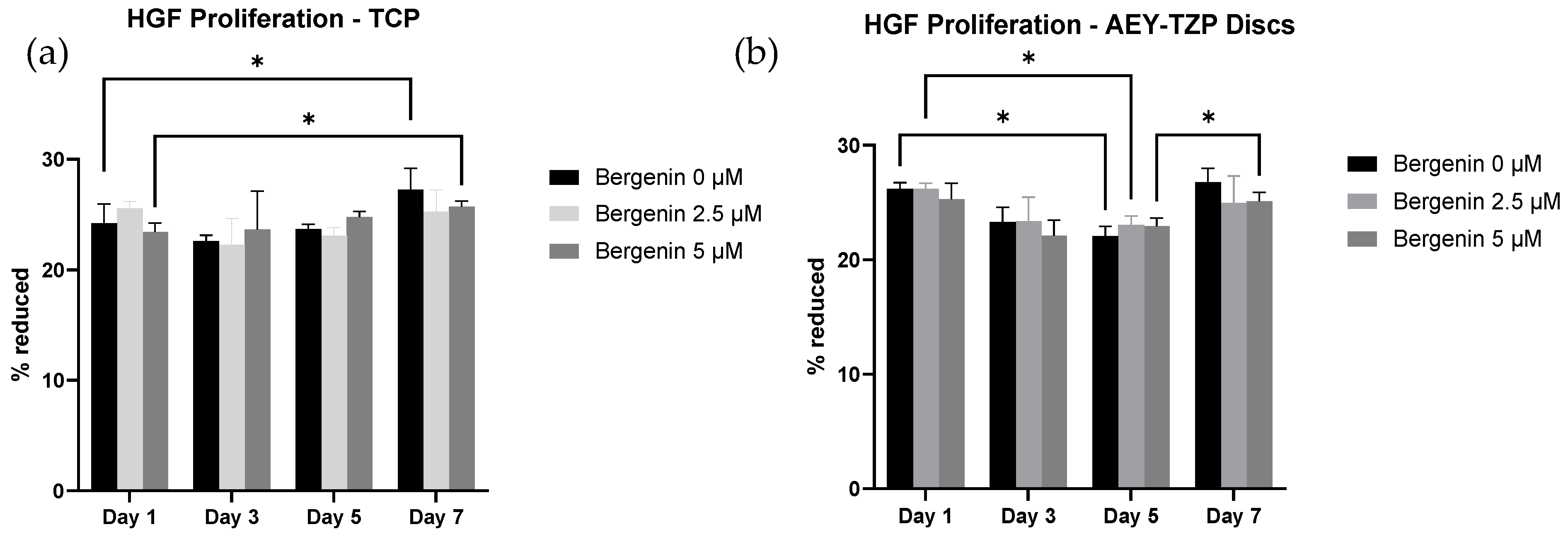
3.2. Cellular Proliferation
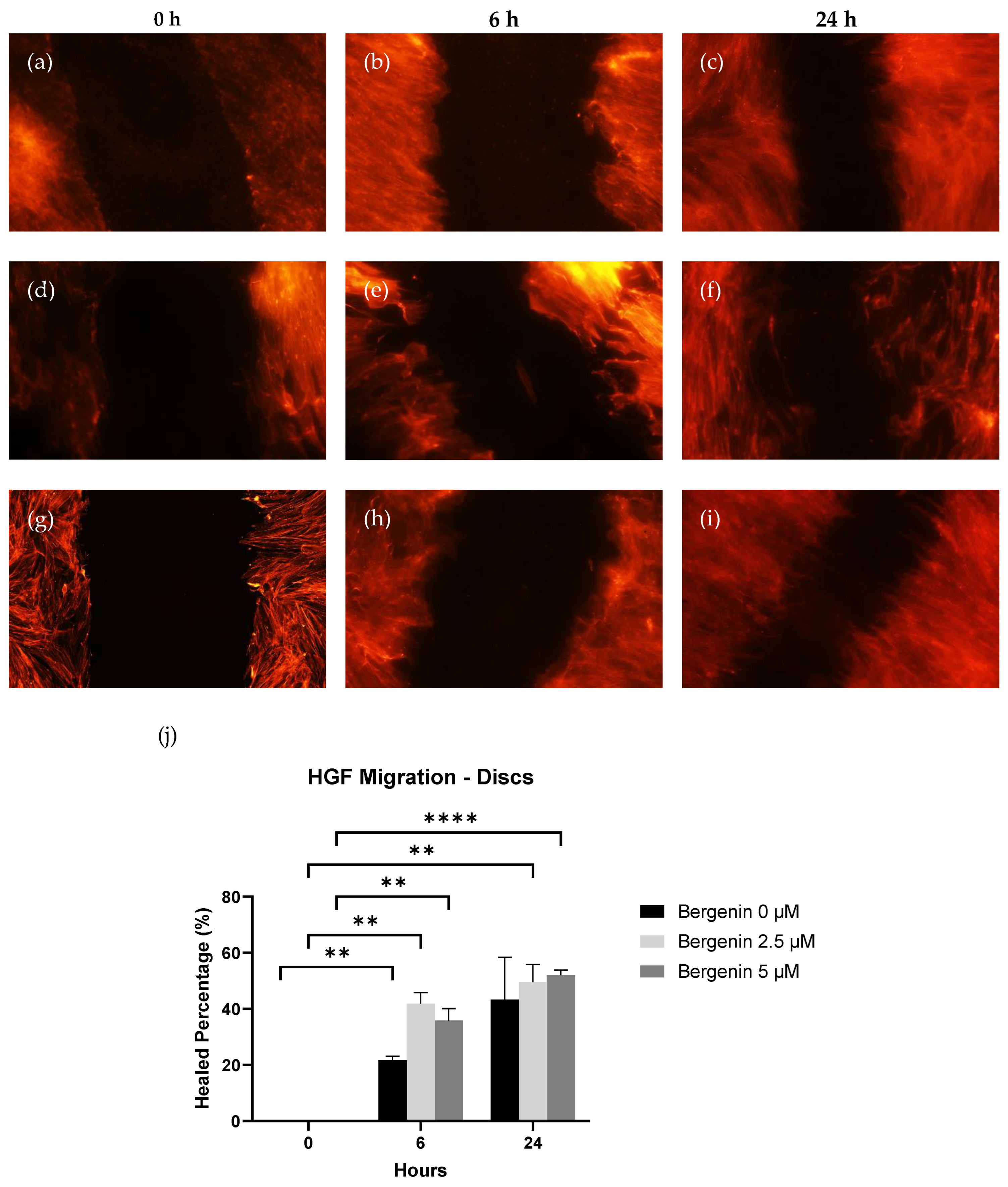
3.3. Cellular Migration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fillion, M.; Aubazac, D.; Bessadet, M.; Allegre, M.; Nicolas, E. The impact of implant treatment on oral health related quality of life in a private dental practice: A prospective cohort study. Health Qual. Life Outcomes 2013, 11, 197. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.W. Titanium Alloys for Dental Implants: A Review. Prosthesis 2020, 2, 100–116. [Google Scholar] [CrossRef]
- Özcan, M.; Hämmerle, C. Titanium as a Reconstruction and Implant Material in Dentistry: Advantages and Pitfalls. Materials 2012, 5, 1528–1545. [Google Scholar] [CrossRef]
- Ferrari, M.; Carrabba, M.; Vichi, A.; Goracci, C.; Cagidiaco, M.C. Influence of Abutment Color and Mucosal Thickness on Soft Tissue Color. Int. J. Oral. Maxillofac. Implant. 2017, 32, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Lops, D.; Stellini, E.; Sbricoli, L.; Cea, N.; Romeo, E.; Bressan, E. Influence of abutment material on peri-implant soft tissues in anterior areas with thin gingival biotype: A multicentric prospective study. Clin. Oral. Implant. Res. 2017, 28, 1263–1268. [Google Scholar] [CrossRef]
- Kim, K.T.; Eo, M.Y.; Nguyen, T.T.H.; Kim, S.M. General review of titanium toxicity. Int. J. Implant. Dent. 2019, 5, 10. [Google Scholar] [CrossRef]
- Grech, J.; Antunes, E. Zirconia in dental prosthetics: A literature review. J. Mater. Res. Technol. 2019, 8, 4956–4964. [Google Scholar] [CrossRef]
- Munro, T.; Miller, C.M.; Antunes, E.; Sharma, D. Interactions of Osteoprogenitor Cells with a Novel Zirconia Implant Surface. J. Funct. Biomater. 2020, 11, 50. [Google Scholar] [CrossRef]
- Tan, N.C.P.; Miller, C.M.; Antunes, E.; Sharma, D. Impact of physical decontamination methods on zirconia implant surface and subsequent bacterial adhesion: An in-vitro study. Clin. Exp. Dent. Res. 2022, 8, 313–321. [Google Scholar] [CrossRef]
- Lacefield, W.R. Materials characteristics of uncoated/ceramic-coated implant materials. Adv. Dent. Res. 1999, 13, 21–26. [Google Scholar] [CrossRef]
- Wenz, H.J.; Bartsch, J.; Wolfart, S.; Kern, M. Osseointegration and clinical success of zirconia dental implants: A systematic review. Int. J. Prosthodont. 2008, 21, 27–36. [Google Scholar] [PubMed]
- Moon, I.S.; Berglundh, T.; Abrahamsson, I.; Linder, E.; Lindhe, J. The barrier between the keratinized mucosa and the dental implant. An experimental study in the dog. J. Clin. Periodontol. 1999, 26, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Palaiologou, A.A.; Yukna, R.A.; Moses, R.; Lallier, T.E. Gingival, dermal, and periodontal ligament fibroblasts express different extracellular matrix receptors. J. Periodontol. 2001, 72, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Nhlapo, N.; Dzogbewu, T.C.; de Smidt, O. A systematic review on improving the biocompatibility of titanium implants using nanoparticles. Manuf. Rev. 2020, 7, 31. [Google Scholar] [CrossRef]
- Nicolas, J.; Magli, S.; Rabbachin, L.; Sampaolesi, S.; Nicotra, F.; Russo, L. 3D Extracellular Matrix Mimics: Fundamental Concepts and Role of Materials Chemistry to Influence Stem Cell Fate. Biomacromolecules 2020, 21, 1968–1994. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.C.; Lang, N.P.; Schmidlin, K.; Zwahlen, M.; Pjetursson, B.E. The effect of different implant neck configurations on soft and hard tissue healing: A randomized-controlled clinical trial. Clin. Oral. Implant. Res. 2011, 22, 14–19. [Google Scholar] [CrossRef]
- Zhao, B.; van der Mei, H.C.; Subbiahdoss, G.; de Vries, J.; Rustema-Abbing, M.; Kuijer, R.; Busscher, H.J.; Ren, Y. Soft tissue integration versus early biofilm formation on different dental implant materials. Dent. Mater. 2014, 30, 716–727. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29 (Suppl. S3), 197–212; discussion 232–193. [Google Scholar] [CrossRef]
- Louropoulou, A.; Slot, D.E.; Van der Weijden, F. The effects of mechanical instruments on contaminated titanium dental implant surfaces: A systematic review. Clin. Oral. Implant. Res. 2014, 25, 1149–1160. [Google Scholar] [CrossRef]
- Mahato, N.; Wu, X.; Wang, L. Management of peri-implantitis: A systematic review, 2010–2015. Springerplus 2016, 5, 105. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammacher, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head. Face Med. 2014, 10, 34. [Google Scholar] [CrossRef]
- Wang, W.C.; Lagoudis, M.; Yeh, C.W.; Paranhos, K.S. Management of peri-implantitis—A contemporary synopsis. Singap. Dent. J. 2017, 38, 8–16. [Google Scholar] [CrossRef]
- Flemingson; Emmadi, P.; Ambalavanan, N.; Ramakrishnan, T.; Vijayalakshmi, R. Effect of three commercial mouth rinses on cultured human gingival fibroblast: An in vitro study. Indian J. Dent. Res. 2008, 19, 29–35. [Google Scholar] [CrossRef]
- Wyganowska-Swiatkowska, M.; Kotwicka, M.; Urbaniak, P.; Nowak, A.; Skrzypczak-Jankun, E.; Jankun, J. Clinical implications of the growth-suppressive effects of chlorhexidine at low and high concentrations on human gingival fibroblasts and changes in morphology. Int. J. Mol. Med. 2016, 37, 1594–1600. [Google Scholar] [CrossRef]
- Gutierrez-Venegas, G.; Guadarrama-Solis, A.; Munoz-Seca, C.; Arreguin-Cano, J.A. Hydrogen peroxide-induced apoptosis in human gingival fibroblasts. Int. J. Clin. Exp. Pathol. 2015, 8, 15563–15572. [Google Scholar] [PubMed]
- Wilken, R.; Botha, S.J.; Grobler, A.; Germishuys, P.J. In vitro cytotoxicity of chlorhexidine gluconate, benzydamine-HCl and povidone iodine mouthrinses on human gingival fibroblasts. SADJ 2001, 56, 455–460. [Google Scholar] [PubMed]
- Cline, N.V.; Layman, D.L. The effects of chlorhexidine on the attachment and growth of cultured human periodontal cells. J. Periodontol. 1992, 63, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Lima, N.M.F.; Peruzzo, D.C.; Passador-Santos, F.; Saba-Chufji, E.; Martinez, E.F. In vitro evaluation of gingival fibroblasts proliferation and smear layer formation in pre-conditioned root surfaces. RGO Rev. Gaúcha Odontol. 2016, 64, 387–392. [Google Scholar] [CrossRef]
- Adegboye, O.; Field, M.A.; Kupz, A.; Pai, S.; Sharma, D.; Smout, M.J.; Wangchuk, P.; Wong, Y.; Loiseau, C. Natural-Product-Based Solutions for Tropical Infectious Diseases. Clin. Microbiol. Rev. 2021, 34, e0034820. [Google Scholar] [CrossRef]
- Chen, M.; Ye, C.; Zhu, J.; Zhang, P.; Jiang, Y.; Lu, X.; Wu, H. Bergenin as a Novel Urate-Lowering Therapeutic Strategy for Hyperuricemia. Front. Cell Dev. Biol. 2020, 8, 703. [Google Scholar] [CrossRef] [PubMed]
- Bajracharya, G.B. Diversity, pharmacology and synthesis of bergenin and its derivatives: Potential materials for therapeutic usages. Fitoterapia 2015, 101, 133–152. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Li, Y.; Liu, X.; Huang, Y.; Shen, Y.; Wang, J.; Liu, Z.; Zhao, Y. In vivo and in vitro antimalarial activity of bergenin. Biomed. Rep. 2014, 2, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Nunomura, R.C.S.; Oliveira, V.G.; Da Silva, S.L.; Nunomura, S.M. Characterization of bergenin in Endopleura uchi bark and its anti-inflammatory activity. J. Braz. Chem. Soc. 2009, 20, 1060–1064. [Google Scholar] [CrossRef]
- Suh, K.S.; Chon, S.; Choi, E.M. Bergenin increases osteogenic differentiation and prevents methylglyoxal-induced cytotoxicity in MC3T3-E1 osteoblasts. Cytotechnology 2018, 70, 215–224. [Google Scholar] [CrossRef]
- Sakurai, K.; Kurtz, A.; Stacey, G.; Sheldon, M.; Fujibuchi, W. First Proposal of Minimum Information About a Cellular Assay for Regenerative Medicine. Stem Cells Transl. Med. 2016, 5, 1345–1361. [Google Scholar] [CrossRef]
- Faggion, C.M., Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef]
- Xu, Z.; He, Y.; Zeng, X.; Zeng, X.; Huang, J.; Lin, X.; Chen, J. Enhanced Human Gingival Fibroblast Response and Reduced Porphyromonas gingivalis Adhesion with Titania Nanotubes. Biomed. Res. Int. 2020, 2020, 5651780. [Google Scholar] [CrossRef]
- Zizzari, V.; Borelli, B.; De Colli, M.; Tumedei, M.; Di Iorio, D.; Zara, S.; Sorrentino, R.; Cataldi, A.; Gherlone, E.F.; Zarone, F.; et al. SEM evaluation of human gingival fibroblasts growth onto CAD/CAM zirconia and veneering ceramic for zirconia. Ann. Stomatol. 2013, 4, 244–249. [Google Scholar]
- Liu, Y.; Rath, B.; Tingart, M.; Eschweiler, J. Role of implants surface modification in osseointegration: A systematic review. J. Biomed. Mater. Res. A 2020, 108, 470–484. [Google Scholar] [CrossRef]
- Rausch, M.A.; Shokoohi-Tabrizi, H.; Wehner, C.; Pippenger, B.E.; Wagner, R.S.; Ulm, C.; Moritz, A.; Chen, J.; Andrukhov, O. Impact of Implant Surface Material and Microscale Roughness on the Initial Attachment and Proliferation of Primary Human Gingival Fibroblasts. Biology 2021, 10, 356. [Google Scholar] [CrossRef] [PubMed]
- Rohr, N.; Zeller, B.; Matthisson, L.; Fischer, J. Surface structuring of zirconia to increase fibroblast viability. Dent. Mater. 2020, 36, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Pae, A.; Lee, H.; Kim, H.S.; Kwon, Y.D.; Woo, Y.H. Attachment and growth behaviour of human gingival fibroblasts on titanium and zirconia ceramic surfaces. Biomed. Mater. 2009, 4, 025005. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Tallarico, M.; Penarrocha-Oltra, D.; Monje, A.; Wang, H.L.; Penarrocha-Diago, M. Implant Abutment Cleaning by Plasma of Argon: 5-Year Follow-Up of a Randomized Controlled Trial. J. Periodontol. 2016, 87, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Garcia, B.; Camacho, F.; Penarrocha, D.; Tallarico, M.; Perez, S.; Canullo, L. Influence of plasma cleaning procedure on the interaction between soft tissue and abutments: A randomized controlled histologic study. Clin. Oral. Implant. Res. 2017, 28, 1269–1277. [Google Scholar] [CrossRef]
- D’Ercole, S.; Cellini, L.; Pilato, S.; Di Lodovico, S.; Iezzi, G.; Piattelli, A.; Petrini, M. Material characterization and Streptococcus oralis adhesion on Polyetheretherketone (PEEK) and titanium surfaces used in implantology. J. Mater. Sci. Mater. Med. 2020, 31, 84. [Google Scholar] [CrossRef]
- Peng, T.Y.; Lin, D.J.; Mine, Y.; Tasi, C.Y.; Li, P.J.; Shih, Y.H.; Chiu, K.C.; Wang, T.H.; Hsia, S.M.; Shieh, T.M. Biofilm Formation on the Surface of (Poly)Ether-Ether-Ketone and In Vitro Antimicrobial Efficacy of Photodynamic Therapy on Peri-Implant Mucositis. Polymers 2021, 13, 940. [Google Scholar] [CrossRef]
- Azizi, B.; Budimir, A.; Bago, I.; Mehmeti, B.; Jakovljevic, S.; Kelmendi, J.; Stanko, A.P.; Gabric, D. Antimicrobial efficacy of photodynamic therapy and light-activated disinfection on contaminated zirconia implants: An in vitro study. Photodiagnosis Photodyn. Ther. 2018, 21, 328–333. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, J.; Miller, C.M.; Sharma, D. Effect of Bergenin on Human Gingival Fibroblast Response on Zirconia Implant Surfaces: An In Vitro Study. J. Funct. Biomater. 2023, 14, 474. https://doi.org/10.3390/jfb14090474
Xiong J, Miller CM, Sharma D. Effect of Bergenin on Human Gingival Fibroblast Response on Zirconia Implant Surfaces: An In Vitro Study. Journal of Functional Biomaterials. 2023; 14(9):474. https://doi.org/10.3390/jfb14090474
Chicago/Turabian StyleXiong, John, Catherine M. Miller, and Dileep Sharma. 2023. "Effect of Bergenin on Human Gingival Fibroblast Response on Zirconia Implant Surfaces: An In Vitro Study" Journal of Functional Biomaterials 14, no. 9: 474. https://doi.org/10.3390/jfb14090474
APA StyleXiong, J., Miller, C. M., & Sharma, D. (2023). Effect of Bergenin on Human Gingival Fibroblast Response on Zirconia Implant Surfaces: An In Vitro Study. Journal of Functional Biomaterials, 14(9), 474. https://doi.org/10.3390/jfb14090474