


Guided Tissue Regeneration of Periodontal Infrabony Defects with Frozen Radiation-Sterilized Allogenic Bone Graft Versus Deproteinized Bovine Bone Mineral: 5-Year Outcomes of RCT




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Clinical Measurements
- -
- CAL: distance between the cementoenamel junction (CEJ) or between the apical margin of the crown/restoration and the pocket base;
- -
- PPD: distance between the gingival margin and the pocket base;
- -
- Gingival recession (GR): distance between the CEJ and gingival margin;
- -
- FMPS: the percentage of teeth surfaces with the presence of plaque [24]; all surfaces of all teeth were scored;
- -
- FMBS: the percentage of pockets bleeding after probing [25]; all surfaces of all teeth were scored.
- -
- CAL-G1 = CAL0–CAL1 (after 1 year);
- -
- CAL-G5 = CAL0–CAL5 (after 5 years);
- -
- PPD-R1 = PPD0–PPD1 (after 1 year);
- -
- PPD-R5 = PPD0– PPD5 (after 5 years);
- -
- GR1 = GR0–GR1 (after 1 year);
- -
- GR5 = GR0–GR5 (after 5 years).
2.4. Radiographic Measurements
- -
- CEJ-BD: the distance from the CEJ to the bottom of the defect;
- -
- CEJ-AC: the distance from the CEJ to the interdental bone crest;
- -
- DD: the distance from the spot where the AUX2 crossed the CEJ–BD line to the BD;
- -
- Radiographic angle: the angle between the AUX1 and AUX2 of the treated tooth.
- -
- LDF1 = CEJ-BD1-CEJBD0 (after 1 year);
- -
- LDF5 = CEJ-BD5-CEJ-BD0 (after 5 years);
- -
- %DF1 = LDF1/DD0 (after 1 year);
- -
- %DF5 = LDF5/DD0 (after 5 years).
2.5. Randomization and Allocation Concealment
2.6. Surgical Procedures and Intra-Surgical Measurements
- -
- Defect depth: the distance from the bottom of the defect to the most coronal point of the bony walls surrounding the defect;
- -
- Defect width: the distance between the most coronal part of the bony walls surrounding the defect and the root surface;
- -
- Defect morphology: defects were divided into one-wall, two-wall, and three-wall defects based on the number of present walls.
2.7. Post-Surgical Period and Supportive Periodontal Care
- -
- BOP was observed at >10% of sites, and
- -
- sites with a PPD ≥ 4 mm which exhibited bleeding on probing were present [4].
2.8. Statistical Analysis
3. Results
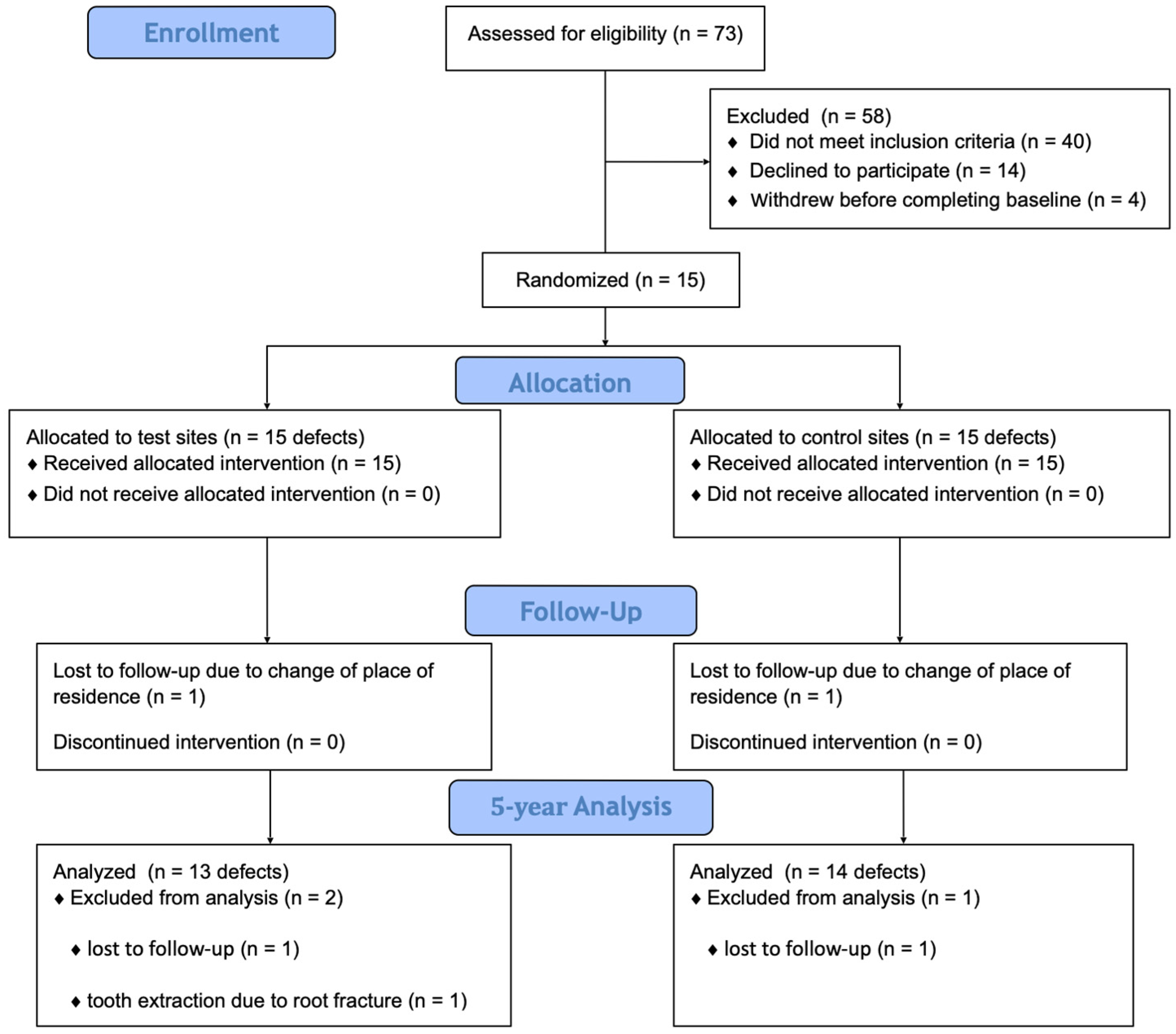
3.1. Experimental Population
3.2. Clinical and Radiographic Outcomes
3.3. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BD | Base of the Defect |
| CAL | Clinical Attachment Level |
| CAL-G | Clinical Attachment Level Gain |
| CEJ | Cementoenamel Junction |
| CI | Confidence Interval |
| DBBM | Deproteinized Bovine Bone Mineral |
| DBM | Demineralized Bone Matrix |
| DD | Radiographic Defect Depth |
| DFDBA | Demineralized Freeze-Dried Bone Allograft |
| FDBA | Freeze-Dried Bone Allograft |
| FMBS | Full-mouth Bleeding Score |
| FMPS | Full-mouth Plaque Score |
| FRSABG | Frozen Radiation-Sterilized Allogenic Bone Graft |
| GR | Gingival Recession |
| GTR | Guided Tissue Regeneration |
| LDF | Linear Defect Fill |
| MPPT | Modified Papilla Preservation Technique |
| n | Number of Defects |
| OFD | Open-Flap Debridement |
| PPD | Probing Pocket Depth |
| PPD-R | Probing Pocket Depth Reduction |
| PRF | Platelet-Rich Fibrin |
| RCT | Randomized Controlled Trial |
| SD | Standard Deviation |
| SPC | Supportive Periodontal Care |
| SPPF | Simplified Papilla Preservation Flap |
| %DF | Percentage Defect Fill |
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S162–S170. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Wennströmm, J.L. The angular bony defect as indicator of further alveolar bone loss. J. Clin. Periodontol. 1991, 18, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Rams, T.E.; Listgarten, M.A.; Slots, J. Radiographic alveolar bone morphology and progressive periodontitis. J. Periodontol. 2018, 89, 424–430. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultant. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49 (Suppl. S24), 4–71. [Google Scholar] [CrossRef]
- Zhou, Z.; Yun, J.; Li, J.; Chen, Y.; Duan, T.; Wang, L.; Han, J.; Jiang, H.B.; Niu, G. Comparison of the efficacy of different biodegradable membranes in guided bone/tissue regeneration: A systematic review and network meta-analysis. Biomed. Mater. 2023, 19, 3. [Google Scholar] [CrossRef]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal regeneration-intrabony defects: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86 (Suppl. S2), S77–S104. [Google Scholar] [CrossRef] [PubMed]
- Bowers, G.M.; Chadroff, B.; Carnevale, R.; Mellonig, J.; Corio, R.; Emerson, J.; Stevens, M.; Romberg, E. Histologic evaluation of new attachment apparatus formation in humans. Part II. J. Periodontol. 1989, 60, 675–682. [Google Scholar] [CrossRef]
- Mellonig, J.T. Human histologic evaluation of a bovine-derived bone xenograft in the treatment of periodontal osseous defects. Int. J. Periodontics Restor. Dent. 2000, 20, 19–29. [Google Scholar]
- Sculean, A.; Nikolidakis, D.; Nikou, G.; Ivanovic, A.; Chapple, I.L.; Stavropoulos, A. Biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontol. 2000 2015, 68, 182–216. [Google Scholar] [CrossRef]
- Reynolds, M.A.; Kao, R.T.; Camargo, P.M.; Caton, J.G.; Clem, D.S.; Fiorellini, J.P.; Geisinger, M.L.; Mills, M.P.; Nares, S.; Nevins, M.L. Periodontal regeneration-intrabony defects: A consensus report from the AAP Regeneration Workshop. J. Periodontol. 2015, 86 (Suppl. S2), S105–S107. [Google Scholar] [CrossRef]
- Ciszyński, M.; Dominiak, S.; Dominiak, M.; Gedrange, T.; Hadzik, J. Allogenic Bone Graft in Dentistry: A Review of Current Trends and Developments. Int. J. Mol. Sci. 2023, 24, 16598. [Google Scholar] [CrossRef] [PubMed]
- Boyan, B.D.; Ranly, D.M.; McMillan, J.; Sunwoo, M.; Roche, K.; Schwartz, Z. Osteoinductive ability of human allograft formulations. J. Periodontol. 2006, 77, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Grassi, F.R.; Grassi, R.; Vivarelli, L.; Dallari, D.; Govoni, M.; Nardi, G.M.; Kalemaj, Z.; Ballini, A. Design Techniques to Optimize the Scaffold Performance: Freeze-dried Bone Custom-made Allografts for Maxillary Alveolar Horizontal Ridge Augmentation. Materials 2020, 13, 1393. [Google Scholar] [CrossRef] [PubMed]
- Bright, R.W.; Friedlaender, G.E.; Sell, K.W. Tissue banking: The United States Navy Tissue Bank. Mil. Med. 1977, 142, 503–510. [Google Scholar] [CrossRef]
- Gocke, D.J. Tissue donor selection and safety. Clin. Orthop. Relat. Res. 2005, 435, 17–21. [Google Scholar] [CrossRef]
- Dziedzic-Goclawska, A.; Kamiński, A.; Uhrynowska-Tyszkiewicz, I.; Stachowicz, W. Irradiation as a safety procedure in tissue banking. Cell Tissue Bank. 2005, 6, 201–219. [Google Scholar] [CrossRef]
- Dziedzic-Gocławska, A.; Ostrowski, K.; Stachowicz, W.; Michalik, J.; Grzesik, W. Effect of radiation sterilization on the osteoinductive properties and the rate of remodelling of bone implants preserved by lyophilization and deep-freezing. Clin. Orthop. 1991, 272, 30–37. [Google Scholar] [CrossRef]
- Brodzikowska, A.; Górski, B.; Szerszeń, M.; Sanz, M. Efficacy of Guided Tissue Regeneration Using Frozen Radiation-Sterilized Allogenic Bone Graft as Bone Replacement Graft Compared with Deproteinized Bovine Bone Mineral in the Treatment of Periodontal Intra-Bony Defects: Randomized Controlled Trial. J. Clin. Med. 2023, 12, 1396. [Google Scholar] [CrossRef]
- De Ry, S.P.; Pagnamenta, M.; Ramseier, C.A.; Roccuzzo, A.; Salvi, G.E.; Sculean, A. Five-year results following regenerative periodontal surgery with an enamel matrix derivative in patients with different smoking status. Quintessence Int. 2022, 53, 832–838. [Google Scholar]
- Mengel, R.; Schreiber, D.; Flores-de-Jacoby, L. Bioabsorbable membrane and bioactive glass in the treatment of intrabony defects in patients with generalized aggressive periodontitis: Results of a 5-year clinical and radiological study. J. Periodontol. 2006, 77, 1781–1787. [Google Scholar] [CrossRef]
- Heden, G.; Wennström, J.L. Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bone defects. J. Periodontol. 2006, 77, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Stalpers, G.; Mollo, A.; Tonetti, M.S. Periodontal regeneration versus extraction and prosthetic replacement of teeth severely compromised by attachment loss to the apex: 5-year results of an ongoing randomized clinical trial. J. Clin. Periodontol. 2011, 38, 915–924. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Pini-Prato, G.; Tonetti, M.S. Periodontal regeneration of human infrabony defects I. Clinical measures. J Periodontol. 1995, 64, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Pini-Prato, G.; Tonetti, M.S. The modified papilla preservation technique. A new surgical approach for interproximal regenerative procedures. J. Periodontol. 1995, 66, 261–266. [Google Scholar] [CrossRef]
- Cortellini, P.; Pini-Prato, G.; Tonetti, M.S. The simplified papilla preservation flap. A novel surgical approach for the management of soft tissues in regenerative procedures. Int. J. Periodontics Restor. Dent. 1999, 19, 589–599. [Google Scholar]
- Nibali, L.; Koidou, V.P.; Nieri, M.; Barbato, L.; Pagliaro, U.; Cairo, F. Regenerative surgery versus access flap for the treatment of intra-bony periodontal defects: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 320–351. [Google Scholar] [CrossRef]
- Sculean, A.; Schwarz, F.; Chiantella, G.C.; Donos, N.; Arweiler, N.B.; Brecx, M.; Becker, J. Five-year results of a prospective, randomized, controlled study evaluating treatment of intra-bony defects with a natural bone mineral and GTR. J. Clin. Periodontol. 2007, 34, 72–77. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Karring, T. Guided tissue regeneration combined with a deproteinized bovine bone mineral (Bio-Oss) in the treatment of intrabony periodontal defects: 6-year results from a randomized-controlled clinical trial. J. Clin. Periodontol. 2010, 37, 200–210. [Google Scholar] [CrossRef]
- Richardson, C.R.; Mellonig, J.T.; Brunsvold, M.A.; McDonnell, H.T.; Cochran, D.L. Clinical evaluation of Bio-Oss: A bovine-derived xenograft for the treatment of periodontal osseous defects in humans. J. Clin. Periodontol. 1999, 26, 421–428. [Google Scholar] [CrossRef]
- Kher, V.K.; Bhongade, M.L.; Shori, T.D.; Kolte, A.P.; Dharamthok, S.B.; Shrirao, T.S. A comparative evaluation of the effectiveness of guided tissue regeneration by using a collagen membrane with or without decalcified freeze-dried bone allograft in the treatment of infrabony defects: A clinical and radiographic study. J. Indian. Soc. Periodontol. 2013, 17, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Alshoiby, M.M.; Fawzy El-Sayed, K.M.; Elbattawy, W.; Hosny, M.M. Injectable platelet-rich fibrin with demineralized freeze-dried bone allograft compared to demineralized freeze-dried bone allograft in intrabony defects of patients with stage-III periodontitis: A randomized controlled clinical trial. Clin. Oral Investig. 2023, 7, 3457–3467. [Google Scholar] [CrossRef]
- Majzoub, J.; Barootchi, S.; Tavelli, L.; Wang, C.W.; Chan, H.L.; Wang, H.L. Guided tissue regeneration combined with bone allograft in infrabony defects: Clinical outcomes and assessment of prognostic factors. J. Periodontol. 2020, 91, 746–755. [Google Scholar] [CrossRef]
- Rummelhart, J.M.; Mellonig, J.T.; Gray, J.L.; Towle, H.J. A comparison of freeze-dried bone allograft and demineralized freeze-dried bone allograft in human periodontal osseous defects. J. Periodontol. 1989, 60, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Atchuta, A.; Gooty, J.R.; Guntakandla, V.R.; Palakuru, S.K.; Durvasula, S.; Palaparthy, R. Clinical and radiographic evaluation of platelet-rich fibrin as an adjunct to bone grafting demineralized freeze-dried bone allograft in intrabony defects. J. Indian Soc. Periodontol. 2020, 24, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.; Perrier, L.; Shakik, S.; Cairncross, Z.; Tricco, A.C.; Lix, L.; Zwarenstein, M.; Rosella, L.; Henry, D. Assessment of Long-term Follow-up of Randomized Trial Participants by Linkage to Routinely Collected Data: A Scoping Review and Analysis. JAMA Netw. Open 2018, 1, e186019. [Google Scholar] [CrossRef]
- Parikh, S. Bone graft substitutes: Past, present, future. J. Postgrad. Med. 2002, 48, 142–148. [Google Scholar]
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone regenerative medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef]
- Turco, G.; Porrelli, D.; Marsich, E.; Vecchies, F.; Lombardi, T.; Stacchi, C.; Lenarda, R. Three-Dimensional Bone Substitutes for Oral and Maxillofacial Surgery: Biological and Structural Characterization. J. Funct. Biomater. 2018, 9, 62. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Bertl, K.; Spineli, L.M.; Sculean, A.; Cortellini, P.; Tonetti, M. Medium- and long-term clinical benefits of periodontal regenerative/reconstructive procedures in intrabony defects: Systematic review and network meta-analysis of randomized controlled clinical studies. J. Clin. Periodontol. 2021, 48, 410–430. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Chiantella, G.C.; Arweiler, N.B.; Becker, J.; Schwarz, F.; Stavropoulos, A. Five-year clinical and histologic results following treatment of human intrabony defects with an enamel matrix derivative combined with a natural bone mineral. Int. J. Periodontics Restor. Dent. 2008, 28, 153–161. [Google Scholar]
- Cortellini, P.; Buti, J.; Pini Prato, G.; Tonetti, M.S. Periodontal regeneration compared with access flap surgery in human intra-bony defects 20-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence and costs. J. Clin. Periodontol. 2017, 44, 58–66. [Google Scholar] [CrossRef]
- Cortellini, P.; Paolo, G.; Prato, P.; Tonetti, M.S. Long-term stability of clinical attachment following guided tissue regeneration and conventional therapy. J. Clin. Periodontol. 1996, 23, 106–111. [Google Scholar] [CrossRef]
- Matuliene, G.; Pjetursson, B.E.; Salvi, G.E.; Schmidlin, K.; Brägger, U.; Zwahlen, M.; Lang, N.P. Influence of residual pockets on progression of periodontitis and tooth loss: Results after 11 years of maintenance. J. Clin. Periodontol. 2008, 35, 685–695. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.S. Long-term tooth survival following regenerative treatment of intrabony defects. J. Periodontol. 2004, 75, 672–678. [Google Scholar] [CrossRef]
- Górski, B.; Jalowski, S.; Górska, R.; Zaremba, M. Treatment of intrabony defects with modified perforated membranes in aggressive periodontitis: A 4-year follow-up of a randomized controlled trial. Clin. Oral Investig. 2020, 24, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.H.A.; Mallala, D.; Alrmali, A.; Shah, B.; Kumar, P.; Wang, H.L. Residual vertical defects: Risk of disease progression, retreatment rates, and cost: A retrospective analysis. Clin. Oral Investig. 2024, 28, 446. [Google Scholar] [CrossRef]
- Thayil, S.T.; Pillai, B.R.M.; Nafeesa, R.B.; Kalarikkal, R.E. Composite outcome measure (COM) and pocket closure as clinical endpoints following treatment of infra bony defects with Guided tissue regeneration and Open flap debridement. J. Indian Soc. Periodontol. 2022, 26, 570–576. [Google Scholar] [CrossRef]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Test Sites (n = 15) | Control Sites (n = 15) | p |
|---|---|---|---|
| Molars (n) | 6 | 6 | |
| Premolars (n) | 5 | 5 | |
| Incisors, canines (n) | 4 | 4 | |
| Upper teeth (n) | 7 | 8 | |
| Lower teeth (n) | 8 | 7 | |
| RVG angle (°) | 23.39 (20.39–26.40) ± 5.42 | 26.49 (22.04–30.45) ± 7.59 | 0.2467 |
| Defect depth (mm) | 6.00 (4.99–7.00) ± 1.81 | 5.80 (4.42–7.18) ± 2.48 | 0.8029 |
| Defect width (mm) | 3.73 (2.97–4.50) ± 1.39 | 3.06 (2.53–3.60) ± 0.96 | 0.1372 |
| One wall (n) | 5 | 4 | |
| Two wall (n) | 5 | 6 | |
| Three wall (n) | 5 | 5 |
| Baseline | 1 Year | 5 Years | p Baseline—1 | p Baseline—5 | p 1–5 | |
|---|---|---|---|---|---|---|
| CAL test (mm) CAL control p | 8.93 (8.13–9.73) ± 1.44 8.73 (7.81–9.69) ± 1.67 0.2219 | 3.23 (2.69–3.65) ± 0.83 4.13 (3.25–5.02) ± 1.59 0.1182 | 4.23 (3.18–5.28) ± 1.74 4.57 (3.94–5.20) ± 1.09 0.5442 | <0.0001 * <0.0001 * | <0.0001 * <0.0001 * | 0.5531 0.4663 |
| ∆CAL test (mm) ∆CAL control p | 5.54 (4.40–6.55) ± 1.18 4.54 (3.95–5.22) ± 1.11 0.0891 | 4.46 (3.21–5.71) ± 2.07 3.86 (2.77–4.94) ± 1.88 0.4330 | 0.5531 0.4663 | |||
| PPD test (mm) PPD control p | 7.67 (6.98–8.35) ± 1.23 7.40 (6.82–9.66) ± 1.06 0.3427 | 3.23 (2.69–3.65) ± 0.83 3.63 (3.21–4.06) ± 0.77 0.0429 * | 3.77 (2.98–4.56) ± 1.30 4.07 (3.30–4.84) ± 1.33 0.5561 | <0.0001 * <0.0001 * | <0.0001 * <0.0001 * | 0.4156 0.3093 |
| ∆PPD test (mm) ∆PPD control p | 4.66 (3.78–5.51) ± 1.24 3.57 (3.18–5.22) ± 1.11 0.0190 * | 3.54 (2.39–4.69) ± 1.90 3.00 (1.96–4.04) ± 1.80 0.4560 | 0.4156 0.3093 | |||
| GR test (mm) GR control p | 1.21 (5.21–6.57) ± 1.23 1.47 (0.84–2.08) ± 1.12 0.7918 | 0.66 (0.42–0.91) ± 0.45 1.03 (0.52–1.55) ± 0.93 0.1651 | 0.69 (0.07–1.32) ± 1.03 0.79 (0.18–1.39) ± 1.05 0.8178 | 0.4981 0.2610 | 0.5763 0.8764 | 0.3870 0.4041 |
| ∆GR test (mm) ∆GR control p | 0.22 (−0.28–0.75) ± 0.91 0.45 (0.11–0.78) ± 0.66 0.3281 | 0.62 (−0.02–1.725) ± 1.04 0.71 (0.10–1.33) ± 1.07 0.8101 | 0.3870 0.4041 | |||
| DD test (mm) DD control p | 5.89 (5.21–6.57) ± 1.23 5.32 (4.31–6.35) ± 1.84 0.2811 | 0.66 (0.42–0.91) ± 0.45 0.92 (0.58–1.27) ± 0.61 0.0334 * | 0.98 (0.60–1.35) ± 0.62 1.14 (0.83–1.45) ± 0.54 0.4647 | <0.0001 * <0.0001 * | <0.0001 * <0.0001 * | 0.0050 * 0.0313 * |
| LDF test (mm) LDF control p | 5.22 (4.56–5.54) ± 1.11 4.33 (3.40–5.18) ± 1.74 0.0478 * | 4.91 (4.07–5.74) ± 1.38 3.93 (3.01–4.85) ± 1.59 0.1014 | 0.0123 * 0.0177 * | |||
| %DF test (mm) %DF control p | 85.89 (81.29–95.11) ± 8.90 83.27 (77.61–90.37) ± 11.41 0.1091 | 83.06 (76.73–89.39) ± 10.47 75.78 (68.54–83.02) ± 12.54 0.1155 | 0.0197 * 0.0283 * |
| Test Sites (n = 15) | Control Sites (n = 15) | |||||||
|---|---|---|---|---|---|---|---|---|
| ≤3 mm | 4 mm | 5 mm | ≥6 mm | ≤3 mm | 4 mm | 5 mm | ≥6 mm | |
| Baseline (n = 30) | - | - | - | 15 | - | - | - | 15 |
| 1 year (n = 29) | 7 | 4 | 3 | - | 7 | 5 | 1 | 1 |
| 4 years (n = 27) | 5 | 4 | 3 | 1 | 5 | 3 | 4 | 2 |
| Parameter | Regression Coefficient | Standard ERROR | Confidence Interval | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Intercept | 0.008 * | ||||
| Sex (male vs. female) | 0.191 | 0.236 | −0.315 | 0.696 | 0.431 |
| Age | 0.160 | 0.142 | −0.144 | 0.464 | 0.278 |
| Surgical procedure (test vs. control) | −0.135 | 0.152 | −0.462 | 0.192 | 0.391 |
| Tooth type (molars vs. incisors, canines, and premolars) | 0.104 | 0.214 | −0.355 | 0.563 | 0.634 |
| Tooth position (upper vs. lower) | −0.016 | 0.190 | −0.424 | 0.391 | 0.933 |
| FMPS | 0.046 | 0.279 | −0.552 | 0.643 | 0.871 |
| FMBS | 0.214 | 0.257 | −0.336 | 0.765 | 0.418 |
| PPD | 0.255 | 0.206 | −0.187 | 0.698 | 0.236 |
| DD | 0.214 | 0.186 | −0.184 | 0.612 | 0.269 |
| RVG angle | 0.159 | 0.177 | −0.220 | 0.537 | 0.383 |
| Patients’ compliance (1 vs. 0) | −0.059 | 0.178 | −0.442 | 0.323 | 0.745 |
| Periodontitis recurrence (1 vs. 0) | 0.828 | 0.164 | 0.477 | 1.180 | <0.001 * |
| Parameter | Regression Coefficient | Standard Error | Confidence Interval | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Intercept | 0.192 | ||||
| Sex (male vs. female) | −0.071 | 0.328 | −0.7777 | 0.630 | 0.825 |
| Age | −0.273 | 0.200 | −0.703 | 0.156 | 0.194 |
| Surgical procedure (test vs. control) | −0.121 | 0.215 | −0.582 | 0.340 | 0.582 |
| Tooth type (molars vs. incisors, canines, and premolars) | 0.231 | 0.316 | −0.447 | 0.910 | 0.476 |
| Tooth position (upper vs. lower) | −0.244 | 0.389 | −1.078 | 0.589 | 0.540 |
| FMPS | 0.099 | 0.347 | −0.645 | 0.842 | 0.780 |
| FMBS | −0.330 | 0.285 | −0.942 | 0.281 | 0.266 |
| CAL | −0.057 | 0.261 | −0.617 | 0.504 | 0.832 |
| DD | 0.027 | 0.249 | −0.506 | 0.561 | 0.914 |
| RVG angle | −0.244 | 0.389 | −1.078 | 0.589 | 0.540 |
| Patients’ compliance (1 vs. 0) | −0.208 | 0.252 | −0.748 | 0.332 | 0.423 |
| Periodontitis recurrence (1 vs. 0) | 0.407 | 0.238 | −0.103 | 0.916 | 0.109 |
| Parameter | Regression Coefficient | Standard Error | Confidence Interval | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Intercept | 0.303 | ||||
| Sex (male vs. female) | −0.163 | 0.235 | −0.666 | 0.341 | 0.500 |
| Age | −0.190 | 0.146 | −0.503 | 0.123 | 0.215 |
| Surgical procedure (test vs. control) | −0.021 | 0.151 | −0.345 | 0.303 | 0.891 |
| Tooth type (molars vs. incisors, canines, and premolars) | −0.082 | 0.241 | −0.600 | 0.435 | 0.738 |
| Tooth position (upper vs. lower) | −0.031 | 0.195 | −0.450 | 0.388 | 0.876 |
| FMPS | −0.262 | 0.287 | −0.877 | 0.354 | 0.378 |
| FMBS | 0.527 | 0.256 | −0.022 | 1.077 | 0.059 |
| PPD | 0.097 | 0.238 | −0.414 | 0.608 | 0.690 |
| CAL | 0.071 | 0.234 | −0.431 | 0.572 | 0.767 |
| RVG angle | 0.047 | 0.177 | −0.331 | 0.426 | 0.793 |
| Patients’ compliance (1 vs. 0) | −0.363 | 0.184 | −0.757 | 0.031 | 0.068 |
| Periodontitis recurrence (1 vs. 0) | 0.763 | 0.172 | 0.394 | 1.131 | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Górski, B.; Brodzikowska, A.; Nijakowski, K.; Sanz, M. Guided Tissue Regeneration of Periodontal Infrabony Defects with Frozen Radiation-Sterilized Allogenic Bone Graft Versus Deproteinized Bovine Bone Mineral: 5-Year Outcomes of RCT. J. Funct. Biomater. 2025, 16, 95. https://doi.org/10.3390/jfb16030095
Górski B, Brodzikowska A, Nijakowski K, Sanz M. Guided Tissue Regeneration of Periodontal Infrabony Defects with Frozen Radiation-Sterilized Allogenic Bone Graft Versus Deproteinized Bovine Bone Mineral: 5-Year Outcomes of RCT. Journal of Functional Biomaterials. 2025; 16(3):95. https://doi.org/10.3390/jfb16030095
Chicago/Turabian StyleGórski, Bartłomiej, Aniela Brodzikowska, Kacper Nijakowski, and Mariano Sanz. 2025. "Guided Tissue Regeneration of Periodontal Infrabony Defects with Frozen Radiation-Sterilized Allogenic Bone Graft Versus Deproteinized Bovine Bone Mineral: 5-Year Outcomes of RCT" Journal of Functional Biomaterials 16, no. 3: 95. https://doi.org/10.3390/jfb16030095
APA StyleGórski, B., Brodzikowska, A., Nijakowski, K., & Sanz, M. (2025). Guided Tissue Regeneration of Periodontal Infrabony Defects with Frozen Radiation-Sterilized Allogenic Bone Graft Versus Deproteinized Bovine Bone Mineral: 5-Year Outcomes of RCT. Journal of Functional Biomaterials, 16(3), 95. https://doi.org/10.3390/jfb16030095