
Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Isolation and Identification of Isolates
2.2. Antibiotic Susceptibility Testing
2.3. Detection of Imipenem and Amikacin MIC for Isolated P. aeruginosa Isolates
2.4. Molecular Detection of bla IMP and aac(6′)-Ib by PCR
2.5. Determination of the Combined Effect between Amikacin and Imipenem against Resistant P. aeruginosa by Checkerboard Technique
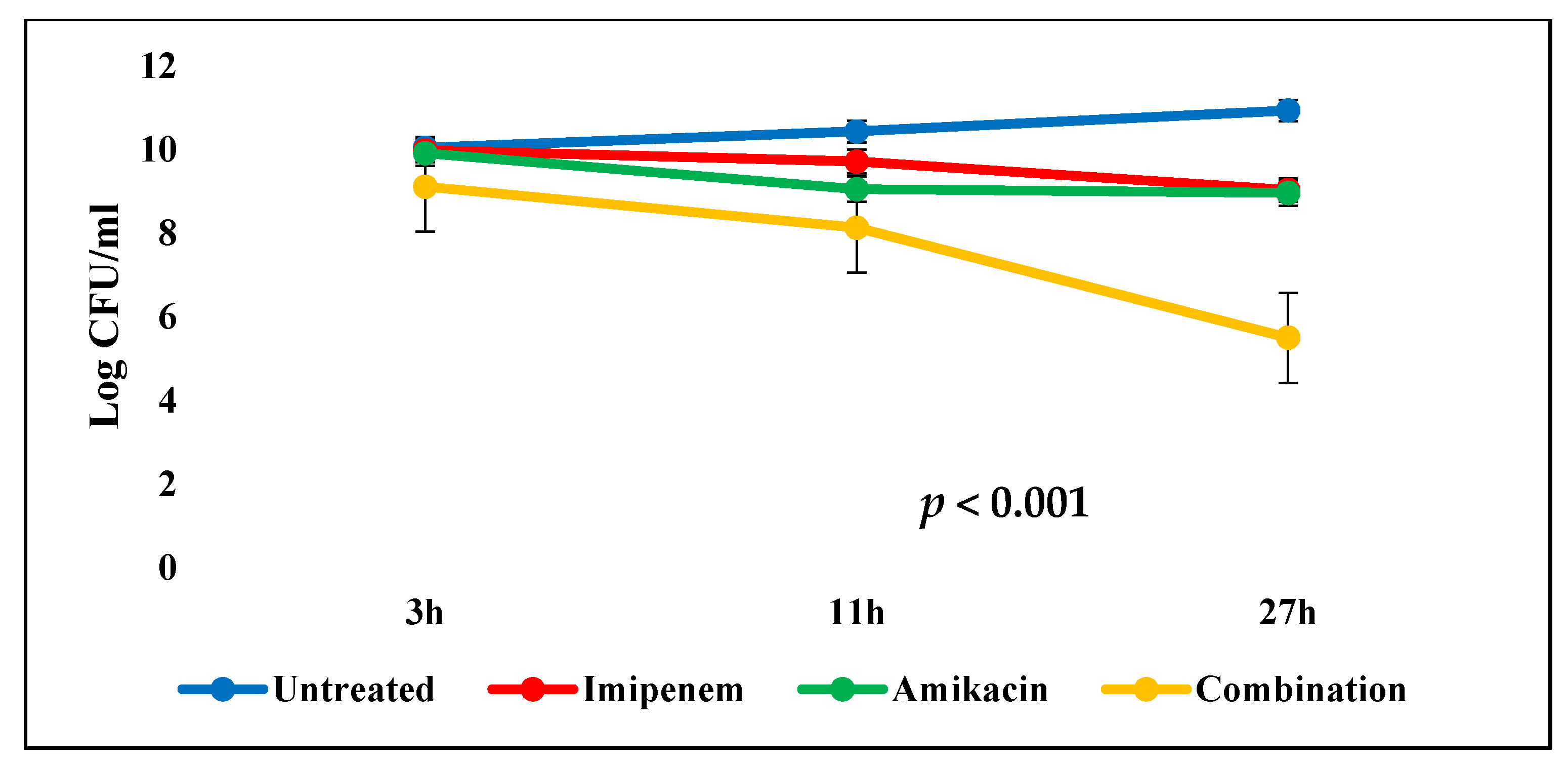
2.6. Time–Kill Studies
2.7. Gene Expression
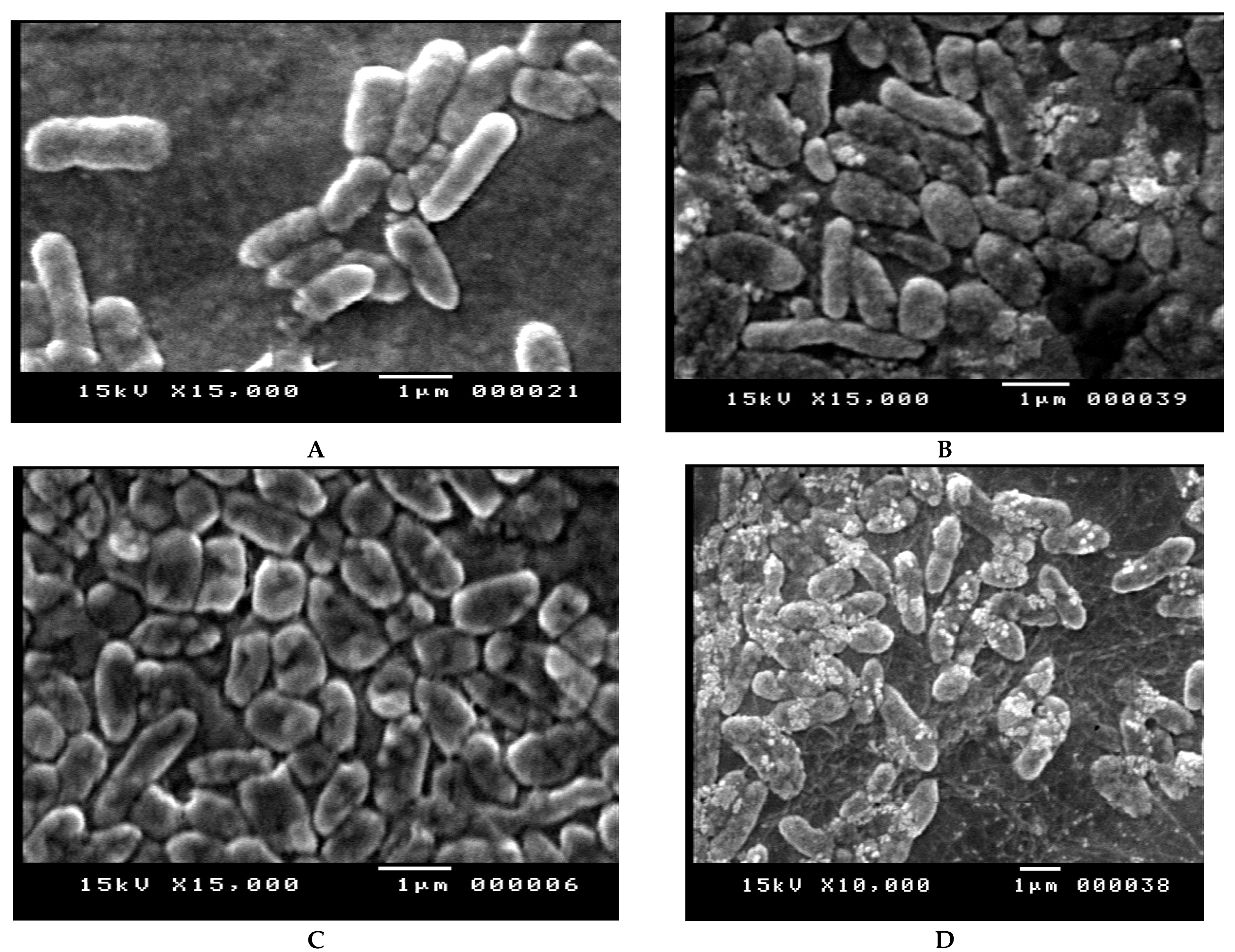
2.8. Scanning Electron Microscopy (SEM)
2.9. In Vivo Studies
3. Discussion
4. Materials and Methods
4.1. Bacterial Isolates
4.2. Antimicrobial Susceptibility Test
4.3. Molecular Detection of bla IMP and aac(6′)-Ib by PCR
4.4. Checkerboard Synergy Testing
4.5. Time-Killing Assay
4.6. Gene Expression of bla IMP and aac(6′)-Ib Combination by Real-Time PCR
4.7. Scanning Electron Microscopy (SEM)
4.8. In Vivo Studies
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Control, Centers for Disease, and Prevention. In Antibiotic Resistance Threats in the United States; Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Moustafa, D.A.; Wu, A.W.; Zamora, D.; Daly, S.M.; Sturge, C.R.; Pybus, C.; Geller, B.L.; Goldberg, J.B.; Greenberg, D.E. Peptide-Conjugated Phosphorodiamidate Morpholino Oligomers Retain Activity against Multidrug-Resistant Pseudomonas Aeruginosa in Vitro and in Vivo. mBio 2021, 12, e02411-20. [Google Scholar] [CrossRef] [PubMed]
- Paz-Zarza, V.M.; Mangwani-Mordani, S.; Martinez-Maldonado, A.; Alvarez-Hernandez, D.; Solano-Galvez, S.G.; Vazquez-Lopez, R. Pseudomonas Aeruginosa: Pathogenicity and Antimicrobial Resistance in Urinary Tract Infection. Rev. Chil. Infectol. 2019, 36, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Luepke, K.H.; Mohr, J.F., 3rd. The Antibiotic Pipeline: Reviving Research and Development and Speeding Drugs to Market. Expert Rev. Anti. Infect. Ther. 2017, 15, 425–433. [Google Scholar] [PubMed]
- Chinese, X.D.R.; Consensus Working Group; Guan, X.; He, L.; Hu, B.; Hu, J.; Huang, X.; Lai, G.; Li, Y.; Liu, Y.; et al. Laboratory Diagnosis, Clinical Management and Infection Control of the Infections Caused by Extensively Drug-Resistant Gram-Negative Bacilli: A Chinese Consensus Statement. Clin. Microbiol. Infect. 2016, 22 (Suppl 1), S15–S25. [Google Scholar]
- Flores-Velázquez, V.J.; Rocío, P. Pseudomonas Aeruginosa: Mechanisms of Resistance to Antibiotics and Case Analysis. GSC Biol. Pharm. Sci. 2021, 14, 179–188. [Google Scholar] [CrossRef]
- Zavascki, A.P.; Bulitta, J.; Landersdorfer, C. Combination therapy for carbapenem-resistant Gram-negative bacteria. Expert Rev. Anti-Infective Ther. 2013, 11, 1333–1353. [Google Scholar] [CrossRef]
- Yadav, R.; Bulitta, J.B.; Nation, R.; Landersdorfer, C.B. Optimization of Synergistic Combination Regimens against Carbapenem- and Aminoglycoside-Resistant Clinical Pseudomonas aeruginosa Isolates via Mechanism-Based Pharmacokinetic/Pharmacodynamic Modeling. Antimicrob. Agents Chemother. 2017, 61, e01011-16. [Google Scholar] [CrossRef] [Green Version]
- Tooke, C.L.; Hinchliffe, P.; Bragginton, E.C.; Colenso, C.K.; Hirvonen, V.H.A.; Takebayashi, Y.; Spencer, J. Beta-Lactamases and Beta-Lactamase Inhibitors in the 21st Century. J. Mol. Biol. 2019, 431, 3472–3500. [Google Scholar] [CrossRef]
- Worthington, R.J.; Melander, C. Overcoming Resistance to Beta-Lactam Antibiotics. J. Org. Chem. 2013, 78, 4207–4213. [Google Scholar] [CrossRef] [Green Version]
- Kresken, M.; Körber-Irrgang, B.; Läuffer, J.; Decker-Burgard, S.; Davies, T. In vitro activities of ceftobiprole combined with amikacin or levofloxacin against Pseudomonas aeruginosa: Evidence of a synergistic effect using time–kill methodology. Int. J. Antimicrob. Agents 2011, 38, 70–75. [Google Scholar] [CrossRef]
- Ramirez, M.S.; Tolmasky, M.E. Aminoglycoside Modifying Enzymes. Drug Resist. Updates 2010, 13, 151–171. [Google Scholar] [CrossRef] [Green Version]
- Coyne, S.; Courvalin, P.; Perichon, B. Efflux-Mediated Antibiotic Resistance in Acinetobacter Spp. Antimicrob. Agents Chemother. 2011, 55, 947–953. [Google Scholar] [CrossRef] [Green Version]
- Obara, M.; Nakae, T. Mechanisms of Resistance to Beta-Lactam Antibiotics in Acinetobacter Calcoaceticus. J. Antimicrob. Chemother. 1991, 28, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Lister, P.D.; Wolter, D.J.; Hanson, N.D. Antibacterial-Resistant Pseudomonas aeruginosa: Clinical Impact and Complex Regulation of Chromosomally Encoded Resistance Mechanisms. Clin. Microbiol. Rev. 2009, 22, 582–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wareham, D.W.; Momin, M.H.F.A.; Phee, L.M.; Hornsey, M.; Standing, J.F. Cefepime/sulbactam as an enhanced antimicrobial combination therapy for the treatment of MDR Gram-negative infections. J. Antimicrob. Chemother. 2019, 75, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, D.P.; Debata, N.K.; Singh, S.K. Extensively drug-resistant and pandrug-resistant Gram-negative bacteria in a tertiary-care hospital in Eastern India: A 4-year retrospective study. J. Glob. Antimicrob. Resist. 2018, 15, 246–249. [Google Scholar] [CrossRef]
- Sharahi, J.Y.; Ahovan, Z.; Maleki, D.T.; Rad, Z.R.; Rad, Z.R.; Goudarzi, M.; Shariati, A.; Bostanghadiri, N.; Abbasi, E.; Hashemi, A. In vitro antibacterial activity of curcumin-meropenem combination against extensively drug-resistant (XDR) bacteria isolated from burn wound infections. Avicenna J. Phytomed. 2019, 10, 3–10. [Google Scholar]
- Costello, S.E.; Deshpande, L.M.; Davis, A.P.; Mendes, R.E.; Castanheira, M. Aminoglycoside-modifying enzyme and 16S ribosomal RNA methyltransferase genes among a global collection of Gram-negative isolates. J. Glob. Antimicrob. Resist. 2019, 16, 278–285. [Google Scholar] [CrossRef]
- Sandberg, A.; Hessler, J.H.R.; Skov, R.L.; Blom, J.; Frimodt-Møller, N. Intracellular Activity of Antibiotics against Staphylococcus aureus in a Mouse Peritonitis Model. Antimicrob. Agents Chemother. 2009, 53, 1874–1883. [Google Scholar] [CrossRef] [Green Version]
- Okanda, T.; Matsumoto, T. In vitro effect of an antimicrobial combination therapy without colistin and tigecycline for CPE and non-CPE. J. Infect. Chemother. 2020, 26, 322–330. [Google Scholar] [CrossRef]
- Uddin, B.M.M.; Ritu, S.; Zubair, A.R.; Surovi, E.S.; Shamsuzzaman, S.M. In Vitro and in Vivo Evaluation of Antibiotic Combination against Imipenem Resistant Acinetobacter Baumannii Strains Isolated from Bangladeshi Patients. Am. J. Infect. Dis. 2020, 8, 83–87. [Google Scholar]
- Poole, K.; Gilmour, C.; Farha, M.A.; Parkins, M.D.; Klinoski, R.; Brown, E.D. Meropenem Potentiation of Aminoglycoside Activity against Pseudomonas Aeruginosa: Involvement of the Mexxy-Oprm Multidrug Efflux System. J. Antimicrob. Chemother. 2018, 73, 1247–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, T.A.; Shang, W.; Bush, K.; Flamm, R.K. Affinity of Doripenem and Comparators to Penicillin-Binding Proteins in Escherichia coli and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2008, 52, 1510–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadurugamuwa, J.L.; Lam, J.S.; Beveridge, T.J. Interaction of gentamicin with the A band and B band lipopolysaccharides of Pseudomonas aeruginosa and its possible lethal effect. Antimicrob. Agents Chemother. 1993, 37, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, B.D. Mechanism of bactericidal action of aminoglycosides. Microbiol. Rev. 1987, 51, 341–350. [Google Scholar] [CrossRef]
- Yadav, R.; Bulitta, J.B.; Schneider, E.K.; Shin, B.S.; Velkov, T.; Nation, R.L.; Landersdorfer, C.B. Aminoglycoside Concentrations Required for Synergy with Carbapenems against Pseudomonas aeruginosa Determined via Mechanistic Studies and Modeling. Antimicrob. Agents Chemother. 2017, 61, e00722-17. [Google Scholar] [CrossRef] [Green Version]
- Hayami, H.; Goto, T.; Kawahara, M.; Ohi, Y. Activities of β-lactams, fluoroquinolones, amikacin and fosfomycin alone and in combination against Pseudomonas aeruginosa isolated from complicated urinary tract infections. J. Infect. Chemother. 1999, 5, 130–138. [Google Scholar] [CrossRef]
- Farhan, S.M.; Ibrahim, R.A.; Mahran, K.M.; Hetta, H.F.; El-Baky, R.M.A. Antimicrobial resistance pattern and molecular genetic distribution of metallo-β-lactamases producing Pseudomonas aeruginosa isolated from hospitals in Minia, Egypt. Infect. Drug Resist. 2019, 12, 2125–2133. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Tech. Bull. Regist. Med. Technol. 1966, 36, 49–52. [Google Scholar] [CrossRef]
- Weinstein, M.P.; Limbago, B.; Patel, J.; Mathers, A.; Campeau, S.; Mazzulli, T.; Eliopoulos, G.M.; Patel, R.; Galas, M.F.; Richter, S.S. M100 Performance Standards for Antimicrobial Susceptibility Testing; Clinical & Laboratory Standards Institute: Annapolis Junction, MD, USA, 2018. [Google Scholar]
- Wilson, K. Preparation of Genomic DNA from Bacteria. Curr. Protoc. Mol. Biol. 2001, 56, 241–245. [Google Scholar] [CrossRef]
- Xia, Y.; Liang, Z.; Su, X.; Xiong, Y. Characterization of Carbapenemase Genes inEnterobacteriaceaeSpecies Exhibiting Decreased Susceptibility to Carbapenems in a University Hospital in Chongqing, China. Ann. Lab. Med. 2012, 32, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.C.; Ji-Hyun, J.; Hyogyeong, K.; Young-Jin, K.; Kyoung-Ryul, L.; Yun-Tae, K. Multiplex Pcr for Simultaneous Detection of Aminoglycoside Resistance Genes in Escherichia Coli and Klebsiella Pneumoniae. Korean J. Clin. Lab. Sci. 2012, 44, 155–165. [Google Scholar]
- Spilker, T.; Coenye, T.; Vandamme, P.; LiPuma, J.J. PCR-Based Assay for Differentiation of Pseudomonas aeruginosa from Other Pseudomonas Species Recovered from Cystic Fibrosis Patients. J. Clin. Microbiol. 2004, 42, 2074–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathe, A.; Szabo, D.; Anderlik, P.; Rozgonyi, F.; Nagy, K. The Effect of Amikacin and Imipenem Alone and in Combination against an Extended-Spectrum Beta-Lactamase-Producing Klebsiella Pneumoniae Strain. Diagn. Microbiol. Infect. Dis. 2007, 58, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Hernández, M.-J.; Pachón, J.; Pichardo, C.; Cuberos, L.; Ibáñez-Martínez, J.; García-Curiel, A.; Caballero-Granado, F.J.; Moreno, I.; Jiménez-Mejías, M.E. Imipenem, doxycycline and amikacin in monotherapy and in combination in Acinetobacter baumannii experimental pneumonia. J. Antimicrob. Chemother. 2000, 45, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.-J.; Lai, C.-C.; Chen, C.-C.; Zhang, C.-C.; Weng, T.-C.; Chiu, Y.-H.; Toh, H.-S.; Chiang, S.-R.; Yu, W.-L.; Ko, W.-C.; et al. Colistin-sparing regimens against Klebsiella pneumoniae carbapenemase-producing K. pneumoniae isolates: Combination of tigecycline or doxycycline and gentamicin or amikacin. J. Microbiol. Immunol. Infect. 2019, 52, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Al-jumaily, A.K.T.; Turkie, A.M. Molecular Investigation of Gene Expression of Beta-Lactamases Enzymes Gen for Pseudomonas Aeruginosa Bacter. Iraqi J. Agric. Sci. 2018, 49, 803. [Google Scholar]
- Yuan, J.S.; Reed, A.; Chen, F.; Stewartjr, C.N. Statistical analysis of real-time PCR data. BMC Bioinform. 2006, 7, 85. [Google Scholar] [CrossRef] [Green Version]
- Soboh, F.; Khoury, A.E.; Zamboni, A.C.; Davidson, D.; Mittelman, M.W. Effects of ciprofloxacin and protamine sulfate combinations against catheter-associated Pseudomonas aeruginosa biofilms. Antimicrob. Agents Chemother. 1995, 39, 1281–1286. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source of Infections | Total Number of Isolates | E. coli | P. aeruginosa | Proteus spp. | Klebsiella spp. | A. baumannii |
|---|---|---|---|---|---|---|
| Wounds | 78 | 29 | 17 | 24 | 5 | 3 |
| Ear infections | 10 | 3 | 6 | 1 | - | - |
| Burns | 15 | 5 | 5 | 5 | - | - |
| Chest infections | 22 | 7 | 8 | - | 5 | 2 |
| Urinary tract infections | 13 | 8 | 5 | - | - | - |
| Gastroenteritis | 12 | 8 | 4 | - | - | - |
| Total (%) * | 150 (100) | 60 (40) | 45 (30) | 30 (20) | 10 (6.67) | 5 (3.33) |
| No. | MIC(µg/mL) | MIC90 | MIC50 | R | % * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | 128 | 256 | 512 | 1024 | 256 | 8 | |||
| 45 | 0 | 0 | 6 | 6 | 6 | 7 | 4 | 3 | 3 | 3 | 3 | 2 | 2 | 13 | 28.9 | ||
| No. | MIC(µg/mL) | MIC90 | MIC50 | R | % * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | 128 | 256 | 512 | 1024 | 256 | 2 | |||
| 45 | 0 | 0 | 20 | 12 | 0 | 0 | 0 | 0 | 5 | 2 | 2 | 2 | 2 | 13 | 28.9 | ||
| P. aeruginosa | MIC (µg/mL) | FICindex | Outcome | |||
|---|---|---|---|---|---|---|
| Amikacin | Imipenem | Amikacin + Imipenem | ||||
| Wound isolate no. 5 | 1024 | 1024 | 32 | 32 | 0.33 | Synergistic |
| Ear isolate no. 3 | 1024 | 256 | 32 | 32 | 0.4 | Synergistic |
| Burn isolate no. 3 | 512 | 256 | 4 | 1 | 0.011 | Synergistic |
| Chest infection isolate no. 1 | 1024 | 256 | 32 | 8 | 0.062 | Synergistic |
| P. aeruginosa Isolate No. | 16S rDNA | bla IMP | aac(6′)-Ib | ||
|---|---|---|---|---|---|
| CT | CT | Fold Change | CT | Fold Change | |
| P Control | 20.51 | 21.94 | - | 23.62 | - |
| P1 | 21.70 | 20.10 | 8.1681 | 21.84 | 7.8354 |
| P2 | 20.45 | Nd | 19.79 | 13.6422 | |
| P3 | 21.08 | 19.15 | 10.2674 | Nd | |
| P4 | 21.13 | 20.37 | 4.5631 | 21.83 | 5.3147 |
| P5 | 20.78 | 19.76 | 5.4642 | 21.90 | 3.9724 |
| Time | Untreated (I) | Imipenem (II) | Amikacin (III) | Combination (IV) | p Value |
|---|---|---|---|---|---|
| 3 h | 10.04 ± 0.03 | 9.98 ± 0.02 | 9.91 ± 0.03 | 9.11 ± 0.02 | <0.001 * |
| 11 h | 10.43 ± 0.01 | 9.71 ± 0.05 | 9.05 ± 0.03 | 8.13 ± 0.03 | <0.001 * |
| 27 h | 10.93 ± 0.04 | 9.03 ± 0.03 | 8.96 ± 0.03 | 5.50 ± 0.52 | <0.001 * |
| Gene | Primer Sequence (5’-3’) | Annealing Temperature (° C) | Product Size (bp) | Reference |
|---|---|---|---|---|
| bla IMP | F:CATGGTTTGGTGGTTCTTGT | 59 | 488 | [33] |
| R:ATAATTTGGCGGACTTTGGC | ||||
| aac(6′)-Ib | F:AGTACTTGCCAAGCGTTTTAGCGC | 51 | 365 | [34] |
| R:CATGTACACGGCTGGACCAT | ||||
| 16S rDNA | F:GACGGGTGAGTAATGCCTA | 55 | 618 | [35] |
| R: CACTGGTGTTCCTTCCTATA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farhan, S.M.; Raafat, M.; Abourehab, M.A.S.; Abd El-Baky, R.M.; Abdalla, S.; EL-Gendy, A.O.; Azmy, A.F. Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa. Antibiotics 2021, 10, 1429. https://doi.org/10.3390/antibiotics10111429
Farhan SM, Raafat M, Abourehab MAS, Abd El-Baky RM, Abdalla S, EL-Gendy AO, Azmy AF. Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa. Antibiotics. 2021; 10(11):1429. https://doi.org/10.3390/antibiotics10111429
Chicago/Turabian StyleFarhan, Sara Mahmoud, Mohamed Raafat, Mohammed A. S. Abourehab, Rehab Mahmoud Abd El-Baky, Salah Abdalla, Ahmed Osama EL-Gendy, and Ahmed Farag Azmy. 2021. "Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa" Antibiotics 10, no. 11: 1429. https://doi.org/10.3390/antibiotics10111429
APA StyleFarhan, S. M., Raafat, M., Abourehab, M. A. S., Abd El-Baky, R. M., Abdalla, S., EL-Gendy, A. O., & Azmy, A. F. (2021). Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa. Antibiotics, 10(11), 1429. https://doi.org/10.3390/antibiotics10111429