1. Introduction
Resistance to antimicrobial medicines and the resultant loss of their effectiveness and treatment failure has become a frightening global health problem [
1]. Resistant infections lead to substantial economic burden, morbidity and mortality [
2,
3]. Resistant infections were responsible for 25,000 deaths per year with a cost of EUR 1.5 billion to the health system in Europe [
3]. When resistance to first-line antimicrobial drugs occurs, more expensive therapies may be used, and longer duration of treatment and hospitalized care are usually required [
2]. Globally, there is significant resistance to both old and new anti-microbial drugs, including third generation cephalosporins, carbepenems and fluoroquinolones [
4,
5], yielding a phenomenon of hard-to-treat infections.
In sub-Saharan Africa, paucity of evidence on antimicrobial resistance (AMR) reflects an underestimated magnitude of the problem, but in countries where data is available, substantial AMR has been found with a rate of 100 percent among some bacteria [
6,
7]. Resistance to third generation cephalosporins, fluoroquinolones, penicillins, chloramphenicol, nalidixic acid and co-trimoxazole in sub-Saharan Africa [
8,
9,
10,
11] has created a challenge for the treatment of infections.
Several factors contribute to antimicrobial resistance. These include inappropriate antimicrobial use and lack of surveillance systems contributing significantly to the spread of antimicrobial resistance. Poor infection prevention and control in healthcare facilities, lack of available, affordable and rapid diagnostic tests, and low-quality medicines are other factors that influence antimicrobial resistance [
2,
12]. Disparities in proper use of antibiotics, infection treatment and hygiene practices, infectious disease burden and availability of first- and second-line drugs contribute to geographical differences in AMR [
12,
13].
Antimicrobial consumption contributes to AMR, and the volume of antimicrobial consumption influences resistance. Global antibiotic consumption has grown in recent years with low- and middle-income countries having the highest increase [
14]. Between 2000 and 2010 antibiotic, use rose by 30%, and the rise in consumption for the treatment of infections such as pneumonia is expected to continue. Heavy antibiotic use by hospitals generates some of the most dangerous and difficult-to-treat infections [
15]. Globally, one-third of hospitalized patients receive at least one antimicrobial prescription, and about 90% of antimicrobials prescribed are systemic antibiotics [
16]. Penicillins with β-lactamase inhibitors, third-generation cephalosporins and fluoroquinolones are the most frequently prescribed antibiotics for hospitalised patients [
16]. Only one-fifth of antimicrobial medicines prescribed for hospitalized patients target a specific micro-organism [
16]. Recent data show that a significant proportion of prescriptions do not specify duration of treatment and reason for use [
16]. However, significant variations exist in antimicrobial use between regions across the globe. Africa is the region with the highest antimicrobial use, predominantly for community acquired infections. Antimicrobial medicines are prescribed for half of hospitalized patients in Africa, and in some countries, antimicrobial use is as high as 75 percent [
16]. Further, Africa has the highest use of antimicrobial drugs without reason and the lowest targeted use for resistant organisms [
16]. Ghana, similar to many sub-Saharan African countries, has limited evidence on antimicrobial drug use in hospitalized patients.
In Ghana, AMR is prevalent, with rates exceeding 75 percent by some organisms [
17]. Methicillin resistant staphylococcus aureus (MRSA), streptococci, salmonella, and
E. coli have demonstrated high resistance to antibiotics in Ghana [
17]. Low susceptibility of bacteria to antibiotics such as tetracycline, co-trimoxazole, nalidixic acid and some penicillins, and emerging resistance to quinolones, cephalosporins, gentamycin and carbapenems in Ghana [
17,
18] is threatening morbidity and mortality outcomes of infectious diseases.
To provide feedback on antimicrobial use and associated resistance and to assess the effect of interventions and improve antimicrobial decision making, surveillance systems must be implemented as part of antimicrobial stewardship programmes [
19,
20,
21]. Surveillance as part of stewardship programmes improves stewardship interventions such as promoting guideline adherence in empirical treatment [
22,
23]. Collecting hospital antimicrobial data and implementing informed interventions for optimal antibiotic use in hospitals has significant potential to reduce antimicrobial resistance at local, national, regional and global levels.
Antibiotic use data collection methods in hospitals allow standardization and comparison of antimicrobial use between hospitals, districts, countries, and regions. A typical example is the antimicrobial point prevalence survey (PPS). The PPS enables data collection with minimized workload and resource requirements at a specific time point, and it is already in use in hospitals [
24]. The Global Point Prevalence Survey (Global-PPS) of antimicrobial drug use and resistance is suited for resource-limited (low- and middle-income) countries and allows comparison of data with high-income countries.
Similar to many sub-Saharan African countries, limited evidence on antimicrobial use with standardized surveillance methods in Ghanaian hospitals stifles the provision of timely and efficient feedback to the health system, and adversely affects the development of evidence-based local antimicrobial stewardship programmes and other interventions aimed at reducing antimicrobial resistance. This study, which is the first comprehensive antimicrobial survey at the Korle Bu Teaching Hospital (KBTH), used the PPS method and was a partnership between Korle-Bu Teaching Hospital from Ghana and the North Middlesex University Hospital (NMUH) from the UK. It was part of the 2019 Global Point Prevalence Survey (Global-PPS) on antimicrobials.
3. Discussion
This was a comprehensive antimicrobial PPS that involved all clinical departments, wards and units of the KBTH. Data collection was carried out over a 3-day period, and all patients’ folders were assessed. Data were collected on those patients on at least one antimicrobial agent during the survey period.
3.1. Antimicrobial Prevalence
This survey identified an overall prevalence of antimicrobial prescriptions among inpatients at the Korle Bu Teaching Hospital to be 53.3%. Among the inpatients surveyed, 83.5% of them received systemic antimicrobials and 65% received more than one antimicrobial. The prevalence rate in this study is comparable to previous studies performed in KBTH among inpatients which found prevalence rates of 51.4% in 2006 [
25] and 53% in 2000 [
26]. This shows that rates of antibiotic use among inpatients in KBTH have been fairly consistent over the past two decades. Studies from other hospitals in Ghana showed comparatively higher prevalence rates with Komfo Anokye Teaching Hospital reporting a prevalence of 64% [
27]; Ho Teaching Hospital recorded 66.7% [
28], and Keta Municipal Hospital recorded 82.0% [
29]. Prevalence from this study compared favourably with antimicrobial prevalence in Africa (63%) but is still relatively high compared to North America (34.0%), South Europe (31.7%) or East Europe (30.3%) [
16]. Higher rates of antimicrobial use are typically linked with the development of antimicrobial resistance and healthcare-associated infections [
30] and thus must be suitably justified.
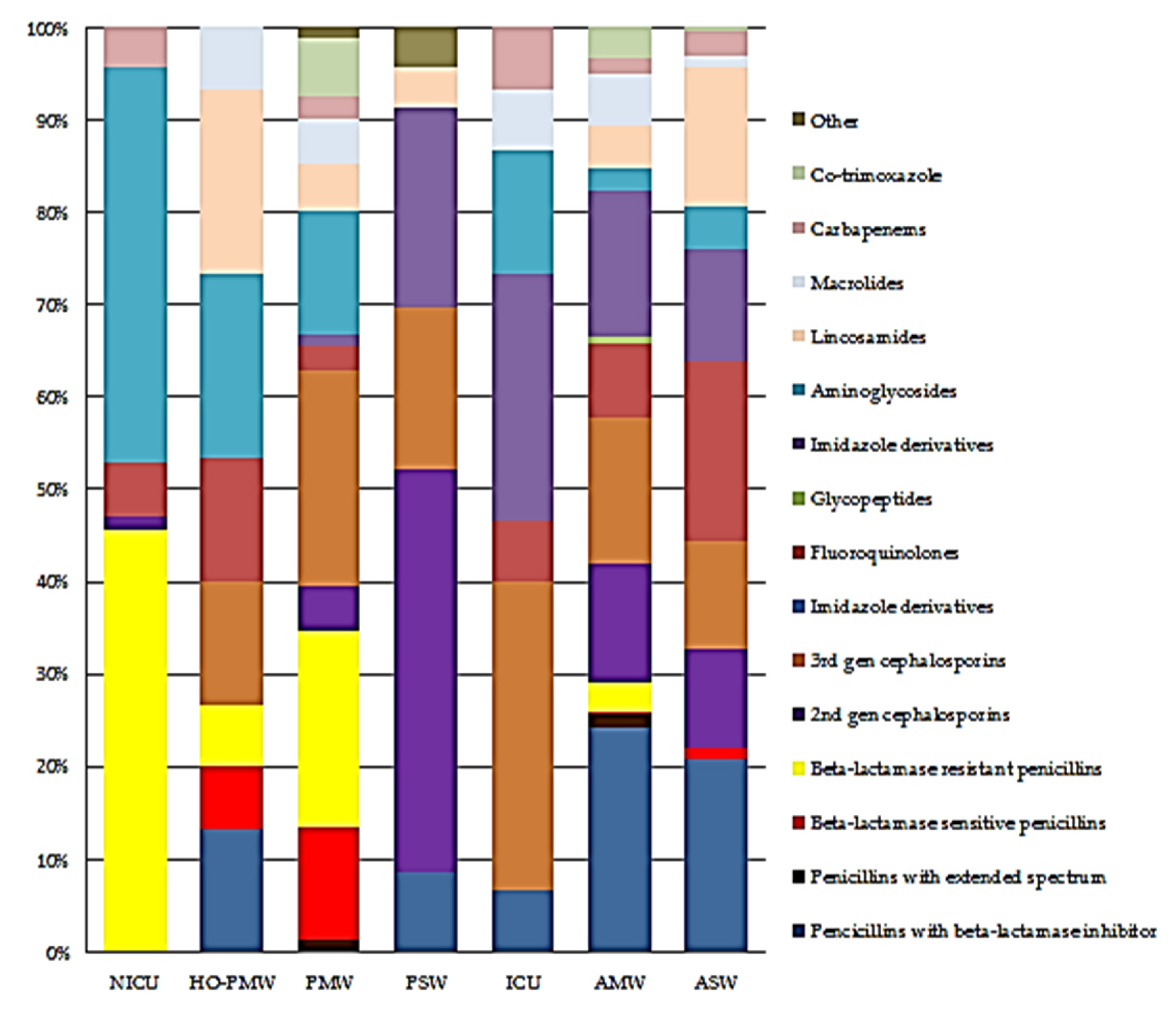
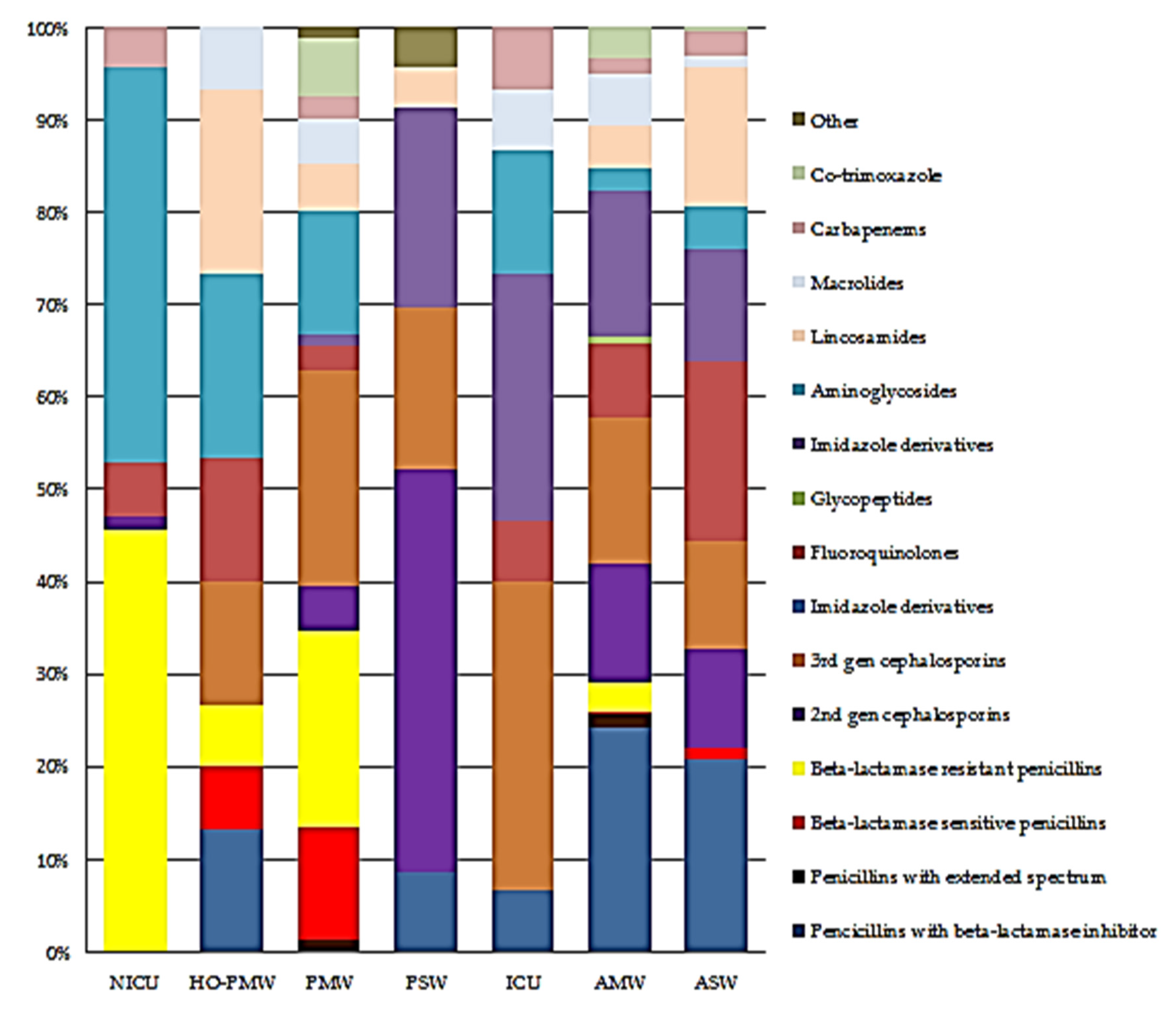
3.2. Most Common Antimicrobials Prescribed
The top four antibiotics prescribed, metronidazole, amoxicillin/clavulanic acid, ceftriaxone and cefuroxime, reinforce the work of Labi et al. [
25] which reported the same antibiotics as the four most used antibiotics at the Korle Bu Teaching Hospital. Beta-lactam antibiotics (cephalosporins and penicillins) were the most frequently used classes. Fluoroquinolones were more frequently prescribed than macrolides and aminoglycosides. The antibiotic use pattern found in this study is largely consistent with those of recently published point prevalence survey of antibiotics [
16,
31,
32,
33] These results suggest that beta lactam antibiotics remain drugs of choice in the management of infections. The usefulness of this group of antibiotics in the future is however threatened, as data show that increased antibiotic use is associated with antimicrobial resistance [
34,
35,
36,
37,
38,
39].
3.3. Most Common Diagnosis for Antimicrobial Use
The top three morbidities requiring antimicrobial therapy in the hospital were pneumonia, skin and soft tissue infections and sepsis with upper respiratory tract infections and malaria as the fourth and fifth topmost respectively. The results are similar to a study carried out in a referral hospital in Kenya in which the respiratory system had the largest proportion of antibiotics prescribed followed by skin, soft tissue, bone and joint (SSTBJ) infections [
32]. It is also quite similar to a survey carried out in 18 hospitals in Egypt, in which amongst patients receiving antibiotics for treatment of infection, the most common anatomical sites of suspected or proven infection were the respiratory tract, gastrointestinal tract, and skin, bone and joints [
40].
Further, in a survey involving paediatric patients from 26 Canadian hospitals, the most commonly treated infections were sepsis (16%) and lower respiratory tract infection (12.1%) [
41]. The consistency in these results may justify the prescribing of these medicines; however, care should be taken to avoid over prescribing.
3.4. Targeted versus Empiric Treatment
Most treatments were empirical for both healthcare- and community-acquired infections. This finding is consistent with recent data from Africa [
42] and other developing countries [
43,
44]. Empirical treatment for community-acquired infections had a higher proportion compared to empirical treatment for healthcare-acquired infections. Versporten et al. published similar findings [
16]. Empirical treatment of infections can be attributed to limited laboratory resources to aid in the identification of specific pathogens and the antimicrobials they are most susceptible to. This results in the use of broad-spectrum empiric treatment in a bid to cover all possible pathogens that could be responsible for the infection. In a randomized comparative prospective study of complications in transrectal prostate biopsy [
44] post-prophylactic treatment, it was found that infection rates were significantly lower in targeted treatment compared to empirical treatment. Further, the supremacy of targeted treatment over empirical treatment was manifested in a meta-analysis [
45]. The increased empirical treatment of infections in the hospital may contribute to the burden of a microorganism. While it has been reported that tertiary hospitals in Ghana perform better in targeted treatment of infections compared to non-tertiary (secondary) settings [
29], results from this study implies that targeted treatment needs more improvement. The hospital’s Drugs and Therapeutics Committee may lead the way in this regard.
3.5. Quality Indicators for Prescribing
In this era of increasing AMR, policies that seek to promote prudent antimicrobial prescribing have been developed and adopted by countries and hospitals [
46]. An evidence-based antimicrobial guideline is preferably the mainstay of such policies [
47]. Adherence to such hospital guidelines is however often low to moderate [
48,
49]. Korle bu Teaching hospital had some positive practices regarding antimicrobial stewardship among the indicators evaluated, but this varied widely by ward type. Guideline compliance was greater than 80% among all the wards surveyed, and this was quite laudable. However, when it came to documenting the reasons for antimicrobial prescriptions, the medical wards fared much better than the surgical or ICU (76.1% vs. 44.3% vs. 41.2% respectively). Possible reasons for these results could be the focus of future studies.
Another important indicator for prudent antimicrobial prescribing is the presence of a stop or review date. Here, the ICU fell short compared to the surgical and medical wards (11.8% vs. 49.9% vs. 38.5%, respectively). A possible reason for this could be the daily review of patients on the ICU wards, hence prescribers not appreciating the need to indicate the stop or review date. An intervention targeting ICU prescribers to include this parameter in their notes will be important for KBTH to improve antimicrobial stewardship.
Considering biomarkers, patients pay per laboratory tests that are not reimbursed; hence, c-reactive protein (CRP) and procalcitonin are often viewed as non-essential expensive extras.
Point prevalence surveys are among the most reliable tools in the assessment of antibiotic utilization at the patient level [
50]. They are also valuable in providing information on antimicrobial resistance. Access to antimicrobial utilization and resistance patterns are pivotal for the success of any antimicrobial stewardship (AMS) programme. In a systematic review and meta-analysis, a significant association was reported between an AMS programme and a decrease in the incidence of antibiotic infections among hospitalized patients [
51]. This calls for regular PPS at all health institutions with the aim of identifying the gaps and fixing them to improve public health.
3.6. Limitations
Data collection in this study was performed over three days only. The seasonal nature of some diseases (asthma, flu, etc.) that require the use of antimicrobial agents may change the prevalence of figures depending on the time the study is performed. This calls for continuous PPS at different times in the year before the actual antimicrobial prevalence in the hospital can be determined. For Ghana, there are only two clear seasons (rainy season and dry season), and the effect may not be as significant compared to countries with four seasons. It is possible that reported figures for microbiological reports may be less than actual because these may have been absent during the survey period, most probably due to the time it takes for such reports to be ready. We did not report on the number of various laboratory tests (blood culture, stools for C. difficile, etc.) performed per year, to avoid under ascertainment. This is because some of the requested tests were performed in private labs outside the hospital.


 ,
, 


{kind=link}
{kind=link}