Abstract
Macrolide and fluoroquinolone resistance (MLr/FQr) in Mycoplasma genitalium (MG) infections is concerning worldwide. Current guidelines recommend performing MLr detection in MG-positive cases to adjust antimicrobial therapy. We aimed to evaluate the usefulness of PCR followed by pyrosequencing for MLr detection in comparison with a one-step commercial assay and to assess the prevalence of MLr and FQr in Badalona, Spain. A total of 415 MG-positive samples by Allplex STI-7 (Seegene) were analyzed for MLr detection by pyrosequencing. From those, 179 samples were further analyzed for MG and MLr by ResistancePlus® MG kit (SpeeDx) and 100 of them also for fluoroquinolone resistance (FQr) by sequencing the parC gene. Regarding MG detection, Allplex and Resistance Plus® showed an overall agreement of 87%, but this value rose to 95.4% if we compare them for MLr detection. Prevalence of MLr was 23.1% in Badalona, but this rate increased to 73.7% in the HIV-positive patients cohort. FQr detection showed 3% of resistant strains. Pyrosequencing is a convenient and cheap technique for MLr detection, but one-step tools should be considered in high-throughput laboratories. Despite the fact that MLr remained moderate and FQr was low in our study, simultaneous MG and MLr detection would improve patient’s management applying resistance-guided treatment strategies.
1. Introduction
Mycoplasma genitalium (MG) is an important sexually transmitted pathogen responsible for 15–20% of nongonococcal urethritis (NGU) in men [1] and cervicitis, pelvic inflammatory disease, preterm birth, and abortion in women [2]. MG is a fastidious microorganism that is difficult to grow from clinical samples and cellular culture is generally limited to reference laboratories [3]. For this reason, molecular detection is the most widely used method for routine diagnosis of MG infection.
MG lacks a cell wall, being intrinsically resistant to beta-lactam antibiotics. Macrolides (ML) have been extensively used worldwide as a first-line treatment, with quinolones as second-line therapy. However, given the high capacity of this microorganism for acquiring antibiotic resistance to both groups, MG becoming an untreatable sexually transmitted infection (STI) is a plausible and close scenario. European guidelines recommend an extended ML regimen to avoid macrolide resistance (MLr) acquisition in susceptible strains [4]. The fourth-generation fluoroquinolone moxifloxacin is recommended as a second option if the strain is resistant to macrolides [4]. Furthermore, treatment failures with both therapies have already been reported—given by dual-resistant strains [5,6]. Alternatively, doxycycline has also been used but with poor efficacy [7]. For this reason, pristinamycin has been established as the primary third-line treatment for patients with ML or fluoroquinolone treatment failure [4].
Therefore, according to current guidelines in STI, MG detection in symptomatic patients and subsequent MLr studies on positive cases should be performed to adjust antimicrobial therapy when ML resistance patterns are detected [4].
Macrolide resistance is caused by point mutations in region V of the 23S rRNA gene at positions 2058, 2059 or 2062 (E. coli numbering). These mutations can be detected by in-house techniques using a two-step approach performing MG detection first and analyzing afterwards MLr presence in MG-positive cases [8,9]. Recently available commercial kits can also be used [10], with many of them able to detect MG and MLr patterns in a single step. Similarly, fluoroquinolone resistance (FQr) is mainly caused by mutations in genes parC or gyrA [11] and detecting these patterns when MLr is detected or especially after moxifloxacin treatment failure could be an interesting option to reserve third-line antimicrobials for selected patients. Quinolone resistance-determining regions (QRDR) can be studied by Sanger sequencing [12] or by new commercial assays authorized only for research purposes [13,14].
Limited data are available regarding MG macrolide and fluoroquinolone resistance in Spain [15,16,17,18]. The aim of this study was to evaluate pyrosequencing as an adequate in-house technique for detecting MG MLr in our two-step routine, by comparing it to a commercial one-step assay and to assess the prevalence of macrolide and fluoroquinolone resistance in Badalona, Spain.
2. Results
2.1. Demographic Data and Clinical Findings
A total of 415 MG-positive specimens detected by Allplex STI-7 assay (Seegene Inc., Seoul, Korea) from 407 individuals were collected between 2016 and 2018 from people who required STI diagnosis, being females in 75.9% of cases (n = 309) and males in 24.1% (n = 98). The mean age of the studied population was 26.2 years (ranging from 16 to 68).
The highest number of positive results was detected in patients up to 25 years-old (n = 199, 47.95%), followed by patients from 26 to 40 years-old (n = 158, 38.07%) and older than 40 years (n = 58, 13.98%). More details about the samples analyzed and their origins can be found in Table 1.

Table 1.
Samples and origin.
Information regarding clinical findings was registered by clinicians during the prospective part of study. Epidemiological information, medical records about symptomatology, or reason for seeking a STI test was obtained for 136 out of 181 patients included, showing that the most common cause was a previous intercourse with a STI-positive patient, followed by urethritis and leukorrhea, as shown in Figure 1. More detailed information about epidemiological data and clinical findings is presented in Table 2.
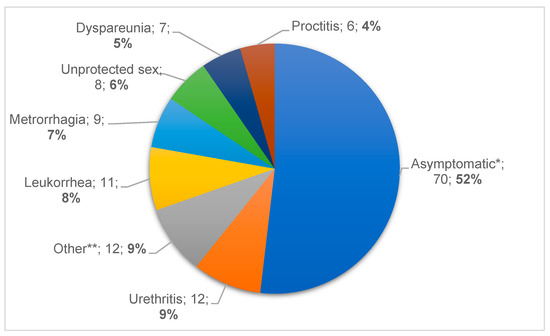
Figure 1.
Symptoms and signs of patients included during the prospective phase of the study (Symptom, n, %). * Asymptomatic section includes STI contacts and patients with previous unprotected sex. ** Other: dysuria (n = 4), pruritus (n = 4), infertility (n = 2), test of cure (n = 1), amenorrhea (n = 1).
Table 2.
Epidemiological data and clinical findings of MG infections of 136 patients included in the prospective phase of the study.
Focusing on risk factors for a MG infection, our cohort included 38 known HIV-positive males, including 94.7% (n = 36) men who have sex with men (MSM). Most of them were asymptomatic (63.2%, n = 24) and, among those with symptoms, proctitis (15.8%, n = 6), urethritis (13.2%, n = 5), or dysuria (7.9%, n = 3) were the most prevalent. Remarkably, in the HIV-positive group, MG was the only pathogen detected in almost half of the cases (n = 17, 44.7%).
Coinfections with other STI agents were detected, such as Chlamydia trachomatis (n = 1, 2.6%), Neisseria gonorrhoeae (n = 3, 7.9%), and Treponema pallidum (n = 6, 15.8%, one case jointly with N. gonorrhoeae). Other microorganisms such as Ureaplasma spp. or M. hominis were found in 31.6% of patients but were not considered because of their uncertain pathogenic role.
2.2. Detection of Macrolide and Fluoroquinolone Resistance
Among the 415 MG-positive samples detected by Allplex STI-7, 21 contained insufficient DNA to perform the resistance study, leaving a total of 394 specimens. Macrolide resistance analysis was performed by two different methods: pyrosequencing, ResistancePlus® MG kit, or by both methods. A subset of 100 samples was analyzed by both methods, whereas additional 215 samples were processed by pyrosequencing only and 79 more by ResistancePlus® MG kit only. The prevalence of macrolide resistance was 23.1%, with a total of 91 samples harboring macrolide resistance-associated mutations. More details are shown in Figure 2.
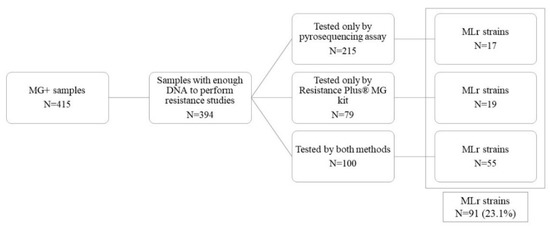
Figure 2.
MLr strains detected during the study period.
Macrolide resistance prevalence was also calculated in both study periods, observing a slight increase in 2018 (26%) in relation with the previous phase (22.2%).
Interestingly, when focusing on the HIV cohort only, the prevalence of macrolide resistance was 73.7% (28/38), with the clinical records showing a previous antibiotic regimen in 19.8% of cases, predominantly macrolides.
A total of 72 specimens had a mutation conferring MLr detected by pyrosequencing and this method revealed four different types of mutation. The most prevalent mutation was A2058G (n = 41, 56.9%), followed by A2059G (n = 27, 37.5%), A2058T (n = 3, 4.2%), and A2062T (n = 1, 1.4%).
The subset of 100 samples with MLr detected by pyrosequencing was further analyzed for MLr by the ResistancePlus® MG kit and for fluoroquinolone resistance detection. As the ResistancePlus® MG assay offers MG detection data, a comparison between that assay and the Allplex STI-7 assay could be performed, with an overall agreement regarding MG detection of 87% between both techniques. When MLr detection was compared, the agreement between the ResistancePlus® MG kit and pyrosequencing was 95.4%.
Regarding fluoroquinolone resistance (FQr), 97 out of the 100 samples showed a wild-type parC gene, whereas three of them had the mutation Ser83(80)Ile. Remarkably, these three strains were also macrolide resistant, corresponding in two cases to men with urethritis and one 18-year-old woman for whom the first sample (collected after an empiric 5 day-course ML treatment) showed an A2059G mutation/parC wild-type strain. The woman was subsequently treated with moxifloxacin and the test of cure showed a double resistance pattern (A2059G/Ser83(80)Ile) after fluoroquinolone therapy.
3. Discussion
Mycoplasma genitalium is a pathogen associated with NGU, balanoposthitis, and chronic prostatitis in men, as well as cervicitis and PID among other consequences in women [1]. Treatment failures are especially concerning due to MG’s capacity of acquiring mutations that confer macrolide or fluoroquinolone resistance. Since 1983, when MG was described as a new species in the urogenital tract [19], multiple reports focusing on antibiotic resistance have been published in Europe [20] and worldwide [21]. Unfortunately, there are limited data of MG infections and resistance patterns in Spain [15,16,17,18].
Most of the MG-positive results came from people below 25 years-old in our study, related to the epidemiological surveillance system to monitor C. trachomatis (CT) performed in Catalonia since 2007. This fact implies that the higher burden of samples received in the microbiology departments for STI testing belong to this population group. Among the HIV cohort, rectal positivity was higher in asymptomatic patients, as previously described by Read et al. [22].
In our setting, multiplex PCR detecting seven STIs and urogenital bacteria (C. trachomatis, N. gonorrhoeae, M. genitalium, T. vaginalis, M. hominis, U. urealyticum, and U. parvum) is currently employed [23]. However, according to most international guidelines [4,24], MG testing is only recommended based on presence of symptoms or in current sexual partners of persons infected with MG in order to avoid unnecessary treatments leading to antibiotic resistance [25,26]. In our case, if MG is detected, clinical records are checked to look for symptoms. If there is no history of any patient’s symptomatology or if the patient is not a sexual partner of a positive case, MG positivity is not displayed. In the same way, commensal bacteria such as Ureaplasma spp. or M. hominis can be detected with the multiplex PCR simultaneously to “true” STI agents. Given their uncertain pathogenic role and controversial treatment benefits [27], these bacteria are only reported in exceptional cases to avoid antimicrobial resistance development.
A comparison between the Allplex STI-7 and the ResistancePlus® MG kit for the detection of MG was performed in a subset of 100 samples, with an overall agreement of 87% (87/100). For 13 discordant cases, ResistancePlus® MG kit did not detect MG while Allplex gave a positive detection, with a subsequent successful 23S rRNA gene pyrosequencing. Therefore, the MG-negative results by the ResistancePlus® MG kit could be explained by low bacterial load plus potentially loss of DNA integrity due to an additional freeze–thaw cycle (specimens were first tested by the Allplex STI-7 assay and then frozen at −20 °C until tested by ResistancePlus® MG). The target used for MG detection by Allplex STI-7 is unknown, while the assay ResistancePlus® MG amplifies the MgPa gene. Thus, a higher sensitivity in the target used by Allplex could also be responsible for its superior performance.
Pyrosequencing was employed as our main technique to detect MLr, given our prior experience of MLr mutation detection in M. pneumoniae [28]. Samples from quality controls were used as references, demonstrating the robustness of the developed method. The commercial assay ResistancePlus® MG kit was also evaluated in a subset of 100 samples. This assay is very convenient for high-throughput laboratories and can be easily implemented in routine diagnosis, allowing MG detection and macrolide resistance determination as a one-step method without requiring specialized instrumentation and covering that need reflected in the current guidelines [4]. However, this assay is not suitable for epidemiological or research purposes on mutation types as it only detects a specific set of 23S rRNA variations associated with MLr but does not distinguish among them nor detects new ones, in contrast to pyrosequencing. Additionally, the lack of a 23S internal control for MLr targets implies that this kit does not discern between absence of mutation and absence of 23S rRNA gene amplification, leading to a risk of false susceptible results when the 23S rRNA gene is not amplified, as previously reported by Le Roy et al. [29]. When compared with pyrosequencing, the overall agreement was 95.4% (83/87). Among the four discordant results, one mutated strain by pyrosequencing was informed as negative by ResistancePlus® MG due to late detection (Ct > 30), which might correspond with low bacterial load. Unfortunately, due to insufficient material, those four specimens could not be tested again.
Overall, the macrolide resistance rate detected in our setting was 23.1%. Our rate is similar to other studies performed in different parts of our country [30,31,32]—slightly higher than the 16.3% detected in the Basque Country [17] but lower than the 36.4% reported by de Salazar et al. [33] in southern Spain. However, their cohort included 25% of MSM versus 9.1% in our cohort. Focusing on Catalonia, our prevalence of resistance is similar to the one reported by Muñoz-Santa et al. (23%) [34] and between the rates published by Lucena-Nemirosky et al. (12.6%) in a routine diagnostic service [18] and Fernández-Huerta et al. (36.1%) in a STI Unit [15].
Among the HIV cohort, given that 94.7% of them were MSM, the high rate of MLr (73.7%) is consistent with previous data reported by Barberá et al. in Spain [35], demonstrating that MSMs have a higher risk of acquisition of macrolide-resistant MG, and by Dionne-Odom et al.’s study, reporting a prevalence of multidrug resistant MG of 74.1% in HIV-MSM patients in Alabama [36]. The subsequent risk of treatment failure highlights the need to perform diagnosis and macrolide resistance detection simultaneously.
Fluoroquinolone resistance (FQr) detection performed in a subset of samples (n = 100) showed 3% of resistant strains that harbored Ser83Ile mutation in the parC gene. This rate is slightly lower than those described in our country by Fernández-Huerta et al. (8.8%), Piñeiro et al. (7.9%, but not all of them were clearly implicated in treatment failure), de Salazar et al. (9.1%), and Adelantado and Beristain (5.5%) [13,17,32,33]. However, our results are concordant with the lower FQr prevalence detected in WHO European regions, in comparison with Western Pacific territories [21].
This study has several limitations. Firstly, our study population comprehended both symptomatic and asymptomatic individuals. This fact could affect macrolide and fluoroquinolone resistance values, in comparison with other Spanish studies [15,33]. Secondly, it was not possible to test all samples for ML resistance with both methods simultaneously. The use of only 100 samples for the comparison of both methods is a limitation of the study but gives a good insight into the usefulness of the pyrosequencing assay. Thirdly, for fluoroquinolone resistance, only parC gene was sequenced for being the most frequently involved in moxifloxacin failure [11].
4. Materials and Methods
4.1. Study Setting, Patients and Sample Collection, and Study Design
The Laboratori Clínic Metropolitana Nord, Germans Trias i Pujol University Hospital (Badalona, Spain) is a laboratory with an influence area covering a total of 1,500,000 inhabitants with more than 100 primary care facilities—including Sexual Reproductive Health Centers (ASSIR)—that centralizes the analysis of all the specimens together with the ones derived from the tertiary hospital Germans Trias i Pujol.
A total of 415 samples were collected by physicians between 2016 and 2018 from 407 patients for whom STI testing was ordered, including symptomatic, asymptomatic, or STI contacts.
Most samples (n = 371) belonged to young people recruited in ASSIRs for epidemiological surveillance purposes to monitor C. trachomatis (CT) prevalence among those under 25 years of age with high-risk sexual behavior [37]. This surveillance has been performed in Catalonia since 2007. The other 44 samples were from the HIV Unit or Gynecology and Obstetrics Department of the Germans Trias i Pujol University Hospital.
The study was designed with a retrospective and a prospective part. For the first phase, a retrospective analysis included 234 MG-positive samples received between 2016 and 2017. During the second phase, a one-year prospective study was carried out from December 2017 to November 2018. A total of 181 MG-positive samples were collected from 173 patients that required STI testing at our medical institution or ASSIR Centers (Badalona and Mataró, Barcelona, Spain). Detailed information is displayed in Table 1.
4.2. Clinical and Microbiological Data
Demographic data (gender, age) were recorded for all MG-positive patients, and epidemiological information such as risk factors for STI (more than 2 sexual partners in the last 6 months, new sexual partner, intermittent condom use, prior STI…), previous antibiotic therapy, symptomatology, and current treatment was registered in the prospective study when available (136 out of 181 patients included in the prospective evaluation). Microbiological data such as the detection of concomitant STIs, syphilis, or HIV, was provided by the Microbiology Department. More information can be found in Table 2.
4.3. Diagnosis of Mycoplasma genitalium
A variety of samples including endocervical, urethral, or rectal swabs and urine samples were molecularly tested for sexual transmitted diseases using the Real-Time PCR STI detection Allplex STI-7 Assay (Seegene Inc., Seoul, Korea), following the manufacturer’s instructions. DNA was previously extracted by either the Microlab NIMBUS (Hamilton Company, Reno, NV, USA) or the STARlet IVD platforms (Seegene Inc., Seoul, Korea).
4.4. Macrolide and Fluoroquinolone Resistance Detection
MG-positive samples were subsequently investigated for macrolide resistance by pyrosequencing, as previously described [28], but using the primers described by Jensen et al. for both PCR and pyrosequencing [8]. The pyrosequencing protocol was optimized using a total of 6 MG-positive samples from external European and Spanish quality programs (Quality Control for Molecular Diagnostics program—QCMD and SEIMC Quality Control Program), sent to multiple laboratories as reference samples for MG detection and macrolide resistance analysis. Given that the mutations associated with macrolide resistance are located in region V of MG 23S rRNA gene, our prior pyrosequencing protocol [28] was modified to a single 45 cycles amplification with a final volume of 50 µL. As previously described by Spuesens et al. [38], this protocol includes four general steps: generating 5′-biotynilated products, processing PCR products to obtain single-stranded DNA where the sequence primer will anneal, sequencing, and analyzing the results.
With this purpose, PCR mixtures (50 µL) contained 0.4 µM of the biotinylated primers Mg 23S-1992Bio and Mg 23S-2138R [8], 0.2 mM of deoxynucleoside triphosphate set (Sigma Aldrich, San Luis, MO, USA), 1× Pfu Buffer (Promega Corporation, Madison, WI, USA), 0.02 U/µL of Pfu DNA polymerase (Promega), 26.6 µL of PCR grade water, and 15 µL of DNA template. The following cycling conditions were used: 5 min at 94 °C, followed by 45 cycles of 30 s at 94 °C, 30 s at 58 °C, and 30 s at 72 °C. A negative control was taken along in each PCR run. The presence of the 147-bp amplified fragment was detected by high-resolution capillary electrophoresis (QIAxcel® Advanced System, Qiagen, Germany).
The resulting biotinylated products were immobilized to Streptavidin Sepharose™ High Performance beads (GE Healthcare) and processed to obtain high-quality single-stranded DNA using the Pyromark™ Vacuum Prep Workstation, according to manufacturer’s instructions. The immobilization and pyrosequencing reactions were based on the protocol of Spuesens et al. [38] with the following modifications: a total 4 µL of streptavidin beads and 26 µL of H2O per sample were used, and the plates were mixed for 10 min instead of 15 min [28].
To evaluate pyrosequencing as an adequate method for MLr study in MG, a subset of 100 samples previously processed by pyrosequencing and that included strains with A2058G (n = 36), A2059G (n = 25), or A2058T (n = 3) mutations and WT samples (n = 36) (including five samples from the European Quality Control—QCMD) was further analyzed by ResistancePlus® MG kit (SpeeDx, Sydney, NSW, Australia). This kit offers the simultaneous detection of MG and 5 mutations at positions 2058 and 2059 in the 23S rRNA gene (E. coli numbering) that are associated with macrolide resistance.
Finally, fluoroquinolone resistance was detected in the same subset by sequencing the parC gene [39,40]. Both processes were carried out at the University of Bordeaux, France.
5. Conclusions
This study provides valuable information about M. genitalium macrolide and fluoroquinolone resistance rates in the young population with STI risk in Badalona, Spain, where there was a lack of data for comparison with other European countries. Pyrosequencing, despite being more time-consuming, is a cheap and useful tool to detect MLr, allowing epidemiological purposes and new mutations description. Given the rate of resistant strains detected in Badalona, Spain, simultaneous and accurate diagnosis of MG and its ML resistance patterns, using either in-house or commercial near-patient reagents that provide results without delay, should be implemented in clinical laboratories. These technologies could substantially improve patient’s clinical management applying resistance-guided treatment strategies, decreasing treatment failures, and lowering total costs.
Author Contributions
Conceptualization, L.M., G.F.-R. and B.R.; methodology, L.M., G.F.-R. and B.R.; validation, C.L.R., G.F.-R., E.J.-L. and B.R.; formal analysis, E.J.-L. and B.R.; investigation, C.L.R., C.C., V.G., J.H.W.-W. and B.R.; resources, C.B., S.P., C.L.R., L.M., V.G. and B.R.; data curation, E.J.-L., J.H.W.-W., C.L.R. and B.R.; writing—original draft preparation, B.R.; writing—review and editing, L.M., C.B., S.P., G.F.-R., E.J.-L. and B.R.; funding acquisition, L.M. and B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by a Germans Trias grant (Programa Talents. Fundació Catalunya-La Pedrera) and the fellowship awarded by the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) to B.R. (Ayuda SEIMC 6/2019).
Institutional Review Board Statement
The study design, including the use of stored samples for the retrospective phase, was approved by the Clinical Research Ethics Committee at Germans Trias i Pujol University Hospital (“Comité Ético de Investigación Clínica”, CEIC, code PI-17-182). The use of a subset of samples from the retrospective phase, belonging to users of Sexual Reproductive Care Centers, was also supported by the Ethics Committee (codes EO-12-014 and PI-17-217).
Informed Consent Statement
Written informed consent was obtained from patients during the prospective phase of the study.
Data Availability Statement
Data are available on reasonable request from the corresponding author.
Acknowledgments
We would like to thank the molecular biology area for their technical support.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Taylor-Robinson, D.; Jensen, J.S. Mycoplasma genitalium: From Chrysalis to multicolored butterfly. Clin. Microbiol. Rev. 2011, 24, 498–514. [Google Scholar] [CrossRef]
- Lis, R.; Rowhani-Rahbar, A.; Manhart, L.E. Mycoplasma genitalium infection and female reproductive tract disease: A meta-analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 418–426. [Google Scholar] [CrossRef]
- Jensen, J.S. Mycoplasma genitalium: The aetiological agent of urethritis and other sexually transmitted diseases. J. Eur. Acad. Dermatol. Venereol. JEADV 2004, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.S.; Cusini, M.; Gomberg, M.; Moi, H.; Wilson, J.; Unemo, M. 2021 European guideline on the management of Mycoplasma genitalium infections. J. Eur. Acad. Dermatol. Venereol. JEADV 2022. [Google Scholar] [CrossRef] [PubMed]
- Lau, A.; Bradshaw, C.S.; Lewis, D.; Fairley, C.K.; Chen, M.Y.; Kong, F.Y.; Hocking, J.S. The Efficacy of Azithromycin for the Treatment of Genital Mycoplasma genitalium: A Systematic Review and Meta-analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 1389–1399. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Le, W.J.; Li, S.; Cao, Y.P.; Su, X.H. Meta-analysis of the efficacy of moxifloxacin in treating Mycoplasma genitalium infection. Int. J. STD AIDS 2017, 28, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Mena, L.A.; Mroczkowski, T.F.; Nsuami, M.; Martin, D.H. A randomized comparison of azithromycin and doxycycline for the treatment of Mycoplasma genitalium-positive urethritis in men. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2009, 48, 1649–1654. [Google Scholar] [CrossRef]
- Jensen, J.S. Protocol for the detection of Mycoplasma genitalium by PCR from clinical specimens and subsequent detection of macrolide resistance-mediating mutations in region V of the 23S rRNA gene. Methods Mol. Biol. 2012, 903, 129–139. [Google Scholar] [CrossRef]
- Touati, A.; Peuchant, O.; Jensen, J.S.; Bebear, C.; Pereyre, S. Direct detection of macrolide resistance in Mycoplasma genitalium isolates from clinical specimens from France by use of real-time PCR and melting curve analysis. J. Clin. Microbiol. 2014, 52, 1549–1555. [Google Scholar] [CrossRef]
- Le Roy, C.; Bebear, C.; Pereyre, S. Performance of Three Commercial Molecular Diagnostic Assays for the Simultaneous Detection of Mycoplasma genitalium and Macrolide Resistance. J. Clin. Microbiol. 2021, 59, e00020-21. [Google Scholar] [CrossRef]
- Couldwell, D.L.; Tagg, K.A.; Jeoffreys, N.J.; Gilbert, G.L. Failure of moxifloxacin treatment in Mycoplasma genitalium infections due to macrolide and fluoroquinolone resistance. Int. J. STD AIDS 2013, 24, 822–828. [Google Scholar] [CrossRef]
- Hamasuna, R.; Le, P.T.; Kutsuna, S.; Furubayashi, K.; Matsumoto, M.; Ohmagari, N.; Fujimoto, N.; Matsumoto, T.; Jensen, J.S. Mutations in ParC and GyrA of moxifloxacin-resistant and susceptible Mycoplasma genitalium strains. PLoS ONE 2018, 13, e0198355. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Huerta, M.; Bodiyabadu, K.; Esperalba, J.; Bradshaw, C.S.; Serra-Pladevall, J.; Garland, S.M.; Fernandez-Naval, C.; Jensen, J.S.; Pumarola, T.; Ebeyan, S.; et al. Multicenter clinical evaluation of a novel multiplex real-time PCR (qPCR) assay for detection of fluoroquinolone resistance in Mycoplasma genitalium. J. Clin. Microbiol. 2019, 57, e00886-19. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, E.L.; Lowry, K.; Ebeyan, S.; Lundgren, M.; Whiley, D.M. Evaluation of the SpeeDx MG parC (Beta) PCR Assay for Rapid Detection of Mycoplasma genitalium Quinolone Resistance-Associated Mutations. J. Clin. Microbiol. 2020, 58, 4045–4048. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Huerta, M.; Vall, M.; Fernandez-Naval, C.; Barbera, M.J.; Arando, M.; Lopez, L.; Andreu, A.; Pumarola, T.; Serra-Pladevall, J.; Esperalba, J.; et al. Mycoplasma genitalium macrolide resistance update: Rate among a 2016–2017 cohort of patients in Barcelona, Spain. Enferm. Infecc. Microbiol. Clin. 2019, 38, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Huerta, M.; Serra-Pladevall, J.; Esperalba, J.; Espasa, M. Mycoplasma genitalium and fluoroquinolone resistance: From genotype to phenotype. Enferm. Infecc. Microbiol. Clin. 2019, 38, 44–45. [Google Scholar] [CrossRef]
- Pineiro, L.; Idigoras, P.; de la Caba, I.; Lopez-Olaizola, M.; Cilla, G. Guided antibiotic therapy for Mycoplasma genitalium infections: Analysis of mutations associated with resistance to macrolides and fluoroquinolones. Enferm. Infecc. Microbiol. Clin. 2019, 37, 394–397. [Google Scholar] [CrossRef]
- Lucena Nemirosky, J.; Espelt, R.; Lopez Grado, E.; Sobrino, J.; Acera, A.; Perez, J.; Jensen, J.S.; Sanchez-Reus, F.; Prim, N. Macrolide resistance in Mycoplasma genitalium in Catalonia, Spain: A 1 year prospective study. J. Antimicrob. Chemother. 2021, 76, 2702–2707. [Google Scholar] [CrossRef]
- Tully, J.G.; Taylor-Robinson, D.; Rose, D.L.; Cole, R.M.; Bove, J.M. Mycoplasma genitalium, a new species from the human urogenital tract. Int. J. Syst. Evol. Microbiol. 1983, 33, 387–396. [Google Scholar] [CrossRef]
- Fernandez-Huerta, M.; Barbera, M.J.; Serra-Pladevall, J.; Esperalba, J.; Martinez-Gomez, X.; Centeno, C.; Pich, O.Q.; Pumarola, T.; Espasa, M. Mycoplasma genitalium and antimicrobial resistance in Europe: A comprehensive review. Int. J. STD AIDS 2020, 31, 190–197. [Google Scholar] [CrossRef]
- Machalek, D.A.; Tao, Y.; Shilling, H.; Jensen, J.S.; Unemo, M.; Murray, G.; Chow, E.P.F.; Low, N.; Garland, S.M.; Vodstrcil, L.A.; et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: A systematic review and meta-analysis. Lancet Infect. Dis. 2020, 20, 1302–1314. [Google Scholar] [CrossRef]
- Read, T.R.H.; Murray, G.L.; Danielewski, J.A.; Fairley, C.K.; Doyle, M.; Worthington, K.; Su, J.; Mokany, E.; Tan, L.T.; Lee, D.; et al. Symptoms, Sites, and Significance of Mycoplasma genitalium in Men Who Have Sex with Men. Emerg. Infect. Dis. 2019, 25, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, G.; Martro, E.; Gonzalez, V.; Saludes, V.; Bascunana, E.; Marco, C.; Rivaya, B.; Lopez, E.; Coll, P.; Matas, L.; et al. Usefulness of a novel multiplex real-time PCR assay for the diagnosis of sexually-transmitted infections. Enferm. Infecc. Microbiol. Clin. 2016, 34, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Soni, S.; Horner, P.; Rayment, M.; Pinto-Sander, N.; Naous, N.; Parkhouse, A.; Bancroft, D.; Patterson, C.; Fifer, H. British Association for Sexual Health and HIV national guideline for the management of infection with Mycoplasma genitalium (2018). Int. J. STD AIDS 2019, 30, 938–950. [Google Scholar] [CrossRef] [PubMed]
- Cina, M.; Baumann, L.; Egli-Gany, D.; Halbeisen, F.S.; Ali, H.; Scott, P.; Low, N. Mycoplasma genitalium incidence, persistence, concordance between partners and progression: Systematic review and meta-analysis. Sex. Transm. Infect. 2019, 95, 328–335. [Google Scholar] [CrossRef]
- Vazquez, F.; Fernandez, J. Resistance-Guided Therapy for Mycoplasma genitalium Infections. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 1469–1471. [Google Scholar] [CrossRef]
- Horner, P.; Donders, G.; Cusini, M.; Gomberg, M.; Jensen, J.S.; Unemo, M. Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women?—A position statement from the European STI Guidelines Editorial Board. J. Eur. Acad. Dermatol. Venereol. JEADV 2018, 32, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Rivaya, B.; Jordana-Lluch, E.; Fernandez-Rivas, G.; Molinos, S.; Campos, R.; Mendez-Hernandez, M.; Matas, L. Macrolide resistance and molecular typing of Mycoplasma pneumoniae infections during a 4 year period in Spain. J. Antimicrob. Chemother. 2020, 75, 2752–2759. [Google Scholar] [CrossRef] [PubMed]
- Le Roy, C.; Henin, N.; Bebear, C.; Pereyre, S. Evaluation of a Commercial Multiplex Quantitative PCR (qPCR) Assay for Simultaneous Detection of Mycoplasma genitalium and Macrolide Resistance-Associated Mutations in Clinical Specimens. J. Clin. Microbiol. 2017, 55, 978–979. [Google Scholar] [CrossRef]
- Asenjo, A.; Kusters, J.G.; Severs, T.T.; Alos, J.I. Mycoplasma genitalium in Spain: Prevalence of genital infection and frequency of resistance to macrolides. Enferm. Infect. Microbiol. Clin. 2018, 36, 169–171. [Google Scholar] [CrossRef]
- Trevino, M.; Rodriguez-Velasco, M.; Manso, T.; Cea, M. Mycoplasma genitalium in Primary Care: Prevalence and azithromycin resistance in Santiago de Compostela Health Care Area. Rev. Esp. Quimioter. 2021, 34, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Adelantado Lacasa, M.; Beristain, X. Prevalence of Mycoplasma genitalium infection and antibiotic resistance in Navarra (North Spain). Sex. Transm. Infect. 2019, 95, 549. [Google Scholar] [CrossRef] [PubMed]
- de Salazar, A.; Barrientos-Duran, A.; Espadafor, B.; Fuentes-Lopez, A.; Chueca, N.; Garcia, F. Macrolide and fluoroquinolone resistance of Mycoplasma genitalium in southern Spain, 2018–2019. Sex. Transm. Infect. 2021, 97, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Munoz Santa, A.; Aramburu Arnuelos, J.; Bernet Sanchez, A.; Belles Belles, A. Mycoplasma genitalium: Analysis of mutations associated with macrolide resistance in Lleida, Spain. Enferm. Infect. Microbiol. Clin. 2021, 285, 106034. [Google Scholar] [CrossRef]
- Barbera, M.J.; Fernandez-Huerta, M.; Jensen, J.S.; Caballero, E.; Andreu, A. Mycoplasma genitalium Macrolide and Fluoroquinolone Resistance: Prevalence and Risk Factors among a 2013–2014 Cohort of Patients in Barcelona, Spain. Sex. Transm. Dis. 2017, 44, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Dionne-Odom, J.; Geisler, W.M.; Aaron, K.J.; Waites, K.B.; Westfall, A.O.; Van Der Pol, B.; Xiao, L. High Prevalence of Multidrug-Resistant Mycoplasma genitalium in Human Immunodeficiency Virus-Infected Men Who Have Sex with Men in Alabama. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 66, 796–798. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Corbeto, E.; Gonzalez, V.; Casabona, J.; Grupo de estudio CN-A. Prevalence and re-infection rate of C. trachomatis genital infections in young people under 25 years in Catalonia. Enferm. Infecc. Y Microbiol. Clin. 2017, 35, 359–363. [Google Scholar] [CrossRef]
- Spuesens, E.B.; Hoogenboezem, T.; Sluijter, M.; Hartwig, N.G.; van Rossum, A.M.; Vink, C. Macrolide resistance determination and molecular typing of Mycoplasma pneumoniae by pyrosequencing. J. Microbiol. Methods 2010, 82, 214–222. [Google Scholar] [CrossRef]
- Tagg, K.A.; Jeoffreys, N.J.; Couldwell, D.L.; Donald, J.A.; Gilbert, G.L. Fluoroquinolone and macrolide resistance-associated mutations in Mycoplasma genitalium. J. Clin. Microbiol. 2013, 51, 2245–2249. [Google Scholar] [CrossRef]
- Yamaguchi, Y.; Takei, M.; Kishii, R.; Yasuda, M.; Deguchi, T. Contribution of topoisomerase IV mutation to quinolone resistance in Mycoplasma genitalium. Antimicrob. Agents Chemother. 2013, 57, 1772–1776. [Google Scholar] [CrossRef] [PubMed][Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).