
Antibiotic Therapy for Prosthetic Joint Infections: An Overview

Abstract
1. Introduction
2. Initial IV Antibiotics and Extended Infusion
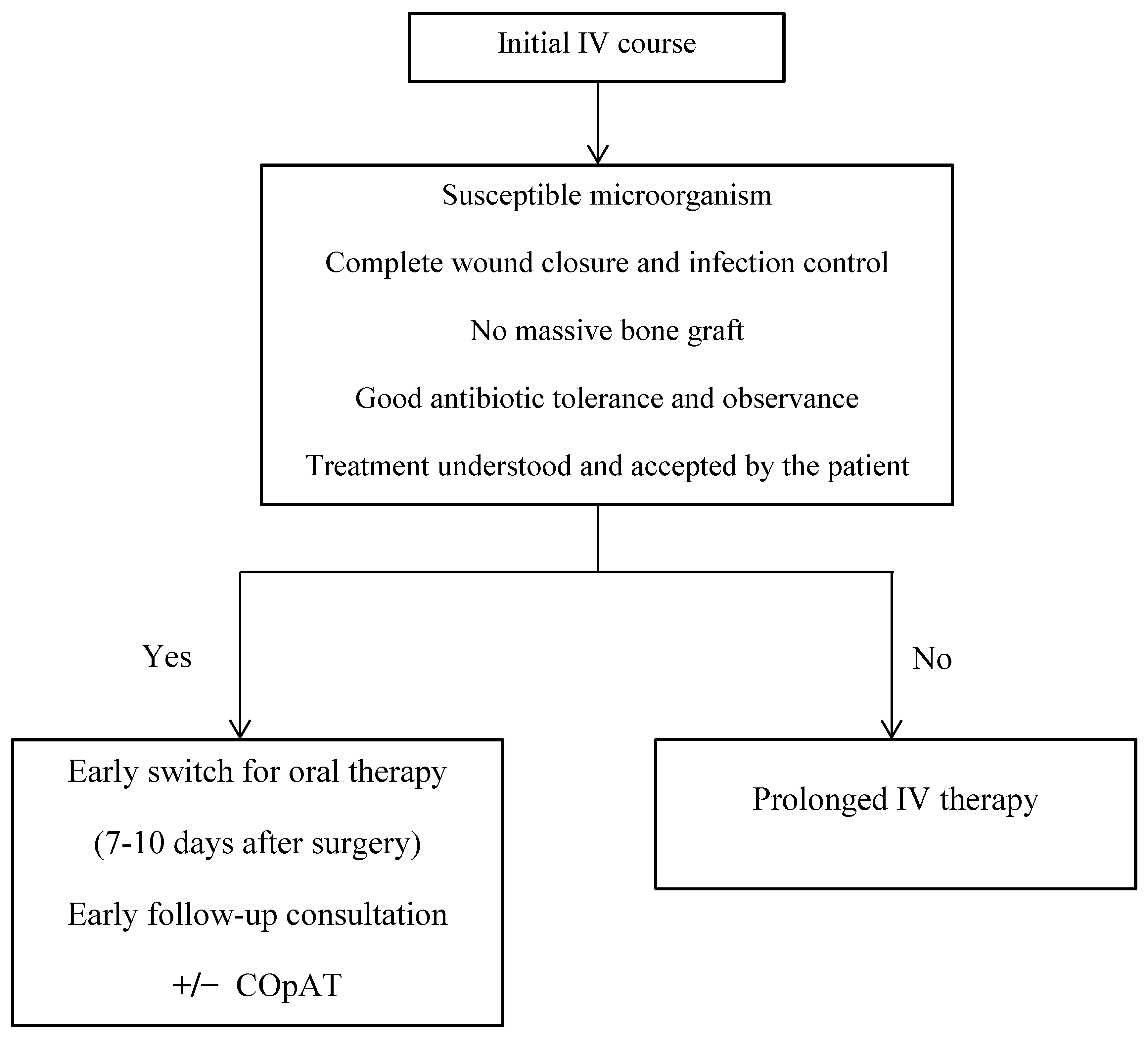
3. Oral vs. IV Therapy
4. Patient Education
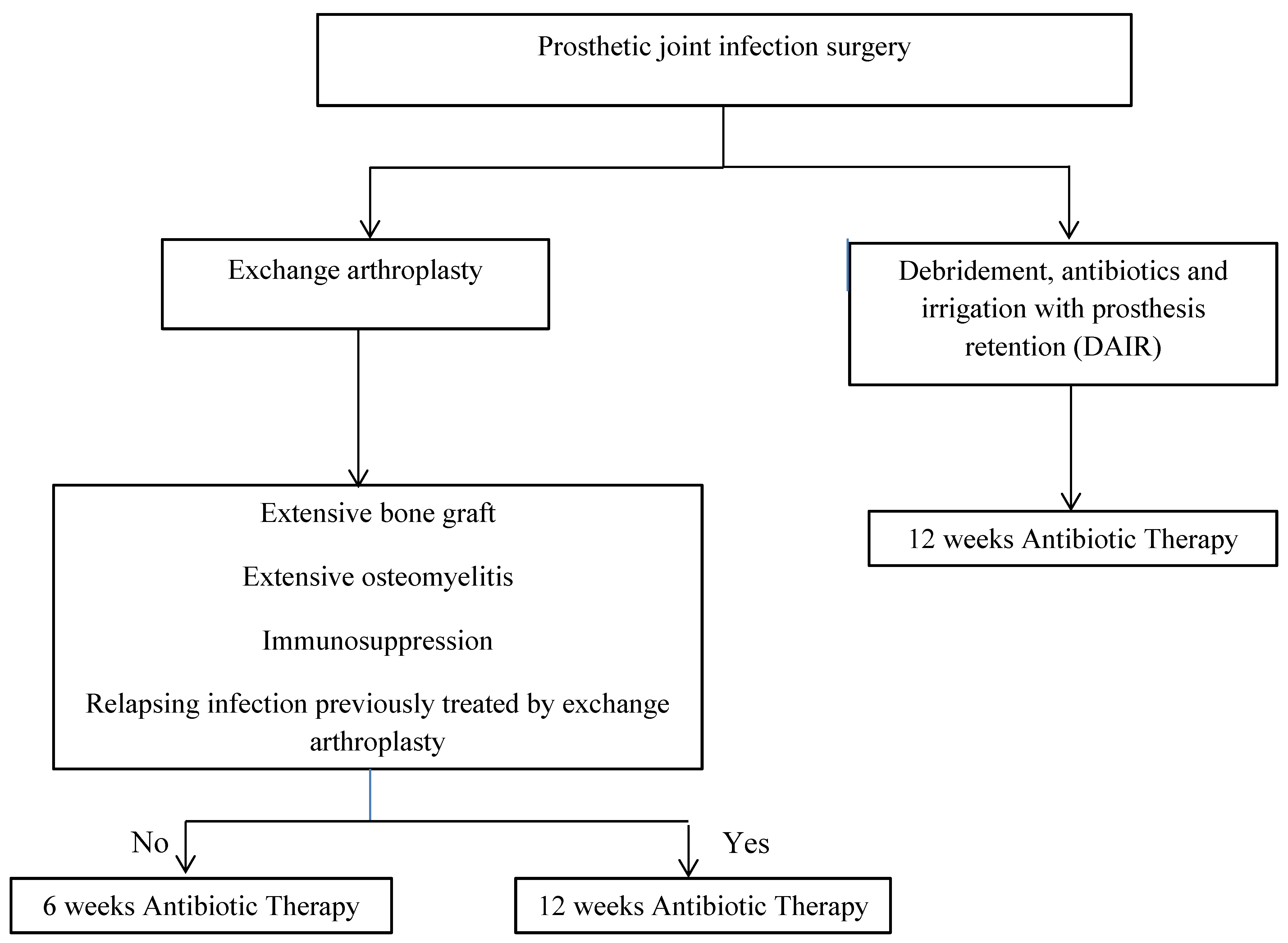
5. Antibiotic Treatment Duration
6. Antibiofilm-Active Drugs
7. Bone Penetration
8. Therapeutic Drug Monitoring (TDM)
9. Empirical Antibiotic Regimens
10. Pathogen-Specific Antibiotic Therapies
10.1. Staphylococcal PJIs
10.2. Streptococcal PJIs
10.3. Enterococcus PJIs
10.4. Pseudomonas aeruginosa PJIs
10.5. Enterobacteriaceae Infections
10.6. Cutibacterium PJIs
10.7. Corynebacterium spp. Infections
10.8. Culture-Negative PJIs
11. Antibiotic Prophylaxis
12. Preoperative Antibiotics
13. Long-Term Suppressive Therapy
14. Perspectives
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erivan, R.; Villatte, G.; Dartus, J.; Reina, N.; Descamps, S.; Boisgard, S. Progression and projection for hip surgery in France, 2008–2070: Epidemiologic study with trend and projection analysis. Orthop. Traumatol. Surg. Res. 2019, 105, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Namba, R.S.; Inacio, M.C.; Paxton, E.W. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: An analysis of 56,216 knees. J. Bone Jt. Surg. Am. 2013, 95, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.R.; Peterson, K.D.; Mu, Y.; Banerjee, S.; Allen-Bridson, K.; Morrell, G.; Dudeck, M.A.; Pollock, D.A.; Horan, T.C. National Healthcare Safety Network (NHSN) report: Data summary for 2006 through 2008, issued December 2009. Am. J. Infect. Control 2009, 37, 783–805. [Google Scholar] [CrossRef] [PubMed]
- Jauregui, J.J.; Tran, A.; Kaveeshwar, S.; Nadarajah, V.; Chaudhri, M.W.; Henn, R.F.; Gilotra, M.N.; Hasan, S.A. Diagnosing a periprosthetic shoulder infection: A systematic review. J. Orthop. 2021, 26, 58–66. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Infectious Diseases Society of America. Executive summary: Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, 1–10. [Google Scholar] [CrossRef]
- Triffault-Fillit, C.; Ferry, T.; Laurent, F.; Pradat, P.; Dupieux, C.; Conrad, A.; Becker, A.; Lustig, S.; Fessy, M.H.; Chidiac, C.; et al. Microbiologic epidemiology depending on time to occurrence of prosthetic joint infection: A prospective cohort study. Clin. Microbiol. Infect. 2019, 25, 353–358. [Google Scholar] [CrossRef]
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorli, L.; Fresco, G.; Fernandez-Sampedro, M.; Del Toro, M.D.; Guıo, L.; et al. Time trends in the etiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef]
- Zeller, V.; Kerroumi, Y.; Meyssonnier, V.; Heym, B.; Metten, M.A.; Desplaces, N.; Marmor, S. Analysis of postoperative and hematogenous prosthetic joint-infection microbiological patterns in a large cohort. J. Infect. 2018, 76, 328–334. [Google Scholar] [CrossRef]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar]
- Zeller, V.; Magreault, S.; Heym, B.; Salmon, D.; Kitzis, M.D.; Billaud, E.; Marmor, S.; Jannot, A.S.; Salomon, L.; Jullien, V. Influence of the clindamycin administration route on the magnitude of clindamycin-rifampicin interaction: A prospective pharmacokinetic study. Clin. Microbiol. Infect. 2021, 27, 1857.e1–1857.e7. [Google Scholar] [CrossRef]
- Fischbacher, A.; Borens, O. Prosthetic-joint Infections: Mortality Over the Last 10 Years. J. Bone Jt. Infect. 2019, 4, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Courjon, J.; Garzaro, M.; Roger, P.M.; Ruimy, R.; Lavrut, T.; Chelli, M.; Raynier, J.L.; Chirio, D.; Demonchy, E.; Cabane, L.; et al. A population pharmacokinetic analysis of continuous infusion of cloxacillin during Staphylococcus aureus bone and joint infections. Antimicrob. Agents Chemother. 2020, 64, e01562-20. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Durand, F.; Kitzis, M.D.; Lhotellier, L.; Ziza, J.M.; Mamoudy, P.; Desplaces, N. Continuous cefazolin infusion to treat bone and joint infections: Clinical efficacy, feasibility, safety, and serum and bone concentrations. Antimicrob. Agents Chemother. 2009, 53, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Dzeing-Ella, A.; Kitzis, M.D.; Ziza, J.M.; Mamoudy, P.; Desplaces, N. Continuous clindamycin infusion, an innovative approach to treating bone and joint infections. Antimicrob. Agents Chemother. 2010, 54, 88–92. [Google Scholar] [CrossRef]
- Dubée, V.; Zeller, V.; Lhotellier, L.; Kitzis, M.D.; Ziza, J.M.; Mamoudy, P.; Desplaces, N. Continuous high-dose vancomycin combination therapy for methicillin-resistant staphylococcal prosthetic hip infection: A prospective cohort study. Clin. Microbiol. Infect. 2013, 19, E98–E105. [Google Scholar] [CrossRef]
- Prié, H.; Meyssonnier, V.; Kerroumi, Y.; Heym, B.; Lidove, O.; Marmor, S.; Zeller, V. Pseudomonas aeruginosa prosthetic joint-infection outcomes: Prospective, observational study on 43 patients. J. Infect. submitted.
- Curis, E.; Pestre, V.; Jullien, V.; Eyrolle, L.; Archambeau, D.; Morand, P.; Gatin, L.; Karoubi, M.; Pinar, N.; Dumaine, V.; et al. Pharmacokinetic variability of clindamycin and influence of rifampicin on clindamycin concentration in patients with bone and joint infections. Infection 2015, 43, 473–481. [Google Scholar] [CrossRef]
- McKinnon, P.S.; Paladino, J.A.; Schentag, J.J. Evaluation of area under the inhibitory curve (AUIC) and time above the minimum inhibitory concentration (T > MIC) as predictors of outcome for cefepime and ceftazidime in serious bacterial infections. Int. J. Antimicrob. Agents 2008, 31, 345–351. [Google Scholar] [CrossRef]
- Chytra, I.; Stepan, M.; Benes, J.; Pelnar, P.; Zidkova, A.; Bergerova, T.; Pradl, R.; Kasal, E. Clinical and microbiological efficacy of continuous versus intermittent application of meropenem in critically ill patients: A randomized open-label controlled trial. Crit. Care 2012, 16, R113. [Google Scholar] [CrossRef]
- Lorente, L.; Lorenzo, L.; Martín, M.M.; Jiménez, A.; Mora, M.L. Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to Gram-negative bacilli. Ann. Pharmacother. 2006, 40, 219–223. [Google Scholar] [CrossRef]
- Longuet, P.; Lecapitaine, A.L.; Cassard, B.; Batista, R.; Gauzit, R.; Lesprit, P.; Haddad, R.; Vanjak, D.; Diamantis, S.; Groupe des référents en infectiologie d’Île-de-France (GRIF). Preparing and administering injectable antibiotics: How to avoid playing God. Med. Mal. Infect. 2016, 46, 242–268. [Google Scholar] [CrossRef] [PubMed]
- Shrayteh, Z.M.; Rahal, M.K.; Malaeb, D.N. Practice of switch from intravenous to oral antibiotics. Springerplus 2014, 3, 717. [Google Scholar] [CrossRef] [PubMed]
- Li, H.K.; Rombach, I.; Zambellas, R.; Walker, A.S.; McNally, M.A.; Atkins, B.L.; Lipsky, B.A.; Hughes, H.C.; Bose, D.; Kümin, M.; et al. Oral versus intravenous antibiotics for bone and joint infection. N. Engl. J. Med. 2019, 380, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Conterno, L.O.; Turchi, M.D. Antibiotics for treating chronic osteomyelitis in adults. Cochrane Database Syst. Rev. 2013, 9, CD004439. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sanchez-Somolinos, M.; Baraia- Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodrıguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef]
- Rodríguez-Pardo, D.; Pigrau, C.; Lora-Tamayo, J.; Soriano, A.; del Toro, M.D.; Cobo, J.; Palomino, J.; Euba, G.; Riera, M.; Sánchez-Somolinos, M.; et al. Gram-negative prosthetic joint infection: Outcome of a debridement; antibiotics and implant retention approach. A large multicentre study. Clin. Microbiol. Infect. 2014, 20, O911–O919. [Google Scholar] [CrossRef]
- Mahoney, M.V.; Swords, K.E. Fluoroquinolones: Friends or foes? Clin. Infect. Dis. 2021, 73, 857–858. [Google Scholar] [CrossRef]
- Seaton, R.A.; Ritchie, N.D.; Robb, F.; Stewart, L.; White, B.; Vallance, C. From ‘OPAT’ to ‘COpAT’: Implications of the OVIVA study for ambulatory management of bone and joint infection. J. Antimicrob. Chemother. 2019, 74, 2119–2121. [Google Scholar] [CrossRef]
- Kardas, P.; Devine, S.; Golembesky, A.; Roberts, C. A systematic review and meta-analysis of misuse of antibiotic therapies in the community. Int. J. Antimicrob. Agents 2005, 26, 106–113. [Google Scholar] [CrossRef]
- West, L.M.; Cordina, M. Educational intervention to enhance adherence to short-term use of antibiotics. Res. Soc. Adm. Pharm. 2019, 15, 193–201. [Google Scholar] [CrossRef]
- McKenna, P.; O’Shea, K.; Masterson, E. Two-stage revision of infected hip arthroplasty using a shortened post-operative course of antibiotics. Arch. Orthop. Trauma Surg. 2009, 129, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Euba, G.; Cobo, J.; Horcajada, J.P.; Soriano, A.; Sandoval, E.; Pigrau, C.; Benito, N.; Falgueras, L.; Palomino, J.; et al. Short- versus long-duration levofloxacin plus rifampicin for acute staphylococcal prosthetic joint infection managed with implant retention: A randomised clinical trial. Int. J. Antimicrob. Agents 2016, 48, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Benkabouche, M.; Racloz, G.; Spechbach, H.; Lipsky, B.A.; Gaspoz, J.M.; Uçkay, I. Four versus six weeks of antibiotic therapy for osteoarticular infections after implant removal: A randomized trial. J. Antimicrob. Chemother. 2019, 74, 2394–2399. [Google Scholar] [CrossRef] [PubMed]
- Bernard, L.; Arvieux, C.; Brunschweiler, B.; Touchais, S.; Ansart, S.; Bru, J.P.; Oziol, E.; Boeri, C.; Gras, G.; Druon, J.; et al. Antibiotic therapy for 6 or 12 weeks for prosthetic joint infection. N. Engl. J. Med. 2021, 384, 1991–2001. [Google Scholar] [CrossRef]
- Lamret, F.; Colin, M.; Mongaret, C.; Gangloff, S.C.; Reffuveille, F. Antibiotic tolerance of Staphylococcus aureus biofilm in periprosthetic joint infections and antibiofilm strategies. Antibiotics. 2020, 9, 547. [Google Scholar] [CrossRef]
- Jacqueline, C.; Caillon, J. Impact of bacterial biofilm on the treatment of prosthetic joint infections. J. Antimicrob. Chemother. 2014, 69 (Suppl. 1), i37–i40. [Google Scholar] [CrossRef]
- Høiby, N.; Bjarnsholt, T.; Givskov, M.; Molin, S.; Ciofu, O. Antibiotic resistance of bacterial biofilms. Int. J. Antimicrob. Agents 2010, 35, 322–332. [Google Scholar] [CrossRef]
- Shoji, M.M.; Chen, A.F. Biofilms in periprosthetic joint infections: A review of diagnostic modalities, current treatments and future directions. J. Knee Surg. 2020, 33, 119–131. [Google Scholar] [CrossRef]
- Hirai, J.; Hagihara, M.; Kato, H.; Sakanashi, D.; Nishiyama, N.; Koizumi, Y.; Yamagishi, Y.; Suematsu, H.; Hanaki, H.; Mikamo, H. Investigation on rifampicin administration from the standpoint of pharmacokinetics/pharmacodynamics in a neutropenic murine thigh infection model. J. Infect. Chemother. 2016, 22, 387–394. [Google Scholar] [CrossRef]
- Sousa, R.; Abreu, M.A. Treatment of Prosthetic Joint Infection with Debridement, Antibiotics and Irrigation with Implant Retention—A Narrative Review. J. Bone Jt. Infect. 2018, 3, 108–117. [Google Scholar] [CrossRef]
- Saginur, R.; StDenis, M.; Ferris, W.; Aaron, S.D.; Chan, F.; Lee, C.; Ramotar, K. Multiple combination bactericidal testing of staphylococcal biofilms from implant-associated infections. Antimicrob. Agents Chemother. 2006, 50, 55–61. [Google Scholar] [CrossRef]
- Raad, I.; Hanna, H.; Jiang, Y.; Dvorak, T.; Reitzel, R.; Chaiban, G.; Sherertz, R.; Hachem, R. Comparative activities of daptomycin, linezolid, and tigecycline against catheter-related methicillin-resistant Staphylococcus bacteremic isolates embedded in biofilm. Antimicrob. Agents Chemother. 2007, 51, 1656–1660. [Google Scholar] [CrossRef]
- Tonnelier, M.; Bouras, A.; Joseph, C.; Samad, Y.E.; Brunschweiler, B.; Schmit, J.L.; Mabille, C.; Lanoix, J.P. Impact of rifampicin dose in bone and joint prosthetic device infections due to Staphylococcus spp.: A retrospective single-center study in France. BMC Infect. Dis. 2021, 21, 174. [Google Scholar]
- Roblot, F.; Besnier, J.M.; Giraudeau, B.; Simonnard, N.; Jonville-Bera, A.P.; Coipeau, P.; Choutet, P.; Autret-Leca, E.; Le Guellec, C. Lack of association between rifampicin plasma concentration and treatment-related side effects in osteoarticular infections. Fundam. Clin. Pharmacol. 2007, 21, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.; Peloquin, C.; Burman, W.; Luo, C.C.; Engle, M.; Prihoda, T.J.; Mac Kenzie, W.R.; Bliven-Sizemore, E.; Johnson, J.L.; Vernon, A. Effects of tuberculosis, race, and human gene SLCO1B1 polymorphisms on rifampin concentrations. Antimicrob. Agents Chemother. 2010, 54, 4192–4200. [Google Scholar]
- Cresswell, F.V.; Meya, D.B.; Kagimu, E.; Grint, D.; Te Brake, L.; Kasibante, J.; Martyn, E.; Rutakingirwa, M.; Quinn, C.M.; Okirwoth, M.; et al. High-dose oral and intravenous rifampicin for the treatment of tuberculous meningitis in predominantly human immunodeficiency virus (HIV)-positive Ugandan adults: A phase ii open-label randomized controlled trial. Clin. Infect. Dis. 2021, 73, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Aarnoutse, R.E.; Kibiki, G.S.; Reither, K.; Semvua, H.H.; Haraka, F.; Mtabho, C.M.; Mpagama, S.G.; van den Boogaard, J.; Sumari-de Boer, I.M.; Magis-Escurra, C.; et al. Pharmacokinetics, tolerability, and bacteriological response of rifampin administered at 600, 900, and 1200 milligrams daily in patients with pulmonary tuberculosis. Antimicrob. Agents Chemother. 2017, 61, e01054-17. [Google Scholar] [PubMed]
- Zimmerli, W.; Sendi, P. Orthopaedic biofilm infections. APMIS 2017, 125, 353–364. [Google Scholar] [CrossRef]
- Bamberger, D.; Foxworth, J.; Bridwell, D.; Shain, C.; Gerding, D. Extravascular antimicrobial distribution and the respective blood and urine concentrations in humans. In Antibiotics in Laboratory Medicine; Lorian, V., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; pp. 719–814. [Google Scholar]
- Boselli, E.; Allaouchiche, B. Diffusion in bone tissue of antibiotics. Presse Med. 1999, 28, 2265–2276. [Google Scholar]
- Spellberg, B.; Lipsky, B.A. Systemic antibiotic therapy for chronic osteomyelitis in adults. Clin. Infect. Dis. 2012, 54, 393–407. [Google Scholar] [CrossRef]
- Mouton, J.W.; Theuretzbacher, U.; Craig, W.A.; Tulkens, P.M.; Derendorf, H.; Cars, O. Tissue concentrations: Do we ever learn? J. Antimicrob. Chemother. 2008, 61, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic penetration into bone and joints: An updated review. Int. J. Infect. Dis. 2019, 8, 128–136. [Google Scholar] [CrossRef]
- Gomez-Junyent, J.; Rigo-Bonnin, R.; Benavent, E.; Soldevila, L.; Padulles, A.; Cabo, X.; Tubau, F.; Ariza, X.; Murillo, O. Efficacy and therapeutic drug monitoring of continuous beta-lactam infusion for osteo-articular infections caused by fluoroquinolone-resistant Pseudomonas aeruginosa: A prospective cohort study. Eur. J. Drug. Metab. Pharmacokinet. 2020, 45, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Goutelle, S.; Conrad, A.; Pouderoux, C.; Braun, E.; Laurent, F.; Gagnieu, M.C.; Cohen, S.; Guitton, J.; Valour, F.; Ferry, T.; et al. Pharmacokinetic/pharmacodynamic dosage individualization of suppressive beta-lactam therapy administered by subcutaneous route in patients with PJI. Front. Med. 2021, 8, 583086. [Google Scholar]
- Zeller, V.; Lhotellier, L.; Marmor, S.; Leclerc, P.; Krain, A.; Graff, W.; Ducroquet, F.; Biau, D.; Leonard, P.; Desplaces, N.; et al. One-stage exchange arthroplasty for chronic periprosthetic hip infection: Results of a large prospective cohort study. J. Bone Jt. Surg. Am. 2014, 96, e1. [Google Scholar] [CrossRef] [PubMed]
- Davies Forsman, L.; Bruchfeld, J.; Alffenaar, J.C. Therapeutic drug monitoring to prevent acquired drug resistance of fluoroquinolones in the treatment of tuberculosis. Eur. Respir. J. 2017, 49, 1700173. [Google Scholar] [CrossRef]
- Ye, C.; Wang, Z.; Hu, Y.; Deng, C.; Liao, L.; Sun, L.; Wang, C. Systematic review and meta-analysis of the efficacy and safety of vancomycin combined with β-lactam antibiotics in the treatment of methicillin-resistant Staphylococcus aureus bloodstream infections. J. Glob. Antimicrob. Resist. 2020, 23, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Sousa, R.; Pereira, A.; Massada, M.; da Silva, M.V.; Lemos, R.; Costa e Castro, J. Empirical antibiotic therapy in prosthetic joint infections. Acta Orthop. Belg. 2010, 76, 254–259. [Google Scholar]
- Ariza, J.; Cobo, J.; Baraia-Etxaburu, J.; Benito, N.; Bori, G.; Cabo, J.; Corona, P.; Esteban, J.; Horcajada, J.P.; Lora-Tamayo, J.; et al. Executive summary of management of prosthetic joint infections. Clinical practice guidelines by the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC). Enferm. Infecc. Microbiol. Clin. 2017, 35, 189–195. [Google Scholar]
- Recommandations pour la Pratique Clinique. Infections Ostéo-Articulaires sur Matériel (Prothèse, Implant, Ostéosynthèse). SPILF 2008. Available online: www.infectiologie.com (accessed on 29 March 2022).
- Karlsen, Ø.E.; Borgen, P.; Bragnes, B.; Figved, W.; Grøgaard, B.; Rydinge, J.; Sandberg, L.; Snorrason, F.; Wangen, H.; Witsøe, E.; et al. Rifampin combination therapy in staphylococcal prosthetic joint infections: A randomized controlled trial. J. Orthop. Surg. Res. 2020, 15, 365. [Google Scholar] [CrossRef]
- Scheper, H.; Gerritsen, L.M.; Pijls, B.G.; Van Asten, S.A.; Visser, L.G.; De Boer, M.G.J. Outcome of debridement, antibiotics, and implant retention for staphylococcal hip and knee prosthetic joint infections, focused on rifampicin use: A systematic review and meta-analysis. Open Forum Infect. Dis. 2021, 8, ofab298. [Google Scholar] [CrossRef]
- Senneville, E.; Joulie, D.; Legout, L.; Valette, M.; Dezèque, H.; Beltrand, E.; Roselé, B.; d’Escrivan, T.; Loïez, C.; Caillaux, M.; et al. Outcome and predictors of treatment failure in total hip/knee prosthetic joint infections due to Staphylococcus aureus. Clin. Infect. Dis. 2011, 53, 334–340. [Google Scholar] [CrossRef]
- Valour, F.; Karsenty, J.; Bouaziz, A.; Ader, F.; Tod, M.; Lustig, S.; Laurent, F.; Ecochard, R.; Chidiac, C.; Ferry, T.; et al. Antimicrobial-related severe adverse events during treatment of bone and joint infection due to methicillin-susceptible Staphylococcus aureus. Antimicrob. Agents Chemother. 2014, 58, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, N.J.; Rivera, C.G.; Stevens, R.W.; Oravec, C.P.; Mara, K.C.; Suh, G.A.; Osmon, D.R.; Beam, E.N.; Abdel, M.P.; Virk, A. Safety and tolerability of fluoroquinolones in patients with staphylococcal periprosthetic joint infections. Clin. Infect. Dis. 2021, 73, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Xie, X.; Lin, H.; Nie, C. Safety and tolerability of fluoroquinolones for periprosthetic joint infection. Clin. Infect. Dis. 2021, 73, 1126–1127. [Google Scholar] [CrossRef] [PubMed]
- Bernard, A.; Kermarrec, G.; Parize, P.; Caruba, T.; Bouvet, A.; Mainardi, J.L.; Sabatier, B.; Nich, C. Dramatic reduction of clindamycin serum concentration in staphylococcal osteoarticular infection patients treated with the oral clindamycin-rifampicin combination. J. Infect. 2015, 71, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Bonnaire, A.; Vernet-Garnier, V.; Lebrun, D.; Bajolet, O.; Bonnet, M.; Hentzien, M.; Ohl, X.; Diallo, S.; Bani-Sadr, F. Clindamycin combination treatment for the treatment of bone and joint infections caused by clindamycin-susceptible, erythromycin-resistant Staphylococcus spp. Diagn. Microbiol. Infect. Dis. 2021, 99, 115225. [Google Scholar] [CrossRef]
- Le Maréchal, M.; Cavalli, Z.; Batailler, C.; Gonzalez, J.F.; Ferreira, A.; Lustig, S.; Ferry, T.; Courjon, J. Management of prosthetic joint infections in France: A national audit to identify key situations requiring innovation and homogenization. BMC Infect. Dis. 2021, 21, 401. [Google Scholar] [CrossRef]
- Boclé, H.; Lavigne, J.P.; Cellier, N.; Crouzet, J.; Kouyoumdjian, P.; Sotto, A.; Loubet, P. Effectiveness of early switching from intravenous to oral antibiotic therapy in Staphylococcus aureus prosthetic bone and joint or orthopedic metalware-associated infections. BMC Musculoskelet. Disord. 2021, 22, 315. [Google Scholar] [CrossRef]
- Parvizi, J.; Azzam, K.; Ghanem, E.; Austin, M.S.; Rothman, R.H. Periprosthetic infection due to resistant staphylococci: Serious problems on the horizon. Clin. Orthop. Relat. Res. 2009, 467, 1732–1739. [Google Scholar] [CrossRef]
- Guo, G.; Wang, J.; You, Y.; Tan, J.; Shen, H. Distribution characteristics of Staphylococcus spp. in different phases of periprosthetic joint infection: A review. Exp. Ther. Med. 2017, 13, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Bart, G.; Zeller, V.; Kerroumi, Y.; Heym, B.; Meyssonnier, V.; Desplaces, N.; Kitzis, M.D.; Ziza, J.M.; Marmor, S. Minocycline combined with vancomycin for the treatment of methicillin-resistant coagulase-negative staphylococcal prosthetic joint infection managed with exchange arthroplasty. J. Bone Jt. Infect. 2020, 5, 110–117. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pérez-Cardona, P.S.C.; Ojeda, V.B.; Pardo, D.R.; Serrallach, C.P.; Farfán, E.G.; Mateu, C.A.; Sanchez, X.F. Clinical experience with daptomycin for the treatment of patients with knee and hip periprosthetic joint infections. J. Antimicrob. Chemother. 2012, 67, 1749–1754. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chang, Y.J.; Lee, M.S.; Lee, C.H.; Lin, P.C.; Kuo, F.C. Daptomycin treatment in patients with resistant staphylococcal periprosthetic joint infection. BMC Infect. Dis. 2017, 17, 736. [Google Scholar] [CrossRef]
- Telles, J.P.; Cieslinski, J.; Tuon, F.F. Daptomycin to bone and joint infections and prosthesis joint infections: A systematic review. Braz. J. Infect. Dis. 2019, 23, 191–196. [Google Scholar] [CrossRef]
- Deroche, L.; Plouzeau, C.; Bémer, P.; Tandé, D.; Valentin, A.S.; Jolivet-Gougeon, A.; Lemarié, C.; Bret, L.; Kempf, M.; Héry-Arnaud, G.; et al. Probabilistic chemotherapy in knee and hip replacement infection: The place of linezolid. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1659–1663. [Google Scholar] [CrossRef]
- Swaminathan, A.; du Cros, P.; Seddon, J.A.; Mirgayosieva, S.; Asladdin, R.; Dusmatova, Z. Peripheral neuropathy in a diabetic child treated with linezolid for multidrug-resistant tuberculosis: A case report and review of the literature. BMC Infect. Dis. 2017, 17, 417. [Google Scholar] [CrossRef]
- Ramsey, T.D.; Lau, T.T.; Ensom, M.H. Serotonergic and adrenergic drug interactions associated with linezolid: A critical review and practical management approach. Ann. Pharmacother. 2013, 47, 543–560. [Google Scholar] [CrossRef]
- Dempsey, S.P.; Sickman, A.; Slagle, W.S. Case report: Linezolid optic neuropathy and proposed evidenced-based screening recommendation. Optom. Vis. Sci. 2018, 95, 468–474. [Google Scholar] [CrossRef]
- Sawada, M.; Oe, K.; Hirata, M.; Kawamura, H.; Ueda, N.; Nakamura, T.; Iida, H.; Saito, T. Linezolid versus daptomycin treatment for periprosthetic joint infections: A retrospective cohort study. J. Orthop. Surg. Res. 2019, 14, 334. [Google Scholar] [CrossRef]
- Smith, W.J.; Putnam, W.C.; Pass, S.E. An evaluation of tedizolid for the treatment of MRSA infections. Expert Opin. Pharmacother. 2018, 19, 1489–1494. [Google Scholar]
- Senneville, E.; Dinh, A.; Ferry, T.; Beltrand, E.; Blondiaux, N.; Robineau, O. Tolerance of prolonged oral tedizolid for prosthetic joint infections: Results of a multicentre prospective study. Antibiotics 2020, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Matt, M.; Duran, C.; Courjon, J.; Lotte, R.; Moing, V.L.; Monnin, B.; Pavese, P.; Chavanet, P.; Khatchatourian, L.; Tattevin, P.; et al. Dalbavancin treatment for prosthetic joint infections in real-life: A national cohort study and literature review. J. Glob. Antimicrob. Resist. 2021, 25, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Alves-Barroco, C.; Paquete-Ferreira, J.; Santos-Silva, T.; Fernandes, A.R. Singularities of pyogenic streptococcal biofilms—From formation to health implication. Front. Microbiol. 2020, 11, 584947. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Senneville, E.; Ribera, A.; Bernard, L.; Dupon, M.; Zeller, V.; Li, H.K.; Arvieux, C.; Clauss, M.; Uçkay, I.; et al. The not-so-good prognosis of streptococcal periprosthetic joint infection managed by implant retention: The results of a large multicenter study. Clin. Infect. Dis. 2017, 64, 1742–1752. [Google Scholar] [CrossRef]
- Mahieu, R.; Dubée, V.; Seegers, V.; Lemarié, C.; Ansart, S.; Bernard, L.; Le Moal, G.; Asseray, N.; Arvieux, C.; Ramanantsoa, C.; et al. The prognosis of streptococcal prosthetic bone and joint infections depends on surgical management-a multicenter retrospective study. Int. J. Infect. Dis. 2019, 85, 175–181. [Google Scholar] [CrossRef]
- Haute Autorité de Sante; Prothèse de Hanche ou de Genou: Diagnostic et Prise en Charge de L’infection dans le Mois Suivant L’implantation, HAS 2014. Available online: https://www.has-sante.fr/jcms/c_1228574/fr/prothese-de-hanche-ou-de-genou-diagnostic-et-prise-en-charge-de-l-infection-dans-le-mois-suivant-l-implantation (accessed on 29 March 2022).
- Fiaux, E.; Titecat, M.; Robineau, O.; Lora-Tamayo, J.; El Samad, Y.; Etienne, M.; Frebourg, N.; Blondiaux, N.; Brunschweiler, B.; Dujardin, F.; et al. Outcome of patients with streptococcal prosthetic joint infections with special reference to rifampicin combinations. BMC Infect. Dis. 2016, 16, 568. [Google Scholar] [CrossRef]
- Kherabi, Y.; Zeller, V.; Kerroumi, Y.; Meyssonnier, V.; Heym, B.; Lidove, L.; Marmor, S. Streptococcal and Staphylococcus aureus prosthetic joint infections: Are they really different? BMC Infect. Dis. submitted.
- Tornero, E.; Senneville, E.; Euba, G.; Petersdorf, S.; Rodriguez-Pardo, D.; Lakatos, B.; Ferrari, M.C.; Pilares, M.; Bahamonde, A.; Trebse, R.; et al. Characteristics of prosthetic joint infections due to Enterococcus sp. and predictors of failure: A multi-national study. Clin. Microbiol. Infect. 2014, 20, 1219–1224. [Google Scholar] [CrossRef]
- Renz, N.; Trebse, R.; Akgün, D.; Perka, C.; Trampuz, A. Enterococcal periprosthetic joint infection: Clinical and microbiological findings from an 8-year retrospective cohort study. BMC Infect. Dis. 2019, 19, 1083. [Google Scholar] [CrossRef]
- Kheir, M.M.; Tan, T.L.; Higuera, C.; George, J.; Della Valle, C.J.; Shen, M.; Parvizi, J. Periprosthetic joint infections caused by enterococci have poor outcomes. J. Arthroplast. 2017, 32, 933–947. [Google Scholar] [CrossRef] [PubMed]
- El Helou, O.C.; Berbari, E.F.; Marculescu, C.E.; El Atrouni, W.I.; Razonable, R.R.; Steckelberg, J.M.; Hanssen, A.D.; Osmon, D.R. Outcome of enterococcal prosthetic joint infection: Is combination systemic therapy superior to monotherapy? Clin. Infect. Dis. 2008, 47, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Thompson, O.; Rasmussen, M.; Stefánsdóttir, A.; Christensson, B.; Åkesson, P. A population-based study on the treatment and outcome of enterococcal prosthetic joint infections. A consecutive series of 55 cases. J. Bone Jt. Infect. 2019, 4, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.C.; Lau, T.T.Y.; Ensom, M.H.H. Combination of ceftriaxone and ampicillin for the treatment of enterococcal endocarditis: A qualitative systematic review. Ann. Pharmacother. 2017, 51, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Euba, G.; Lora-Tamayo, J.; Murillo, O.; Pedrero, S.; Cabo, J.; Verdaguer, R.; Ariza, J. Pilot study of ampicillin-ceftriaxone combination for treatment of orthopedic infections due to Enterococcus faecalis. Antimicrob. Agents Chemother. 2009, 53, 4305–4310. [Google Scholar] [CrossRef][Green Version]
- Shah, N.B.; Osmon, D.R.; Steckelberg, J.M.; Sierra, R.J.; Walker, R.C.; Tande, A.J.; Berbari, E.F. Pseudomonas prosthetic joint infections: A review of 102 episodes. J. Bone Jt. Infect. 2016, 1, 25–30. [Google Scholar] [CrossRef]
- Cerioli, M.; Batailler, C.; Conrad, A.; Roux, S.; Perpoint, T.; Becker, A.; Triffault-Fillit, C.; Lustig, S.; Fessy, M.H.; Laurent, F.; et al. Pseudomonas aeruginosa implant-associated bone and joint infections: Experience in a Regional Reference Center in France. Front. Med. 2020, 7, 513242. [Google Scholar] [CrossRef]
- Breilh, D.; Boselli, E.; Bel, J.C.; Chassard, D.; Saux, M.C.; Allaouchiche, B. Diffusion of cefepime into cancellous and cortical bone tissue. J. Chemother. 2003, 15, 134–138. [Google Scholar] [CrossRef]
- Moody, J.A.; Fasching, C.E.; Peterson, L.R.; Gerding, D.N. Ceftazidime and amikacin alone and in combination against Pseudomonas aeruginosa and Enterobacteriaceae. Diagn. Microbiol. Infect. Dis. 1987, 6, 59–67. [Google Scholar] [CrossRef]
- Grossi, O.; Asseray, N.; Bourigault, C.; Corvec, S.; Valette, M.; Navas, D.; Happi-Djeukou, L.; Touchais, S.; Bemer, P.; Boutoille, D.; et al. Gram-negative prosthetic joint infections managed according to a multidisciplinary standardized approach: Risk factors for failure and outcome with and without fluoroquinolones. J. Antimicrob. Chemother. 2016, 71, 2593–2597. [Google Scholar] [CrossRef]
- Tice, A.; Hoaglund, P.A.; Shoultz, D.A. Outcomes of osteomyelitis among patients treated with outpatient parenteral antimicrobial therapy. Am. J. Med. 2003, 114, 723–728. [Google Scholar] [CrossRef]
- Deconinck, L.; Dinh, A.; Nich, C.; Tritz, T.; Matt, M.; Senard, O.; Bessis, S.; Bauer, T.; Rottman, M.; Salomon, J.; et al. Efficacy of cotrimoxazole (sulfamethoxazole-trimethoprim) as a salvage therapy for the treatment of bone and joint infections (BJIs). PLoS ONE 2019, 14, e0224106. [Google Scholar] [CrossRef] [PubMed]
- Logan, L.K.; Weinstein, R.A. The epidemiology of carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215 (Suppl. 1), S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Hoeffler, U.; Ko, H.L.; Pulverer, G. Antimicrobial susceptibility of Propionibacterium acnes and related microbial species. Antimicrob. Agents Chemother. 1976, 10, 387–394. [Google Scholar] [CrossRef]
- Achermann, Y.; Goldstein, E.J.; Coenye, T.; Shirtcliff, M.E. Propionibacterium acnes: From commensal to opportunistic biofilm-associated implant pathogen. Clin. Microbiol. Rev. 2014, 27, 419–440. [Google Scholar] [CrossRef]
- SPILF. Recommandations pour la Pratique Clinique. Infections Ostéo-Articulaires sur Matériel (Prothèse, Implant, Ostéosynthèse). 2009. Available online: www.infectiologie.com (accessed on 29 March 2022).
- Piggott, D.A.; Higgins, Y.M.; Melia, M.T.; Ellis, B.; Carroll, K.C.; McFarland, E.G.; Auwaerter, P.G. Characteristics and treatment outcomes of Propionibacterium acnes prosthetic shoulder infections in adults. Open Forum Infect. Dis. 2015, 3, ofv191. [Google Scholar] [CrossRef]
- Renz, N.; Mudrovcic, S.; Perka, C.; Trampuz, A. Orthopedic implant-associated infections caused by Cutibacterium spp.—A remaining diagnostic challenge. PLoS ONE 2018, 13, e0202639. [Google Scholar] [CrossRef]
- Furustrand Tafin, U.; Corvec, S.; Betrisey, B.; Zimmerli, W.; Trampuz, A. Role of rifampin against Propionibacterium acnes biofilm in vitro and in an experimental foreign-body infection model. Antimicrob. Agents Chemother. 2012, 56, 1885–1891. [Google Scholar] [CrossRef]
- Jacobs, A.M.; Van Hooff, M.L.; Meis, J.F.; Vos, F.; Goosen, J.H. Treatment of prosthetic joint infections due to Propionibacterium. Similar results in 60 patients treated with and without rifampicin. Acta Orthop. 2016, 87, 60–66. [Google Scholar] [CrossRef]
- Zeller, V.; Ghorbani, A.; Strady, C.; Leonard, P.; Mamoudy, P.; Desplaces, N. Propionibacterium acnes: An agent of prosthetic joint infection and colonization. J. Infect. 2007, 55, 119–124. [Google Scholar] [CrossRef]
- Corvec, S. Clinical and biological features of Cutibacterium (formerly Propionibacterium) avidum, an unrecognized microorganism. Clin. Microb. Rev. 2018, 31, e00064-17. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Letembet, V.A.; Meyssonnier, V.; Heym, B.; Ziza, J.M.; Marmor, S. Cutibacterium (formerly Propionibacterium) avidum: A rare but avid agent of prosthetic hip infection. J. Arthroplast. 2018, 33, 2246–2250. [Google Scholar] [CrossRef] [PubMed]
- Kalt, F.; Schulthess, B.; Sidler, F.; Herren, S.; Fucentese, S.F.; Zingg, P.O.; Berli, M.; Zinkernagel, A.S.; Zbinden, R.; Achermann, Y. Corynebacterium species rarely cause Orthopedic Infections. J. Clin. Microbiol. 2018, 56, e01200-18. [Google Scholar] [CrossRef] [PubMed]
- Noussair, L.; Salomon, E.; El Sayed, F.; Duran, C.; Bouchand, F.; Roux, A.L.; Gaillard, J.L.; Bauer, T.; Rottman, M.; Dinh, A. Monomicrobial bone and joint infection due to Corynebacterium striatum: Literature review and amoxicillin-rifampin combination as treatment perspective. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Chauvelot, P.; Ferry, T.; Tafani, V.; Diot, A.; Tasse, J.; Conrad, A.; Chidiac, C.; Braun, E.; Lustig, S.; Laurent, F.; et al. Bone and joint infection involving Corynebacterium spp.: From clinical features to pathophysiological pathways. Front. Med. 2021, 7, 539501. [Google Scholar] [CrossRef]
- Schoen, C.; Unzicker, C.; Stuhler, G.; Elias, J.; Einsele, H.; Grigoleit, G.U.; Abele-Horn, M.; Mielke, S. Life-threatening infection caused by daptomycin-resistant Corynebacterium jeikeium in a neutropenic patient. J. Clin. Microbiol. 2009, 47, 2328–2331. [Google Scholar] [CrossRef]
- Yoon, H.K.; Cho, S.H.; Lee, D.Y.; Kang, B.H.; Lee, S.H.; Moon, D.G.; Kim, D.H.; Nam, D.C.; Hwang, S.C. A review of the literature on culture-negative periprosthetic joint infection: Epidemiology, diagnosis and treatment. Knee Surg. Relat. Res. 2017, 29, 155–164. [Google Scholar] [CrossRef]
- Van Sloten, M.; Gómez-Junyent, J.; Ferry, T.; Rossi, N.; Petersdorf, S.; Lange, J.; Corona, P.; Araújo Abreu, M.; Borens, O.; Zlatian, O.; et al. Should all patients with a culture-negative periprosthetic joint infection be treated with antibiotics?: A multicentre observational study. Bone Jt. J. 2022, 104-B, 183–188. [Google Scholar] [CrossRef]
- Ribera, A.; Morata, L.; Moranas, J.; Agullo, J.L.; Martinez, J.C.; Lopez, Y.; Garcia, D.; Cabo, J.; Garcia-Ramiro, S.; Soriano, A.; et al. Clinical and microbiological findings in prosthetic joint replacement due to aseptic loosening. J. Infect. 2014, 69, 235–243. [Google Scholar] [CrossRef]
- Wang, C.; Huang, Z.; Li, W.; Fang, X.; Zhang, W. Can metagenomic next-generation sequencing identify the pathogens responsible for culture-negative prosthetic joint infection? BMC Infect. Dis. 2020, 20, 253. [Google Scholar] [CrossRef]
- Hersh, B.; Shah, N.; Rothenberger, S.D.; Zlotnicki, J.P.; Klatt, B.A.; Urish, K.L. Do culture negative periprosthetic joint infections remain culture negative? J. Arthroplast. 2019, 34, 2757–2762. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Health Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, E.; Parvizi, J.; Clohisy, J.; Burnett, S.; Sharkey, P.F.; Barrack, R. Perioperative antibiotics should not be withheld in proven cases of periprosthetic infection. Clin. Orthop. Relat. Res. 2007, 461, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.S.J.; Aggarwal, A.; Givens, S.A.; McClure, J.T.; Morgan, P.M.; Barrack, R.L. Prophylactic antibiotics do not affect cultures in the treatment of an infected TKA: A prospective trial. Clin. Orthop. Relat. Res. 2010, 468, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Wouthuyzen-Bakker, M.; Benito, N.; Soriano, A. The effect of preoperative antimicrobial prophylaxis on intraoperative culture results in patients with a suspected or confirmed prosthetic joint infection: A systematic review. J. Clin. Microbiol. 2017, 55, 2765–2774. [Google Scholar] [CrossRef] [PubMed]
- Hawn, M.T.; Richman, J.S.; Vick, C.C.; Deierhoi, R.J.; Graham, L.A.; Henderson, W.G.; Itani, K.M. Timing of surgical antibiotic prophylaxis and the risk of surgical site infection. JAMA Surg. 2013, 148, 649–657. [Google Scholar] [CrossRef]
- Siddiqi, A.; Forte, S.A.; Docter, S.; Bryant, D.; Sheth, N.P.; Chen, A.F. Perioperative antibiotic prophylaxis in total joint arthroplasty: A systematic review and meta-analysis. J. Bone Jt. Surg. Am. 2019, 101, 828–842. [Google Scholar] [CrossRef]
- Béal, C.; Zeller, V.; Kerroumi, Y.; Meyssonnier, V.; Heym, B.; Chazerain, P.; Marmor, S. Successive new-pathogen prosthetic joint reinfections: Observational cohort study on 61 patients. Jt. Bone Spine 2022, 89, 105254. [Google Scholar] [CrossRef]
- Ferry, T.; Kolenda, C.; Batailler, C.; Gustave, C.A.; Lustig, S.; Malatray, M.; Fevre, C.; Josse, J.; Petitjean, C.; Chidiac, C.; et al. Phage therapy as adjuvant to conservative surgery and antibiotics to salvage patients with relapsing S. aureus prosthetic knee infection. Front. Med. 2020, 7, 570572. [Google Scholar] [CrossRef]
- Ferry, T.; Kolenda, C.; Batailler, C.; Gaillard, G.; Gustave, C.A.; Lustig, S.; Fevre, C.; Petitjean, C.; Leboucher, G.; Laurent, F.; et al. Case report: Arthroscopic “Debridement antibiotics and implant retention with local injection of personalized phage therapy to salvage a relapsing P. aeruginosa prosthetic knee infection. Front. Med. 2021, 8, 569159. [Google Scholar] [CrossRef]
- Qin, S.; Xu, K.; Nie, B.; Ji, F.; Zhang, H. Approaches based on passive and active antibacterial coating on titanium to achieve antibacterial activitiy. J. Biomed. Mater. Res. A 2018, 106, 2531–2539. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intravenous Antibiotic Therapy | Oral Antibiotic Therapy | |
|---|---|---|
| Indications | Initial PJI treatment Use of drugs not orally available Treatment of resistant or difficult to treat microorganism | Oral switch after initial IV therapy Suppressive antibiotic therapy |
| Advantages | Allows use of high drug dosages PK/PD optimization (extended or continuous infusion) 100% bioavailability (avoids nonobservance, malabsorption and hepatic first-pass effect) Better gastro-intestinal tolerance Better monitoring during hospitalization or outpatient parenteral antibiotic therapy | No venous access No risk of catheter-related complication Better rehabilitation and mobility |
| Risks Disadvantages | Venous catheter-related complications (infection, thrombosis,…) Reduced mobility Longer hospital stay | Lower bioavailability due to drug-specific absorption and hepatic first effect Frequent gastro-intestinal intolerance Possible non observance More parameters that can vary antibiotic serum concentrations |
| Microorganism | Initial IV therapy | Oral switch |
|---|---|---|
| Methicillin-susceptible Staphylococcus | Cefazolin or oxacillin + rifampicin | Levofloxacin + rifampicin |
| Methicillin-resistant Staphylococcus | Vancomycin or daptomycin + another drug depending on the strains’ susceptibility (rifampicin or minocycline or linezolide) | No oral switch |
| C. acnes | Amoxicillin or clindamycin (check clindamycin susceptibility) | Amoxicillin or clindamycin |
| Streptococcus | Amoxicillin | Amoxicillin |
| Enterococcus faecalis | Amoxicillin ± initial gentamicin | Amoxicillin |
| Corynebacterium | Susceptible strain: amoxicillin Resistant strain: vancomycin ± rifampicin | Susceptible strain: amoxicillin |
| Enterobacteriaceae | Ceftriaxone or cefotaxime | Ciprofloxacin or levofloxacin |
| Pseudomonas aeruginosa (ciprofloxacin susceptible strain) | Ceftazidime or cefepime + initial amikacine followed by ceftazidime or cefepime + oral ciprofloxacin At least 3 weeks | Ciprofloxacin |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Vavasseur, B.; Zeller, V. Antibiotic Therapy for Prosthetic Joint Infections: An Overview. Antibiotics 2022, 11, 486. https://doi.org/10.3390/antibiotics11040486
Le Vavasseur B, Zeller V. Antibiotic Therapy for Prosthetic Joint Infections: An Overview. Antibiotics. 2022; 11(4):486. https://doi.org/10.3390/antibiotics11040486
Chicago/Turabian StyleLe Vavasseur, Benjamin, and Valérie Zeller. 2022. "Antibiotic Therapy for Prosthetic Joint Infections: An Overview" Antibiotics 11, no. 4: 486. https://doi.org/10.3390/antibiotics11040486
APA StyleLe Vavasseur, B., & Zeller, V. (2022). Antibiotic Therapy for Prosthetic Joint Infections: An Overview. Antibiotics, 11(4), 486. https://doi.org/10.3390/antibiotics11040486