
Predictive Scores for Late-Onset Neonatal Sepsis as an Early Diagnostic and Antimicrobial Stewardship Tool: What Have We Done So Far?

 ,
,
Abstract
1. Introduction
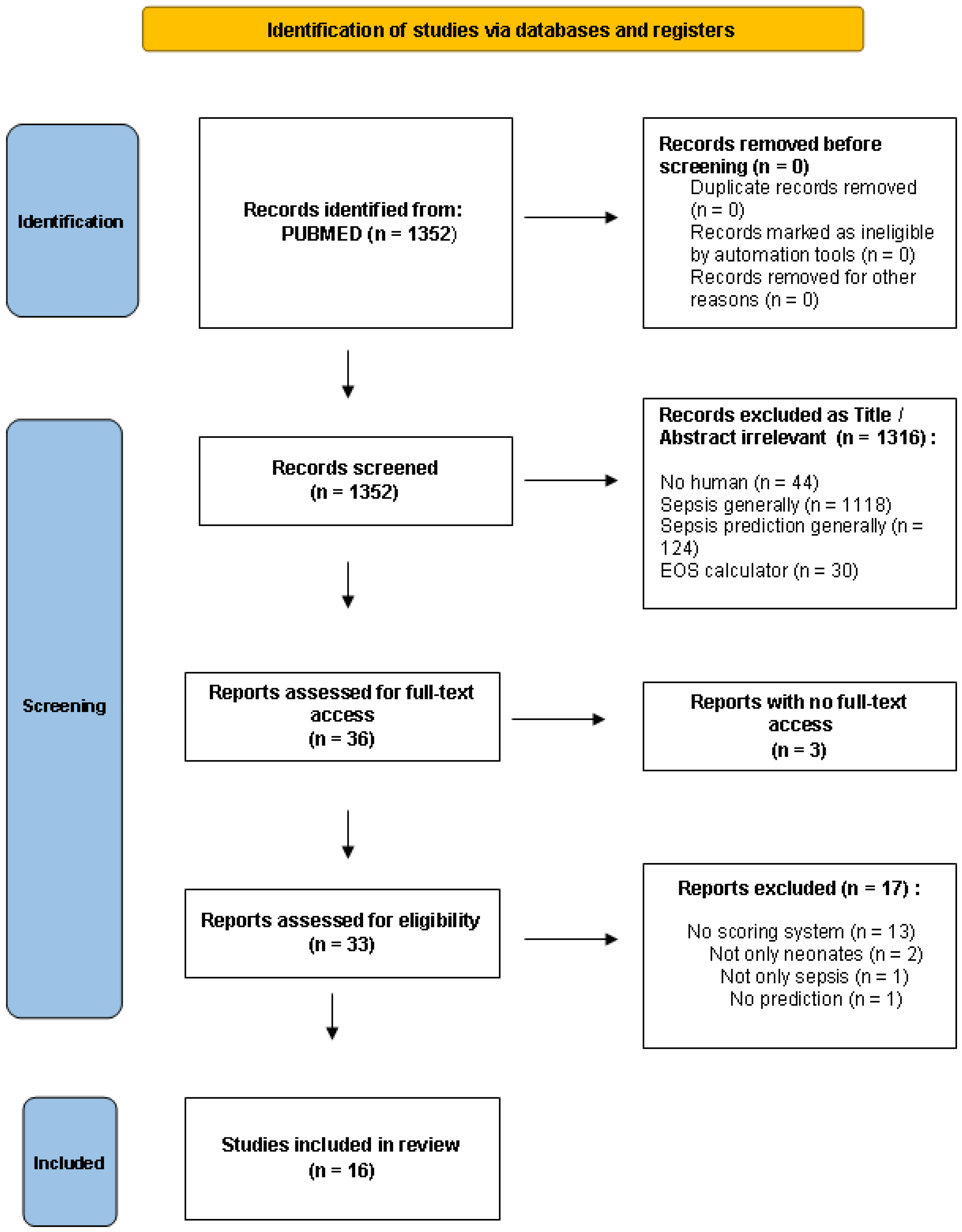
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Inclusion and Eligibility Criteria
2.4. Selection Process
3. Results
- Clinical
- Laboratory
- Clinical and laboratory
- Risk factors
- Clinical, laboratory and risk factors
- Clinical, laboratory and management
3.1. Scores with Clinical Variables
3.2. Scores with Laboratory Variables
3.3. Scores with Clinical and Laboratory Variables
3.4. Scores Based on Risk Factors
3.5. Scores Based on Clinical, Laboratory and Risk Factors
3.6. Clinical, Laboratory and Management
4. Discussion
4.1. Predictive Scores: Clinical vs. Laboratory Parameters
4.2. Prematurity and Low Birth Weight (LBW) Infants
4.3. Clinical and Laboratory Parameters of High Diagnostic Value
4.4. New Diagnostic Techniques
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANC | Absolute neutrophil count |
| BC | Blood culture |
| BW | Birth weight |
| CRP | C-reactive protein |
| CSF | Cerebrospinal fluid |
| CVC | Central venous catheter |
| EOS | Early-onset neonatal sepsis |
| GA | Gestational age |
| HABSI | Healthcare-associated bloodstream infection |
| HR | Heart rate |
| HRC | Heart rate characteristics |
| HSS | Hematologic scoring system |
| I:M ratio | Immature to mature neutrophil ratio |
| I:T ratio | Immature to total neutrophil ratio |
| LAT | Latex agglutination test |
| LBW | Low birth weight |
| LOS | Late-onset neonatal sepsis |
| mESR | Micro erythrocyte sedimentation rate |
| ML | Machine learning |
| NBW | Normal birth weight |
| NICU | Neonatal Intensive Care Unit |
| NLR | Negative likelihood ratio |
| NOSEP score | Nosocomial Sepsis Predictive Score |
| NPV | Negative predictive value |
| NS | Neonatal sepsis |
| PLR | Positive likelihood ratio |
| PLT | Platelet |
| PMN | Polymorphonuclear |
| PPV | Positive predictive value |
| Se | Sensitivity |
| Sp | Specificity |
| TPN | Total parenteral nutrition |
| UAC | Umbilical artery catheter |
| UVC | Umbilical vein catheter |
| VLBW | Very low birth weight |
| WBC | White blood cell |
References
- Wynn, J.L.; Wong, H.R.; Shanley, T.P.; Bizzarro, M.J.; Saiman, L.; Polin, R.A. Time for a Neonatal-Specific Consensus Definition for Sepsis. Pediatr. Crit. Care Med. 2014, 15, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Helmbrecht, A.R.; Marfurt, S.; Chaaban, H. Systematic Review of the Effectiveness of the Neonatal Early-Onset Sepsis Calculator. J. Périnat. Neonatal. Nurs. 2019, 33, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- Wang, H.; Liddell, C.A.; Coates, M.M.; Mooney, M.D.; Levitz, C.E.; Schumacher, A.E.; Apfel, H.; Iannarone, M.; Phillips, B.; Lofgren, K.T.; et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 957–979. [Google Scholar] [CrossRef]
- Jernberg, C.; Löfmark, S.; Edlund, C.; Jansson, J.K. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology 2010, 156, 3216–3223. [Google Scholar] [CrossRef]
- Cotten, C.M.; Taylor, S.; Stoll, B.; Goldberg, R.N.; Hansen, N.I.; Sánchez, P.J.; Ambalavanan, N.; Benjamin, D.K., Jr. Prolonged Duration of Initial Empirical Antibiotic Treatment Is Associated With Increased Rates of Necrotizing Enterocolitis and Death for Extremely Low Birth Weight Infants. Pediatrics 2009, 123, 58–66. [Google Scholar] [CrossRef]
- Hill, D.; Hoffmann, C.; Abt, M.C.; Du, Y.; Kobuley, D.; Kirn, T.J.; Bushman, F.D.; Artis, D. Metagenomic analyses reveal antibiotic-induced temporal and spatial changes in intestinal microbiota with associated alterations in immune cell homeostasis. Mucosal Immunol. 2009, 3, 148–158. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.-A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2015, 387, 168–175. [Google Scholar] [CrossRef]
- Neonatal bacteraemia: Diagnosis and management. BMJ 1979, 2, 1385–1386. [CrossRef][Green Version]
- Tam, P.-Y.I.; Bendel, C. Diagnostics for neonatal sepsis: Current approaches and future directions. Pediatr. Res. 2017, 82, 574–583. [Google Scholar] [CrossRef]
- Fanaroff, A.A.; Korones, S.B.; Wright, L.L.; Verter, J.; Poland, R.L.; Bauer, C.R.; Tyson, J.E.; Philips, J.B.; Edwards, W.; Lucey, J.F.; et al. Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. Pediatr. Infect. Dis. J. 1998, 17, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Mathur, N.; Saxena, L.; Sarkar, R.; Puri, R. Superiority of acridine orange-stained buffy coat smears for diagnosis of partially treated neonatal septicemia. Acta Paediatr. 1993, 82, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Xanthou, M. Leucocyte Blood Picture in Healthy Full-term and Premature Babies During Neonatal Period. Arch. Dis. Child. 1970, 45, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Verstraete, E.H.; Blot, K.; Mahieu, L.; Vogelaers, D.; Blot, S. Prediction Models for Neonatal Health Care–Associated Sepsis: A Meta-analysis. Pediatrics 2015, 135, e1002–e1014. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, M.; Flores, A.; Luna, R.A.; Versalovic, J. Molecular microbiological methods in the diagnosis of neonatal sepsis. Expert Rev. Anti-Infect. Ther. 2010, 8, 1037–1048. [Google Scholar] [CrossRef]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Hornik, C.P.; Fort, P.; Clark, R.H.; Watt, K.; Benjamin, D.K., Jr.; Smith, P.B.; Manzoni, P.; Jacqz-Aigrain, E.; Kaguelidou, F.; Cohen-Wolkowiez, M. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum. Dev. 2012, 88, S69–S74. [Google Scholar] [CrossRef]
- Shah, B.A.; Padbury, J.F. Neonatal sepsis. Virulence 2013, 5, 170–178. [Google Scholar] [CrossRef]
- Ng, P.C.; Lam, H. Biomarkers in Neonatology: The Next Generation of Tests. Neonatology 2012, 102, 145–151. [Google Scholar] [CrossRef]
- Sharma, D.; Farahbakhsh, N.; Shastri, S.; Sharma, P. Biomarkers for diagnosis of neonatal sepsis: A literature review. J. Matern. Neonatal Med. 2017, 31, 1646–1659. [Google Scholar] [CrossRef]
- Tzialla, C.; Achille, C.; Bollani, L.; Stronati, M.; Borghesi, A.; Manzoni, P. New Diagnostic Possibilities for Neonatal Sepsis. Am. J. Perinatol. 2018, 35, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, L.; Harris, M.C. New technologies for the rapid diagnosis of neonatal sepsis. Curr. Opin. Pediatr. 2012, 24, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Rodwell, R.L.; Leslie, A.L.; Tudehope, D.I. Early diagnosis of neonatal sepsis using a hematologic scoring system. J. Pediatr. 1988, 112, 761–767. [Google Scholar] [CrossRef]
- Töllner, U. Early diagnosis of septicemia in the newborn. Eur. J. Pediatr. 1982, 138, 331–337. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Singh, S.A.; Dutta, S.; Narang, A. Predictive clinical scores for diagnosis of late onset neonatal septicemia. J. Trop. Pediatr. 2003, 49, 235–239. [Google Scholar] [CrossRef][Green Version]
- Dalgic, N.; Ergenekon, E.; Koc, E.; Atalay, Y. NOSEP and Clinical Scores for Nosocomial Sepsis in a Neonatal Intensive Care Unit. J. Trop. Pediatr. 2005, 52, 226–227. [Google Scholar] [CrossRef]
- Kudawla, M.; Dutta, S.; Narang, A. Validation of a Clinical Score for the Diagnosis of Late Onset Neonatal Septicemia in Babies Weighing 1000-2500 g. J. Trop. Pediatr. 2007, 54, 66–69. [Google Scholar] [CrossRef]
- Rosenberg, R.E.; Ahmed, A.N.U.; Saha, S.K.; Chowdhury, M.A.; Ahmed, S.; Law, P.A.; Black, R.E.; Santosham, M.; Darmstadt, G.L. Nosocomial Sepsis Risk Score for Preterm Infants in Low-resource Settings. J. Trop. Pediatr. 2009, 56, 82–89. [Google Scholar] [CrossRef]
- Narasimha, A.; Kumar, M.L.H. Significance of Hematological Scoring System (HSS) in Early Diagnosis of Neonatal Sepsis. Indian J. Hematol. Blood Transfus. 2011, 27, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Makkar, M.; Pathak, R.; Garg, S.; Gupta, C.; Mahajan, N.C. Performance evaluation of hematologic scoring system in early diagnosis of neonatal sepsis. J. Clin. Neonatol. 2013, 2, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.P.; Lake, D.E.; O’Shea, T.M.; Moorman, J.R. Heart Rate Characteristics and Clinical Signs in Neonatal Sepsis. Pediatr. Res. 2007, 61, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Husada, D.; Chanthavanich, P.; Chotigeat, U.; Sunttarattiwong, P.; Sirivichayakul, C.; Pengsaa, K.; Chokejindachai, W.; Kaewkungwal, J. Predictive model for bacterial late-onset neonatal sepsis in a tertiary care hospital in Thailand. BMC Infect. Dis. 2020, 20, 151. [Google Scholar] [CrossRef]
- Mahieu, L.M.; De Muynck, A.O.; De Dooy, J.J.; Laroche, S.M.; Van Acker, K.J. Prediction of nosocomial sepsis in neonates by means of a computer-weighted bedside scoring system (NOSEP score). Crit. Care Med. 2000, 28, 2026–2033. [Google Scholar] [CrossRef]
- Mahieu, L.M.; De Dooy, J.J.; Cossey, V.R.; Goossens, L.L.; Vrancken, S.L.; Jespers, A.Y.; Vandeputte, C.T.; De Muynck, A.O. Internal and external validation of the NOSEP prediction score for nosocomial sepsis in neonates*. Crit. Care Med. 2002, 30, 1459–1466. [Google Scholar] [CrossRef]
- Okascharoen, C.; Sirinavin, S.; Thakkinstian, A.; Kitayaporn, D.; Supapanachart, S. A Bedside Prediction-Scoring Model for Late-Onset Neonatal Sepsis. J. Perinatol. 2005, 25, 778–783. [Google Scholar] [CrossRef]
- Okascharoen, C.; Hui, C.; Cairnie, J.; Morris, A.M.; Kirpalani, H. External validation of bedside prediction score for diagnosis of late-onset neonatal sepsis. J. Perinatol. 2007, 27, 496–501. [Google Scholar] [CrossRef][Green Version]
- Singh, M.; Narang, A.; Bhakoo, O.N. Predictive Perinatal Score in the Diagnosis of Neonatal Sepsis. J. Trop. Pediatr. 1994, 40, 365–368. [Google Scholar] [CrossRef]
- Reilly, B.M.; Evans, A.T. Translating Clinical Research into Clinical Practice: Impact of Using Prediction Rules To Make Decisions. Ann. Intern. Med. 2006, 144, 201–209. [Google Scholar] [CrossRef]
- McGinn, T.G.; Guyatt, G.H.; Wyer, P.C.; Naylor, C.D.; Stiell, I.G.; Richardson, W.S.; Evidence-Based Medicine Working Group. Users’ Guides to the Medical Literature: XXII. JAMA 2000, 284, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Neal, S.R.; Musorowegomo, D.; Gannon, H.; Borja, M.C.; Heys, M.; Chimhini, G.; Fitzgerald, F. Clinical prediction models to diagnose neonatal sepsis: A scoping review protocol. BMJ Open 2020, 10, e039712. [Google Scholar] [CrossRef] [PubMed]
- Helguera-Repetto, A.C.; Soto-Ramírez, M.D.; Villavicencio-Carrisoza, O.; Yong-Mendoza, S.; Yong-Mendoza, A.; León-Juárez, M.; González-Y-Merchand, J.A.; Zaga-Clavellina, V.; Irles, C. Neonatal Sepsis Diagnosis Decision-Making Based on Artificial Neural Networks. Front. Pediatr. 2020, 8, 525. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Jung, S.Y.; Baek, H.; Choi, C.W.; Jung, Y.H.; Yoo, S. A Predictive Model Based on Machine Learning for the Early Detection of Late-Onset Neonatal Sepsis: Development and Observational Study. JMIR Med. Inform. 2020, 8, e15965. [Google Scholar] [CrossRef]
- Stanculescu, I.; Williams, C.K.I.; Freer, Y. Autoregressive Hidden Markov Models for the Early Detection of Neonatal Sepsis. IEEE J. Biomed. Health Inform. 2013, 18, 1560–1570. [Google Scholar] [CrossRef]
- Mani, S.; Ozdas, A.; Aliferis, C.; Varol, H.A.; Chen, Q.; Carnevale, R.; Chen, Y.; Romano-Keeler, J.; Nian, H.; Weitkamp, J.-H. Medical decision support using machine learning for early detection of late-onset neonatal sepsis. J. Am. Med. Inform. Assoc. 2014, 21, 326–336. [Google Scholar] [CrossRef]
- Masino, A.J.; Harris, M.C.; Forsyth, D.; Ostapenko, S.; Srinivasan, L.; Bonafide, C.; Balamuth, F.; Schmatz, M.; Grundmeier, R.W. Machine learning models for early sepsis recognition in the neonatal intensive care unit using readily available electronic health record data. PLoS ONE 2019, 14, e0212665. [Google Scholar] [CrossRef]
- Thakur, J.; Pahuja, S.K.; Pahuja, R. Performance Comparison of Systemic Inflammatory Response Syndrome with Logistic Regression Models to Predict Sepsis in Neonates. Children 2017, 4, 111. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Country, Year | Method | Design | Population | Scoring System (Points) | Main Findings |
|---|---|---|---|---|---|---|
| [27] | India, 2003 | Prospective | Original | 80 neonates: 105 episodes (30 definite, 17 probable sepsis and 58 no sepsis) 91% preterm, 93% LBW |
| Score different in septic and no septic infants. Most prevalent signs in septic babies: apnea, lethargy, tachycardia. Most specific signs in septic babies: grunting, hypothermia, chest retractions. |
| [28] | Turkey, 2005 | Retrospective | Original and external validation (comparison with NOSEP score of Mahieu et al.) | 102 neonates: 132 episodes (51 blood culture (+), 51 no sepsis) |
| Score different in septic and no septic infants. Feeding intolerance and higher I:T ratio as significant predictors of NS. |
| [29] | India, 2008 | Prospective | Validation (of Singh et al.) | 202 neonates: 220 episodes (60 definite sepsis) Weight: 1000–2500 g |
| The most frequent signs in septic infants: lethargy, apnea and pre feeds aspirates. All clinical signs decreased in frequency from 0 h to 24 h. Different score at 0 h and at 24 h: Se better at 0 h (all sick neonates included), Sp, PPV, NPV better at 24 h. Better prediction of NS at 24 h (PPV↑ at 24 h). Score combined with sepsis screen: ↑Se, NPV but ↓Sp, PPV |
| [30] | Bangladesh, 2010 | Retrospective | Validation (of Singh et al.) and original | 160 neonates: 193 episodes (105 culture (+) in 98 neonates, 88 culture (−) in 79 neonates)GA ≤ 33 weeks (very preterm), ≤72 h admitted to hospital |
| First bedside clinical score for very premature neonates in a low-resource setting. This external validation performed significantly lower Sensitivity than the original study. As the number of sings presented within 48 h of sepsis evaluation was increased, Se and NPV were reduced, while Sp and PPV were augmented. Sensitivity reducing when more than 1 signs were present. |
| Reference | Country, Year | Method | Design | Population | Scoring System (Points) | Main Findings |
|---|---|---|---|---|---|---|
| [23] | Australia, 1988 | Prospective | Original (HSS) | 287 neonates: 298 episodes (27 sepsis, 23 probable infection, 248 non infected) Group 1: 243 neonates (≤24 h of age) Subgroup 1: 113 neonates (preterm) Subgroup 2: 130 neonates (term) Group 2: 55 neonates (days 2–30) Age 1–30 days (EOS and LOS), with perinatal risk factors or clinical suspicion of sepsis |
| Sepsis more common in preterm than in term neonates. I:T ratio, abnormal PMN count and I:M ratio: the most frequent lab findings. Most specific sings: PLTs, degenerative changes. The higher the score, the greater the probability of NS. Cut-off score performed better than the most accurate hematologic variable (I:T ratio). HSS provides an objective assessment. Many factors can affect hematologic response. Importance in combining lab + clinical data. Emphasis on EOS rather than LOS. Suggested as a screening test for diagnosing NS. |
| [31] | India, 2011 | Prospective | Validation of HSS (by Rodwell et al.) | 50 neonates: 50 episodes (12 sepsis, 26 probable infections, 12 no sepsis) Aged 24 h–8 days (EOS and LOS), 58% term and 42% preterm, with perinatal risk factors or clinical suspicion of sepsis. |
| Total PMN count and immature PMN count: the most sensitive signs in sepsis. Total WBC count, I:T ratio and PLT count: the most specific findings in sepsis. Best PPV: I:T ratio and PLT count. I:T ratio and degenerative changes: the most reliable variables. The higher the score, the greater the probability of NS. Suggested as a screening test for diagnosing NS. |
| [32] | India, 2013 | Prospective | Validation of HSS (by Rodwell et al.) | 110 neonates: 110 episodes (42 sepsis, 22 probable infection, 46 normal) Age birth-1 week (EOS and LOS), 57% preterm and 43% term, with perinatal risk factors or clinical suspicion of sepsis |
| Immature PMN: the most sensitive variable. I:M ratio: the most specific and the most predictive sign. I:T ratio: the most reliable indicator of sepsis. HSS more sensitive, specific and predictive in preterm than in term neonates. The higher the score, the higher the likelihood of NS. Emphasis on preterm (57%) than in term. Suggested as screening test for diagnosing NS. |
| Reference | Country, Year | Method | Design | Population | Scoring System (Points) | Main Findings |
|---|---|---|---|---|---|---|
| [24] | Germany, 1982 | Retrospective and prospective | Original | 403 neonates: Retrospective: 83 with sepsis Prospective: 39 with sepsis, 42 with amniotic infection, 28 with post-asphyxia syndrome, 28 premature with cerebral hemorrhage, 183 controls |
| Analysis was divided into 3 phases: onset, at the beginning and at the peak of the illness. Each phase gave different results: as the illness evolved, the scores got higher. Changes in skin coloration: the most frequent sign of NS. Septic neonates performed high scores (47% at the beginning of the illness and 92% in seriously ill infants), in contrast with non-septic neonates. |
| [33] | USA, 2007 | Prospective | Original | 337 neonates: 76 episodes of proven sepsis (blood culture (+) in 63 neonates, 80 episodes of clinical sepsis (blood culture (–) in 63 neonates Age ≥ 7 days old and ≥ 7 days of HRC monitoring Out of 337 neonates: 172 were < 1500 g (VLBW) |
| Hyperglycemia and abnormal WBC count: highly associated with NS only the time of the blood culture. Hypotonia and lethargy: great association with NS only the time preceding the blood culture. Infants with sepsis had higher scores than controls. Hypotension in only 3% of infants with NS (not included in the score). HRC index and clinical score were predictive for NS in the next 24 h. Clinical tests less useful before the NS, because signs and symptoms are present less often. Infants with clinical or proven sepsis: higher scores than controls. Feeding intolerance: the most predictive clinical sign of NS. Feeding intolerance, hypotonia, lethargy and abnormal I:T ratio: the most predictive findings. I:T ratio the most robust independent predictor. Increase in the score in the 24 h before the clinical diagnosis HRC index adjunctive to clinical information proved useful. |
| [34] | Thailand, 2020 | Retrospective | Original | 208 neonates: 52 sepsis (only proven bacterial LOS), 156 controls Aged ≥ 7 days |
| Duration of hospitalization, intracranial hemorrhage, high-risk pregnancies and resuscitation: the most powerful risk factors. Abnormal temperature and abnormal HR: the most common sings in NS. Abnormal HRC occurred early in the course of the illness. Abnormalities were found 12–24 h before the clinical diagnosis of NS. No infant with hypothermia had LOS. Antibiotic therapy to be guided according to the score. |
| [35] | Belgium, 2000 | Prospective and retrospective | Original (NOSEP score) | 119 neonates: 154 episodes: Derivation cohort: 104 episodes of presumed NS in 80 neonates (43 proven sepsis)Validation cohort: 50 episodes of proven NS in 39 neonates >48 h in NICU | NOSEP-1 score:
| Score for nosocomial NS. BW, GA, presence of CVC, prolonged hospital stay and exposure to TPN (especially lipid emulsions) > 14 days: strongly associated with NS. TPN as the only independently associated factor. Fever and neutrophil fraction as powerful signs for prediction. Adding catheter cultures improves the diagnostic power of the score. NOSEP score as accurate as a continuous computerized scoring system. Only 2 variables do not rely on lab results. Waiting for the results for assessment. |
| [36] | Belgium, 2002 | Prospective | Validation of NOSEP score (by Mahieu et al.) and new score | 128 neonates: 155 episodes:Internal validation: 62 episodes of presumed NS in 49 neonates (20 proven NS) External validation: 93 episodes of presumed NS in 79 neonates (51 proven NS) >48 h in NICU | NOSEP-1 score:
NOSEP-NEW-I:
| Score for nosocomial NS. External validation was set in multiple NICUs. Score was higher in septic neonates in both internal and external validations. Internal validation was better than the external. Score suggested as a tool for detection of NS and for reduction of unnecessary use of antibiotics in NICUs. |
| [37] | Thailand, 2005 | Retrospective | Original | 173 neonates: Derivation phase: 100 neonates (17 NS), 40% premature and 18% LBW Validation phase: 73 neonates (25 NS), 69% premature and 49% LBW Hospitalized for >72 h after birth |
| First bedside score for neonates hospitalized > 72 h. Hypotension and abnormal body temperature had the strongest association with NS. Risk variables: LBW, prematurity and TPN: no significant association with LOS, while UVC usage independently associated. Combination of clinical, laboratory and management variables: suspicion of LOS without waiting for the lab results. Score based mostly on clinical sings. Risk groups: stratification of risk for LOS (low, intermediate, high risk) and benefit for decision-making. |
| [38] | Canada, 2007 | Prospective | Validation (of Okascharoen et al.) | 105 neonates: 35 NS Aged 2–90 days >48 h in NICU |
| No significant difference in GA, BW, utilization of CVC and duration of TPN between septic and non septic children. Only utilization of UVC proved to make a difference. External validation performed similar accuracy with the internal validation. From low to intermediate risk: Se, Sp ↓ Clinicians predict LOS as strongly as the scoring system, but tend to overestimate the possibility of LOS: score performed better in prediction comparing to clinicians viewpoint. When the neonatal population consists only of proven LOS records, NS was underestimated, while when suspected LOS episodes are present, LOS tended to be overestimated. |
| Reference | Model Application/Cut-Off Score | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|---|
| [39] | ≥1 for definite sepsis | 87 | 29 | 38 | 85 |
| ≥1 for definite +/or probable sepsis | 81 | 29 | 48 | 65 | |
| [28] | NOSEP score (8–24) | 64 | 58 | 45 | 75 |
| Clinical score (6–12) | 56 | 71 | 86 | 33 | |
| [29] | ≥1 | ||||
| 0 h | 90 | 22.5 | 30.3 | 85.7 | |
| 24 h | 75 | 60.6 | 41.7 | 86.6 | |
| (+) screen and/or 0 h | 95 | 18.1 | 30.3 | 90.6 | |
| [30] | Singh et al. score | 56.6 | 52.1 | 78.1 | 28.4 |
| Score: 1 | 77.1 | 50 | 64.9 | 64.7 | |
| [23] | ≥3 for sepsis | 96 | 78 | 31 | 99 |
| ≥3 for sepsis or probable infection | 98 | - | 58 | - | |
| [31] | ≤2: sepsis is unlikely 3–4 sepsis is possible ≥5 sepsis or infection is very likely | - | - | - | - |
| [32] | ≤2: sepsis is unlikely 3–4 sepsis is possible ≥5 sepsis or infection is very likely | - | - | - | - |
| [24] | <4,5: sepsis is excluded with high probability 5–10: probable infection that leads to sepsis >10: sepsis is certain | - | - | - | - |
| [33] | - | - | - | - | |
| [34] | 2 | 88.5 | 90.4 | 75.4 | 95.9 |
| 3 | 82.7 | 93.6 | 81.1 | 94.2 | |
| [39] | ≥1 for LBW ≥4 for NBW | - | - | - | - |
| [35] | NOSEP ≥ 8 | 95 | 43 | 54 | 93 |
| [36] | NOSEP | 73 | 57 | 67 | 63 |
| NOSEP-NEW-I | 84 | 42 | 64 | 69 | |
| NOSEP-NEW-II | 82 | 67 | 75 | 76 | |
| [37] | Validation set: 4 | 92 | 56 | 56 | 90 |
| [38] | 3 | 97 | 39 | 43 | 96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sofouli, G.A.; Kanellopoulou, A.; Vervenioti, A.; Dimitriou, G.; Gkentzi, D. Predictive Scores for Late-Onset Neonatal Sepsis as an Early Diagnostic and Antimicrobial Stewardship Tool: What Have We Done So Far? Antibiotics 2022, 11, 928. https://doi.org/10.3390/antibiotics11070928
Sofouli GA, Kanellopoulou A, Vervenioti A, Dimitriou G, Gkentzi D. Predictive Scores for Late-Onset Neonatal Sepsis as an Early Diagnostic and Antimicrobial Stewardship Tool: What Have We Done So Far? Antibiotics. 2022; 11(7):928. https://doi.org/10.3390/antibiotics11070928
Chicago/Turabian StyleSofouli, Georgia Anna, Aimilia Kanellopoulou, Aggeliki Vervenioti, Gabriel Dimitriou, and Despoina Gkentzi. 2022. "Predictive Scores for Late-Onset Neonatal Sepsis as an Early Diagnostic and Antimicrobial Stewardship Tool: What Have We Done So Far?" Antibiotics 11, no. 7: 928. https://doi.org/10.3390/antibiotics11070928
APA StyleSofouli, G. A., Kanellopoulou, A., Vervenioti, A., Dimitriou, G., & Gkentzi, D. (2022). Predictive Scores for Late-Onset Neonatal Sepsis as an Early Diagnostic and Antimicrobial Stewardship Tool: What Have We Done So Far? Antibiotics, 11(7), 928. https://doi.org/10.3390/antibiotics11070928