

Development of a Predictive Dosing Nomogram to Achieve PK/PD Targets of Amikacin Initial Dose in Critically Ill Patients: A Non-Parametric Approach
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
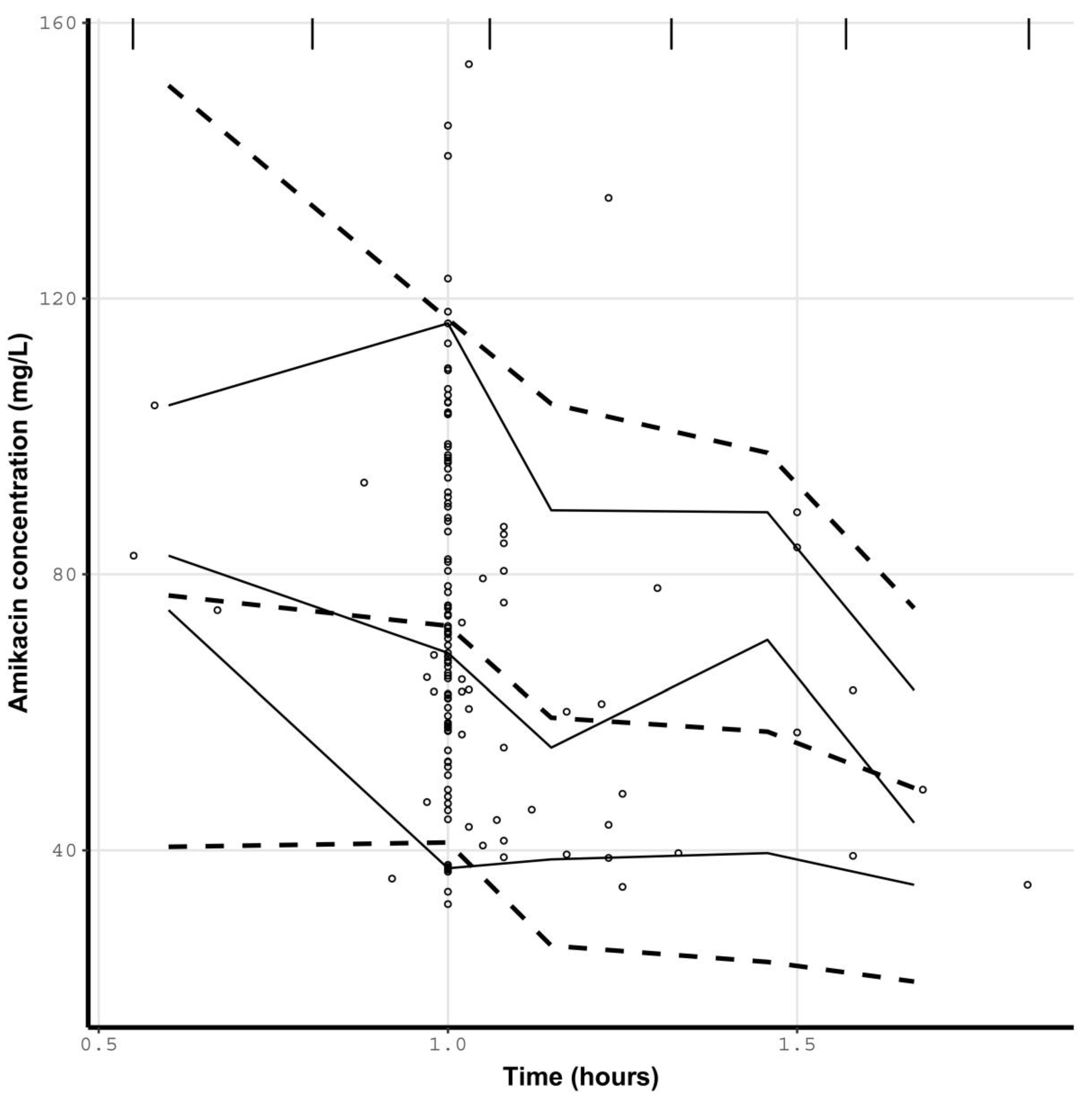
2.1. Patients’ Characteristics and Amikacin Concentrations
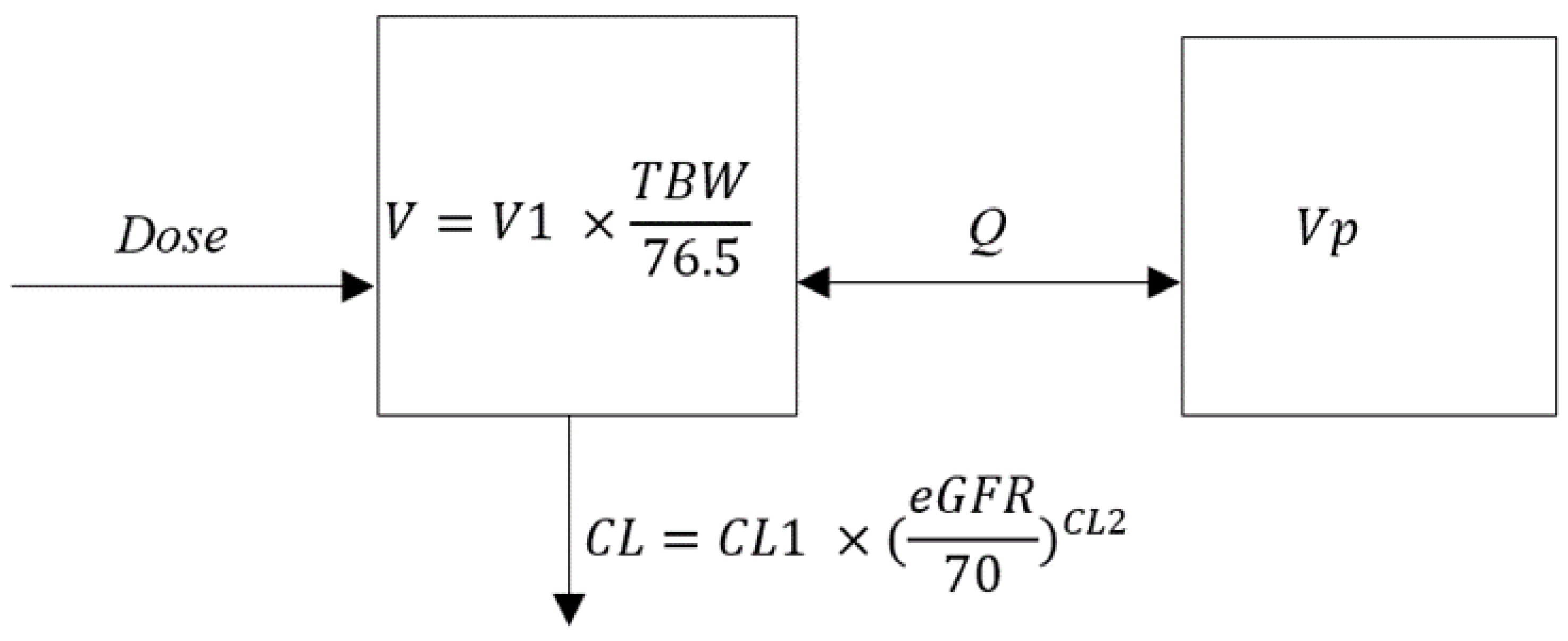
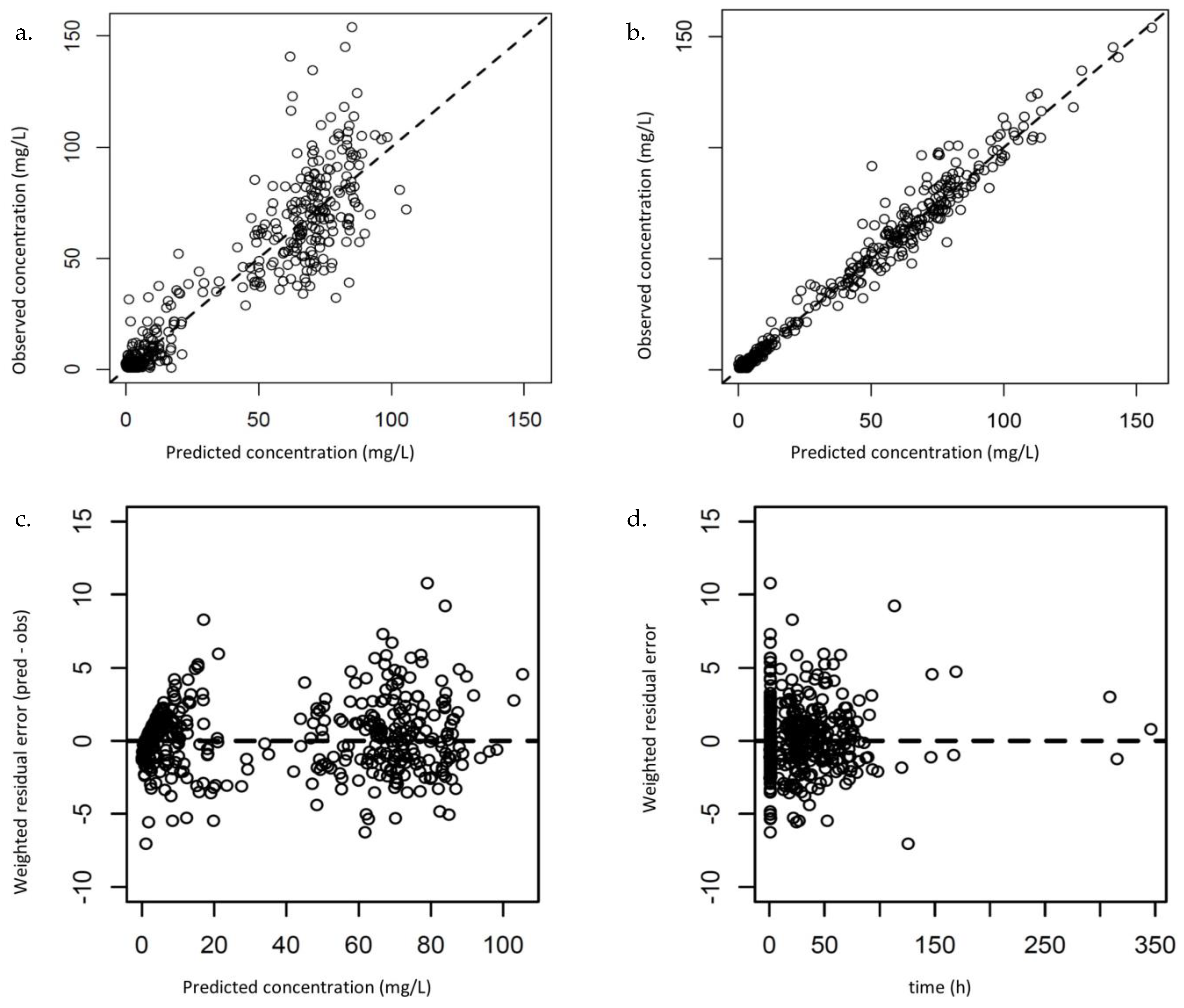
2.2. Population PK Modeling and Evaluation with Pmetrics
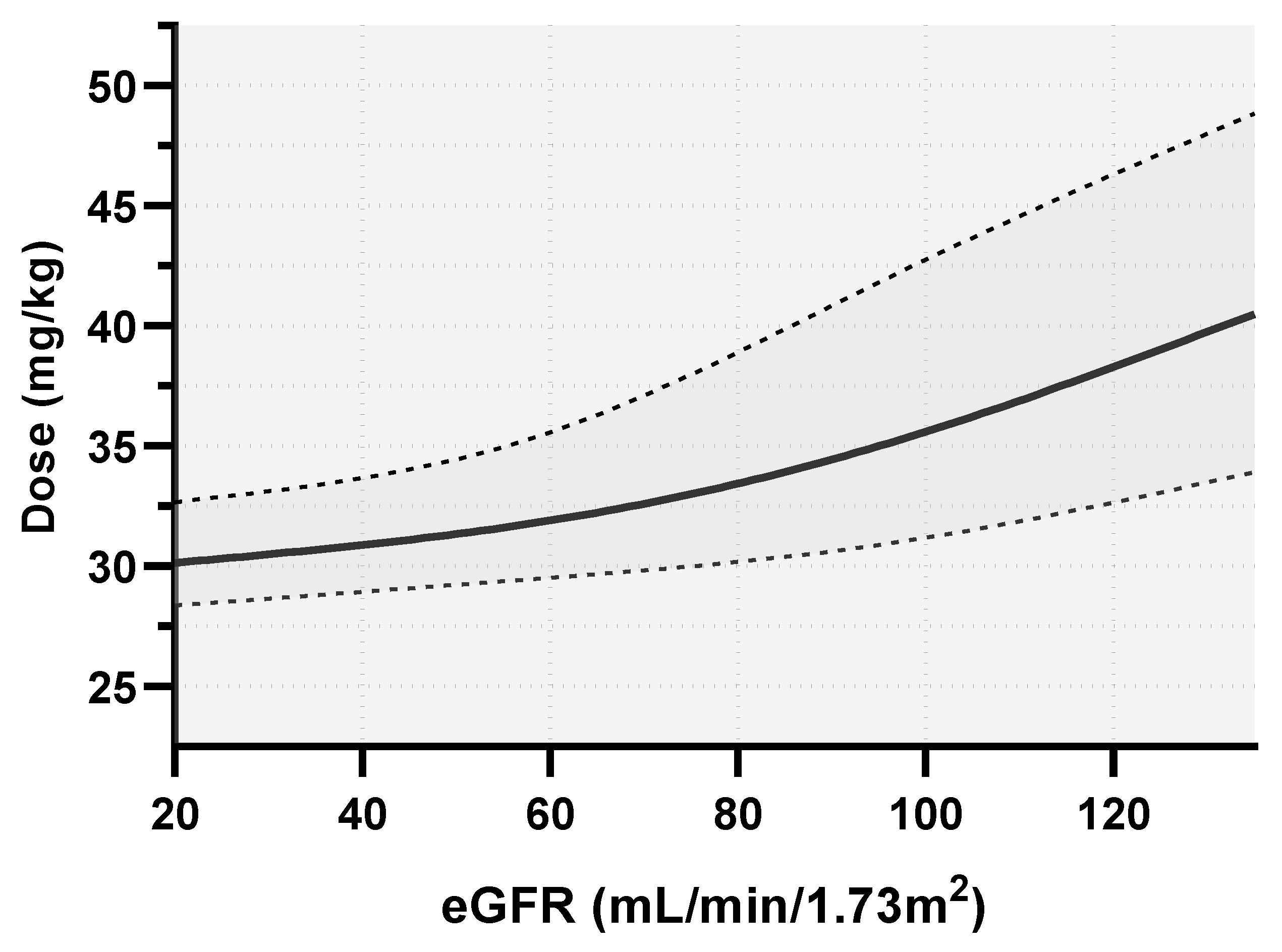
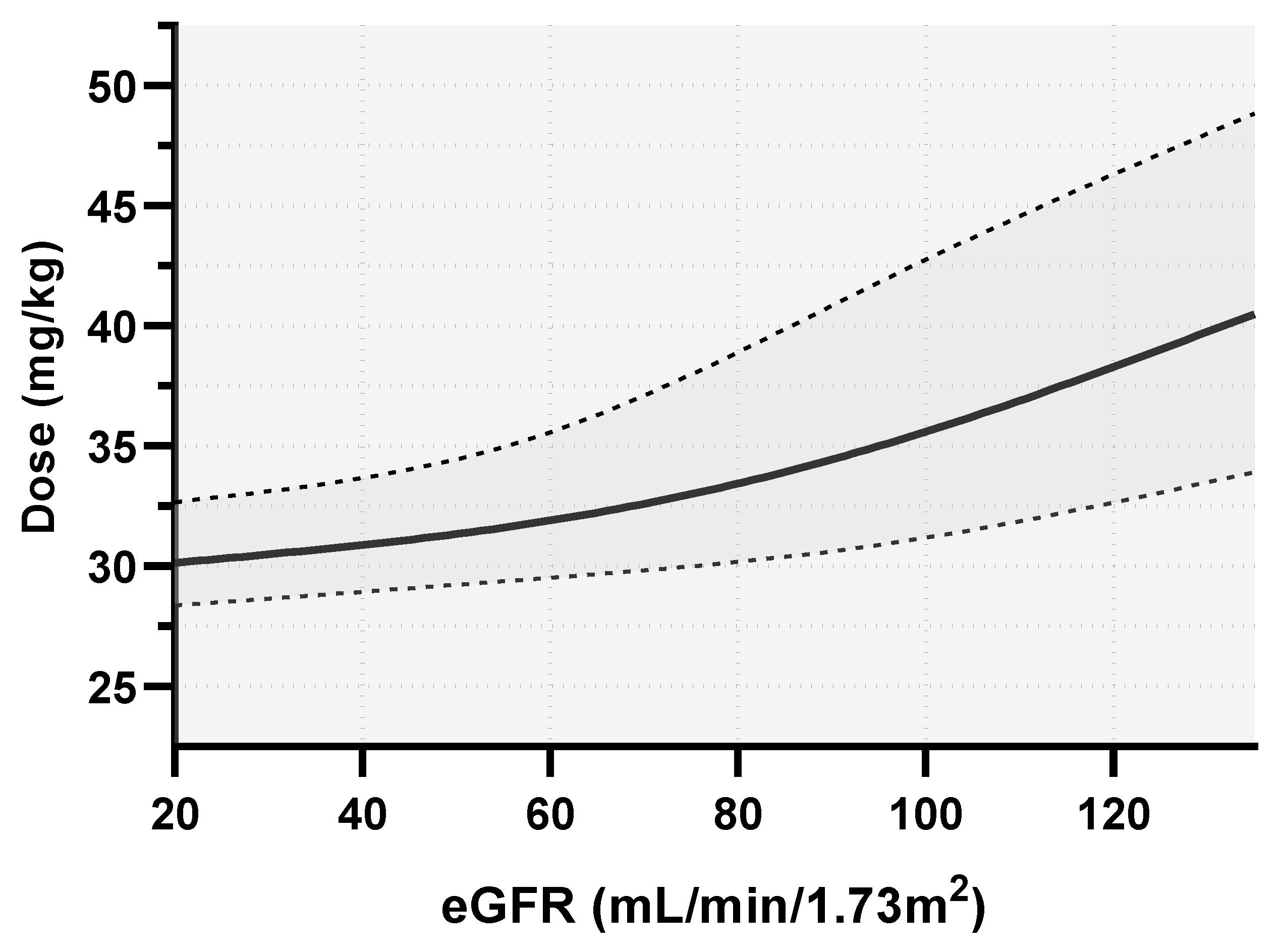
2.3. Monte Carlo Simulations and Dosing Nomograms
3. Discussion
4. Materials and Methods
4.1. Patient Population and Data Collection
4.2. Bacterial Susceptibility Testing and Amikacin Quantification
4.3. Population Pharmacokinetics Analysis
4.3.1. Base Model
4.3.2. Covariate Model
4.3.3. Model Evaluation
4.4. PTA and Dosing Nomogram
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Micek, S.T.; Welch, E.C.; Khan, J.; Pervez, M.; Doherty, J.A.; Reichley, R.M.; Kollef, M.H. Empiric Combination Antibiotic Therapy Is Associated with Improved Outcome against Sepsis Due to Gram-Negative Bacteria: A Retrospective Analysis. Antimicrob. Agents Chemother. 2010, 54, 1742–1748. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Safdar, N.; Kethireddy, S.; Chateau, D. A Survival Benefit of Combination Antibiotic Therapy for Serious Infections Associated with Sepsis and Septic Shock Is Contingent Only on the Risk of Death: A Meta-Analytic/Meta-Regression Study. Crit. Care Med. 2010, 38, 1651–1664. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Zarychanski, R.; Light, B.; Parrillo, J.; Maki, D.; Simon, D.; Laporta, D.; Lapinsky, S.; Ellis, P.; Mirzanejad, Y.; et al. Early Combination Antibiotic Therapy Yields Improved Survival Compared with Monotherapy in Septic Shock: A Propensity-Matched Analysis. Crit. Care Med. 2010, 38, 1773–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Coste, A.; Deslandes, G.; Jalin, L.; Corvec, S.; Caillon, J.; Boutoille, D.; Grégoire, M.; Bretonnière, C. PK/PD Targets of Amikacin and Gentamicin in ICU Patients. Médecine Mal. Infect. 2020, 50, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.D.; Lietman, P.S.; Smith, C.R. Clinical Response to Aminoglycoside Therapy: Importance of the Ratio of Peak Concentration to Minimal Inhibitory Concentration. J. Infect. Dis. 1987, 155, 93–99. [Google Scholar] [CrossRef]
- Duszynska, W.; Taccone, F.S.; Hurkacz, M.; Kowalska-Krochmal, B.; Wiela-Hojeńska, A.; Kübler, A. Therapeutic Drug Monitoring of Amikacin in Septic Patients. Crit. Care 2013, 17, R165. [Google Scholar] [CrossRef] [Green Version]
- Kashuba, A.D.M.; Nafziger, A.N.; Drusano, G.L.; Bertino, J.S. Optimizing Aminoglycoside Therapy for Nosocomial Pneumonia Caused by Gram-Negative Bacteria. Antimicrob. Agents Chemother. 1999, 43, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Zelenitsky, S.A.; Harding, G.K.M.; Sun, S.; Ubhi, K.; Ariano, R.E. Treatment and Outcome of Pseudomonas Aeruginosa Bacteraemia: An Antibiotic Pharmacodynamic Analysis. J. Antimicrob. Chemother. 2003, 52, 668–674. [Google Scholar] [CrossRef]
- Agence française de sécurité sanitaire des produits de santé. Update on Good Use of Injectable Aminoglycosides, Gentamycin, Tobramycin, Netilmycin, Amikacin. Pharmacological Properties, Indications, Dosage, and Mode of Administration, Treatment Monitoring. Médecine Mal. Infect. 2012, 42, 301–308. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoints Tables for Interpretation of MICs and Zone Diameter. Version 12.0; 2022. Available online: https://www.eucast.org/ (accessed on 28 November 2022).
- Allou, N.; Bouteau, A.; Allyn, J.; Snauwaert, A.; Valance, D.; Jabot, J.; Bouchet, B.; Galliot, R.; Corradi, L.; Montravers, P.; et al. Impact of a High Loading Dose of Amikacin in Patients with Severe Sepsis or Septic Shock. Ann. Intensive Care 2016, 6, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goutelle, S.; Fritsch, G.; Leroy, M.; Piron, C.; Salvez, C.; Incagnoli, P.; David, J.S.; Friggeri, A. Amikacin in Emergency Surgery: How to Dose It Optimally? Anaesth. Crit. Care Pain Med. 2022, 41, 100990. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Lipman, J. Pharmacokinetic Issues for Antibiotics in the Critically Ill Patient. Crit. Care Med. 2009, 37, 840–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Blanco, J.S.; Sáez Fernández, E.M.; Calvo, M.V.; Lanao, J.M.; Martín-Suárez, A. Evaluation of Current Amikacin Dosing Recommendations and Development of an Interactive Nomogram: The Role of Albumin. Pharmaceutics 2021, 13, 264. [Google Scholar] [CrossRef]
- Marsot, A.; Guilhaumou, R.; Riff, C.; Blin, O. Amikacin in Critically Ill Patients: A Review of Population Pharmacokinetic Studies. Clin. Pharmacokinet. 2017, 56, 127–138. [Google Scholar] [CrossRef]
- Burdet, C.; Pajot, O.; Couffignal, C.; Armand-Lefèvre, L.; Foucrier, A.; Laouénan, C.; Wolff, M.; Massias, L.; Mentré, F. Population Pharmacokinetics of Single-Dose Amikacin in Critically Ill Patients with Suspected Ventilator-Associated Pneumonia. Eur. J. Clin. Pharmacol. 2015, 71, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Matar, K.M.; Al-lanqawi, Y.; Abdul-Malek, K.; Jelliffe, R. Amikacin Population Pharmacokinetics in Critically Ill Kuwaiti Patients. BioMed Res. Int. 2013, 2013, 202818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chennavasin, P.; Brater, D.C. Nomograms for Drug Use in Renal Disease. Clin. Pharmacokinet. 1981, 6, 193–214. [Google Scholar] [CrossRef]
- Chai, M.G.; Cotta, M.O.; Abdul-Aziz, M.H.; Roberts, J.A. What Are the Current Approaches to Optimising Antimicrobial Dosing in the Intensive Care Unit? Pharmaceutics 2020, 12, 638. [Google Scholar] [CrossRef]
- Bellouard, R.; Deschanvres, C.; Deslandes, G.; Dailly, É.; Asseray, N.; Jolliet, P.; Boutoille, D.; Gaborit, B.; Grégoire, M. Population Pharmacokinetic Study of Cefazolin Dosage Adaptation in Bacteremia and Infective Endocarditis Based on a Nomogram. Antimicrob. Agents Chemother. 2019, 63, e00806-19. [Google Scholar] [CrossRef] [Green Version]
- Grégoire, M.; Dailly, E.; Le Turnier, P.; Garot, D.; Guimard, T.; Bernard, L.; Tattevin, P.; Vandamme, Y.M.; Hoff, J.; Lemaitre, F.; et al. High-Dose Ceftriaxone for Bacterial Meningitis and Optimization of Administration Scheme Based on Nomogram. Antimicrob. Agents Chemother. 2019, 63, e00634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pea, F.; Viale, P.; Cojutti, P.; Furlanut, M. Dosing Nomograms for Attaining Optimum Concentrations of Meropenem by Continuous Infusion in Critically III Patients with Severe Gram-Negative Infections: A Pharmacokinetics/Pharmacodynamics-Based Approach. Antimicrob. Agents Chemother. 2012, 56, 6343–6348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baptista, J.P.; Roberts, J.A.; Sousa, E.; Freitas, R.; Deveza, N.; Pimentel, J. Decreasing the Time to Achieve Therapeutic Vancomycin Concentrations in Critically III Patients: Developing and Testing of a Dosing Nomogram. Crit. Care 2014, 18, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goutelle, S.; Woillard, J.B.; Neely, M.; Yamada, W.; Bourguignon, L. Nonparametric Methods in Population Pharmacokinetics. J. Clin. Pharmacol. 2022, 62, 142–157. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised Antibiotic Dosing for Patients Who Are Critically Ill: Challenges and Potential Solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roger, C.; Nucci, B.; Louart, B.; Friggeri, A.; Knani, H.; Evrard, A.; Lavigne, J.P.; Allaouchiche, B.; Lefrant, J.Y.; Roberts, J.A.; et al. Impact of 30 Mg/Kg Amikacin and 8 Mg/Kg Gentamicin on Serum Concentrations in Critically Ill Patients with Severe Sepsis. J. Antimicrob. Chemother. 2016, 71, 208–212. [Google Scholar] [CrossRef] [Green Version]
- Gálvez, R.; Luengo, C.; Cornejo, R.; Kosche, J.; Romero, C.; Tobar, E.; Illanes, V.; Llanos, O.; Castro, J. Higher than Recommended Amikacin Loading Doses Achieve Pharmacokinetic Targets without Associated Toxicity. Int. J. Antimicrob. Agents 2011, 38, 146–151. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Pai, M.P.; Nafziger, A.N.; Bertino, J.S. Simplified Estimation of Aminoglycoside Pharmacokinetics in Underweight and Obese Adult Patients. Antimicrob. Agents Chemother. 2011, 55, 4006–4011. [Google Scholar] [CrossRef]
- Sangla, F.; Marti, P.E.; Verissimo, T.; Pugin, J.; de Seigneux, S.; Legouis, D. Measured and Estimated Glomerular Filtration Rate in the ICU: A Prospective Study. Crit. Care Med. 2020, 48, e1232–e1241. [Google Scholar] [CrossRef] [PubMed]
- Velissaris, D.; Karamouzos, V.; Marangos, M.; Pierrakos, C.; Karanikolas, M. Pharmacokinetic Changes and Dosing Modification of Aminoglycosides in Critically Ill Obese Patients: A Literature Review. J. Clin. Med. Res. 2014, 6, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, T.; Fujii, S.; Shigemi, A.; Takesue, Y. A Meta-Analysis of the Target Trough Concentration of Gentamicin and Amikacin for Reducing the Risk of Nephrotoxicity. J. Infect. Chemother. 2020, 27, 256–261. [Google Scholar] [CrossRef]
- Marik, P.E.; Lipman, J.; Kobilski, S.; Scribante, J. A Prospective Randomized Study Comparing Once- versus Twice-Daily Amikacin Dosing in Critically Ill Adult and Paediatric Patients. J. Antimicrob. Chemother. 1991, 28, 753–764. [Google Scholar] [CrossRef]
- Lane, A.Z.; Wright, G.E.; Blair, D.C. Ototoxicity and Nephrotoxicity of Amikacin: An Overview of Phase II and Phase III Experience in the United States. Am. J. Med. 1977, 62, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Ledesma, K.R.; Wang, W.; Tam, V.H. Characterization of Amikacin Drug Exposure and Nephrotoxicity in an Animal Model. Antimicrob. Agents Chemother. 2020, 64, e00859. [Google Scholar] [CrossRef]
- Marsot, A.; Hraiech, S.; Cassir, N.; Daviet, F.; Parzy, G.; Blin, O.; Papazian, L.; Guilhaumou, R. Aminoglycosides in Critically Ill Patients: Which Dosing Regimens for Which Pathogens? Int. J. Antimicrob. Agents 2020, 56, 106124. [Google Scholar] [CrossRef]
- Logre, E.; Enser, M.; Tanaka, S.; Dubert, M.; Claudinon, A.; Grall, N.; Mentec, H.; Montravers, P.; Pajot, O. Amikacin Pharmacokinetic/Pharmacodynamic in Intensive Care Unit: A Prospective Database. Ann. Intensive Care 2020, 10, 75. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Data from the EUCAST MIC Distribution Website. Available online: https://mic.eucast.org/search/?search%5Bmethod%5D=mic&search%5Bantibiotic%5D=1&search%5Bspecies%5D=-1&search%5Bdisk_content%5D=-1&search%5Blimit%5D=50 (accessed on 24 January 2021).
- Ramirez, M.S.; Tolmasky, M.E. Amikacin: Uses, Resistance, and Prospects for Inhibition. Molecules 2017, 22, 2267. [Google Scholar] [CrossRef] [Green Version]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Du Bois, D.; Du Bois, E.F. A Formula to Estimate the Approximate Surface Area If Height and Weight Be Known. 1916. Nutrition 1989, 5, 303–311. [Google Scholar] [PubMed]
- Lorentz, F.H. Der Konstitutionsindex der Frau. Klin. Wochenschr. 1929, 8, 734–736. [Google Scholar] [CrossRef]
- Traynor, A.M.; Nafziger, A.N.; Bertino, J.S. Aminoglycoside Dosing Weight Correction Factors for Patients of Various Body Sizes. Antimicrob. Agents Chemother. 1995, 39, 545–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neely, M.N.; van Guilder, M.G.; Yamada, W.M.; Schumitzky, A.; Jelliffe, R.W. Accurate Detection of Outliers and Subpopulations with Pmetrics, a Nonparametric and Parametric Pharmacometric Modeling and Simulation Package for R. Ther. Drug Monit. 2012, 34, 467–476. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient’s Characteristics | Median [Q1–Q3] or n (%) |
|---|---|
| Age (years) | 62 [49–72] |
| Sex (male) | 90 (65.2) |
| Total body weight (kg) | 76.5 [62.0–88.5] |
| Height (cm) | 170 [163–177] |
| Body mass index (kg/m2) | 25.6 [21.9–31.4] |
| Body mass index ≥ 30 kg/m2, n (%) | 41 (29.7) |
| Body surface area (m2) | 1.89 [1.72–2.03] |
| SAPS II | 41 [31–56] |
| Total proteinemia (g/L) | 55 [48–62] |
| Albuminemia (g/L) | 26.0 [20.6–30.8] |
| Serum creatinine (µmol/L) | 91 [61–171] |
| eGFR (CKD–EPI formula, mL/min/1.73 m2) | 70.0 [41.9–111.5] |
| Renal replacement therapy | 9 (6.5) |
| Vasopressors use | 79 (57.3) |
| Invasive mechanical ventilation | 94 (68.1) |
| Parameter 1 | Median (95% CI) | MAWD (95% CI) | Range |
|---|---|---|---|
| CL1 | 4.41 (3.84–5.27) | 1.24 (0.64–1.99) | 0.01–15.00 |
| CL2 | 0.72 (0.57–0.92) | 0.29 (0.15–0.56) | 0.01–10.00 |
| V1 | 20.40 (16.58–26.49) | 5.45 (2.58–8.88) | 0.01–60.00 |
| Vp | 16.32 (13.71–23.99) | 7.20 (3.94–14.95) | 0.10–100.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coste, A.; Bellouard, R.; Deslandes, G.; Jalin, L.; Roger, C.; Ansart, S.; Dailly, E.; Bretonnière, C.; Grégoire, M. Development of a Predictive Dosing Nomogram to Achieve PK/PD Targets of Amikacin Initial Dose in Critically Ill Patients: A Non-Parametric Approach. Antibiotics 2023, 12, 123. https://doi.org/10.3390/antibiotics12010123
Coste A, Bellouard R, Deslandes G, Jalin L, Roger C, Ansart S, Dailly E, Bretonnière C, Grégoire M. Development of a Predictive Dosing Nomogram to Achieve PK/PD Targets of Amikacin Initial Dose in Critically Ill Patients: A Non-Parametric Approach. Antibiotics. 2023; 12(1):123. https://doi.org/10.3390/antibiotics12010123
Chicago/Turabian StyleCoste, Anne, Ronan Bellouard, Guillaume Deslandes, Laurence Jalin, Claire Roger, Séverine Ansart, Eric Dailly, Cédric Bretonnière, and Matthieu Grégoire. 2023. "Development of a Predictive Dosing Nomogram to Achieve PK/PD Targets of Amikacin Initial Dose in Critically Ill Patients: A Non-Parametric Approach" Antibiotics 12, no. 1: 123. https://doi.org/10.3390/antibiotics12010123
APA StyleCoste, A., Bellouard, R., Deslandes, G., Jalin, L., Roger, C., Ansart, S., Dailly, E., Bretonnière, C., & Grégoire, M. (2023). Development of a Predictive Dosing Nomogram to Achieve PK/PD Targets of Amikacin Initial Dose in Critically Ill Patients: A Non-Parametric Approach. Antibiotics, 12(1), 123. https://doi.org/10.3390/antibiotics12010123