
New Antimicrobials for the Treatment of Neonatal Sepsis Caused by Multi-Drug-Resistant Bacteria: A Systematic Review


Abstract
:1. Introduction
1.1. Epidemiology
1.2. Current Treatment Options
2. Results
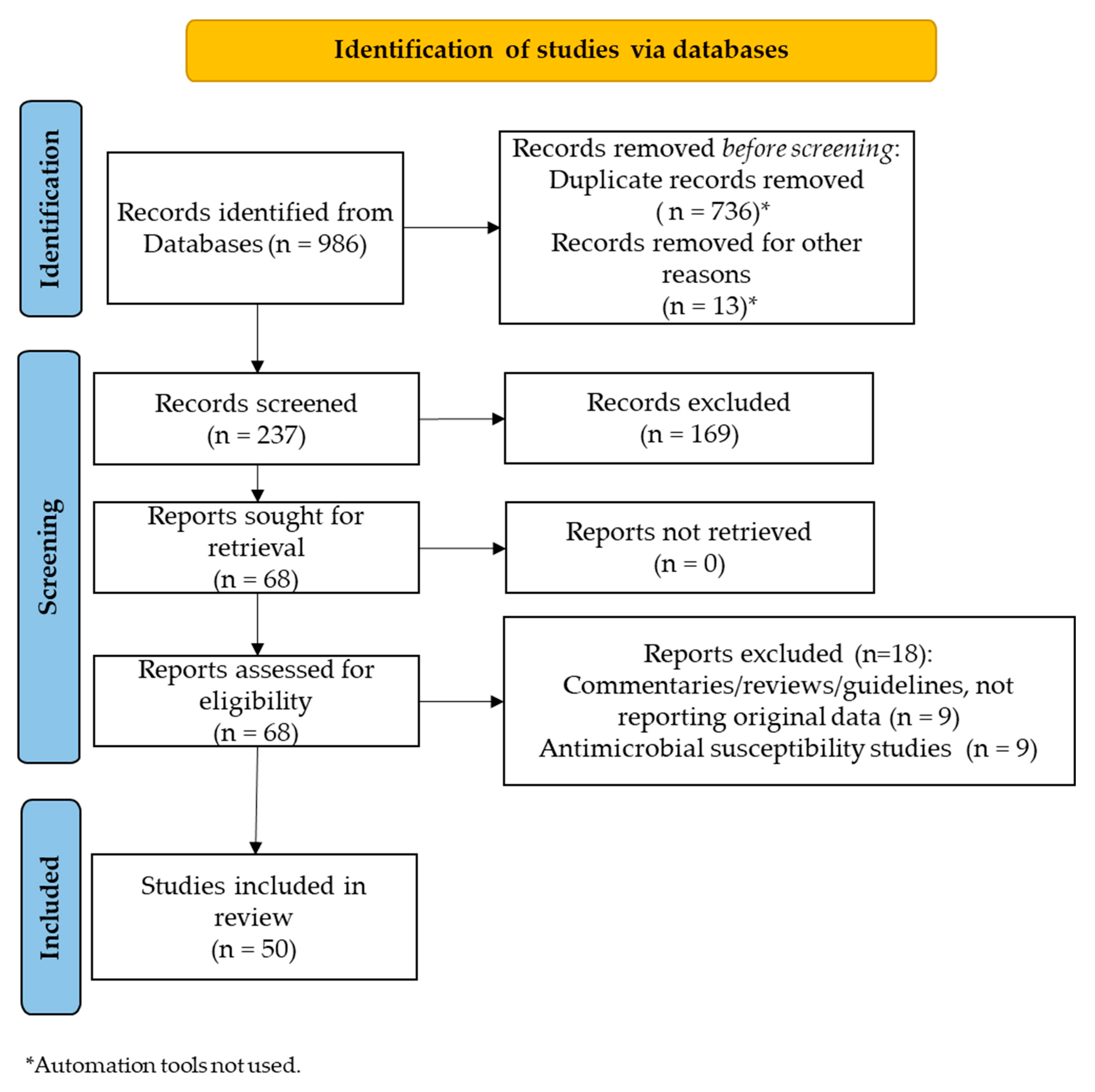
2.1. Study Selection
2.2. Treatment of MDR Gram-Negative Bacteria
2.2.1. Ceftazidime/Avibactam
2.2.2. Ceftolozane/Tazobactam
2.2.3. Cefiderocol
2.2.4. Meropenem/Vaborbacatam
2.3. Treatment of Gram-Positive Bacteria with Resistance of Concerns
2.3.1. Ceftaroline
2.3.2. Dalbavancin
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Eligibility
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Reichert, F.; Cassini, A.; Horner, R.; Harder, T.; Markwart, R.; Tröndle, M.; Savova, Y.; Kissoon, N.; Schlattmann, P.; et al. Global incidence and mortality of neonatal sepsis: A systematic review and meta-analysis. Arch. Dis. Child. 2021, 106, 745–752. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Li, G.; Bielicki, J.A.; Ahmed AS MN, U.; Islam, M.S.; Berezin, E.N.; Gallacci, C.B.; Guinsburg, R.; da Silva Figueiredo, C.E.; Vieira, R.S.; Silva, A.R.; et al. Towards understanding global patterns of antimicrobial use and resistance in neonatal sepsis: Insights from the NeoAMR network. Arch. Dis. Child. 2020, 105, 26–31. [Google Scholar] [CrossRef]
- Sands, K.; Carvalho, M.J.; Portal, E.; Thomson, K.; Dyer, C.; Akpulu, C.; Andrews, R.; Ferreira, A.; Gillespie, D.; Hender, T.; et al. Characterization of antimicrobial-resistant Gram negative bacteria that cause neonatal sepsis in seven low and middle-income countries. Nat. Microbiol. 2021, 6, 512–523. [Google Scholar] [CrossRef]
- Thomson, K.M.; Dyer, C.; Liu, F.; Sands, K.; Portal, E.; Carvalho, M.J.; Barrell, M.; Boostrom, I.; Dunachie, S.; Farzana, R.; et al. Effects of antibiotic resistance, drug target attainment, bacterial pathogenicity and virulence, and antibiotic access and affordability on outcomes in neonatal sepsis: An international microbiology and drug evaluation prospective substudy (BARNARDS). Lancet Infect. Dis. 2021, 21, 1677–1688. [Google Scholar] [CrossRef]
- Investigators of the Delhi Neonatal Infection Study (DeNIS) Collaboration. Characterization and antimicrobial resistance of sepsis pathogens in neonates born in tertiary care centres in Delhi, India: A cohort study. Lancet Glob. Health 2016, 4, e752–e760. [Google Scholar] [CrossRef]
- Wang, J.; Lv, Y.; Yang, W.; Zhao, P.; Yin, C. Epidemiology and clinical characteristics of infection/colonization due to carbapenemase-producing Enterobacterale in neonatal patients. BMC Microbiol. 2022, 22, 177. [Google Scholar] [CrossRef]
- Pathak, A.; Tejan, N.; Dubey, A.; Chauhan, R.; Fatima, N.; Jyoti Singh, S.; Bhayana, S.; Sahu, C. Outbrteak of colistin resistant, carbapenemase (blaNDM, blaOXA-232) producing Klebsiella pneumoniae causing blood stream infection among neonates at a tertiary care hospital in India. Front. Cell. Infect. Microbiol. 2023, 13, 1051020. [Google Scholar] [CrossRef]
- Alanezi, G.; Almulhem, A.; Aldriwesh, M.; Bawazeer, M. A triple antimicrobial regimen for multi-drug resistant Klebsiella pneumoniae in a neonatal intensive care unit outbreak: A case series. J. Infect. Public Health 2022, 15, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Manandhar, S.; Nguyen, Q.; Pham, D.; Amatya, P.; Rabaa, M.; Dongol, S.; Basnyat, B.; Dixit, S.; Baker, S.; Karkey, A. A fatal outbreak of neonatal sepsis caused by mcr-10-carrying Enterobacter kobei in a tertiary care hospital in Nepal. J. Hosp. Infect. 2022, 125, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Labi, A.-K.M.; Enweronu-Laryea, C.C.M.; Nartey, E.T.; Bjerrum, S.M.; Ayibor, P.K.M.; Andersen, L.P.; Newman, M.J.M.; Kurtzhals, J.A.L.M. Bloodstream Infections at Two Neonatal Intensive Care Units in Ghana: Multidrug Resistant Enterobacterales Undermine the Usefulness of Standard Antibiotic Regimes. Pediatr. Infect. Dis. J. 2021, 40, 1115–1121. [Google Scholar] [CrossRef]
- Agosta, M.; Bencardino, D.; Argentieri, M.; Pansani, L.; Sisto, A.; Degli Atti, M.L.C.; D’amore, C.; Bagolan, P.; Iacobelli, B.D.; Magnani, M.; et al. Clonal Spread of Hospital-Acquired NDM-1-Producing Klebsiella pneumoniae and Escherichia coli in an Italian Neonatal Surgery Unit: A Retrospective Study. Antibiotics 2023, 12, 642. [Google Scholar] [CrossRef] [PubMed]
- Berglund, B.; Hoang, N.T.B.; Lundberg, L.; Le, N.K.; Tärnberg, M.; Nilsson, M.; Bornefall, E.; Khu, D.T.K.; Welander, J.; Le, H.T.; et al. Clonal spread of carbapenem-resistant Klebsiella pneumoniae among patients at admission and discharge at a Vietnamese neonatal intensive care unit. Antimicrob. Resist. Infect. Control 2021, 10, 162. [Google Scholar] [CrossRef]
- Villinger, D.; Schultze, T.G.; Musyoki, V.M.; Inwani, I.; Aluvaala, J.; Okutoyi, L.; Ziegler, A.-H.; Wieters, I.; Stephan, C.; Museve, B.; et al. Genomic transmission analysis of multidrug-resistant Gram-negative bacteria within a newborn unit of a Kenyan tertiary hospital: A four-month prospective colonization study. Front. Cell. Infect. Microbiol. 2022, 12, 892126. [Google Scholar] [CrossRef]
- Agosta, M.; Bencardino, D.; Argentieri, M.; Pansani, L.; Sisto, A.; Degli Atti, M.L.C.; D’amore, C.; Putignani, L.; Bagolan, P.; Iacobelli, B.D.; et al. Prevalence and Molecular Typing of Carbapenemase-Producing Enterobacterales among Newborn Patients in Italy. Antibiotics 2022, 11, 431. [Google Scholar] [CrossRef]
- Carvalho, M.J.; Sands, K.; Thomson, K.; Portal, E.; Mathias, J.; Milton, R.; Gillespie, D.; Dyer, C.; Akpulu, C.; Boostrom, I.; et al. Antibiotic resistance genes in the gut microbiota of mothers and linked neonates with or without sepsis from low- and middle-income countries. Nat. Microbiol. 2022, 7, 1337–1347. [Google Scholar] [CrossRef]
- Okomo, U.; Akpalu, E.N.K.; Le Doare, K.; Roca, A.; Cousens, S.; Jarde, A.; Sharland, M.; Kampmann, B.; E Lawn, J. Aetiology of invasive bacterial infection and antimicrobial resistance in neonates in sub-Saharan Africa: A systematic review and meta-analysis in line with the STROBE-NI reporting guidelines. Lancet Infect. Dis. 2019, 3099, 1219–1234. [Google Scholar] [CrossRef]
- Gu, S.; Lai, J.; Kang, W.; Li, Y.; Zhu, X.; Ji, T.; Feng, J.; Zhao, L.; Li, Z.; Dong, L.; et al. Drug resistance characteristics and molecular typing of Escherichia coli isolates from neonates in class A tertiary hospitals: A multicentre study across China. J. Infect. 2022, 85, 499–506. [Google Scholar] [CrossRef]
- Ren, Z.; Yang, S.; Han, J.; Nie, C.; Wang, C.; Wang, J.; Zheng, X.; Yang, H.; Zhang, Q.; Pei, J.; et al. Reduction of antibiotic use and multi-drug resistance bacteria infection in neonates after improvement of antibiotics use strategy in a level 4 neonatal intensive care unit in southern China. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-Y.; Chen, S.-Q.; Yan, Y.-Y.; Hu, Y.-Y.; Wei, J.; Wu, Q.-P.; Lin, Z.-L.; Lin, J. Identification and antimicrobial resistance of pathogens in neonatal septicemia in China—A meta-analysis. Int. J. Infect. Dis. 2018, 71, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Puopolo, K.M.; Hansen, N.I.; Sánchez, P.J.; Bell, E.F.; Carlo, W.A.; Cotten, C.M.; D’Angio, C.T.; Kazzi, S.N.J.; Poindexter, B.B.; et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef] [PubMed]
- Flannery, D.D.; Chiotos, K.; Gerber, J.S.; Puopolo, K.M. Neonatal multidrug-resistant gram-negative infection: Epidemiology, mechanisms of resistance, and management. Pediatr. Res. 2022, 91, 380–391. [Google Scholar] [CrossRef]
- Flannery, D.D.; Akinboyo, I.C.; Mukhopadhyay, S.; Tribble, A.C.; Song, L.; Chen, F.; Li, Y.; Gerber, J.S.; Puopolo, K.M. Antibiotic Susceptibility of Escherichia coli among Infants Admitted to Neonatal Intensive Care Units across the US from 2009 to 2017. JAMA Pediatr. 2021, 175, 168–175. [Google Scholar] [CrossRef]
- Patel, S.J.; Green, N.; Clock, S.A.; Paul, D.A.; Perlman, J.M.; Zaoutis, T.; Ferng, Y.-H.; Alba, L.; Jia, H.; Larson, E.L.; et al. Gram-Negative Bacilli in Infants Hospitalized in the Neonatal Intensive Care Unit. J. Pediatr. Infect. Dis. Soc. 2017, 6, 227–230. [Google Scholar] [CrossRef]
- Daniels, K.; Arrieta, A.; Nieves, D.J.; Bhakta, K.; Tran, M.T.; Osborne, S.; Morphew, T. Ampicillin and Gentamicin Treatment for Early Onset Neonatal Sepsis: When One Size Does Not Fit All. Clin. Pediatr. 2023, 24, 99228221150612. [Google Scholar] [CrossRef]
- Cailes, B.; Kortsalioudaki, C.; Buttery, J.; Pattnayak, S.; Greenough, A.; Matthes, J.; Russell, A.B.; Kennea, N.; Heath, P. Antimicrobial resistance in UK neonatal units: neonIN infection surveillance network. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F474–F478. [Google Scholar] [CrossRef]
- Gkentzi, D.; Kortsalioudaki, C.; Cailes, B.C.; Zaoutis, T.; Kopsidas, J.; Tsolia, M.; Spyridis, N.; Siahanidou, S.; Sarafidis, K.; Heath, P.T.; et al. Epidemiology of infections and antimicrobial use in Greek Neonatal Units. Arch. Dis. Child. Fetal. Neonatal Ed. 2019, 104, F293–F297. [Google Scholar] [CrossRef]
- Köstlin-Gille, N.; Härtel, C.; Haug, C.; Göpel, W.; Zemlin, M.; Müller, A.; Poets, C.F.; Herting, E.; Gille, C. Epidemiology of Early and Late Onset Neonatal Sepsis in Very Low Birthweight Infants: Data from the German Neonatal Network. Pediatr. Infect. Dis. J. 2021, 40, 255–259. [Google Scholar] [CrossRef]
- Orman, A.; Celik, Y.; Evik, G.; Ersöz, G.; Kuyucu, N.; Ozmen, B.O. Should Perirectal Swab Culture Be Performed in Cases Admitted to the Neonatal Intensive Care Unit? Lessons Learned from the Neonatal Intensive Care Unit. Children 2023, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Odoyo, E.; Matano, D.; Tiria, F.; Georges, M.; Kyanya, C.; Wahome, S.; Mutai, W.; Musila, L. Environmental contamination across multiple hospital departments with multidrug-resistant bacteria pose an elevated risk of healthcare-associated infections in Kenyan hospitals. Antimicrob. Resist. Infect. Control 2023, 12, 22. [Google Scholar] [CrossRef] [PubMed]
- Van der Hoeven, A.; Bekker, V.; Jansen, S.J.; Saccoccia, B.; Berkhout, R.J.; Lopriore, E.; Veldkamp, K.E.; van der Beek, M.T. Impact of transition from open bay to single room design neonatal intensive care unit on multidrug-resistant organism colonization rates. J. Hosp. Infect. 2022, 120, 90–97. [Google Scholar] [CrossRef]
- Saporito, L.; Graziano, G.; Mescolo, F.; Amodio, E.; Insinga, V.; Rinaudo, G.; Aleo, A.; Bonura, C.; Vitaliti, M.; Corsello, G.; et al. Efficacy of a coordinated strategy for containment of multidrug-resistant Gram-negative bacteria carriage in a Neonatal Intensive Care Unit in the context of an active surveillance program. Antimicrob. Resist. Infect. Control 2021, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Litz, J.E.; Goedicke-Fritz, S.; Härtel, C.; Zemlin, M.; Simon, A. Management of early- and late-onset sepsis: Results from a survey in 80 German NICUs. Infection 2019, 47, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Matrat, L.; Plaisant, F.; Barreto, C.; Claris, O.; Butin, M. Increasing use of linezolid in a tertiary NICU during a 10-year period: Reasons and concerns for the future. Antimicrob. Resist. Infect. Control 2020, 9, 156. [Google Scholar] [CrossRef]
- Marom, R.; Mandel, D.; Haham, A.; Berger, I.; Ovental, A.; Raskind, C.; Grisaru-Soen, G.; Adler, A.; Lellouche, J.; Schwartz, D.; et al. A silent outbreak of vancomycin-resistant Enterococcus faecium in a neonatal intensive care unit. Antimicrob. Resist. Infect. Control 2020, 9, 87. [Google Scholar] [CrossRef]
- Darlow, C.A.; da Costa, R.M.A.; Ellis, S.; Franceschi, F.; Sharland, M.; Piddock, L.; Das, S.; Hope, W. Potential Antibiotics for the Treatment of Neonatal Sepsis Caused by Multidrug-Resistant Bacteria. Paediatr. Drugs 2021, 23, 465–484. [Google Scholar] [CrossRef]
- Williams, P.C.; Qazi, S.A.; Agarwal, R.; Velaphi, S.; Bielicki, J.A.; Nambiar, S.; Giaquinto, C.; Bradley, J.; Noel, G.J.; Ellis, S.; et al. Antibiotics needed to treat multidrug-resistant infections in neonates. Bull. World Health Organ. 2022, 100, 797–807. [Google Scholar] [CrossRef]
- Tzialla, C.; Borghesi, A.; Pozzi, M.; Stronati, M. Neonatal infections due to multi-resistant strains: Epidemiology, current treatment, emerging therapeutic approaches and prevention. Clin. Chim. Acta 2015, 451 Pt A, 71–77. [Google Scholar] [CrossRef]
- Chiusaroli, L.; Liberati, C.; Vaseti, M.; Rulli, L.; Barbieri, E.; Giacquinto, C.; Donà, D. Therapeutic Options and Outcomes for the Treatment of Neonates and Preterms with Gram-Negative Multidrug-Resistant Bacteria: A Systematic Review. Antibiotics 2022, 11, 1088. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Velaphi, S.; Ellis, S.; Walker, A.S.; Standing, J.F.; Heath, P.; Sharland, M.; Donà, D. The use of polymyxins to treat carbapenem resistant infections in neonates and children. Expert Opin. Pharmacother. 2019, 20, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Chiotos, K.; Hayes, M.; Gerber, J.S.; Tamma, P.D. Treatment of Carbapenem-Resistant Enterobacteriaceae Infections in Children. J. Pediatr. Infect. Dis. Soc. 2020, 9, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Chiusaroli, L.; Liberati, C.; Rulli, L.; Barbieri, E.; De Pieri, M.; Di Chiara, C.; Mengato, D.; Giacquinto, C.; Donà, D. Therapeutic Options and Outcomes for the Treatment of Children with Gram-Positive Bacteria with Resistances of Concern: A Systematic Review. Antibiotics 2023, 12, 261. [Google Scholar] [CrossRef]
- Zavicefta. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zavicefta (accessed on 25 March 2023).
- Vaborem. Available online: https://www.ema.europa.eu/en/documents/product-information/vaborem-epar-product-information_it.pdf (accessed on 25 March 2023).
- Recarbrio. Available online: https://www.ema.europa.eu/en/documents/product-information/recarbrio-epar-product-information_it.pdf (accessed on 25 March 2023).
- Zerbaxa. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zerbaxa (accessed on 25 March 2023).
- Fetcroja. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/fetcroja (accessed on 25 March 2023).
- Zinforo. Available online: https://www.ema.europa.eu/en/documents/product-information/zinforo-epar-product-information_en.pdf (accessed on 25 March 2023).
- Xydalba. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/xydalba (accessed on 25 March 2023).
- Tenkasi (previously Orbactiv). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tenkasi-previously-orbactiv (accessed on 18 May 2023).
- VIBATIV (telavancin) for Injection. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/022407_vibativ_toc.cfm (accessed on 18 May 2023).
- Sivextro. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/sivextro (accessed on 18 May 2023).
- Zeftera. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zeftera-previously-zevtera (accessed on 18 May 2023).
- Xerava. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/xerava (accessed on 18 May 2023).
- Bradley, J.S.; Armstrong, J.; Arrieta, A.; Bishai, R.; Das, S.; Delair, S.; Edeki, T.; Holmes, W.C.; Li, J.; Moffett, K.S.; et al. Phase I Study Assessing the Pharmacokinetic Profile, Safety, and Tolerability of a Single Dose of Ceftazidime-Avibactam in Hospitalized Pediatric Patients. Antimicrob. Agents Chemother. 2016, 60, 6252–6259. [Google Scholar] [CrossRef]
- Tamma, P.D.; Fan, Y.; Bergman, Y.; Sick-Samuel, A.C.; Hsu, A.J.; Timp, W.; Simner, P.J.; Prokesch, B.C.; Greenberg, D.E. Successful Treatment of Persistent Burkholderia cepacia Complex Bacteremia with Ceftazidime-Avibactam. Antimicrob. Agents Chemother. 2018, 62, e02213-17. [Google Scholar] [CrossRef]
- Iosifidis, E.; Chorafa, E.; Agakidou, E.; Kontou, A.; Violaki, A.; Volakli, E.; Christou, E.I.; Zarras, C.; Drossou-Agakidou, V.; Sdougka, M.; et al. Use of Ceftazidime-avibactam for the Treatment of Extensively drug-resistant or Pan drug-resistant Klebsiella pneumoniae in Neonates and Children <5 Years of Age. Pediatr. Infect. Dis. J. 2019, 38, 812–815. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Roilides, E.; Broadhurst, H.; Cheng, K.; Huang, L.; MasCasullo, V.; Newell, P.; Stone, G.G.; Tawadrous, M.; Wajsbrot, D.; et al. Safety and Efficacy of Ceftazidime-Avibactam in the Treatment of Children ≥3 Months to <18 Years with Complicated Urinary Tract Infection: Results from a Phase 2 Randomized, Controlled Trial. Pediatr. Infect. Dis. J. 2019, 38, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Broadhurst, H.; Cheng, K.; Mendez, M.; Newell, P.; Prchlik, M.; Stone, G.G.; Talley, A.K.; Tawadrous, M.; Wajsbrot, D.; et al. Safety and Efficacy of Ceftazidime-Avibactam Plus Metronidazole in the Treatment of Children ≥3 Months to <18 Years with Complicated Intra-Abdominal Infection: Results from a Phase 2, Randomized, Controlled Trial. Pediatr. Infect. Dis. J. 2019, 38, 816–824. [Google Scholar] [CrossRef]
- Esposito, P.; Sbrana, F.; Di Toro, A.; Gombos, S.; Tascini, C. Ceftazidine-avibactam salvage therapy in newborn with KPC-producing Klebsiella pneumoniae invasive infections. Minerva Anestesiol. 2019, 85, 804–805. [Google Scholar] [CrossRef]
- Vargas, M.; Buonomo, A.R.; Buonanno, P.; Iacovazzo, C.; Servillo, G. Successful treatment of KPC-MDR septic shock with ceftazidime-avibactam in a pediatric critically ill patient. IDCases 2019, 18, e00634. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Condren, M.; Walter, J. Ceftazidime-avibactam for the treatment of multidrug resistant Burkholderia cepacia complex in a pediatric cystic fibrosis patient. Pediatr. Pulmonol. 2020, 55, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.A.; Bonacorsi, S.; Fahd, M.; Baruchel, A.; Cointe, A.; Poey, N.; Jacquier, H.; Doit, C.; Monjault, A.; Tenaillon, O.; et al. Successful Treatment of Bacteremia Due to NDM-1-Producing Morganella morganii with Aztreonam and Ceftazidime-Avibactam Combination in a Pediatric Patient with Hematologic Malignancy. Antimicrob. Agents Chemother. 2019, 63, e02463-18. [Google Scholar] [CrossRef] [PubMed]
- Coskun, I.; Atici, S. Successful Treatment of Pandrug-resistant Klebsiella pneumoniae Infection with Ceftazidime-avibactam in a Preterm Infant: A Case Report. Pediatr. Infect. Dis. J. 2020, 39, 854–856. [Google Scholar] [CrossRef]
- Ji, Z.; Sun, K.; Li, Z.; Cheng, W.; Yang, J. Carbapenem-Resistant Klebsiella pneumoniae Osteomyelitis Treated with Ceftazidime-Avibactam in an Infant: A Case Report. Infect. Drug Resist. 2021, 14, 3109–3113. [Google Scholar] [CrossRef]
- Franzese, R.C.; McFadyen, L.; Watson, K.J.; Ricobene, T.; Carrothers, T.J.; Vourvahis, M.; Chan, P.L.S.; Raber, S.; Bradley, J.S.; Lovern, M. Population Pharmacokinetic Modeling and Probability of Pharmacodynamic Target Attainment for Ceftazidime-Avibactam in Pediatric Patients Aged 3 Months and Older. Clin. Pharmacol. Ther. 2022, 111, 635–645. [Google Scholar] [CrossRef]
- Asfour, S.; Alaklobi, F.A.; Abdelrahim, A.; Taha, M.Y.; Asfour, R.A.; Khalil, T.M.; Al-Mouqdad, M.M. Intravenous Ceftazidime-Avibactam in Extremely Premature Neonates with Carbapenem-Resistant Enterobacteriaceae: Two Case Report. J. Pediatr. Pharmacol. Ther. 2022, 27, 192–197. [Google Scholar] [CrossRef]
- Nascimento, A.; Passaro, M.F.; de S Silva, P.S.; Rodriguez, S.; Martins, M.K.; Oliveira, S.C.; Moriel, P.; Visacri, M.B. Off-Label Use of Ceftazidime-Avibactam in a Premature Infant with Multidrug-Resistant Klebsiella pneumoniae Infection: A Case Report. J. Pharm. Pract. 2022. [Google Scholar] [CrossRef] [PubMed]
- Almangour, T.A.; Alsubaie, S.; Ghonem, L.; Almohaini, H.A.; Bakheet, H.M.; Altweijri, I. Ceftazidime-avibactam for the Treatment of Multidrug-resistant Pseudomonas aeruginosa Central Nervous System Infection in Pediatric Patient: A Case Report. Pediatr. Infect. Dis. J. 2022, 41, 436–438. [Google Scholar] [CrossRef]
- Perruccio, K.; D’Amico, M.R.; Baretta, V.; Onofrillo, D.; carraro, F.; Calore, E.; Muggeo, P.; Colombini, A.; Zama, D.; Meazza, C.; et al. Ceftolozane/Tazobactam and Ceftazidime/Avibactam: An Italian Multi-center Retrospective Analysis of Safety and Efficacy in Children with Hematologic Malignancies and Multi-drug Resistant Gram-negative Bacteria Infections. Pediatr. Infect. Dis. J. 2022, 41, 994–996. [Google Scholar] [CrossRef]
- Aitken, S.L.; Kontoyiannis, D.P.; DePombo, A.M.; Bhatti, M.M.; Tverdek, F.P.; Gettys, S.C.; Nicolau, D.P.; Nunez, C.A. Use of Ceftolozane/Tazobactam in the Treatment of Multidrug-resistant Pseudomonas aeruginosa Bloodstream Infection in a Pediatric Leukemia Patient. Pediatr. Infect. Dis. J. 2016, 35, 1040–1042. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Ang, J.Y.; Arrieta, A.C.; Larson, K.B.; Rizk, M.L.; Caro, L.; Yang, S.; Yu, B.; Johnson, M.G.; Rhee, E.G. Pharmacokinetics and Safety of Single Intravenous Doses of Ceftolozane/Tazobactam in Children with Proven or Suspected Gram-Negative Infection. Pediatr. Infect. Dis. J. 2018, 37, 1130–1136. [Google Scholar] [CrossRef]
- Martin-Cazana, M.; Grau, S.; Epalza, C.; Branas, P.; Flores, M.; Olmedilla, M.; Blazquez-Gamero, D. Successful ceftolozane-tazobactam rescue therapy in a child with endocarditis caused by multidrug-resistant Pseudomonas aeruginosa. J. Pediatr. Child Health 2019, 55, 985–987. [Google Scholar] [CrossRef] [PubMed]
- Zikri, A.; el Masri, K. Use of Ceftolozane/tazobactam for the Treatment of Multidrug-resistant Pseudomonas aeruginosa Pneumonia in a Pediatric Patient with Combined Immunodeficiency (CID): A Case Report from a Tertiary Hospital in Saudi Arabia. Antibiotics 2019, 8, 67. [Google Scholar] [CrossRef]
- Ang, J.Y.; Arrieta, A.; Bradley, J.S.; Zhang, Z.; Yu, B.; Rizk, M.L.; Johnson, M.G.; Rhee, E.G. Ceftolozane/Tazobactam in Neonates and Young Infants: The Challenges of Collecting Pharmacokinetics and Safety Data in This Vulnerable Patient Population. Am. J. Perinatol. 2021, 38, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Larson, K.B.; Patel, Y.T.; Willavize, S.; Bradley, J.S.; Rhee, E.G.; Caro, L.; Rizk, M.L. Ceftolozane-Tazobactam Population Pharmacokinetics and Dose Selection for Further Clinical Evaluation in Pediatric Patients with Complicated Urinary Tract or Complicated Intra-abdominal Infections. Antimicrob. Agents Chemother. 2019, 63, e02578-18. [Google Scholar] [CrossRef]
- Molloy, L.; Abdulhamid, I.; Srivastava, R.; Ang, J.Y. Ceftolozane/Tazobactam Treatment of Multidrug-resistant Pseudomonas aeruginosa Infections in Children. Pediatr. Infect. Dis. J 2020, 39, 419–420. [Google Scholar] [CrossRef]
- Arrieta, A.C.; Ang, J.Y.; Zhang, Z.; Larson, K.B.; Yu, B.; Johnson, M.G.; Rhee, E.G.; Feng, E.H.; Rizk, M.L. Plasma pharmacokinetics of ceftolozane/tazobactam in pediatric patients with cystic fibrosis. Pediatr. Pulmonol. 2020, 55, 2025–2032. [Google Scholar] [CrossRef]
- Butragueno-Laiseca Troconiz, I.F.; Grau, S.; Campillo, N.; Garcia, X.; Padilla, B.; Fernandez, S.N.; Santiago, M.J. Finding the Dose for Ceftolozane-Tazobactam in Critically Ill Children with and without Acute Kidney Injury. Antibiotics 2020, 9, 887. [Google Scholar] [CrossRef]
- Roilides, E.; Ashouri, N.; Bradley, J.S.; Johnson, M.G.; Lonchar, J.M.; Su, F.H.M.; Huntington, J.A.; Popejoy, M.W.; Bensaci, M.; De Anda, C.; et al. Safety and Efficacy of Ceftolozane/Tazobactam Versus Meropenem in Neonates and Children with Complicated Urinary Tract Infection, Including Pyelonephritis: A Phase 2, Randomized Clinical Trial. Pediatr. Infect. Dis. J. 2023, 42, 292–298. [Google Scholar] [CrossRef]
- Jackson, C.A.; Newland, J.; Demetieva, N.; Lonchar, J.; Su, F.; Huntington, J.A.; Bensaci, M.; Popejoy, M.; Johnson, M.G.; De Anda, C.; et al. Safety and Efficacy of Ceftolozane/Tazobactam Plus Metronidazole Versus Meropenem from a Phase 2, Randomized Clinical Trial in Pediatric Participants with Complicated Intra-abdominal Infection. Pediatr. Infect. Dis. J. 2021, 8, 668–669. [Google Scholar] [CrossRef]
- Katsube, T.; Echols, R.; Wajima, T. Prediction of Cefiderocol Pharmacokinetics and Probability of Target Attainment in Pediatric Subjects for Proposing Dose Regimen. Open Forum Infect. Dis. 2019, 6 (Suppl. S2), S330–S331. [Google Scholar]
- Alamarat, Z.; Babic, J.; Tran, T.T.; Wootton, S.H.; Dinh, A.Q.; Miller, W.R.; Hanson, B.; Wanger, A.; Gary, J.L.; Arias, C.A.; et al. Long-Term Compassionate Use of Cefiderocol to Treat Chronic Osteomyelitis Caused by Extensively Drug-Resistant Pseudomonas aeruginosa and Extended-Spectrum-β-Lactamase-Producing Klebsiella pneumoniae in a Pediatric Patient. Antimicrob. Agents Chemother. 2020, 64, e01872-19. [Google Scholar] [CrossRef] [PubMed]
- Warner, C.; Bartelt, L.A.; Lachiewicz, A.M.; Tompkins, K.M.; Miller, M.B.; Alby, K.; Jones, M.B.; Carr, a.L.; Alexander, J.; Gainey, A.B.; et al. Cefiderocol for the Treatment of Adult and Pediatric Patients with Cystic Fibrosis and Achromobacter xylosoxidans Infections. Clin. Infect. Dis. 2021, 73, e1754–e1757. [Google Scholar] [CrossRef]
- Grasa, C.D.; Gomez-Gil, M.R.; Pacheco, S.S.R.; Del Rosal, T.; Moreno, F.; Gerig, N.; Fernandez, B.O.; Calvo, C.; Baquero-Artigao, F. Compassionate use of cefiderocol for VIM metallo-β-lactamase-producing Pseudomonas aeruginosa infection in a toddler with Burkitt lymphoma. J. Glob. Antimicrob. Resist. 2021, 26, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Bawankule, S.; Nabar, N.; Joshi, P.; Singhal, T. Cefiderocol as Salvage Therapy for Carbapenem-Resistant Klebsiella pneumoniae Sepsis in an Extremely Preterm Neonate. Indian. J. Pediatr. 2023, 90, 310. [Google Scholar] [CrossRef]
- Monari, C.; Spagnolo, F.; Piasaturo, M.; Ascione, S.; Donnarumma, G.; Calò, F.; Caredda, E.; Montella, F.; Maietta, A.; Montaldo, P.; et al. Bloodstream Infection Due to a VIM-Metallo-β-Lactamase-Producing Klebsiella pneumoniae Treated with Cefiderocol in a Preterm Newborn. Infect. Dis. Ther. 2023, 12, 727–734. [Google Scholar] [CrossRef]
- Hanretty, A.M.; Kaur, I.; Evangelista, A.T.; Moore, W.S.; Enache, A.; Chopra, A.; Cies, J.J. Pharmacokinetics of the Meropenem Component of Meropenem-Vaborbactam in the Treatment of KPC-Producing Klebsiella pneumoniae Bloodstream Infection in a Pediatric Patient. Pharmacotherapy 2018, 38, e87–e91. [Google Scholar] [CrossRef]
- Gainey, A.B.; Burch, A.K.; Brownstein, M.J.; Brown, D.E.; Fackler, J.; Horne, B.; Biswas, B.; Bivens, B.N.; Malagon, F.; Daniels, R. Combining bacteriophages with cefiderocol and meropenem/vaborbactam to treat a pan-drug resistant Achromobacter species infection in a pediatric cystic fibrosis patient. Pediatr. Pulmonol. 2020, 55, 2990–2994. [Google Scholar] [CrossRef]
- Cannavino, C.R.; Nemeth, A.; Korczowski, B.; Bradley, J.S.; O’Neal, T.; Jandourek, A.; Friedland, H.D.; Kaplan, S.L. A Randomized, Prospective Study of Pediatric Patients with Community-acquired Pneumonia Treated with Ceftaroline Versus Ceftriaxone. Pediatr. Infect. Dis. J. 2016, 35, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Blumer, J.; Ghonghadze, T.; Cannavino, C.; O’Neal, T.; Jandourek, A.; Friedland, H.D.; Bradley, J.S. A Multicenter, Randomized, Observer-blinded, Active-controlled Study Evaluating the Safety and Effectiveness of Ceftaroline Compared with Ceftriaxone Plus Vancomycin in Pediatric Patients with Complicated Community-acquired Bacterial Pneumonia. Pediatr. Infect. Dis. J. 2016, 35, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Korczowski, B.; Antadze, T.; Giorgobani, M.; Stryjewski, M.; Jandourek, A.; Smith, A.; O’Neal, T.; Bradley, J.S. A Multicenter, Randomized, Observer-blinded, Active-controlled Study to Evaluate the Safety and Efficacy of Ceftaroline Versus Comparator in Pediatric Patients with Acute Bacterial Skin and Skin Structure Infection. Pediatr. Infect. Dis. J. 2016, 35, e239–e247. [Google Scholar] [CrossRef]
- Riccobene, T.A.; Khariton, T.; Knebel, W.; Das, S.; Li, J.; Jandourek, A.; carrothers, T.J.; Bradley, J.S. Population PK Modeling and Target Attainment Simulations to Support Dosing of Ceftaroline Fosamil in Pediatric Patients with Acute Bacterial Skin and Skin Structure Infections and Community-Acquired Bacterial Pneumonia. J. Clin. Pharmacol. 2017, 57, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Salerno, S.N.; Bernhardt, J.; laughon, M.; Jhaveri, R.; Massaro, M.; Gonzales, D. Pharmacokinetics of Ceftaroline in a Preterm Infant with Methicillin-Resistant Staphylococcus Aureus Pneumonia. J. Pediatr. Infect. Dis. Soc. 2018, 7, 342–345. [Google Scholar] [CrossRef]
- Branstetter, J.; Searcy, H.; benner, K.; Yarbroug, A.; Crowder, C.; Troxler, B. Ceftaroline vs. vancomycin for the treatment of acute pulmonary exacerbations in pediatric patients with cystic fibrosis. Pediatr. Pulmonol. 2020, 55, 3337–3342. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Stone, G.G.; Chan, P.L.S.; Raber, S.R.; Riccobene, T.; Mas Casullo, V.; Yan, J.L.; Hendrick, V.M.; Hammond, J.; Leister-Tebbe, H. Phase 2 Study of the Safety, Pharmacokinetics and Efficacy of Ceftaroline Fosamil in Neonates and Very Young Infants with Late-onset Sepsis. Pediatr. Infect. Dis. J. 2020, 39, 411–418. [Google Scholar] [CrossRef]
- Ferguson, C.L.; Cowart, M.C.; Jordan-Villegas, A.; Laham, F. High-level ceftaroline resistance in a paediatric patient with invasive methicillin-resistant Staphylococcus aureus infection without previous ceftaroline exposure. J. Clin. Pharm. Ther. 2021, 46, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Heger, M.L.; Al-Sayyad, B. Ceftaroline and Daptomycin Combination Antibiotic Therapy for a Methicillin-Resistant Staphylococcus Aureus Liver Abscess in a Premature Infant. J. Pediatr. Pharmacol. Ther. 2022, 27, 754–759. [Google Scholar] [CrossRef]
- Chan, P.L.S.; McFadyen, L.; Quaye, A.; Leister-Tebbe, H.; Hendrick, V.M.; Hammond, J.; Raber, S. The use of extrapolation based on modeling and simulation to support high-dose regimens of ceftaroline fosamil in pediatric patients with complicated skin and soft-tissue infections. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 551–563. [Google Scholar] [CrossRef]
- Riccobene, T.A.; Carrothers, T.J.; Knebel, W.; Raber, s.; Chan, P.L.S. Pharmacokinetic and Pharmacodynamic Target Attainment in Adult and Pediatric Patients Following Administration of Ceftaroline Fosamil as a 5-Minute Infusion. Clin. Pharmacol. Drug Dev. 2021, 10, 420–427. [Google Scholar] [CrossRef]
- Bradley, J.S.; Puttagunta, S.; Rubino, C.M.; Blumer, J.L.; Dunne, M.; Sullivan, J.E. Pharmacokinetics, Safety and Tolerability of Single Dose Dalbavancin in Children 12–17 Years of Age. Pediatr. Infect. Dis. J. 2015, 34, 748–752. [Google Scholar] [CrossRef]
- Gonzalez, D.; Bradley, J.S.; Blumer, J.; Yogev, R.; Watt, K.V.; James, L.P.; Palazzi, D.L.; Bhatt-Metha, V.; Sullivan, J.E.; Zhang, L.; et al. Dalbavancin Pharmacokinetics and Safety in Children 3 Months to 11 Years of Age. Pediatr. Infect. Dis. J. 2017, 36, 645–653. [Google Scholar] [CrossRef]
- Carrothers, T.J.; Lagraauw, H.M.; Lindbom, L.; Riccobene, T.A. Population Pharmacokinetic and Pharmacokinetic/Pharmacodynamic Target Attainment Analyses for Dalbavancin in Pediatric Patients. Pediatr. Infect. Dis. J. 2023, 42, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Giorgobiani, M.; Burroughgs, M.H.; antadze, T.; carrothers, T.J.; Riccobene, T.A.; Patel, R.; Lin, T.; Stefanova, P. The Safety and Efficacy of Dalbavancin and Active Comparator in Pediatric Patients with Acute Bacterial Skin and Skin Structure Infections. Pediatr. Infect. Dis. J. 2023, 42, 199–205. [Google Scholar] [CrossRef]
- Karampatakis, T.; Tsergouli, K.; Lowrie, K. Efficacy and safety of ceftazidime-avibactam compared to other antimicrobials for the treatment of infections caused by carbapenem-resistant Klebsiella pneumoniae strains, a systematic review and meta-analysis. Microb. Pathog. 2023, 179, 106090. [Google Scholar] [CrossRef] [PubMed]
- Wagenlehner, F.M.; Umeh, O.; Steenbergen, J.; Yuan, G.; Darouiche, R.O. Ceftolozane tazobactam compared with levofloxacin in the treatment of complicated urinary-tract infections including pyelonephritis: A randomised, double-blind, phase 3 trial (ASPECTcUTI). Lancet 2015, 385, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.; Hershberger, E.; Miller, B.; Popejoy, M.; Friedland, I.; Steenbergen, J.; Yoon, M.; Collins, S.; Yuan, G.; Barie, P.S.; et al. Ceftolozane/tazobactam plus metronidazole for complicated intra-abdominal infections in an era of multidrug resistance: Results from a randomized, double-blind, phase 3 trial (ASPECT-cIAI). Clin. Infect. Dis. 2015, 60, 1462–1471. [Google Scholar] [CrossRef]
- Chi, Y.; Xu, J.; Bai, N.; Liang, B.; Cai, Y. The efficacy and safety of ceftolozane-tazobactam in the treatment of GNB infections: A systematic review and meta-analysis of clinical studies. Expert Rev. Anti-Infect. Ther. 2023, 21, 189–201. [Google Scholar] [CrossRef]
- Bassetti, M.; Echols, R.; Matsungnaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, t.; Niki, Y.; Paterson, d.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, R.G.; Matsunaga, Y.; Ariyasu, M.; Clevenbergh, P.; Echols, R.; Kaye, K.S.; Kollef, M.; Menon, A.; Pogue, J.M.; Shorr, A.F.; et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): A randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2021, 21, 213–225. [Google Scholar] [CrossRef]
- Timsit, J.F.; Paul, M.; Shields, R.; Echols, R.; Baba, T.; Yamano, Y.; Portsmouth, S. Cefiderocol for the Treatment of Infections Due to Metallo-B-lactamase-Producing Pathogens in the CREDIBLE-CR and APEKS-NP Phase 3 Randomized Studies. Clin. Infect. Dis. 2022, 75, 1081–1084. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, r.A.; Mathers, a.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P). Clin. Infect. Dis. 2022, 75, 187–212. [Google Scholar] [CrossRef]
- Lan, S.H.; Chang, S.P.; Lai, C.C.; Lu, L.C.; Chao, C.M. Efficacy and Safety of Ceftaroline for the Treatment of Community-Acquired Pneumonia: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 824. [Google Scholar] [CrossRef] [PubMed]
- Zasowski, E.J.; Trinh, T.D.; Claeys, K.C.; Lagnf, A.M.; Bathia, s.; Klinker, K.P.; Veve, M.P.; Estrada, S.J.; Johns, S.T.; Sawyer, A.T.; et al. Multicenter cohort study of ceftaroline versus daptomycin for the treatment of methicicllin-resistant Staphylococcus aureus bloodstream infection. Open Forum Infect Dis. 2021, 9, ofab606. [Google Scholar] [CrossRef]
- Wilcox, M.H.; Corey, G.R.; Talbot, G.H.; Thye, D.; Friedland, D.; Baculik, t.; CANVAS 2 investigators. CANVAS 2: The second Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65 (Suppl. S4), iv53–iv65. [Google Scholar] [CrossRef] [PubMed]
- Corrado, M.L. Integrated safety summary of CANVAS 1 and 2 trials: Phase III, randomized, double-blind studies evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. Antimicrob. Chemother. 2010, 65 (Suppl. S4), iv67–iv71. [Google Scholar] [CrossRef]
- Corey, G.R.; Wilcox, M.H.; Talbot, G.H.; Thye, D.; Friedlan, D.; Baculik, T.; CANVAS 1 investigators. CANVAS 1: The first Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65 (Suppl. S4), iv41–iv51. [Google Scholar] [CrossRef]
- Al-Sweih, N.; Jamal, W.; Mokaddas, E.; Habashy, N.; Kurdi, A.; Mohamed, N. Evaluation of the in vitro activity of ceftaroline, ceftazidime/avibactam and comparator antimicrobial agents against clinical isolates from paediatric patients in Kuwait: ATLAS data 2012-19. JAC Antimicrob. Resist. 2021, 3, dlab159. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.Y.; Riccobene, T.; Debabov, D. Antimicrobial Activity of Ceftazidime-Avibactam Against Contemporary Pathogens from Urinary Tract Infections and Intra-abdominal Infections Collected from US Children During the 2016–2019 INFORM Surveillance Program Pediatr. Infect. Dis. J. 2021, 40, 338–343. [Google Scholar] [CrossRef]
- Marner, M.; Kolberg, L.; Horst, J.; Bohringer, N.; Hubner, J.; Kresna, I.D.M.; Liu, Y.; Mettal, U.; Wang, L.; Meyer-Buhn, M.; et al. Antimicrobial Activity of Ceftazidime-Avibactam, Ceftolozane-Tazobactam, Cefiderocol, and Novel Darobactin Analogs against Multidrug-Resistant Pseudomonas aeruginosa Isolates from Pediatric and Adolescent Cystic Fibrosis Patients. Microbiol. Spectr. 2023, 11, e0443722. [Google Scholar] [CrossRef] [PubMed]
- Shortbridge, D.; Duncan, L.; Pfaller, R.D.; Pfaller, M.A.; Flamm, R.K. Activity of ceftolozane-tazobactam and comparators when tested against Gram-negative isolates collected from paediatric patients in the USA and Europe between 2012 and 2016 as part of a global surveillance programme. Int. J. Antimicrob. Agents 2019, 53, 637–643. [Google Scholar] [CrossRef]
- Kanwar, N.; Harrison, C.J.; Pence, M.A.; Qin, X.; Selvarangan, R. Comparative in vitro antipseudomonal activity of ceftolozane/tazobactam against Pseudomonas aeruginosa isolates from children with cystic fibrosis. Diagn. Microbiol. Infect. Dis. 2023, 105, 115904. [Google Scholar] [CrossRef]
- Kanwar, N.; Banerjee, D.; Harrison, C.J.; Newland, J.G.; Qin, X.; Zerr, D.M.; Zaotis, T.; Selvarangan, R. Comparative in vitro effectiveness of ceftolozane/tazobactam against pediatric gram-negative drug-resistant isolates. J. Chemother. 2021, 33, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Mendes, R.E.; Castanheira, M.; Flamm, R.K.; Jones, R.N.; Sader, H.S. Ceftaroline Activity Tested Against Bacterial Isolates Causing Community-acquired Respiratory Tract Infections and Skin and Skin Structure Infections in Pediatric Patients from United States Hospitals: 2012–2014. Pediatr. Infect. Dis. J. 2017, 36, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Touw, D.J.; van den Anker, J.N. Therapeutic Drug Monitoring of Antimicrobial Drugs in Neonates: An Opinion Article. Ther. Drug Monit. 2022, 44, 65–74. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study Type | Country | Patient Characteristics | N | Organisms | Study Intervention | Outcomes | |
|---|---|---|---|---|---|---|---|
| Bradley 2016 [57] | Phase I Pharmacokinetics | US | 3 month–2 years | 8 | n.p. | 50 mg/kg Single 2 h infusion | Pharmacokinetics model validation 1/8 drug-related mild AEs (sinus tachycardia) |
| Tamma 2018 [58] | Case report | US | 2 month BSI | 1 | Burkholderia cepacia | 50 mg/kg q8h Continuous infusion Duration: 6 weeks | 1/1 BC sterilization 1/1 clinical recovery No drug-related AEs |
| Iosifidis 2019 [59] | Case series | Greece | Newborns including preterm, LOS | 6 | XDR or PDR Klebsiella pneumoniae | 50 mg/kg q8h Duration: 4–38 days (median 14 d) | 6/6 BC sterilization 6/6 clinical recovery No drug-related AEs |
| Bradley 2019 [60] | Phase II RCT | US | 3 month–2 years UTI | 95 | Enterobacterales | Randomization 3:1 to C/A 40–50 mg/kg q8h or cefepime Duration: ≥72 h | In C/A group: 17/22 urine sterilization 21/22 clinical recovery No drug-related AEs |
| Bradley 2019 [61] | Phase II RCT | US | 3 month–18 years complicated intra-abdominal infection | 83 | Escherichia coli Pseudomonas aeruginosa | Randomization 3:1 to C/A 40–50 mg/kg q8h + metronidazole or MEM Duration: ≥72 h | In C/A group: 57/61 clinical recovery No drug-related AEs |
| Esposito 2019 [62] | Case report | Italy | Preterm infant BW 680 g, LOS + meningitidis (30 DOL) | 1 | KPC-producing Klebsiella pneumoniae | 75 mg/kg q8h Duration: 47 days | 1/1 BC sterilization 1/1 clinical recovery 1/1 uncertain mild drug-related AE (thrombocytopenia) |
| Vargas 2019 [63] | Case report | Italy | 14 years BSI and pneumonia | 1 | MDR Klebsiella pneumoniae | 2.5 g q8h Duration: 14 days | 1/1 Clinical cure No drug-related AEs |
| Nguyem 2019 [64] | Case report | US | 16 years CF Pulmonary exacerbation | 1 | Burkholderia cepacia | 2.5 g q8h Duration: 14 days | 1/1 Sputum sterilization 1/1 Clinical cure No drug-related AEs |
| Hobson 2019 [65] | Case report | France | 3 years BSI in acute leukemia | 1 | MDR Morganella morganii | 150 mg/kg/d Duration: n.p. | 1/1 BC sterilization 1/1 Clinical cure No drug-related AEs |
| Coskum 2020 [66] | Case report | Turkey | Preterm infant GA 27 weeks, UTI (25 DOL) | 1 | PDR Klebsiella pneumoniae | 40 mg/kg q8h Duration: 10 days | 1/1 urine sterilization 1/1 clinical recovery 1/1 uncertain mild drug-related AE (glycosuria) |
| Ji 2021 [67] | Case report | China | 2 month Shoulder osteomyelitis | 1 | CR Klebsiella pneumoniae | 200 mg q8h Duration: 14 days | 1/1 clinical recovery No drug-related AEs |
| Franzese 2021 [68] | Pharmacokinetics | US | 3 month–18 years | 153 | n.p. | 40 mg/kg for infants < 6 month Single 2 h infusion | Pharmacokinetic model validation |
| Asfour 2022 [69] | Case series | Saudi Arabia | Preterm infants GA 27–28 weeks LOS + meningitidis (DOL 11) LOS (DOL 37) | 2 | CR Klebsiella pneumoniae | 50 mg/kg q8h Duration: 5–21 days | 2/2 BC sterilization 1/2 clinical recovery 1/2 death No drug-related AEs |
| Nascimento 2022 [70] | Case report | Brazil | Preterm infant GA 29 weeks LOS (46 DOL) | 1 | MDR Klebsiella pneumoniae | 40 mg/kg q8h Duration: 14 days | 1/1 BC sterilization 1/1 clinical recovery No drug-related AEs |
| Almangour 2022 [71] | Case report | Saudi Arabia | 2 years Ventriculoperitoneal shunt infection | 1 | MDR Pseudomonas aeruginosa | 62.5 mg/kg q8h Duration: 21 days | 1/1 CSF sterilization 1/1 Clinical cure No drug-related AEs |
| Perruccio 2022 [72] | Case series | Italy | 7 month–17 years Malignancy BSI, pneumonia, appendicitis | 21 (+4 C/T) | MDR Enterobacterales | 50mg/kg q8h Duration: 6–19 days | 23/25 Clinical cure 2/25 Death No drug-related AEs |
| Study Type | Country | Patient Characteristics | N | Organisms | Study Intervention | Outcomes | |
|---|---|---|---|---|---|---|---|
| Aitken 2016 [73] | Case report | US | 9 years BSI in acute leukemia | 1 | MDR P. aeruginosa | 1st course: 50 mg/kg q8h Duration: 3 weeks 2nd course: 40 mg 7 Kg q6h Duration: 3 weeks | 1/1 BC sterilization (relapse after 1st course) 1/1 Clinical cure (relapse after 1st course) No drug-related AEs |
| Bradley 2018 [74] | Phase I Pharmacokinetics | US | >7 days <18 years | 34 | Proven or suspected Gram neg infection | 20 mg/kg for pts 7d–3 month Single 1 h infusion | Pharmacokinetics model validation No drug-related AEs |
| Martin-Cazana 2019 [75] | Case report | Spain | 5 years BSI and endocarditis in congenital heart disease | 1 | MDR P. aeruginosa | 50 mg/kg q8h Extended infusion (3 h) Duration: 6 weeks | 1/1 BC sterilization 1/1 Clinical cure No drug-related AEs |
| Zikri 2019 [76] | Case report | Saudi Arabia | 14 years BSI and pneumonia in immunodeficiency | 1 | MDR P. aeruginosa | 1.5 g q8h Duration: n.p. | 1/1 Clinical cure No drug-related AEs |
| Ang 2019 [77] | Phase I Pharmacokinetics | US | >7 days <3 month | 13 | Proven or suspected Gram neg infection | 20 mg/kg Single 1 h infusion | Pharmacokinetics model validation No drug-related AEs |
| Larson 2020 [78] | Pharmacokinetics | US | simulation model (0–18 years) | — | — | — | Recommended doses: 20 mg/kg q8h (birth–12 years) |
| Molloy 2020 [79] | Case series | US | 3 month–19 years | 13 | MDR P. aeruginosa (7 pneumonia, 3 CF, 2 abdominal infections, 1 osteomyelitis) | 20 mg/kg q8h Duration: up to 8 weeks | 12/13 clinical cure 2/13 uncertain drug-related AEs (transaminitis, neutropenia) No drug-related AEs in pts < 1 years |
| Arrieta 2020 [80] | Pharmacokinetics | US | 2–18 years CF Respiratory disease | 18 | n.p. | 18–30 mg/kg (2–7 years) | 100% target attainment probability No differences CF vs. non-CF |
| Butragueno-Laiseca 2020 [81] | Pharmacokinetics | US | 9–19 month CF | 3 | MDR P. aeruginosa | 30–40 mg/kg q8h | Recommended doses: 35 mg/kg q8h if normal renal function 10 mg/kg q8h if acute renal injury 30 mg/kg if renal replacement therapy |
| Perruccio 2022 [72] | Case series | Italy | 7 month–17 years Malignancy BSI, pneumonia, appendicitis | 4 (+21C/A) | MDR Enterobacterales | 1g q8h Duration: 14–20 days | 23/25 Clinical cure 2/25 Death No drug-related AEs |
| Roiledes 2023 [82] | Phase II RCT | US/Europe | 7d–18 years Complicated UTI | 95 | E. coli K. pneumoniae P. aeruginosa | Randomization 3:1 to C/T 20 mg/kg q8h or MEM Duration: 7–14 days | 94% vs. 80% clinical cure 14% mild drug-related AEs (diarrhea, increased transaminases, neutropenia) No severe drug-related AEs |
| Jackson 2023 [83] | Phase II RCT | US/Europe | 0–18 years Complicated intra-abdominal infection | 91 | E. coli | Randomization to C/T 20 mg/kg q8h + metronidazole or MEM | Clinical cure: 80 vs. 95% In C/T group: 13/70 mild drug-related AEs (diarrhea, increased transaminases, increased alkaline phosphatase, vaginal mycosis, dysgeusia) No sere drug-related AEs |
| Antibiotic | Study Type | Country | Patient Characteristics | N | Organisms | Study Intervention | Outcomes | |
|---|---|---|---|---|---|---|---|---|
| Katsube 2019 [84] | Cefiderocol | Pharmacokinetics | Japan | simulation model (0–18 years) | — | — | — | Recommended doses: GA < 32 weeks: <2 month 30 mg/kg q8h >2 month 40 mg/kg q8h GA ≥ 32 weeks: <2 month 40 mg/kg q8h >2 month 60 mg/kg q8h |
| Alamarat 2020 [85] | Cefiderocol | Case report | US | 15 years Chronic osteomyelitis | 1 | XDR P. aeruginosa + ESBL producing K. pneumoniae | 2g q8h Extended infusion (3 h) Duration: 14 weeks (+surgery) | 1/1 Bone biopsy specimen sterilization 1/1 Clinical cure No drug-related AEs |
| Warner 2021 [86] | Cefiderocol | Case series | US | 0–18 years CF Pulmonary exacerbation | 2 | Achromobacter xylosoxidans | 60 mg/kg q8h | 2/2 clinical recovery 1/2 relapse No drug-related AEs |
| Grasa 2021 [87] | Cefiderocol | Case report | Spain | 2 years BSI in Burkitt lymphoma | 1 | Carbapenemase-producing P. aeruginosa | 60 mg/kg q8h Duration: 7 days | 1/1 Clinical cure No drug-related AEs |
| Bawankule 2022 [88] | Cefiderocol | Case report | India | Preterm 27 weeks GA DOL 9 LOS + NEC | 1 | KPC-producing K. pneumoniae | 30 mg/kg q6h Duration: 14 days | 1/1 BC sterilization 1/1 clinical recovery No drug-related AEs |
| Monari 2023 [89] | Cefiderocol | Case report | Italy | Preterm 31 weeks GA DOL 20 LOS | 1 | KPC-producing K. pneumoniae | 60 mg/kg loading dose 40 mg/kg q8h Extended infusion (3–4 h) Duration: 9 days | 1/1 BC sterilization 1/1 clinical recovery No drug-related AEs |
| Henretty 2018 [90] | Meropenem/Vaborvactam | Case report Pharmacokinetics | US | 4 years CLABSI | 1 | KPC-producing K. pneumoniae | 40 mg/kg q6h, 3 h infusion Duration: 14 days | 1/1 BC sterilization 1/1 Clinical cure 100% MEM concentration > MIC |
| Gainey 2020 [91] | Meropenem/Vaborvactam +Cefiderocol +bacteriophage | Case report | US | 10 years CF | 1 | Achromobacter spp. resistant to FDC and M/V | Duration: 14 days | 1/1 Sputum sterilization 1/1 Clinical cure |
| Antibiotic | Study Type | Country | Patient Characteristics | N | Organisms | Study Intervention | Outcomes | |
|---|---|---|---|---|---|---|---|---|
| Cannavino 2016 [92] | Ceftaroline | RCT | US, Europe | 2 month–17 years, CABP | 160 | 8 mg/kg q8h (2–6 month) 1 h infusion Duration: | 92% clinical cure 10% drug-related AEs (diarrhea, vomiting) | |
| Blumer 2016 [93] | Ceftaroline | RCT | US | 2 month–18 years Complicated CABP | 38 2 month–2 years: 6 | 3/29 MSSA 1/29 MRSA Others: S. pneumonia, S. pyogenes, H. Influenzae, P. aeruginosa | Randomization 3:1 to ceftaroline 10 mg/kg q8h (2–6 month) or ceftriaxone+ vancomycin Duration: 3–19 days | In ceftaroline group: 24/29 clinical cure 7/30 drug-related AEs (vomiting, diarrhea, increased AST/ALT, dermatitis, rush) |
| Korczowski 2016 [94] | Ceftaroline | RCT | US, Europe, South America, Africa | 2 month–17 years SSSI | 159 | Mostly S. aureus (42% MRSA) | Randomization 2:1 to ceftaroline 8 mg/kg q8h (2–6 month) or comparator (cefazolin or vancomycin) Duration: 5–14 days | 96% clinical cure 94% microbiological eradication MRSA 89% microbiological eradication |
| Riccobene 2017 [95] | Ceftaroline | Pharmacokinetics | US | — simulation model (0–18 years) | — | — | — | 8 mg/kg q8h (2 month–2 years) has >97% probability of target attainment |
| Salerno 2018 [96] | Ceftaroline | Case report | US | Preterm 24 weeks GA DOL 43 LOS and pneumonia | 1 | MRSA | 8.5 mg/kg q8h Duration: 21 days | 1/1 BC sterilization 1/1 clinical cure No drug-related AEs Pharmacokinetics target attained |
| Branstetter 2020 [97] | Ceftaroline | Retrospective | US | 0–21 years CF pulmonary exacerbation | 90* | 71/90 MRSA 21/90 Pseudomonas coinfection | Randomization 1:1 to ceftaroline or vancomycin Doses and duration not reported | No differences in lung function and readmission rate |
| Bradley 2020 [98] | Ceftaroline | Phase II | US | 7–60 d, LOS | 11 | E. coli Staphyloccocus spp. | 4–6 mg/kg q8h, 1h infusion Duration: 2–14 days | 0/11 clinical failure 1/11 mild AE (diarrhea) Pharmacokinetic target attainment probability > 95% |
| Ferguson 2020 [99] | Ceftaroline | Case report | 20 month BSI, wound infection, endocarditis, septic pulmonary emboli | 1 | MRSA | 8 mg/kg q6h Duration: 1 days (shifted to vancomycin) | Resistance to ceftaroline despite no previous exposure | |
| Heger 2022 [100] | Ceftaroline | Case report | US | Preterm GA 30 weeks DOL 54 Hepatic abscess and infected portal thrombus | 1 | MRSA | 8 mg/kg q8h Duration: 18 days | 1/1 clinical cure No drug-related AEs |
| Chan 2021 [101] | Ceftaroline | Pharmacokinetics | US | simulation model (0–18 years) | — | — | — | 10 mg/kg q8h (2 month–2 years) has 99% probability of target attainment |
| Riccobene 2021 [102] | Ceftaroline | Pharmacokinetics | US | simulation model 2 month–18 years | — | — | — | 5 min or 60 min infusion have >99% probability of target attainment |
| Bradley 2015 [103] | Dalbavancin | Pharmacokinetics | US | 12–17 years | 10 | n.p. | 15 mg/kg single dose | Slightly lower exposure than adults given 1 g |
| Gonzalez 2017 [104] | Dalbavancin | Phase I Pharmacokinetics | US | 3 month–11 years Suspected or confirmed bacterial infection | 43 | n.p. | — | Recommended regimens 3 month–6 years: 15 mg/kg day 1 + 7.5 mg/kg day 8 OR 22.5 mg/kg day 1 5 probable drug-related AEs (rash, dermatitis, urticaria, elevated liver enzymes); no drug-related severe AEs |
| Carrothers 2023 [105] | Dalbavancin | Pharmacokinetics | US | — simulation model 0–18 years SSSI, neonatal sepsis | 211 | n.p. | — | 22.5 mg/kg 30 min single infusion has probability of target attainment >94% |
| Giorgobiani 2023 [106] | Dalbavancin | Phase III RCT | US | 0–18 years SSSI 0–3 month BSI | 191 (0–3 month: 5) | S. aureus, S. pyogenes, S. mitis/S. oralis, E. faecalis | Randomization 3:3:1 to DAL 1 dose or DAL 2 doses or comparator (<3 month: DAL 1 dose 18 mg/kg or comparator) 30 min infusion Duration | Clinical cure 97 vs. 99 vs. 89% No drug-related AEs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poggi, C.; Dani, C. New Antimicrobials for the Treatment of Neonatal Sepsis Caused by Multi-Drug-Resistant Bacteria: A Systematic Review. Antibiotics 2023, 12, 956. https://doi.org/10.3390/antibiotics12060956
Poggi C, Dani C. New Antimicrobials for the Treatment of Neonatal Sepsis Caused by Multi-Drug-Resistant Bacteria: A Systematic Review. Antibiotics. 2023; 12(6):956. https://doi.org/10.3390/antibiotics12060956
Chicago/Turabian StylePoggi, Chiara, and Carlo Dani. 2023. "New Antimicrobials for the Treatment of Neonatal Sepsis Caused by Multi-Drug-Resistant Bacteria: A Systematic Review" Antibiotics 12, no. 6: 956. https://doi.org/10.3390/antibiotics12060956