

SWOT and Root Cause Analyses of Antimicrobial Resistance to Oral Antimicrobial Treatment of Cystitis

Abstract
1. Introduction
2. Antimicrobial Resistance (AMR)
Contribution of Urinary Tract Infections (UTIs) to AMR
3. The Urinary Bladder
4. Cystitis Etiology and Treatment
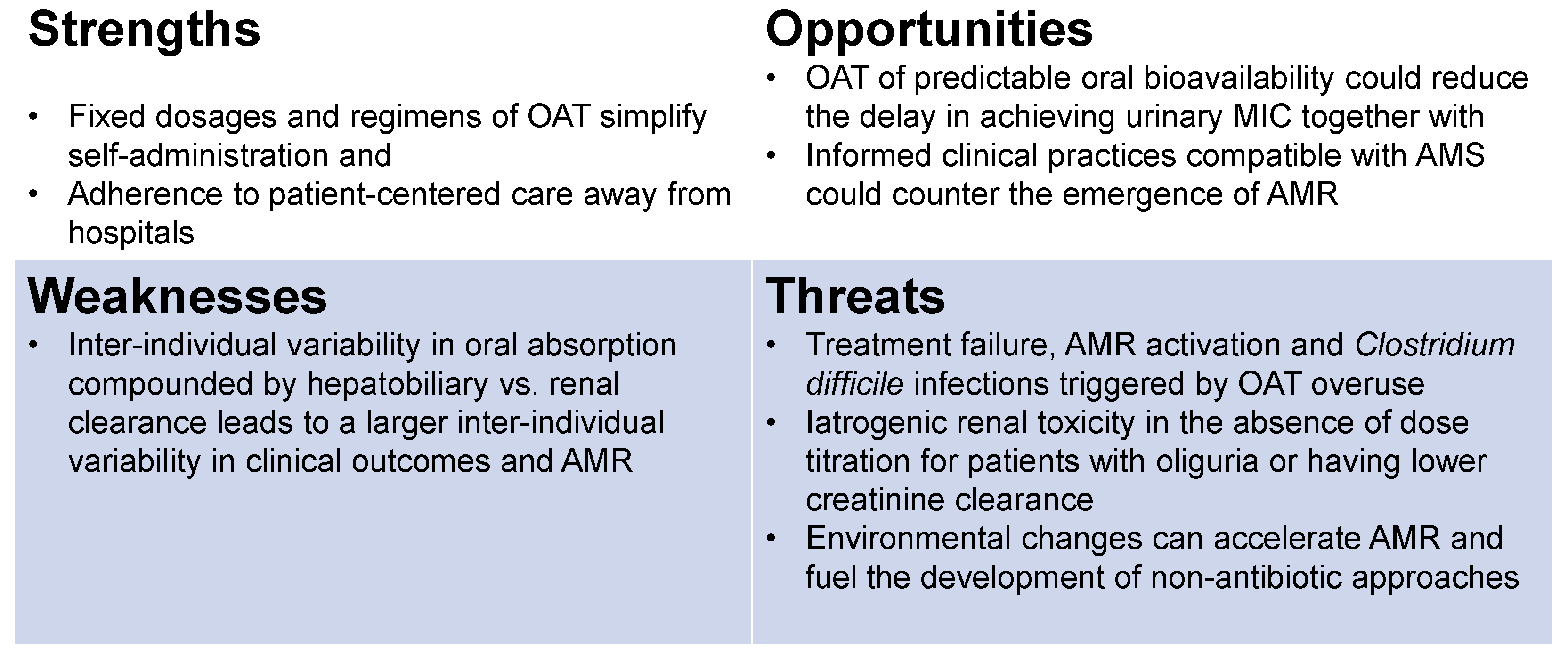
4.1. SWOTs of Oral Antimicrobial Therapy (OAT) for Cystitis
Volume of Distribution (Vd) and Clearance of OAT
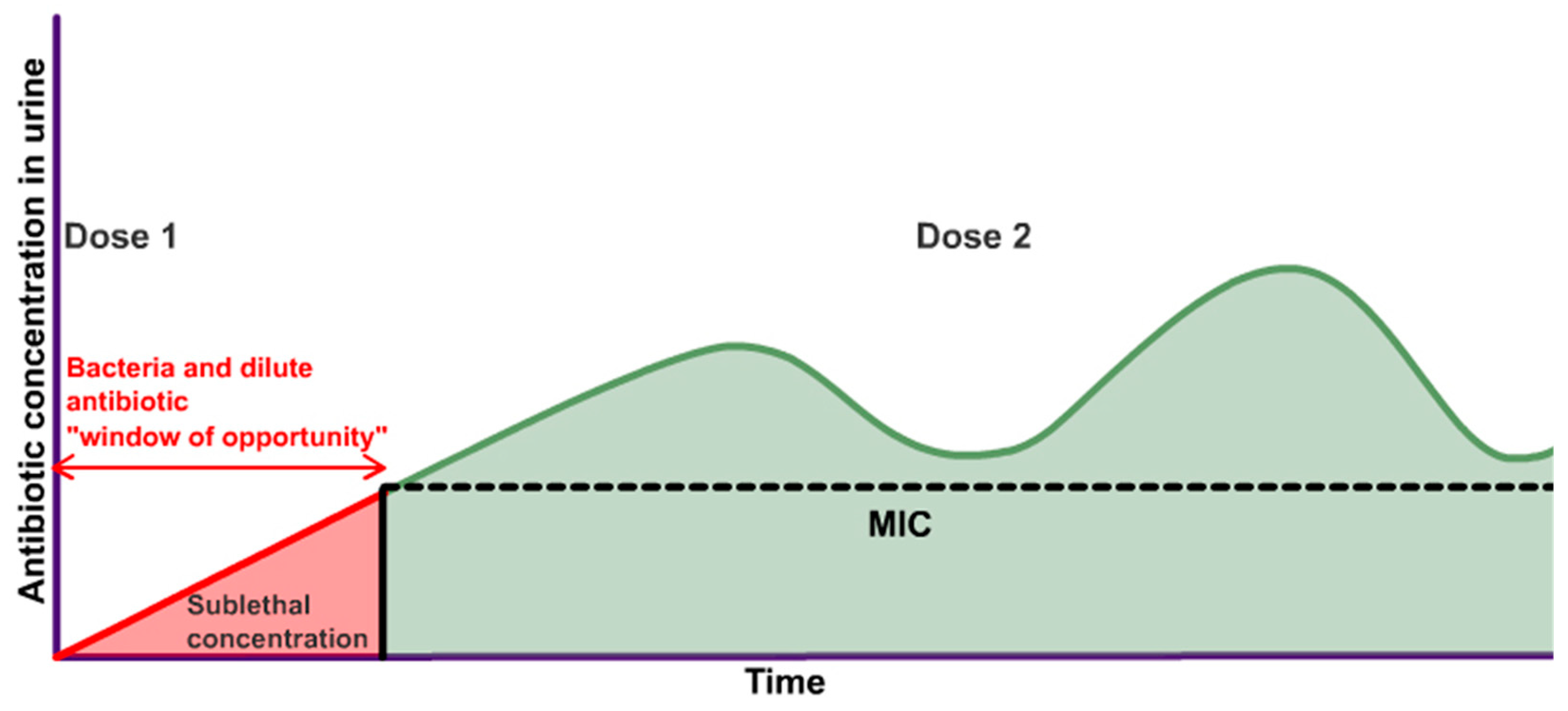
4.2. Root Cause Analysis of AMR—Delay and Variability in Urinary MIC
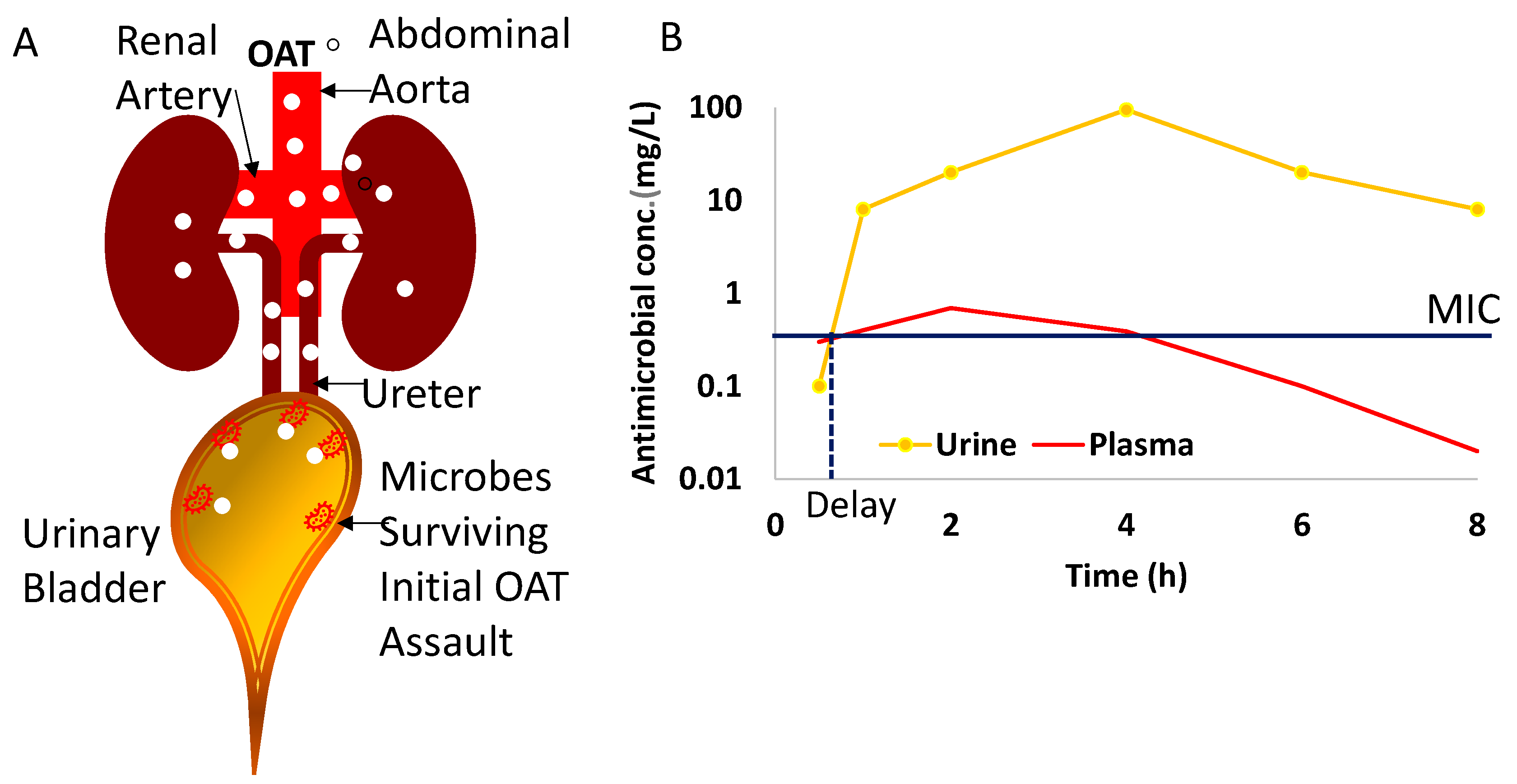
- The variability in the initial drug concentration due to variable absorption from the gut [25,32,96,97,98,99,100,101,102,103], hepatobiliary vs. renal clearance delaying the achievement of the MIC in urine [20,23,28,30,87,101,105,109], and variability in urine in-flow rate of 0.3–15 mL/min (~50× difference) [26,56] could reduce the delay in achieving the urinary MIC;
5. Discussion
- (1)
- (2)
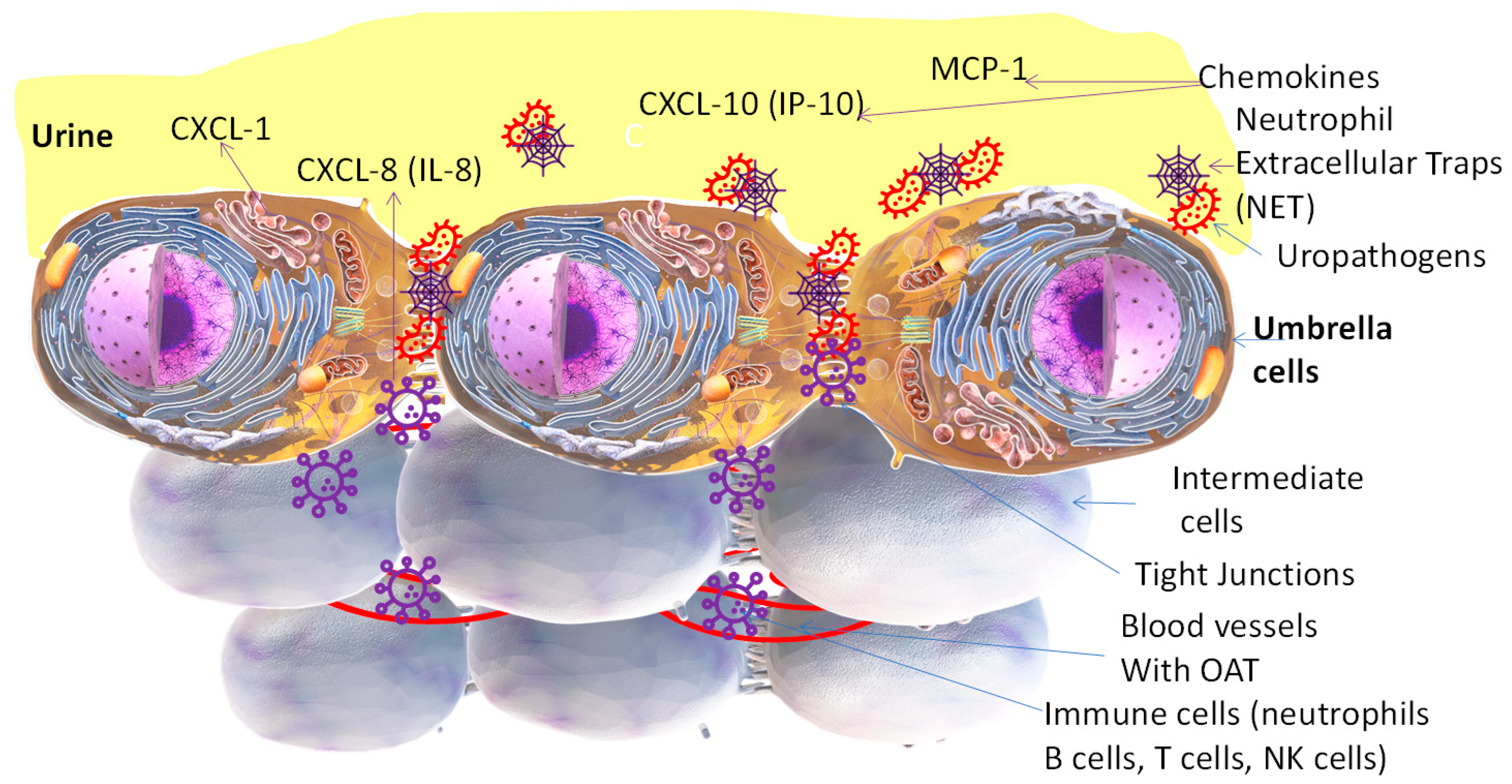
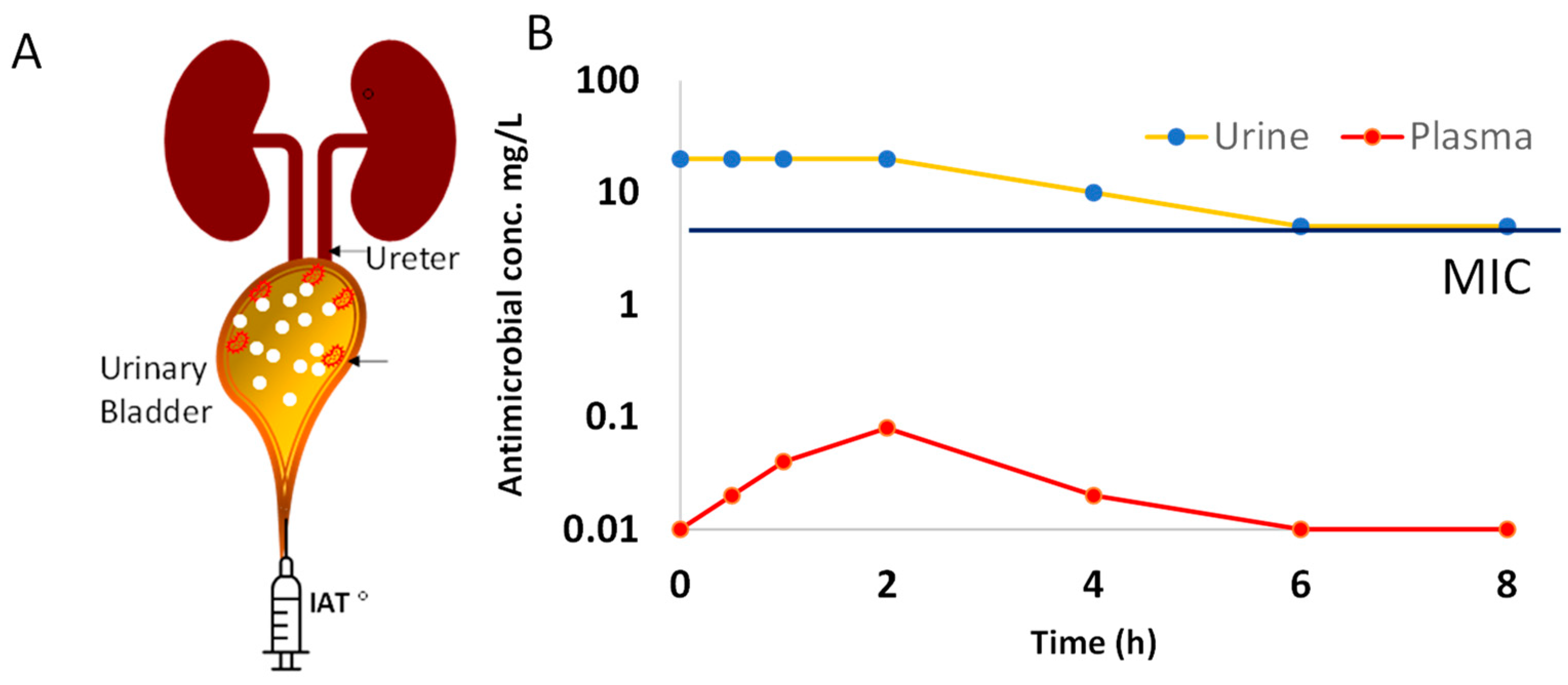
- Interchangeable use of the term UTI and cystitis. While absorbed OAT can reach pathogens in upper urinary tracts via perfused blood, the uropathogens causing cystitis can only be eliminated by the urinary fraction of absorbed OAT (Figure 2), because the circulating levels [126,127,130] of the drug are less likely to reach the planktonic microbes and those attaching to the apical side of umbrella cells (Figure 1);
- (3)
- (4)
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeLong, E.F.; Pace, N.R. Environmental diversity of bacteria and archaea. Syst. Biol. 2001, 50, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Reysenbach, A.L.; Shock, E. Merging genomes with geochemistry in hydrothermal ecosystems. Science 2002, 296, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.N.T.; Gorrell, R.; Kwok, T.; Connallon, T.; McDonald, M.J. Horizontal gene transfer facilitates the molecular reverse-evolution of antibiotic sensitivity in experimental populations of H. pylori. Nat. Ecol. Evol. 2024, 8, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Wong, C. Antibiotic resistance is a growing threat—Is climate change making it worse? Nature 2024. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Gonze, D.; Coyte, K.Z.; Lahti, L.; Faust, K. Microbial communities as dynamical systems. Curr. Opin. Microbiol. 2018, 44, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.S.; Gupta, R.; Vetsigian, K.H. Multi-stable bacterial communities exhibit extreme sensitivity to initial conditions. FEMS Microbiol. Ecol. 2021, 97, fiab073. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.S.; Vetsigian, K.H. Stochastic exits from dormancy give rise to heavy-tailed distributions of descendants in bacterial populations. Mol. Ecol. 2019, 28, 3915–3928. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Potter, R.F.; Marino, J.; Muenks, C.E.; Lammers, M.G.; Dien Bard, J.; Dingle, T.C.; Humphries, R.; Westblade, L.F.; Burnham, C.A.; et al. Comparative genomics reveals the correlations of stress response genes and bacteriophages in developing antibiotic resistance of Staphylococcus saprophyticus. mSystems 2023, 8, e0069723. [Google Scholar] [CrossRef] [PubMed]
- Cahill, D.J.; Fry, C.H.; Foxall, P.J. Variation in urine composition in the human urinary tract: Evidence of urothelial function in situ? J. Urol. 2003, 169, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Sabih, A.; Leslie, S.W. Complicated Urinary Tract Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Kwok, M.; McGeorge, S.; Mayer-Coverdale, J.; Graves, B.; Paterson, D.L.; Harris, P.N.A.; Esler, R.; Dowling, C.; Britton, S.; Roberts, M.J. Guideline of guidelines: Management of recurrent urinary tract infections in women. BJU Int. 2022, 130 (Suppl. S3), 11–22. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Maranchie, J.; Dhir, R.; Moon, C.H.; Biatta, S.; Balasubramani, G.K.; Yoshimura, N.; Fitzgerald, J.; Chermansky, C.; Kaufman, J.; et al. Unraveling the Complexity of bladder-centric chronic pain by intravesical contrast enhanced MRI. Continence 2023, 7, 101041. [Google Scholar] [CrossRef]
- Groah, S.L.; Rounds, A.K.; Perez-Losada, M. Intravesical Lactobacillus rhamnosus GG Alters Urobiome Composition and Diversity Among People With Neurogenic Lower Urinary Tract Dysfunction. Top. Spinal Cord Inj. Rehabil. 2023, 29, 44–57. [Google Scholar] [CrossRef]
- Hull, R.; Rudy, D.; Donovan, W.; Svanborg, C.; Wieser, I.; Stewart, C.; Darouiche, R. Urinary tract infection prophylaxis using Escherichia coli 83972 in spinal cord injured patients. J. Urol. 2000, 163, 872–877. [Google Scholar] [CrossRef]
- Zhang, H.L.; Perez, R.; Krishnan, J.; Lautenbach, E.; Anderson, D.J. Risk Factors for Recurrence of Community-Onset Urinary Tract Infections Caused by Extended-Spectrum Cephalosporin-Resistant Enterobacterales. Open Forum Infect. Dis. 2023, 10, ofad561. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, Z.; Zheng, L.; Gong, Z.; Li, Y.; Jin, Y.; Huang, Y.; Chi, M. Urinary Tract Infections Caused by Uropathogenic Escherichia coli: Mechanisms of Infection and Treatment Options. Int. J. Mol. Sci. 2023, 24, 10537. [Google Scholar] [CrossRef]
- Koley, S.; Ghosh, A.; Mukherjee, M. Occurrence of Imipenem-Resistant Uropathogenic Escherichia coli in Pregnant Women: An Insight into Their Virulence Profile and Clonal Structure. Curr. Microbiol. 2024, 81, 56. [Google Scholar] [CrossRef]
- Boueroy, P.; Chopjitt, P.; Hatrongjit, R.; Morita, M.; Sugawara, Y.; Akeda, Y.; Iida, T.; Hamada, S.; Kerdsin, A. Fluoroquinolone resistance determinants in carbapenem-resistant Escherichia coli isolated from urine clinical samples in Thailand. PeerJ 2023, 11, e16401. [Google Scholar] [CrossRef]
- Green, S.I.; Clark, J.R.; Santos, H.H.; Weesner, K.E.; Salazar, K.C.; Aslam, S.; Campbell, J.W.; Doernberg, S.B.; Blodget, E.; Morris, M.I.; et al. A Retrospective, Observational Study of 12 Cases of Expanded-Access Customized Phage Therapy: Production, Characteristics, and Clinical Outcomes. Clin. Infect. Dis. 2023, 77, 1079–1091. [Google Scholar] [CrossRef]
- Von Vietinghoff, S.; Shevchuk, O.; Dobrindt, U.; Engel, D.R.; Jorch, S.K.; Kurts, C.; Miethke, T.; Wagenlehner, F. The global burden of antimicrobial resistance—Urinary tract infections. Nephrol. Dial. Transplant. 2023, 39, 581–588. [Google Scholar] [CrossRef]
- Radera, S.; Agarwal, J.; Srivastava, S.; Gupta, P.; Pandey, A. Association of Virulence Markers with Resistance to Oral Antibiotics in Escherichia coli Isolates Causing Uncomplicated Community-Acquired Cystitis. Cureus 2023, 15, e39458. [Google Scholar] [CrossRef]
- Zhai, Y.; Pribis, J.P.; Dooling, S.W.; Garcia-Villada, L.; Minnick, P.J.; Xia, J.; Liu, J.; Mei, Q.; Fitzgerald, D.M.; Herman, C.; et al. Drugging evolution of antibiotic resistance at a regulatory network hub. Sci. Adv. 2023, 9, eadg0188. [Google Scholar] [CrossRef]
- Huttner, A.; Wijma, R.A.; Stewardson, A.J.; Olearo, F.; Von Dach, E.; Harbarth, S.; Bruggemann, R.J.M.; Mouton, J.W.; Muller, A.E. The pharmacokinetics of nitrofurantoin in healthy female volunteers: A randomized crossover study. J. Antimicrob. Chemother. 2019, 74, 1656–1661. [Google Scholar] [CrossRef]
- Edwina, A.E.; Koch, B.C.P.; Muller, A.E.; Al Jalali, V.; Matzneller, P.; Zeitlinger, M.; Sassen, S.D.T. Population plasma and urine pharmacokinetics and the probability of target attainment of fosfomycin in healthy male volunteers. Eur. J. Clin. Pharmacol. 2023, 79, 775–787. [Google Scholar] [CrossRef]
- Sharma, R.P.; Burgers, E.J.; Beltman, J.B. Development of a Physiologically Based Pharmacokinetic Model for Nitrofurantoin in Rabbits, Rats, and Humans. Pharmaceutics 2023, 15, 2199. [Google Scholar] [CrossRef]
- Wijma, R.A.; Koch, B.C.P.; van Gelder, T.; Mouton, J.W. High interindividual variability in urinary fosfomycin concentrations in healthy female volunteers. Clin. Microbiol. Infect. 2018, 24, 528–532. [Google Scholar] [CrossRef]
- Cadorniga, R.; Diaz Fierros, M.; Olay, T. Pharmacokinetic study of fosfomycin and its bioavailability. Chemotherapy 1977, 23 (Suppl. S1), 159–174. [Google Scholar] [CrossRef]
- Shimizu, K. Fosfomycin: Absorption and excretion. Chemotherapy 1977, 23 (Suppl. S1), 153–158. [Google Scholar] [CrossRef]
- Davis, C. Sequential intravenous/oral ciprofloxacin as an empiric antimicrobial therapy: Results of a Canadian multicenter study. The Canadian Collaborative Investigational Group. Clin. Ther. 1994, 16, 505–521. [Google Scholar]
- McAteer, J.; Lee, J.H.; Cosgrove, S.E.; Dzintars, K.; Fiawoo, S.; Heil, E.L.; Kendall, R.E.; Louie, T.; Malani, A.N.; Nori, P.; et al. Defining the Optimal Duration of Therapy for Hospitalized Patients with Complicated Urinary Tract Infections and Associated Bacteremia. Clin. Infect. Dis. 2023, 76, 1604–1612. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Barth, A.; Hossain, M.; Perry, C.R.; Gross, A.S.; Ogura, H.; Shabbir, S.; Thomas, S.; Dumont, E.F.; Brimhall, D.B.; Srinivasan, M.; et al. Pharmacokinetic, Safety, and Tolerability Evaluations of Gepotidacin (GSK2140944) in Healthy Japanese Participants. Clin. Pharmacol. Drug Dev. 2023, 12, 38–56. [Google Scholar] [CrossRef]
- Wagenlehner, F.; Perry, C.R.; Hooton, T.M.; Scangarella-Oman, N.E.; Millns, H.; Powell, M.; Jarvis, E.; Dennison, J.; Sheets, A.; Butler, D.; et al. Oral gepotidacin versus nitrofurantoin in patients with uncomplicated urinary tract infection (EAGLE-2 and EAGLE-3): Two randomised, controlled, double-blind, double-dummy, phase 3, non-inferiority trials. Lancet 2024, 403, 741–755. [Google Scholar] [CrossRef]
- Fillastre, J.P.; Leroy, A.; Josse, S.; Moulin, B. Pharmacokinetics of trometamol-fosfomycin in patients with renal insufficiency. Pathol. Biol. 1988, 36, 728–730. [Google Scholar]
- Potel, G.; Meignier, M.; Baron, D.; Reynaud, A.; Touze, M.D.; Courtieu, A.L. Pharmacokinetics of fosfomycin in normal and burn patients. Effect of probenecid. Drugs Exp. Clin. Res. 1989, 15, 177–184. [Google Scholar]
- Mengistu, D.A.; Alemu, A.; Abdukadir, A.A.; Mohammed Husen, A.; Ahmed, F.; Mohammed, B. Incidence of Urinary Tract Infection among Patients: Systematic Review and Meta-Analysis. Inquiry 2023, 60, 469580231168746. [Google Scholar] [CrossRef]
- Faine, B.A.; Rech, M.A.; Vakkalanka, P.; Gross, A.; Brown, C.; Harding, S.J.; Slocum, G.; Zimmerman, D.; Zepeski, A.; Rewitzer, S.; et al. High prevalence of fluoroquinolone-resistant UTI among US emergency department patients diagnosed with urinary tract infection, 2018–2020. Acad. Emerg. Med. 2022, 29, 1096–1105. [Google Scholar] [CrossRef]
- Rafat, D.; Agrawal, A.; Khalid, S.; Khan, A.U.; Nawab, T.; Sultan, A. Bacterial abundance and antimicrobial resistance patterns of uropathogens among pregnant women with asymptomatic bacteriuria: Association with glycemic status. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2024, 21, 100263. [Google Scholar] [CrossRef]
- Bilsen, M.P.; van Uhm, J.I.M.; Stalenhoef, J.E.; van Nieuwkoop, C.; Groenwold, R.H.H.; Visser, L.G.; Lambregts, M.M.C. Intravesical aminoglycoside instillations as prophylaxis for recurrent urinary tract infection: Patient satisfaction, long-term safety and efficacy. JAC Antimicrob. Resist. 2023, 5, dlad040. [Google Scholar] [CrossRef]
- Lin, K.; Zahlanie, Y.; Ortwine, J.K.; Mang, N.S.; Wei, W.; Brown, L.S.; Prokesch, B.C. Decreased Outpatient Fluoroquinolone Prescribing Using a Multimodal Antimicrobial Stewardship Initiative. Open Forum Infect. Dis. 2020, 7, ofaa182. [Google Scholar] [CrossRef]
- Yu, J.Y.; McKenna, V.A.; Dumyati, G.K.; Lubowski, T.J.; Carreno, J.J. Antibiotic Prescribing in New York State Medicare Part B Beneficiaries Diagnosed with Cystitis Between 2016 and 2017. Open Forum Infect. Dis. 2020, 7, ofz544. [Google Scholar] [CrossRef]
- Nair, M.; Zeegers, M.P.; Varghese, G.M.; Burza, S. India’s National Action Plan on Antimicrobial Resistance: A critical perspective. J. Glob. Antimicrob. Resist. 2021, 27, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, N.E.; Price, V.; Cunningham-Oakes, E.; Tsang, K.K.; Nunn, J.G.; Midega, J.T.; Anjum, M.F.; Wade, M.J.; Feasey, N.A.; Peacock, S.J.; et al. Innovations in genomic antimicrobial resistance surveillance. Lancet Microbe 2023, 4, e1063–e1070. [Google Scholar] [CrossRef] [PubMed]
- NICE antimicrobial stewardship: Right drug, dose, and time? Lancet 2015, 386, 717. [CrossRef]
- Plough, H.H. Penicillin resistance of Staphylococcus aureus and its clinical implications. Am. J. Clin. Pathol. 1945, 15, 446–451. [Google Scholar] [CrossRef]
- Milano, A.; Sulejmani, A.; Intra, J.; Sala, M.R.; Leoni, V.; Carcione, D. Antimicrobial Resistance Trends of Escherichia coli Isolates from Outpatient and Inpatient Urinary Infections over a 20-Year Period. Microb. Drug Resist. 2022, 28, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Bennett, N.; Malloy, M.J.; James, R.; Fang, X.; Thursky, K.; Worth, L.J. Prophylactic Antimicrobial Prescribing in Australian Residential Aged-Care Facilities: Improvement is Required. Drugs Real World Outcomes 2022, 9, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed]
- Zodrow, R.; Olson, A.; Willis, S.; Grauer, D.; Klatt, M. Characterization of antibiotic overuse for common infectious disease states at hospital discharge. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e229. [Google Scholar] [CrossRef] [PubMed]
- Higgins, H.; Freeman, R.; Doble, A.; Hood, G.; Islam, J.; Gerver, S.; Henderson, K.L.; Demirjian, A.; Hopkins, S.; Ashiru-Oredope, D. Appropriateness of acute-care antibiotic prescriptions for community-acquired infections and surgical antibiotic prophylaxis in England: Analysis of 2016 national point prevalence survey data. J. Hosp. Infect. 2023, 142, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Shafik, A.; Ahmed, I.; El Sibai, O.; Shafik, A.A. Does the composition of voided urine reflect that of the renal pelvis? Urol. Res. 2006, 34, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, R.; van de Pol, M.H.; Deen, P.M.; van Os, C.H.; Wetzels, J.F. Dissociation between urine osmolality and urinary excretion of aquaporin-2 in healthy volunteers. Nephrol. Dial. Transplant. 2000, 15, 1155–1161. [Google Scholar] [CrossRef][Green Version]
- Ashdown, H.H. Absorption from the Mucous Membrane of the Urinary Bladder. J. Anat. Physiol. 1887, 21, 299–324.291. [Google Scholar]
- Torimoto, K.; Matsushita, C.; Itami, Y.; Iwamoto, T.; Owari, T.; Gotoh, D.; Miyake, M.; Hori, S.; Nakai, Y.; Aoki, K.; et al. Assessment of bladder function for stabilizing urinary volume overnight with recording of brain waves (ABSORB study). Low. Urin. Tract Symptoms 2022, 14, 72–77. [Google Scholar] [CrossRef]
- Hilson, A.J.; Lewis, C.A.; Harland, S.J. The permeability of the human bladder to water assessed using tritiated water. Contrib. Nephrol. 1990, 79, 41–44. [Google Scholar] [CrossRef]
- Watanabe, H.; Azuma, Y. Periodical measurement of urine volume in the bladder during sleep: Temporary volume reduction suggestive of absorption. Int. J. Urol. 2016, 23, 182–187. [Google Scholar] [CrossRef]
- Shah, A.M.; Vodovotz, Y.; Yoshimura, N.; Chermansky, C.J.; Fitzgerald, J.; Tyagi, P. Temporally complex inflammatory networks in an animal model reveal signatures for interstitial cystitis and bladder pain syndrome phenotype. Neurourol. Urodyn. 2023, 42, 1839–1848. [Google Scholar] [CrossRef]
- Singh, N.; Zabbarova, I.; Ikeda, Y.; Kanai, A.; Chermansky, C.; Yoshimura, N.; Tyagi, P. Role of hyperpolarization-activated cyclic nucleotide-gated channels in aging bladder phenotype. Life Sci. 2022, 289, 120203. [Google Scholar] [CrossRef]
- Morizawa, Y.; Torimoto, K.; Hori, S.; Gotoh, D.; Nakai, Y.; Miyake, M.; Tanaka, N.; Hirayama, A.; Fujimoto, K. Sodium plays an important role in the absorption of intravesical fluid. Low Urin. Tract Symptoms 2021, 13, 177–182. [Google Scholar] [CrossRef]
- Sugaya, K.; Ogawa, Y.; Nishizawa, O.; de Groat, W.C. Decrease in intravesical saline volume during isovolumetric cystometry in the rat. Neurourol. Urodyn. 1997, 16, 125–132. [Google Scholar] [CrossRef]
- Tyagi, P.; Tyagi, V.; Qu, X.; Chuang, Y.C.; Kuo, H.C.; Chancellor, M. Elevated CXC chemokines in urine noninvasively discriminate OAB from UTI. Am. J. Physiol. Ren. Physiol. 2016, 311, F548–F554. [Google Scholar] [CrossRef]
- Sonn, G.A.; Jones, S.N.; Tarin, T.V.; Du, C.B.; Mach, K.E.; Jensen, K.C.; Liao, J.C. Optical biopsy of human bladder neoplasia with in vivo confocal laser endomicroscopy. J. Urol. 2009, 182, 1299–1305. [Google Scholar] [CrossRef]
- Gupta, D.K.; Lewis, C.E.; Varady, K.A.; Su, Y.R.; Madhur, M.S.; Lackland, D.T.; Reis, J.P.; Wang, T.J.; Lloyd-Jones, D.M.; Allen, N.B. Effect of Dietary Sodium on Blood Pressure: A Crossover Trial. JAMA 2023, 330, 2258–2266. [Google Scholar] [CrossRef]
- Russell, S.K.; Harrison, J.K.; Olson, B.S.; Lee, H.J.; O’Brien, V.P.; Xing, X.; Livny, J.; Yu, L.; Roberson, E.D.O.; Bomjan, R.; et al. Uropathogenic Escherichia coli infection-induced epithelial trained immunity impacts urinary tract disease outcome. Nat. Microbiol. 2023, 8, 875–888. [Google Scholar] [CrossRef]
- Eldrup, J.; Thorup, J.; Nielsen, S.L.; Hald, T.; Hainau, B. Permeability and ultrastructure of human bladder epithelium. Br. J. Urol. 1983, 55, 488–492. [Google Scholar] [CrossRef]
- Staehelin, L.A.; Chlapowski, F.J.; Bonneville, M.A. Lumenal plasma membrane of the urinary bladder. I. Three-dimensional reconstruction from freeze-etch images. J. Cell Biol. 1972, 53, 73–91. [Google Scholar] [CrossRef]
- Volter, D.; Schmidt, B. The reabsorption of creatinine from the rabbit bladder. Urol. Res. 1975, 3, 183–186. [Google Scholar] [CrossRef]
- Staerk, K.; Gronnemose, R.B.; Palarasah, Y.; Lund, L.; Andersen, T.E. Intracellular uropathogenic Escherichia coli are undetectable in urinary bladders after oral mecillinam treatment: An experimental study in a pig model of cystitis. Microb. Pathog. 2022, 173, 105817. [Google Scholar] [CrossRef]
- Lapides, J. Mechanisms of urinary tract infection. Urology 1979, 14, 217–225. [Google Scholar] [CrossRef][Green Version]
- Islam, M.M.; Takeyama, N. Role of Neutrophil Extracellular Traps in Health and Disease Pathophysiology: Recent Insights and Advances. Int. J. Mol. Sci. 2023, 24, 15805. [Google Scholar] [CrossRef]
- Krivosikova, K.; Supcikova, N.; Gaal Kovalcikova, A.; Janko, J.; Pastorek, M.; Celec, P.; Podracka, L.; Tothova, L. Neutrophil extracellular traps in urinary tract infection. Front. Pediatr. 2023, 11, 1154139. [Google Scholar] [CrossRef]
- Schmidt, E.P.; Overdier, K.H.; Sun, X.; Lin, L.; Liu, X.; Yang, Y.; Ammons, L.A.; Hiller, T.D.; Suflita, M.A.; Yu, Y.; et al. Urinary Glycosaminoglycans Predict Outcomes in Septic Shock and Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2016, 194, 439–449. [Google Scholar] [CrossRef]
- Mambatta, A.K.; Jayarajan, J.; Rashme, V.L.; Harini, S.; Menon, S.; Kuppusamy, J. Reliability of dipstick assay in predicting urinary tract infection. J. Fam. Med. Prim. Care 2015, 4, 265–268. [Google Scholar] [CrossRef]
- Bogovic Crncic, T.; Girotto, N.; Ilic Tomas, M.; Kristofic, I.; Klobucar, S.; Baticic, L.; Curko-Cofek, B.; Sotosek, V. Innate Immunity in Autoimmune Thyroid Disease during Pregnancy. Int. J. Mol. Sci. 2023, 24, 15442. [Google Scholar] [CrossRef]
- Lurie, S.; Rahamim, E.; Piper, I.; Golan, A.; Sadan, O. Total and differential leukocyte counts percentiles in normal pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 16–19. [Google Scholar] [CrossRef]
- Yang, F.; Feng, C.; Zhang, X.; Lu, J.; Zhao, Y. The Diverse Biological Functions of Neutrophils, Beyond the Defense Against Infections. Inflammation 2017, 40, 311–323. [Google Scholar] [CrossRef]
- Tyagi, P.; Motley, S.S.; Koyama, T.; Kashyap, M.; Gingrich, J.; Yoshimura, N.; Fowke, J.H. Molecular correlates in urine for the obesity and prostatic inflammation of BPH/LUTS patients. Prostate 2018, 78, 17–24. [Google Scholar] [CrossRef]
- Olszyna, D.P.; Prins, J.M.; Dekkers, P.E.; De Jonge, E.; Speelman, P.; Van Deventer, S.J.; Van Der Poll, T. Sequential measurements of chemokines in urosepsis and experimental endotoxemia. J. Clin. Immunol. 1999, 19, 399–405. [Google Scholar] [CrossRef]
- Albert, X.; Huertas, I.; Pereiro, I.I.; Sanfelix, J.; Gosalbes, V.; Perrota, C. Antibiotics for preventing recurrent urinary tract infection in non-pregnant women. Cochrane Database Syst. Rev. 2004, 2004, CD001209. [Google Scholar] [CrossRef]
- Smith, S.G.; Griffith, B.E.; Zaharoff, D.A. Analyzing the effects of instillation volume on intravesical delivery using biphasic solute transport in a deformable geometry. Math. Med. Biol. 2019, 36, 139–156. [Google Scholar] [CrossRef]
- Gyftopoulos, K.; Matkaris, M.; Vourda, A.; Sakellaropoulos, G. Clinical implications of the anatomical position of the urethra meatus in women with recurrent post-coital cystitis: A case-control study. Int. Urogynecol. J. 2019, 30, 1351–1357. [Google Scholar] [CrossRef]
- Saito, T.; Hitchens, T.K.; Foley, L.M.; Singh, N.; Mizoguchi, S.; Kurobe, M.; Gotoh, D.; Ogawa, T.; Minagawa, T.; Ishizuka, O.; et al. Functional and histologic imaging of urinary bladder wall after exposure to psychological stress and protamine sulfate. Sci. Rep. 2021, 11, 19440. [Google Scholar] [CrossRef]
- Veranic, P.; Jezernik, K. Succession of events in desquamation of superficial urothelial cells as a response to stress induced by prolonged constant illumination. Tissue Cell 2001, 33, 280–285. [Google Scholar] [CrossRef]
- Tyagi, P.; Tyagi, V.; Yoshimura, N.; Witteemer, E.; Barclay, D.; Loughran, P.A.; Zamora, R.; Vodovotz, Y. Gender-based reciprocal expression of transforming growth factor-beta1 and the inducible nitric oxide synthase in a rat model of cyclophosphamide-induced cystitis. J. Inflamm. 2009, 6, 23. [Google Scholar] [CrossRef]
- Tyagi, P.; Moon, C.H.; Connell, M.; Ganguly, A.; Cho, K.J.; Tarin, T.; Dhir, R.; Sholosh, B.; Maranchie, J. Intravesical Contrast-Enhanced MRI: A Potential Tool for Bladder Cancer Surveillance and Staging. Curr. Oncol. 2023, 30, 4632–4647. [Google Scholar] [CrossRef]
- Szczesniewski, J.J.; Marquez-Sanchez, M.T.; Padilla-Fernandez, B.; Llanes-Gonzalez, L.; Lorenzo-Gomez, M.F. Recurrent Bacteriuria as a Prognosis Marker in the Adjuvant Treatment of Non-Muscle Invasive Bladder Cancer. Clin. Genitourin. Cancer 2024, 22, 102048. [Google Scholar] [CrossRef]
- Tartaglione, T.A.; Johnson, C.R.; Brust, P.; Opheim, K.; Hooton, T.M.; Stamm, W.E. Pharmacodynamic evaluation of ofloxacin and trimethoprim-sulfamethoxazole in vaginal fluid of women treated for acute cystitis. Antimicrob. Agents Chemother. 1988, 32, 1640–1643. [Google Scholar] [CrossRef]
- Mores, C.R.; Price, T.K.; Wolff, B.; Halverson, T.; Limeira, R.; Brubaker, L.; Mueller, E.R.; Putonti, C.; Wolfe, A.J. Genomic relatedness and clinical significance of Streptococcus mitis strains isolated from the urogenital tract of sexual partners. Microb. Genom. 2021, 7, mgen000535. [Google Scholar] [CrossRef]
- Ahn, S.T.; Han, D.E.; Lee, D.H.; Kim, J.W.; Park, H.S.; Moon, D.G.; Oh, M.M. Single-dose amikacin plus 7 days of amoxicillin/clavulanate to treat acute cystitis caused by extended-spectrum beta-lactamase-producing Escherichia coli: A retrospective cohort study. Investig. Clin. Urol. 2021, 62, 310–316. [Google Scholar] [CrossRef]
- Periasamy, S.; Joo, H.S.; Duong, A.C.; Bach, T.H.; Tan, V.Y.; Chatterjee, S.S.; Cheung, G.Y.; Otto, M. How Staphylococcus aureus biofilms develop their characteristic structure. Proc. Natl. Acad. Sci. USA 2012, 109, 1281–1286. [Google Scholar] [CrossRef]
- Vaskova, S.; Slobodnikova, L.; Fajtl, D.; Blazickova, S.; Botek, R.; Melichacova, V. Biofilm-producing potential of urinary pathogens isolated from chronic and recurrent urinary tract infections and impact of biofilm on gentamicin and colistin in vitro efficacy. Epidemiol. Mikrobiol. Imunol. 2020, 69, 3–9. [Google Scholar]
- Macesic, N.; Dennis, A.; Hawkey, J.; Vezina, B.; Wisniewski, J.A.; Cottingham, H.; Blakeway, L.V.; Harshegyi, T.; Pragastis, K.; Badoordeen, G.Z.; et al. Genomic investigation of multispecies and multivariant blaNDM outbreak reveals key role of horizontal plasmid transmission. Infect. Control Hosp. Epidemiol. 2024, 1–8, online ahead of print. [Google Scholar] [CrossRef]
- Saini, P.; Bandsode, V.; Singh, A.; Mendem, S.K.; Semmler, T.; Alam, M.; Ahmed, N. Genomic insights into virulence, antimicrobial resistance, and adaptation acumen of Escherichia coli isolated from an urban environment. mBio 2024, 15, e0354523. [Google Scholar] [CrossRef]
- Avery, O.T.; Macleod, C.M.; McCarty, M. Studies on the Chemical Nature of the Substance Inducing Transformation of Pneumococcal Types: Induction of Transformation by a Desoxyribonucleic Acid Fraction Isolated from Pneumococcus Type Iii. J. Exp. Med. 1944, 79, 137–158. [Google Scholar] [CrossRef]
- Asemota, A.O.; Schneider, E.B.; Mowry, E.M.; Venkatesan, A. Common comorbid and secondary conditions leading to hospitalization in multiple sclerosis patients in the United States. Clin. Neurol. Neurosurg. 2023, 232, 107851. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Esquivel, J.; Zelenitsky, S.; Lawrence, C.K.; Adam, H.J.; Golden, A.; Hink, R.; Berry, L.; Schweizer, F.; Zhanel, M.A.; et al. Omadacycline: A Novel Oral and Intravenous Aminomethylcycline Antibiotic Agent. Drugs 2020, 80, 285–313. [Google Scholar] [CrossRef]
- Borgia, M.; Longo, A.; Lodola, E. Relative bioavailability of fosfomycin and of trometamol after administration of single dose by oral route of fosfomycin trometamol in fasting conditions and after a meal. Int. J. Clin. Pharmacol. Ther. Toxicol. 1989, 27, 411–417. [Google Scholar]
- Baietto, L.; Corcione, S.; Pacini, G.; Perri, G.D.; D’Avolio, A.; De Rosa, F.G. A 30-years review on pharmacokinetics of antibiotics: Is the right time for pharmacogenetics? Curr. Drug Metab. 2014, 15, 581–598. [Google Scholar] [CrossRef]
- Stocco, G.; Lucafo, M.; Decorti, G. Pharmacogenomics of Antibiotics. Int. J. Mol. Sci. 2020, 21, 5975. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Pozdirca, M.; Golden, A.R.; Lawrence, C.K.; Zelenitsky, S.; Berry, L.; Schweizer, F.; Bay, D.; Adam, H.; Zhanel, M.A.; et al. Sulopenem: An Intravenous and Oral Penem for the Treatment of Urinary Tract Infections Due to Multidrug-Resistant Bacteria. Drugs 2022, 82, 533–557. [Google Scholar] [CrossRef]
- Breiby, M.; Aarbakke, J.; Sundsfjord, J.; Goussius, G.; Pape, J. Effect of posture on ampicillin pharmacokinetics, glomerular filtration rate and renal plasma flow in resting subjects. Br. J. Clin. Pharmacol. 1983, 16, 691–694. [Google Scholar] [CrossRef]
- Roberts, M.S.; Denton, M.J. Effect of posture and sleep on pharmacokinetics. I. Amoxycillin. Eur. J. Clin. Pharmacol. 1980, 18, 175–183. [Google Scholar] [CrossRef]
- Forsberg, J.; Bedard, E.; Mahmoud, S.H. Bioavailability of Orally Administered Drugs in Critically Ill Patients. J. Pharm. Pract. 2023, 36, 967–979. [Google Scholar] [CrossRef]
- Duployez, C.; Loiez, C.; Cattoen, C.; Descamps, D.; Wallet, F.; Vachee, A.; Microbiologist Network from Nord-Pas-de-Calais. In vitro susceptibility to mecillinam of Escherichia coli strains isolated from the urine of pregnant women. Med. Mal. Infect. 2016, 46, 436–441. [Google Scholar] [CrossRef]
- Bergan, T. Degree of absorption, pharmacokinetics of fosfomycin trometamol and duration of urinary antibacterial activity. Infection 1990, 18 (Suppl. S2), S65–S69. [Google Scholar] [CrossRef]
- Hirai, T.; Shiraishi, C.; Nakai, S.; Ushiro, M.; Hanada, K.; Iwamoto, T. Population kinetic-pharmacodynamic analysis of serum potassium in patients receiving sulfamethoxazole/trimethoprim. Basic Clin. Pharmacol. Toxicol. 2022, 131, 380–391. [Google Scholar] [CrossRef]
- Cunha, B.A.; Giuga, J.; Gerson, S. Predictors of ertapenem therapeutic efficacy in the treatment of urinary tract infections (UTIs) in hospitalized adults: The importance of renal insufficiency and urinary pH. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 673–679. [Google Scholar] [CrossRef]
- Curtis, S.J.; Kwong, J.C.; Chaung, Y.L.; Mazza, D.; Walsh, C.J.; Chua, K.Y.; Stewardson, A.J. Resistance to first-line antibiotic therapy among patients with uncomplicated acute cystitis in Melbourne, Australia: Prevalence, predictors and clinical impact. JAC Antimicrob. Resist. 2024, 6, dlad145. [Google Scholar] [CrossRef]
- Mponponsuo, K.; Brown, K.A.; Fridman, D.J.; Johnstone, J.; Langford, B.J.; Lee, S.M.; MacFadden, D.R.; Patel, S.N.; Schwartz, K.L.; Daneman, N. Highly versus less bioavailable oral antibiotics in the treatment of gram-negative bloodstream infections: A propensity-matched cohort analysis. Clin. Microbiol. Infect. 2023, 29, 490–497. [Google Scholar] [CrossRef]
- Takahashi, M.; Hagiya, H.; Higashionna, T.; Nakano, Y.; Sato, K.; Haruki, Y.; Haruki, M.; Honda, H.; Ogawa, H.; Ueda, K.; et al. Antimicrobial prescription practices for outpatients with uncomplicated cystitis in Japan. Sci. Rep. 2022, 12, 5921. [Google Scholar] [CrossRef]
- Zayyad, H.; Eliakim-Raz, N.; Leibovici, L.; Paul, M. Revival of old antibiotics: Needs, the state of evidence and expectations. Int. J. Antimicrob. Agents 2017, 49, 536–541. [Google Scholar] [CrossRef]
- Drekonja, D.M.; Rector, T.S.; Cutting, A.; Johnson, J.R. Urinary tract infection in male veterans: Treatment patterns and outcomes. JAMA Intern. Med. 2013, 173, 62–68. [Google Scholar] [CrossRef]
- Kadivarian, S.; Heydarpour, F.; Karimpour, H.; Shahbazi, F. Measured versus estimated creatinine clearance in critically ill patients with acute kidney injury: An observational study. Acute Crit. Care 2022, 37, 185–192. [Google Scholar] [CrossRef]
- Gugliotta, G.; Calagna, G.; Adile, G.; Polito, S.; Saitta, S.; Speciale, P.; Palomba, S.; Perino, A.; Granese, R.; Adile, B. Is intravesical instillation of hyaluronic acid and chondroitin sulfate useful in preventing recurrent bacterial cystitis? A multicenter case control analysis. Taiwan J. Obstet. Gynecol. 2015, 54, 537–540. [Google Scholar] [CrossRef]
- Genovese, C.; Davinelli, S.; Mangano, K.; Tempera, G.; Nicolosi, D.; Corsello, S.; Vergalito, F.; Tartaglia, E.; Scapagnini, G.; Di Marco, R. Effects of a new combination of plant extracts plus d-mannose for the management of uncomplicated recurrent urinary tract infections. J. Chemother. 2018, 30, 107–114. [Google Scholar] [CrossRef]
- King, G.K.; Goodes, L.M.; Hartshorn, C.; Thavaseelan, J.; Jonescu, S.; Watts, A.; Rawlins, M.; Woodland, P.; Synnott, E.L.; Barrett, T.; et al. Intravesical hyaluronic acid with chondroitin sulphate to prevent urinary tract infection after spinal cord injury. J. Spinal Cord Med. 2023, 46, 830–836. [Google Scholar] [CrossRef]
- Rahnama’i, M.S.; Javan Balegh Marand, A.; Roschmann-Doose, K.; Steffens, L.; Arendsen, H.J. The efficacy and safety of intravesical chondroitin sulphate solution in recurrent urinary tract infections. BMC Urol. 2022, 22, 188. [Google Scholar] [CrossRef]
- Anderson, G.D. Pregnancy-induced changes in pharmacokinetics: A mechanistic-based approach. Clin. Pharmacokinet. 2005, 44, 989–1008. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, L.; Unadkat, J.D.; Mao, Q. Effect of pregnancy on nitrofurantoin disposition in mice. J. Pharm. Sci. 2009, 98, 4306–4315. [Google Scholar] [CrossRef]
- Tyagi, P.; Ganguly, A.; Chermansky, C.; Tarin, T.V.; Yoshimura, N.; Maranchie, J. Does large volume of distribution of lidocaine masks its systemic uptake from bladder? Am. J. Clin. Exp. Urol. 2023, 11, 121–135. [Google Scholar]
- Alpers, D.H.; Tomkins, G.M. The Order of Induction and Deinduction of the Enzymes of the Lactose Operon in E. coli. Proc. Natl. Acad. Sci. USA 1965, 53, 797–802. [Google Scholar] [CrossRef]
- Sumi, C.D.; Heffernan, A.J.; Lipman, J.; Roberts, J.A.; Sime, F.B. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin. Pharmacokinet. 2019, 58, 1407–1443. [Google Scholar] [CrossRef]
- Mouhssine, M.; Al Ani, D.; Al Shibli, A.; Ghatasheh, G.; Al Amri, A.; Matta, H.; Chedid, R.; Narchi, H. Intravesical gentamicin instillation in the prevention of recurrent urinary tract infections in children with neurogenic bladder—A single-center retrospective observational study. J. Pediatr. Urol. 2023, 19, 64-e1. [Google Scholar] [CrossRef]
- Zoqlam, R.; Lazauskaite, S.; Glickman, S.; Zaitseva, L.; Ilie, P.C.; Qi, S. Emerging molecular mechanisms and genetic targets for developing novel therapeutic strategies for treating bladder diseases. Eur. J. Pharm. Sci. 2022, 173, 106167. [Google Scholar] [CrossRef]
- Valentine-King, M.A.; Trautner, B.W.; Zoorob, R.J.; Salemi, J.L.; Gupta, K.; Grigoryan, L. Predicting Antibiotic Susceptibility among Patients with Recurrent Urinary Tract Infection Using a Prior Culture. J. Urol. 2024, 211, 144–152. [Google Scholar] [CrossRef]
- Tyagi, P.; Biatta, S.; Moon, C.H.; Yoshimura, N.; Fitzgerald, J.; Maranchie, J.; Chermansky, C. A Virtual Method for Measuring Bladder Blood Flow Relative to Femoral Artery. J. Urol. 2024, 211. in press. [Google Scholar]
- Tyagi, P.; Ganguly, A.; Foley, L.; Hitchens, T.; Yoshimura, N. A Radiation-Free, Virtual Measurement of Mouse Bladder Blood Flow. J. Urol. 2024, 211. in press. [Google Scholar]
- Parmelee, D.J.; Walovitch, R.C.; Ouellet, H.S.; Lauffer, R.B. Preclinical evaluation of the pharmacokinetics, biodistribution, and elimination of MS-325, a blood pool agent for magnetic resonance imaging. Investig. Radiol. 1997, 32, 741–747. [Google Scholar] [CrossRef]
- Zhang, H. Trisodium-[(2-(R)-[(4,4-diphenylcyclohexyl)phosphono-oxymethyl]-diethylenetriaminepentaacetato)(aquo)gadolinium(III): Gadofosveset. In Molecular Imaging and Contrast Agent Database (MICAD); National Center for Biotechnology Information (US): Bethesda, MD, USA, 2004. [Google Scholar]
- Miodonski, A.J.; Litwin, J.A. Microvascular architecture of the human urinary bladder wall: A corrosion casting study. Anat. Rec. 1999, 254, 375–381. [Google Scholar] [CrossRef]
- Lee, P.J.; Kuo, H.C. High incidence of lower urinary tract dysfunction in women with recurrent urinary tract infections. Low. Urin. Tract Symptoms 2020, 12, 33–40. [Google Scholar] [CrossRef]
- Yang, L.; Wang, K.; Li, H.; Denstedt, J.D.; Cadieux, P.A. The influence of urinary pH on antibiotic efficacy against bacterial uropathogens. Urology 2014, 84, 731.e1–731.e7. [Google Scholar] [CrossRef]
- Matsuzaki, T.; Scotcher, D.; Darwich, A.S.; Galetin, A.; Rostami-Hodjegan, A. Towards Further Verification of Physiologically-Based Kidney Models: Predictability of the Effects of Urine-Flow and Urine-pH on Renal Clearance. J. Pharmacol. Exp. Ther. 2019, 368, 157–168. [Google Scholar] [CrossRef]
- Ma, Q.; Gao, Y.; Lu, J.; Liu, X.; Wang, R.; Shi, Y.; Liu, J.; Su, H. The effect of regular aerobic exercise on renal function in patients with CKD: A systematic review and meta-analysis. Front. Physiol. 2022, 13, 901164. [Google Scholar] [CrossRef]
- Alou, L.; Aguilar, L.; Sevillano, D.; Gimenez, M.J.; Cafini, F.; Valero, E.; Relano, M.T.; Prieto, J. Urine bactericidal activity against resistant Escherichia coli in an in vitro pharmacodynamic model simulating urine concentrations obtained after 2000/125 mg sustained-release co-amoxiclav and 400 mg norfloxacin administration. J. Antimicrob. Chemother. 2006, 57, 714–719. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Parkinson, K.; Higgins, S.; Denisuik, A.; Adam, H.; Pitout, J.; Noreddin, A.; Karlowsky, J.A. Pharmacodynamic activity of fosfomycin simulating urinary concentrations achieved after a single 3-g oral dose versus Escherichia coli using an in vitro model. Diagn. Microbiol. Infect. Dis. 2017, 88, 271–275. [Google Scholar] [CrossRef]
- Andretta, E.; Longo, R.; Balladelli, M.; Sgarabotto, C.; Sgarabotto, D. Intravesical Gentamicin: An Option for Therapy and Prophylaxis against Recurrent UTIs and Resistant Bacteria in Neurogenic Bladder Patients on Intermittent Catheterization. Antibiotics 2022, 11, 1335. [Google Scholar] [CrossRef]
- Gallardo, S.; Troncoso-Marino, A.; Nadal-Braque, N.; Amado-Guirado, E.; Mallecot, Y.H.; Llor, C.; Group, P.-I.B.S. Improved management of cystitis in primary care following the implementation of a simple multifaceted intervention. Aten. Primaria 2022, 54, 102493. [Google Scholar] [CrossRef]
- Ingalls, E.M.; Veillette, J.J.; Olson, J.; May, S.S.; Dustin Waters, C.; Gelman, S.S.; Vargyas, G.; Hutton, M.; Tinker, N.; Fontaine, G.V.; et al. Impact of a Multifaceted Intervention on Antibiotic Prescribing for Cystitis and Asymptomatic Bacteriuria in 23 Community Hospital Emergency Departments. Hosp. Pharm. 2023, 58, 401–407. [Google Scholar] [CrossRef]
- Kon, S.; Meslovich, D.; Valdez, C.; Jenkins, T.C.; Shihadeh, K.; Franco-Paredes, C.; Price, C.S. Long-term impact of fluoroquinolone-sparing strategies for empirical treatment of acute uncomplicated cystitis among ambulatory patients. Ther. Adv. Infect. Dis. 2022, 9, 20499361221129415. [Google Scholar] [CrossRef]
- Khan, S.A.; Rahman, E.U.; Chobufo, M.D.; Yasin, A.; Monaghan, T.F.; Weiss, J.P.; Lazar, J.M. Nocturia is an Independent Predictor of Abdominal Aortic Calcification in Women: Results from the National Health and Nutrition Examination Survey. J. Community Health 2020, 45, 1111–1115. [Google Scholar] [CrossRef]
- Durkin, M.J.; Schmitz, V.; Hsueh, K.; Troubh, Z.; Politi, M.C. Older adults’ and caregivers’ perceptions about urinary tract infection and asymptomatic bacteriuria guidelines: A qualitative exploration. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e224. [Google Scholar] [CrossRef]
- Frimodt-Moller, N.; Bjerrum, L. Treating urinary tract infections in the era of antibiotic resistance. Expert Rev. Anti-Infect. Ther. 2023, 21, 1301–1308. [Google Scholar] [CrossRef]
- Antibiotic therapy for acute uncomplicated pyelonephritis in women. Take resistance into account. Prescrire Int. 2014, 23, 296–300. [Google Scholar]
- Safari, M.S.; Mohabatkar, H.; Behbahani, M. Novel surface biochemical modifications of urinary catheters to prevent catheter-associated urinary tract infections. J. Biomed. Mater. Res. Part B Appl. Biomater. 2024, 112, e35372. [Google Scholar] [CrossRef]
- Teng, X.; Yao, C.; McCoy, C.P.; Zhang, S. Comparison of Superhydrophilic, Liquid-Like, Liquid-Infused, and Superhydrophobic Surfaces in Preventing Catheter-Associated Urinary Tract Infection and Encrustation. ACS Biomater. Sci. Eng. 2024, 10, 1162–1172. [Google Scholar] [CrossRef]
- Perelshtein, I.; Shoshani, S.; Jacobi, G.; Natan, M.; Dudchenko, N.; Perkas, N.; Tkachev, M.; Bengalli, R.; Fiandra, L.; Mantecca, P.; et al. Protecting the Antibacterial Coating of Urinal Catheters for Improving Safety. ACS Appl. Bio Mater. 2024, 7, 990–998. [Google Scholar] [CrossRef]
- Kyser, A.J.; Mahmoud, M.Y.; Johnson, N.T.; Fotouh, B.; Steinbach-Rankins, J.M.; Gilbert, N.M.; Frieboes, H.B. Development and Characterization of Lactobacillus rhamnosus-Containing Bioprints for Application to Catheter-Associated Urinary Tract Infections. ACS Biomater. Sci. Eng. 2023, 9, 4277–4287. [Google Scholar] [CrossRef]
- Zhao, M.; Geng, S.; Zhang, L.; Fan, X.; Tong, F.; Meng, X.; Wang, T.; Fang, X.; Mei, Q.; Pan, A. Prevention of urinary tract infection using a silver alloy hydrogel-coated catheter in critically ill patients: A single-center prospective randomized controlled study. J. Intensive Med. 2024, 4, 118–124. [Google Scholar] [CrossRef]
- Michael, M.; Hodson, E.M.; Craig, J.C.; Martin, S.; Moyer, V.A. Short compared with standard duration of antibiotic treatment for urinary tract infection: A systematic review of randomised controlled trials. Arch. Dis. Child. 2002, 87, 118–123. [Google Scholar] [CrossRef]
- Michael, M.; Hodson, E.M.; Craig, J.C.; Martin, S.; Moyer, V.A. Short versus standard duration oral antibiotic therapy for acute urinary tract infection in children. Cochrane Database Syst. Rev. 2003, 1, CD003966. [Google Scholar] [CrossRef]
- Parekh, S.; Hayes, C.V.; Loader, J.; Ashiru-Oredope, D.; Hand, K.; Hicks, G.; Lecky, D. The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England’s Community Pharmacies. Antibiotics 2023, 12, 647. [Google Scholar] [CrossRef]
- Bocquier, A.; Erkilic, B.; Babinet, M.; Pulcini, C.; Agrinier, N.; Group, O.S. Resident-, prescriber-, and facility-level factors associated with antibiotic use in long-term care facilities: A systematic review of quantitative studies. Antimicrob. Resist. Infect. Control 2024, 13, 29. [Google Scholar] [CrossRef]
- Morris, C.J.; Rohn, J.L.; Glickman, S.; Mansfield, K.J. Effective Treatments of UTI-Is Intravesical Therapy the Future? Pathogens 2023, 12, 417. [Google Scholar] [CrossRef]
- Malik, Z. Effectiveness and safety of intravesical Gentamicin therapy in patients with recurrent urinary tract infections caused by multidrug resistant organisms. J. Pak. Med. Assoc. 2024, 74, 118–122. [Google Scholar] [CrossRef]
- Abrams, P.; Hashim, H.; Tomson, C.; Macgowan, A.; Skews, R.; Warren, K. The use of intravesical gentamicin to treat recurrent urinary tract infections in lower urinary tract dysfunction. Neurourol. Urodyn. 2017, 36, 2109–2116. [Google Scholar] [CrossRef]
- Marei, M.M.; Jackson, R.; Keene, D.J.B. Intravesical gentamicin instillation for the treatment and prevention of urinary tract infections in complex paediatric urology patients: Evidence for safety and efficacy. J. Pediatr. Urol. 2021, 17, 65.e1–65.e11. [Google Scholar] [CrossRef]
- Stalenhoef, J.E.; van Nieuwkoop, C.; Menken, P.H.; Bernards, S.T.; Elzevier, H.W.; van Dissel, J.T. Intravesical Gentamicin Treatment for Recurrent Urinary Tract Infections Caused by Multidrug Resistant Bacteria. J. Urol. 2019, 201, 549–555. [Google Scholar] [CrossRef]
- Cox, L.; He, C.; Bevins, J.; Clemens, J.Q.; Stoffel, J.T.; Cameron, A.P. Gentamicin bladder instillations decrease symptomatic urinary tract infections in neurogenic bladder patients on intermittent catheterization. Can. Urol. Assoc. J. 2017, 11, E350–E354. [Google Scholar] [CrossRef]
- Rieger, M.M.; Shah, N.M.; Ferrante, K.L.; Tan-Kim, J.; Jacobs, M.B.; Brubaker, L.; Alperin, M. Intraoperative Gentamicin Intravesical Instillation for Prevention of Urinary Tract Infection after Urogynecologic Surgery: A Randomized Controlled Trial. Urogynecology 2022, 28, 825–833. [Google Scholar] [CrossRef]
- de Jong, T.P.; Donckerwolcke, R.A.; Boemers, T.M. Neomycin toxicity in bladder irrigation. J. Urol. 1993, 150, 1199. [Google Scholar] [CrossRef]
- Gerharz, E.W.; Weingartner, K.; Melekos, M.D.; Varga, S.; Feiber, H.; Riedmiller, H. Neomycin-induced perception deafness following bladder irrigation in patients with end-stage renal disease. Br. J. Urol. 1995, 76, 479–481. [Google Scholar] [CrossRef]
- Kobayashi, Y. The role of chemokines in neutrophil biology. Front. Biosci. 2008, 13, 2400–2407. [Google Scholar] [CrossRef] [PubMed]
- Bosch, B.; Hartikainen, A.; Ronkainen, A.; Scheperjans, F.; Arkkila, P.; Satokari, R. Development of a Protocol for Anaerobic Preparation and Banking of Fecal Microbiota Transplantation Material: Evaluation of Bacterial Richness in the Cultivated Fraction. Microorganisms 2023, 11, 2901. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Key Findings/Implications |
|---|---|
| Wright et al., 2021 [6] | Study aids drawing the link between the delay in urinary MIC and time dependent evolution of uropathogens with AMR |
| Edwina et al., 2023 [24] | Delay in the attainment of urinary MIC of Fosfomycin relative the plasma MIC |
| Mponponsuo et al., 2023 [109]; Forsberg et al., 2023 [103] | Significance of oral bioavailability in clinical outcomes of OAT in uncomplicated cystitis |
| Faine et al., 2022 [38] | Prevalence of fluoroquinolone-resistant cystitis evinces a modest compliance with AMS and risks potential adverse reactions like Clostridium difficile infections |
| Cunha et al., 2016 [107]; Potel et al., 1989 [35] | Importance of renal insufficiency, urinary pH, and volume of distribution in therapeutic efficacy of OAT and injectable treatments |
| Sumi et al., 2019 [122] | OAT concentration required to suppress AMR |
| Andretta et al., 2022 [140] | Evidence supporting the efficacy of intravesical administration to counter AMR and recurrent cystitis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyagi, P.; Tyagi, S.; Stewart, L.; Glickman, S. SWOT and Root Cause Analyses of Antimicrobial Resistance to Oral Antimicrobial Treatment of Cystitis. Antibiotics 2024, 13, 328. https://doi.org/10.3390/antibiotics13040328
Tyagi P, Tyagi S, Stewart L, Glickman S. SWOT and Root Cause Analyses of Antimicrobial Resistance to Oral Antimicrobial Treatment of Cystitis. Antibiotics. 2024; 13(4):328. https://doi.org/10.3390/antibiotics13040328
Chicago/Turabian StyleTyagi, Pradeep, Shachi Tyagi, Laurence Stewart, and Scott Glickman. 2024. "SWOT and Root Cause Analyses of Antimicrobial Resistance to Oral Antimicrobial Treatment of Cystitis" Antibiotics 13, no. 4: 328. https://doi.org/10.3390/antibiotics13040328
APA StyleTyagi, P., Tyagi, S., Stewart, L., & Glickman, S. (2024). SWOT and Root Cause Analyses of Antimicrobial Resistance to Oral Antimicrobial Treatment of Cystitis. Antibiotics, 13(4), 328. https://doi.org/10.3390/antibiotics13040328