
Antibiotic Stewardship in Surgical Departments


Abstract
1. Introduction
2. Results and Discussion
2.1. Antimicrobial Stewardship Principles and Practices
2.2. The Impact of Infections in Surgical Wards
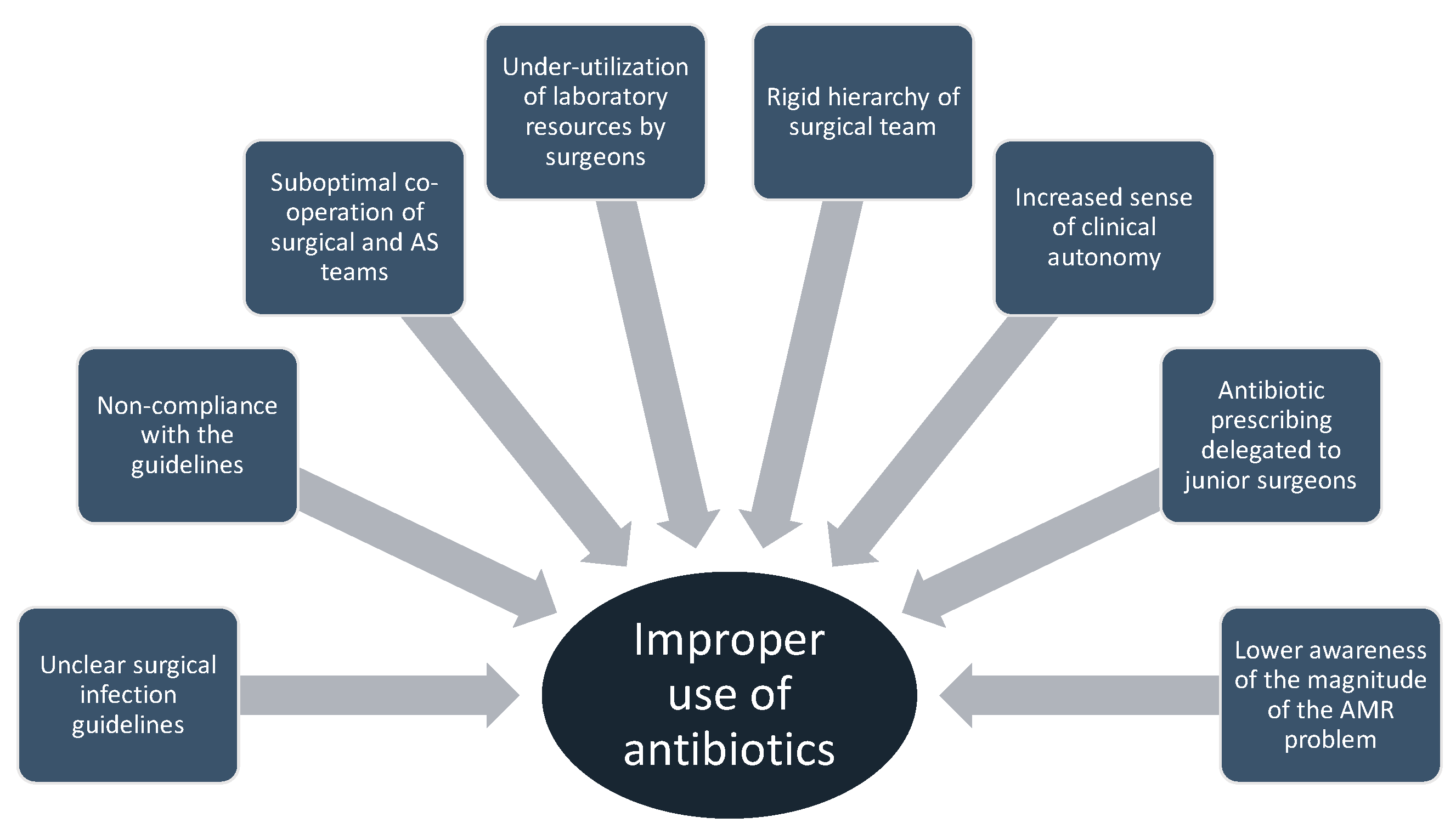
2.3. The Use of Antibiotics in Surgical Departments—The Importance of Education and Prescribing Etiquette
2.4. The Microbiology Laboratory and Diagnostic Stewardship—The Role of Biomarkers
2.5. The Antibiotic Stewardship Team—New Technologies and Antimicrobial Stewardship
3. Materials and Methods
4. Conclusions
- HAIs affect 5-15% of hospitalized patients, leading to increased vulnerability to MDROs
- AS objectives include empirical therapy suggestion, therapy de-escalation, IV to oral switch, and discontinuation of empirical treatment when no evidence of infection
- AS aims for optimal clinical outcomes and reduction in antimicrobial resistance
- Evidence-based guidelines and education are essential for reducing infections and AMR
- AS interventions should be tailored to local conditions and implemented through behavior-changing techniques
- AS in surgical wards should focus on SSI prevention and SAP
- SSIs occur in 1-3% of inpatient surgeries, contributing to patient injury, mortality, and increased healthcare costs
- Proper antibiotic use in surgery faces challenges such as unclear indications and lack of adherence
- Education plays a vital role in AS programs, including continuous training on AMR
- DS involves choosing the right test for the right patient at the right time, utilizing rapid diagnostics and biomarkers for prompt pathogen identification
Author Contributions
Funding
Conflicts of Interest
References
- Rice, L.B. The Maxwell Finland Lecture: For the Duration- Rational Antibiotic Administration in an Era of Antimicrobial Resistance and Clostridium Difficile. Clin. Infect. Dis. 2008, 46, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Labricciosa, F.; Coccolini, F.; Coimbra, R.; Zidan, F.; Ansaloni, L.; Al-Hasan, M.; Ansari, S.; Barie, P.; Cainzos, M.; et al. It is time to define an organizational model for the prevention and management of infections along the surgical pathway: A world-wide cross-sectional survey. World J. Emerg. Surg. 2022, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Menz, B.; Charani, E.; Gordon, D.; Leather, A.; Moonesinghe, D.; Phillips, C. Surgical Antibiotic prophylaxis in an era of antibiotic resistance: Common resistant bacteria and wider considerations for practice. Infect. Drug Resist. 2021, 14, 5235–5252. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Rice, L.B. Duration of antibiotic therapy: Shorter is Better. Arch. Intern. Med. 2019, 171, 210–211. [Google Scholar] [CrossRef]
- Anderson, D.; Jenkins, T.; Evans, S.; Harris, A.; Weinstein, R.; Tamma, P.; Han, J.; Banerjee, R.; Patel, R.; Zaoutis, T.; et al. Stewardship and Infection Control Committee of the Antibacterial Resistance Leadership Group. Clin. Infect. Dis. 2017, 64 (Suppl. S1), S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Mendelson, M.; Pallett, S.; Ahmad, R.; Mpundu, M.; Mbamalu, O.; Bosaconsa, C.; Nampoothiri, V.; Singh, S.; Smadja, N.; et al. An analysis of existing national action plans for antimicrobial resistance-gaps and opportunities in strategies optimizing antibiotic use in human populations. Lancet Glob. Health 2023, 11, e466–e474. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.; Kullar, R.; Bauer, K.; File, T., Jr. Eight habits of highly effective antimicrobial stewardship programs to meet the Joint Commission standards for hospitals. Clin. Infect. Dis. 2017, 64, 1134–1139. [Google Scholar] [CrossRef]
- Teillant, A.; Gandra, S.; Barter, D.; Morgan, D.; Laxminarayan, R. Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modeling study. Lancet Infect. Dis. 2015, 15, 1429–1437. [Google Scholar] [CrossRef]
- Arias, C.; Murray, B. Antibiotic-resistant bugs in 21st century-A clinical super challenge. N. Engl. J. Med. 2009, 360, 439–443. [Google Scholar] [CrossRef]
- Rhee, C. Using Procalcitonin to guide antibiotic therapy. Open Forum Infect. Dis. 2016, 4, ofw249. [Google Scholar] [CrossRef]
- Schuts, E.; Hulscher, M.; Mouton, J.; Verduin, C.; Cohen Stuart, J.; Overdiek, H.; van der Linden, P.; Natsch, S.; Hertogh, C.; Wolfs, T. Current evidence on hospital antimicrobial stewardship objectives: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 847–865. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Weber, D.; Ruppe, E.; Bassetti, M.; Wright, B.; Ansaloni, L.; Catena, F.; Cocclini, F.; Abu-Zidan, F.; Coimbra, R.; et al. Antimicrobials: A global alliance for optimizing their rational use in intra-abdominal infections (AGORA). World J. Emerg. Surg. 2016, 11, 33. [Google Scholar] [CrossRef]
- Murray, E.; Holmes, A. Addressing healthcare –associated infections and antimicrobial resistance from an organizational perspective: Progress and challenges. J. Antimicrob. Chemother. 2012, 67, i29–i36. [Google Scholar] [CrossRef]
- Zingg, W.; Storr, J.; Park, B.; Ahmad, R.; Tarrant, C.; Castro-Sanchez, E.; Tomczyk, S.; Kilpatrick, C.; Allegranzi, B.; Cardo, D.; et al. 2017 Geneva IPC-Think Tank. Implementation research for the prevention of antimicrobial resistance and healthcare-associated infections; 2017 Geneva infection prevention and control (IPC)- think tank (part 1). Antimicrob. Resist. Infect. Control 2019, 8, 87. [Google Scholar] [CrossRef]
- Peters, A.; Schmid, M.; Parneix, P.; Lebowicz, D.; de Kraker, M.; Sauser, J.; Zingg, W.; Pittet, D. Impact of environmental hygiene interventions on healthcare-associated infections and patient colonization: A systematic review. Antimicrob. Resist. Infect. Control 2022, 11, 38. [Google Scholar] [CrossRef]
- Mehtar, D.; Wanyoro, A.; Ogunsola, F.; Ameh, E.; Nthumba, P.; Kilpatrick, C.; Revathi, G.; Antoniadou, A.; Giamarelou, H.; Apisarnthanarak, A.; et al. Implementation of surgical site infection in low- and middle- income countries: A position statement for the International Society for Infectious Diseases. Int. J. Infect. Dis. 2020, 100, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Van Dijck, C.; Vlieghe, E.; Cox, J. Antibiotic stewardship interventions in hospitals in low- and middle-income countries: A systematic review. Bull. World Health Organ. 2018, 96, 266–280. [Google Scholar] [CrossRef] [PubMed]
- Dellit, T.H.; Owens, R.C.; McGowan, J., Jr.; Gerding, D.; Weinstein, R.A.; Burke, J.; Huskins, W.C.; Paterson, D.; Fishman, N.; Carpenter, C.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Dik, J.W.; Poelman, R.; Friedrich, A.W.; Panday, P.N.; Lo-Ten-Foe, J.; van Assen, S.; van Gemert-Pijnen, J.; Niesters, H.G.M.; Hendrix, R.; Sinha, B. An integrated stewardship model: Antimicrobial, infection prevention and diagnostic (AID). Future Microbiol. 2016, 11, 93–102. [Google Scholar] [CrossRef]
- Dik, J.; Poelman, R.; Friedrich, A.; Niesters, H.; Rossen, J.; Sinha, B. Integrated stewardship model comprising antimicrobial, infection prevention and diagnostic stewardship (AID Stewardship). J. Clin. Microbiol. 2017, 55, 3306–3307. [Google Scholar] [CrossRef] [PubMed]
- Nampoothiri, V.; Bonaconsa, C.; Surendran, S.; Mbamalu, O.; Nambatya, W.; Babigumira, P.; Ahmad, R.; Castro-Sanchez, E.; Broom, A.; Szymczak, J.; et al. What does antimicrobial stewardship look like where you are? Global narratives from participants in a massive open online course. JAC Antimicrob. Resist. 2021, 4, dlab186. [Google Scholar] [CrossRef]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C.; on behalf of ESGAP (ESCMID Study Group for Antimicrobial stewardship). What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef]
- Huttner, B.; Harbarth, S.; Nathwani, D.; ESCMID Study Group for Antibiotic Policies (ESGAP). Success stories of implementation of antimicrobial stewardship: A narrative review. Clin. Microbiol. Infect. 2014, 20, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.; Scott, C.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.; Ramsay, C.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.; Houck, P.; Richards, C.; Steele, L.; Dellinger, P.; Fry, D.; Wright, C.; Ma, A.; Carr, K.; Red, L. Use of antimicrobial prophylaxis for major surgery: Baseline results from the National Surgical Infection Prevention project. Arch. Surg. 2005, 140, 174–182. [Google Scholar] [CrossRef]
- Schena, C.; de’ Angelis, G.; Carra, M.; Bianchi, G.; de’ Angelis, N. Antimicrobial challenge in Acute Care surgery. Antibiotics 2022, 11, 1315. [Google Scholar] [CrossRef]
- Zimlichman, E.; Henderson, D.; Tamir, O.; Franz, C.; Song, P.; Yamin, C.; Keohane, C.; Denham, C.; Bates, D. Health care-associated infections: A meta-analysis of costs and financial impact on the US health care system. JAMA Intern. Med. 2013, 173, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D. Editorial commentary: Accountability for surgical site infections: Will the playing field be level? Clin. Infect. Dis. 2013, 57, 1289–1291. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.; Wertheim, H.; Sumprandit, N.; Vlieghe, W.; Hara, G.; Gould, I.; Goossens, H. Antibiotic resistance- the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Jin, J.; Akau Ola, S.; Yip, C.; Nthumba, P.; Ameh, E.; de Jonge, S.; Mehes, M.; Waiqanabete, H.; Henry, J.; Hill, A. The impact of Quality Improvement Interventions in improving surgical infections and mortalitry in low and middle-income countries: A systematic review and meta-analysis. World J. Surg. 2021, 45, 2993–3006. [Google Scholar] [CrossRef] [PubMed]
- Berrios-Torres, S.; Umsscheid, C.; Bratzler, D.; Leas, B.; Stone, E.; Kelz, R.; Reinke, C.; Morgan, S.; Solomkin, J.; Mazuski, J.; et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Calderwood, M.S.; Anderson, D.J.; Bratzier, D.W.; Dellinger, E.P.; Garcia-Houchins, S.; Maragakis, L.; Nyquist, A.C.; Perkins, K.M.; Preas, M.A.; Saiman, L.; et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2023, 44, 695–720. [Google Scholar] [CrossRef] [PubMed]
- Lipsett, P. Surgical site invention prevention-what we know and what we do not know. JAMA Surg. 2017, 152, 791–792. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.; Dellinger, E.P.; Olsen, K.M.; Perl, T.; Auwaerter, G.; Bolon, M.; Fish, D.; Napolitano, L.; Sawyer, R.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Health-Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [PubMed]
- Young, P.; Khadaroo, R.G. Surgical site infections. Surg. Clin. N. Am. 2014, 94, 1245–1264. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Righi, E.; Astilean, A.; Corcione, S.; Petrolo, A.; Farina, E.; De Rosa, F. Antimicrobial prophylaxis in minor and major surgery. Minerva Anesthesiol. 2015, 81, 76–91. [Google Scholar]
- Sievert, D.; Ricks, P.; Edwards, J.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S.; National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Tian, B.; Agnoletti, V.; Ansaloni, L.; Coccolini, F.; Bravi, F.; Sartelli, M.; Valicelli, C.; Catena, F. management of intra-abdominal infections: The role of procalcitonin. Antibiotics 2023, 12, 1406. [Google Scholar] [CrossRef]
- Chrysou, K.; Zorkotou, O.; Kalofolia, S.; Papagiannakopoulou, P.; Mamali, V.; Chrysos, G.; Themeli-Digalaki, K.; Sypsas, N.; Tsakris, A.; Pournaras, S. Impact of a 4-year antimicrobial stewardship program implemented in a Greek tertiary hospital. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 127–132. [Google Scholar] [CrossRef]
- Stocker, H.; Mehlhorn, C.; Jordan, K.; Eckholt, L.; Jefferys, L.; Arasteh, K. Clinical and economic effects of an antimicrobial stewardship intervention in a surgical intensive care unit. Infection 2020, 48, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Mokrani, D.; Chommeloux, J.; de Chambrun, M.; Hekimian, G.; Luyt, C. Antibiotic stewardship in the in the ICU: Time to shift into overdrive. Ann. Intensive Care 2023, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Ansaloni, L.; Bartoletti, M.; Catena, F.; Cardi, M.; Cortese, F.; Di Marzo, F.; Pea, F.; Plebani, M.; Rossolini, G.M.; et al. The role of procalcitonin in reducing antibiotics across the surgical pathway. World J. Emerg. Surg. 2021, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Castro-Sanchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the determinants of antimicrobial prescribing within hospitals: The role of “prescribing etiquette”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Choi, J.; Kim, C.; Kim, J.; Kim, H.; Lee, D. Implementation of procalcitonin in antibiotic stewardship: Derivation of a consensus algorithm for procalcitonin use in clinical practice. Infect. Chemother. 2022, 54, 621–636. [Google Scholar] [CrossRef] [PubMed]
- Illing, J.C.; Morrow, G.; Rothwell, C.; Burford, B.; Baldauf, B.; Davies, C.; Peile, E.; Spencer, J.; Johnson, N.; Allen, M.; et al. Perceptions of UK medical graduates’ preparedness for practice: A multi-centre qualitative study reflecting the importance of learning on the job. BMC Med. Educ. 2013, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Labricciosa, F.; Barbadoro, P.; Pagani, L.; Ansaloni, L.; Brink, A.; Carlet, J.; Khanna, A.; Chichom-Mefire, A.; Coccollini, F.; et al. The Global Alliance for Infections in Surgery: Defining a model for antimicrobial stewardship- results from an international cross-sectional survey. World J. Emerg. Surg. 2017, 12, 34. [Google Scholar] [CrossRef]
- Martinez-Sobalvarro, J.; Alves Pereira, A., Jr.; Birges Pereira, L.; Oliveira Baldoni, A.; Speroni Ceron, C.; Marques Dos Reis, T. Antimicrobial stewardship for surgical antibiotic prophylaxis and surgical site infections: A systematic review. Int. J. Clin. Pharm. 2022, 44, 301–319. [Google Scholar] [CrossRef] [PubMed]
- Cabral, S.; Harris, A.; Cosgrove, S.; Magder, L.; Tamma, P.; Goodman, K. Adherence to antimicrobial prophylaxis guidelines for elective surgeries across 825 US Hospitals, 2019–2020. Clin. Infect. Dis. 2023, 76, 2106–2115. [Google Scholar] [CrossRef]
- Malcolm, W.; Nathwani, D.; Davey, P.; Cromwell, T.; Patton, A.; Reilly, J.; Cairns, S.; Bennie, M. From intermittent antibiotic point prevalence surveys to quality improvement: Experience in Scottish hospitals. Antimicrob. Resist. Infect. Control 2013, 2, 3. [Google Scholar] [CrossRef]
- Lamb, G.; Phillips, G.; Charani, E.; Holmes, A.; Satta, G. Antibiotic prescribing practices in general surgery: A mixed methods quality improvement project. Infect. Prev. Pract. 2021, 3, 100166. [Google Scholar] [CrossRef] [PubMed]
- Spernovasilis, N.; Kritsotakis, E.; Mathioudaki, A.; Vouidaski, A.; Markai, I.; Psaroudaki, D.; Ioannou, P.; Kofteridis, D. Antimicrobial prescribing before and after the implementation of carbapenem-focused antimicrobial stewardship program in a Greek tertiary hospital during the COVID-19 pandemic. Antibiotics 2022, 12, 39. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Cataldo, M.; Albanese, A.; Tumbarello, M.; Arduini, E.; Spanu, T.; Fadda, G.; Anile, C.; Maira, G.; Federico, G.; et al. Vancomycin versus cefazolin prophylaxis for cerebrospinal shunt placement in a hospital with a high prevalence of methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 2008, 69, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Peel, T.; Astbury, S.; Cheng, A.; Paterson, D.; Buising, K.; Spelman, T.; Tran-Duy, A.; Adie, S.; Boyce, G.; McDougall, C.; et al. Trial of Vancomycin and cefazolin as surgical prophylaxis in arthroplasty. N. Engl. J. Med. 2023, 389, 1488–1498. [Google Scholar] [CrossRef] [PubMed]
- Dona, I.; Labella, M.; Bogas, G.; de Santa Maria, R.; Salas, M.; Ariza, A.; Torres, M. Antibiotic allergy de-labelling: A pathway against antibiotic resistance. Antibiotics 2022, 11, 1055. [Google Scholar] [CrossRef] [PubMed]
- Norvell, M.; Porter, M.; Ricco, M.; Koonce, R.; Hogan, C.; Basier, E.; Wong, M.; Jeffres, M. Cefazolin vs Second line Antibiotics for surgical site infection prevention after total joint athroplasty among patients with a beta-lactam allergy. Open Forum Infect. Dis. 2023, 10, ofad224. [Google Scholar] [CrossRef] [PubMed]
- Van Kasteren, M.; Mannien, J.; Ott, A.; Kullberg, B.J.; de Boer, A.; Gyssens, I. Antibiotic prophylaxis and the risk of surgical site infections following total hip arthroplasty: Timely administration is the most important factor. Clin. Infect. Dis. 2007, 44, 907–921. [Google Scholar] [CrossRef]
- Zelenitsky, S.; Calic, D.; Arora, R.; Grocott, H.; Lakowski, T.; Lillico, R.; Ariano, R. Antimicrobial prophylaxis for patients undergoing cardiac surgery: Intraoperative cefazolin concentrations and sternal wound infections. Antimicrob. Agents Chemother. 2018, 62, e01360. [Google Scholar] [CrossRef]
- Balch, A.; Wendelboe, A.; Vesely, S.; Bratzler, D. Antibiotic prophylaxis for surgical site infections as a risk factor for infection with Clostridium difficile. PLoS ONE 2017, 12, e0179117. [Google Scholar] [CrossRef]
- Harbarth, S.; Samore, M.H.; Lichtenberg, D.; Carmeli, Y. Prolonged antibiotic prophylaxis after cardiovascular surgery and its effect on surgical site infections and antimicrobial resistance. Circulation 2000, 101, 2916–2921. [Google Scholar] [CrossRef]
- Harbarth, S.; Samore, M.H.; Carmeli, Y. Antibiotic prophylaxis and the risk of Clostridium difficile-associated diarrhea. J. Hosp. Infect. 2001, 48, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Saleem, Z.; Ahsan, U.; Haseeb, A.; Altaf, U.; Batool, N.; Rani, H.; Jaffer, J.; Shahid, F.; Hussain, M.; Amir, A.; et al. Antibiotic utilization Patterns for different wound types among surgical patients: Findings and implications. Antibiotics 2023, 12, 678. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Barchitta, M.; Maugeri, A.; Sodano, L.; Pasquarella, C.; GISIO Working Groups of the Italian Society of Hygiene, Preventive Medicine and Public Health (Siti). Appropriate perioperative antibiotic prophylaxis: Challenges, strategies, and quality indicators. Epidemiol. Prev. 2015, 39 (Suppl. S1), 27–32. [Google Scholar]
- Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 2221–2248. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, R.G.; Claridge, J.A.; Nathens, A.B.; Rotstein, O.D.; Duane, T.M.; Evans, H.L.; Cook, P.J.; O’ Neill, P.J.; Mazuski, J.E.; Askari, R.; et al. Trial of short-course antimicrobial therapy. N. Engl. J. Med. 2015, 372, 1996–2005. [Google Scholar] [CrossRef] [PubMed]
- Foolad, F.; Nagel, J.; Eschenauer, G.; Patel, T.; Nguyen, C. Disease-based antimicrobial stewardship: A review of active and passive approaches to patient management. J. Antimicrob. Chemother. 2017, 72, 3232–3244. [Google Scholar] [CrossRef] [PubMed]
- Harnoss, J.; Zelienka, I.; Probst, P.; Grummich, K.; Miller-Lantzach, C.; Harnoss, J.; Ulrich, A.; Blichler, M.; Diener, M. Antibiotics versus surgical therapy for uncomplicated appendicitis: Systematic review and meta-analysis of controlled trial (PROSPERO2015:CRD42015016882). Ann. Surg. 2017, 265, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Chabok, A.; Pahlman, L.; Hjern, F.; Haapaniemi, S.; Smedh, K.; AVOD Study Group. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br. J. Surg. 2012, 99, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Parniczky, A.; Lantos, T.; Toth, E.; Szakacs, Z.; Godi, S.; Hagendom, R.; Illes, D.; Koncz, B.; Marta, K.; Miko, A.; et al. Antibiotic therapy in acute pancreatitis: From global overuse to evidence based recommendations. Pancreatology 2019, 19, 488–499. [Google Scholar] [CrossRef] [PubMed]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar] [CrossRef]
- Severino, A.; Varca, S.; Airola, C.; Mezza, T.; Gasbarrini, A.; Franceschi, F.; Candelli, M.; Nista, E. Antibiotic utilization in acute pancreatitis: A narrative review. Antibiotics 2023, 12, 1120. [Google Scholar] [CrossRef]
- Baltatzis, M.; Mason, J.; Chandrabalan, V.; Stathakis, P.; McIntyre, B.; Jegatheeswaran, S.; Jamdar, S.; O’ Reilly, D.; Siriwardena, A. Antibiotic use in acute pancreatitis: An audit of current practice in a tertiary centre. Pancreatology 2016, 16, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.; Wey, E. Antimicrobial stewardship in solid organ transplant- Opportunities in the National Health Service. Transpl. Infect. Dis. 2023, 25, e13961. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, P.; Karakonstantis, S.; Schouten, J.; Kostyanev, T.; Charani, E.; Vlahovic-Palcevski, V.; Kofteridis, D.; Supported by the ESCMID Group for Antimicrobial Stewardship- ESGAP. Importance of antimicrobial stewardship in solid organ transplant recipients: An ESCMID perspective. Transpl. Infect. Dis. 2022, 24, e13852. [Google Scholar] [CrossRef] [PubMed]
- Hand, J. The time is now: Antimicrobial stewardship in solid organ transplantation. Curr. Opin. Organ. Transpl. 2021, 26, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Tessier, J. A work in progress: Antimicrobial stewardship in solid organ transplant patient populations. Curr. Opin. Infect. Dis. 2022, 35, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.; Atamna, A.; Katchman, E.; Orenbuch-Harroch, E.; Nesher, L.; Bitterman, R.; Yahav, D.; Nutman, A. Current state of antimicrobial stewardship in solid organ transplantation in Israel. Transpl. Infect. Dis. 2022, 24, e13875. [Google Scholar] [CrossRef] [PubMed]
- Shafiekhani, M.; Shabani- Borujeni, M.; Karimian, A.; MomeniTabar, M.; Zare, Z.; Arabsheybani, S.; Vazin, A. Antibiotic stewardship implementation at the largest solid organ transplantation center in Asia: A retrospective cohort study. BMC Surg. 2023, 23, 81. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Mazzaferri, F.; de Smet, A.; Bragantini, D.; Eggimann, P.; Huttner, B.; Kuijper, E.; Lucet, J.; Mutters, N.; Sanguinetti, M.; et al. ESCMID-EUCIC clinical guidelines on decolonization of multidrug-resistant Gram-negative bacteria carriers. Clin. Microbiol. Infect. 2019, 25, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Righi, E.; Mutters, N.; Guirao, X.; Del Toro, M.; Eckmann, C.; Friedrich, A.; Giannella, M.; Kluytmans, J.; Presteri, E.; Christaki, E.; et al. ESCMID/EUCIC clinical practice guidelines on perioperative antibiotic prophylaxis in patients colonized by multidrug-resistant Gram-negative bacteria before surgery. Clin. Microbiol. Infect. 2023, 29, 463–479. [Google Scholar] [CrossRef]
- Giannella, M.; Bartoletti, M.; Conti, M.; Righi, E. Carbapenemase-producing Enterobacteriacae in transplant patients. J. Antimicrob. Chemother. 2021, 76, i27–i39. [Google Scholar] [CrossRef]
- Giblin, T.; Sinkowitz-Cochran, R.; Harris, P.; Jacobs, S.; Liberatore, K.; Palfreyman, M.; Harrison, E.; Cardo, D. Clinicians’ perceptions of the problem of antimicrobial resistance in health care facilities. Arch. Intern. Med. 2004, 164, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Deo, D.; Tan, S.; Bahtigur, N.; Lwin, N. The effectiveness of an antimicrobial stewardship program in an Australian rural hospital. Aust. J. Rural Health 2023, 31, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Imlay, H.; Spellberg, B. Shorter is better: The case for short antibiotic courses for common infections in solid organ transplant recipients. Transpl. Infect. Dis. 2022, 24, e13896. [Google Scholar] [CrossRef] [PubMed]
- Spernovasilis, N.; Ierodiakonou, D.; Spanias, C.; Mathioudaki, A.; Ioannou, P.; Petrakis, E.; Kofteridis, D. Doctor’s perceptions, attitudes and practices towards the management of multidrug-resistant organism infections after the implementation of an antimicrobial stewardship programme during the COVID-19 pandemic. Trop. Med. Infect. Dis. 2021, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.; Butters, T.; Moore, L.; Castro-Sanchez, E.; Cooke, F.; Holmes, A. Exploring the coverage of antimicrobial stewardship across UK clinical postgraduate training curricula. J. Antimicrob. Chemother. 2016, 71, 3284–3292. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Ahmad, R.; Rawson, T.; Castro-Sanchez, E.; Tarrant, C.; Holmes, A. The differences in antibiotic decision-making between acute surgical and acute medical teams: An ethnographic study of culture and team dynamics. Clin. Infect. Dis. 2019, 69, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Zakhour, J.; Haddad, S.; Kerbage, A.; Wertheim, H.; Tattevin, P.; Voss, A.; Unal, S.; Ouwdraogo, A.; Kanj, S. International Society of Antimicrobial Chemotherapy (ISAC) and the Alliance for the prudent use of antibiotics. Diagnostic stewardship in infectious diseases: A continuum of antimicrobial stewardship in the fight against antimicrobial resistance. Int. J. Antimicrob. Agents 2023, 52, 106816. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Malani, P.; Diekema, D.J. Diagnostic Stewardship- Leveraging the laboratory to improve antimicrobial use. JAMA 2017, 318, 607–608. [Google Scholar] [CrossRef]
- Mantzana, P.; Netsika, F.; Arhonti, M.; Meletis, G.; Kandilioti, E.; Kiriakopoulou, M.; Kagkalou, G.; Vasilaki, O.; Tychala, A.; Protonotariou, E.; et al. Performance evaluation of Alfred60 AST rapid sudceptibility testing directly from positivw blood cultures in the routine laboratory workflow. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1487–1494. [Google Scholar] [CrossRef]
- Leggieri, N.; Rida, A.; Francois, P.; Schrenzel, J. Molecular diagnosis of bloodstream infection: Planning to (physically) reach the bedside. Curr. Opin. Infect. Dis. 2010, 23, 311–319. [Google Scholar] [CrossRef]
- Kondo, M.; Simon, M.; Westblade, L.; Jenkins, S.; Babady, N.; Loo, A.; Calfee, D.; SHEA Research Network. Implementation of infectious diseases rapid molecular diagnostic tests and antimicrobial stewardship program involvement in acute-care hospitals. Infect. Control Hosp. Epidemiol. 2021, 42, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, N.; Mishra, A.; Gupta, R.; Ray, S. Biomarkers in sepsis- looking for the Holy Grail or chasing a mirage! World J. Crit. Care Med. 2023, 12, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Christ-Crain, M.; Muller, B. Procalctitonin in bacterial infections-hype, hope, more or less? Swiss Med. Wkly. 2005, 135, 451–460. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Giamarellos-Bourboulis, E. Antimicrobial stewardship using biomarkers: Accumulating evidence for the critically ill. Antibiotics 2022, 11, 367. [Google Scholar] [CrossRef] [PubMed]
- Desmard, M.; Bendara, A.; Boudinet, S.; Mal, H.; Dehoux, M.; Thabut, G.; Montravers, P. Post-operative kinetics of procalcitonin after lung transplantation. J. Heart Lung Transpl. 2015, 34, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Bouadma, L.; Luyt, C.; Tubach, F.; Vracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’ exposure to intensive care units (PRORATA trial): A multicenter randomized controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Hochreiter, M.; Kohler, T.; Schweiger, A.; Keck, F.; Bein, B.; von Spiegel, T.; Schroeder, S. Procalcitonin to guide duration of antibiotic therapy in intensive care patients: A randomized prospective controlled trial. Crit. Care 2009, 13, R83. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Antonelli, M.; Blasi, F.; Casagranda, I.; Chieregato, A.; Fumagalli, R.; Girardis, M.; Piertalli, F.; Plebani, M.; Rossolini, G.; et al. Procalcitonin-guided antibiotic therapy: An expert consensus. Clin. Chem. Lab. Med. 2018, 56, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, S.; Hochreiter, M.; Koehler, T.; Schweiger, A.M.; Bein, B.; Keck, F.S.; von Spiegel, T. Procalcitonin (PCT)-guided algorithm reduces length of antibiotic treatment in surgical intensive care patients with severe sepsis: Results of a prospective randomized study. Lagenbecks Arch. Surg. 2009, 394, 221–226. [Google Scholar] [CrossRef]
- Gallo, A.; Ianiro, G.; Montalto, M.; Cammarota, G. The role of biomarkers in diverticular disease. J. Clin. Gastroenterol. 2016, 50 (Suppl. S1), 526–528. [Google Scholar] [CrossRef]
- Yu, C.; Juan, L.I.; Wu, M.; Shen, C.; Wu, J.; Lee, C. Systematic review and meta-analysis of the diagnostic accuracy of procalcitonin, C-reactive protein and white blood cell count for suspected acute appendicitis. Br. J. Surg. 2013, 100, 322–329. [Google Scholar] [CrossRef]
- Parli, S.; Trivedi, G.; Woodworth, A.; Chang, P. Procalcitonin: Usefulness in Acute Surgery and Trauma. Surg. Infect. 2018, 19, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Chomba, R.N.; Moeng, M.S.; Lowman, W. Procalcitonin guided antibiotic therapy for suspected and confirmed sepsis of patients in a surgical trauma ICU: A prospective, two-period cross-over interventional study. S. Afr. J. Surg. 2020, 5, 143–149. [Google Scholar] [CrossRef]
- Dodds Ashley, E.; Davis, S.; Heil, E.; LaPlante, K.; Chahine, E.; Bosso, J. Best care for patients achieved through multidisciplinary stewardship. Clin. Infect. Dis. 2018, 67, 1637. [Google Scholar] [CrossRef] [PubMed]
- Pulcini, C.; Morel, C.; Tacconelli, E.; Beovic, B.; de With, K.; Goossens, H.; Harbarth, S.; Holmes, A.; Howard, P.; Morris, A.; et al. Human resources estimates and funding for antibiotic stewardship teams are urgently needed. Clin. Microbiol. Infect. 2017, 23, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Ostrowsky, B.; Banerjee, R.; Bonomo, R.; Cosgrove, S.; Davidson, L.; Doron, S.; Gilbert, D.; Jezek, A.; Lynch, J.B., III; Septimus, E.J. Infectious Diseases Physicians: Leading the way in antimicrobial stewardship. Clin. Infect. Dis. 2018, 66, 995–1003. [Google Scholar] [CrossRef]
- Pliakos, E.; Andreatos, N.; Shehadeh, F.; Ziakas, P.; Mylonakis, E. The Cost- Effectiveness of rapid diagnostic testing for the diagnosis of bloodstream infections with or without Antimicrobial stewardship. Clin. Microbiol. Rev. 2018, 31, e00095-17. [Google Scholar] [CrossRef]
- Klinker, K.; Hidayat, L.; DeRyke, C.A.; DePestel, D.; Motyl, M.; Bauer, K. Antimicrobial stewardship and antibiograms: Importance of moving beyond traditional antibiograms. Ther. Adv. Infect. Dis. 2021, 8, 20499361211011373. [Google Scholar] [CrossRef]
- Sakagianni, A.; Koufopoulou, C.; Feretzakis, G.; Kalles, D.; Verykios, V.; Myrianthefs, P.; Fildisis, G. Using machine learning to predict antimicrobial resistance- a literature review. Antibiotics 2023, 12, 452. [Google Scholar] [CrossRef]
- Rawson, T.; Wilson, R.; O’Hare, D.; Herrero, P.; Kambugu, A.; Lamorde, M.; Ellington, M.; Georgiou, P.; Cass, A.; Hope, W.; et al. Optimizing antimicrobial use: Challenges, advances and opportunities. Nat. Rev. Microbiol. 2021, 19, 747–758. [Google Scholar] [CrossRef]
- Kherabi, Y.; Messika, J.; Peiffer-Smadja, N. Machine learning, antimicrobial stewardship, and solid organ transplantation: Is this the future? Transpl. Infect. Dis. 2022, 24, e13957. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pathogen | Variation over Time | Type of Surgery Where Prevalent | ||
|---|---|---|---|---|
| 1990–1996 | 2007 | 2010 | ||
| S. aureus | 20% | 30% | 30.4% | Prostheses, implants |
| Cardiac | ||||
| Neurosurgery | ||||
| Ophthalmic | ||||
| Orthopedic | ||||
| Vascular | ||||
| Coagulase negative staphylococci | 14% | 13.7% | 11.7% | Prostheses, implants |
| Cardiac | ||||
| Neurosurgery | ||||
| Ophthalmic | ||||
| Orthopedic | ||||
| Vascular | ||||
| Enterococcus spp. | 12% | 11.2% | 11.6% | Colorectal |
| Obstetrics and gynecology | ||||
| Gram-negative bacilli | Appendectomy | |||
| E. coli | 8% | 9.6% | 9.4% | Biliary tract |
| P. aeruginosa | 8% | 5.6% | 5.5% | Colorectal |
| Enterobacter spp. | 7% | 4.2% | 4% | Gastroduodenal |
| Klebsiella spp. | 3% | 4% | 4% | Obstetrics and gynecology |
| 2007–2008 | 2009–2010 | |
|---|---|---|
| Methicillin R S. aureus | 48.0 | 43.7 |
| Vancomycin R Enterococcus | ||
| E. faecium | 65.2 | 65.3 |
| E. faecalis | ||
| Klebsiella spp. | ||
| Cephalosporin R | 19.4 | 13.2 |
| Carbapenem R | 9.6 | 7.9 |
| MDR | 10.9 | 6.8 |
| E. coli | ||
| Cephalosporin R | 9.1 | 10.9 |
| Fluoroquinolone R | 27.2 | 28.3 |
| Carbapenem R | 1.5 | 2.0 |
| MDR | 1.1 | 1.6 |
| Enterobacter spp. | ||
| Cephalosporin R | 30.6 | 27.7 |
| Carbapenem R | 2.8 | 2.4 |
| MDR | 1.5 | 1.7 |
| Pseudomonas aeruginosa | ||
| Aminoglycoside R | 4.4 | 6.0 |
| Cephalosporin R | 13.6 | 11.2 |
| Fluoroquinolone R | 15.8 | 16.9 |
| Carbapenem R | 11.2 | 11.6 |
| Piperacillin/Tazobactam R | 6.8 | 6.8 |
| MDR | 4.9 | 5.3 |
| Acinetobacter baumannii | ||
| Carbapenem R | 38.6 | 37.3 |
| MDR | 49.3 | 43.9 |
| Type of Surgery | Indication | Timing | Duration | Antibiotic Choice | Overall |
|---|---|---|---|---|---|
| Orthopedic | 99.4% | 73% | 70.2% | 57.7% | 43.6% |
| Abdominal surgery including herniorrhaphy | 12.4% | ||||
| Cardiac | 97.4% | 66.1% | |||
| Clean or clean-contaminated | 18.6% | 30.3% | 26.7% | 30.8% | 9.4% |
| Caesarean section | 59.5–100% | ||||
| Vascular | 95% | 87% | 98% | 80% | |
| Emergency trauma laparotomy | |||||
| Various | 44.8–95% | 53.4–100% | 59.4–88.7% | 25.5–98% | 6.9–100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kourbeti, I.; Kamiliou, A.; Samarkos, M. Antibiotic Stewardship in Surgical Departments. Antibiotics 2024, 13, 329. https://doi.org/10.3390/antibiotics13040329
Kourbeti I, Kamiliou A, Samarkos M. Antibiotic Stewardship in Surgical Departments. Antibiotics. 2024; 13(4):329. https://doi.org/10.3390/antibiotics13040329
Chicago/Turabian StyleKourbeti, Irene, Aikaterini Kamiliou, and Michael Samarkos. 2024. "Antibiotic Stewardship in Surgical Departments" Antibiotics 13, no. 4: 329. https://doi.org/10.3390/antibiotics13040329
APA StyleKourbeti, I., Kamiliou, A., & Samarkos, M. (2024). Antibiotic Stewardship in Surgical Departments. Antibiotics, 13(4), 329. https://doi.org/10.3390/antibiotics13040329