
Antimicrobial Stewardship in the Emergency Department Observation Unit: Definition of a New Indicator and Evaluation of Antimicrobial Use and Clinical Outcomes

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Results
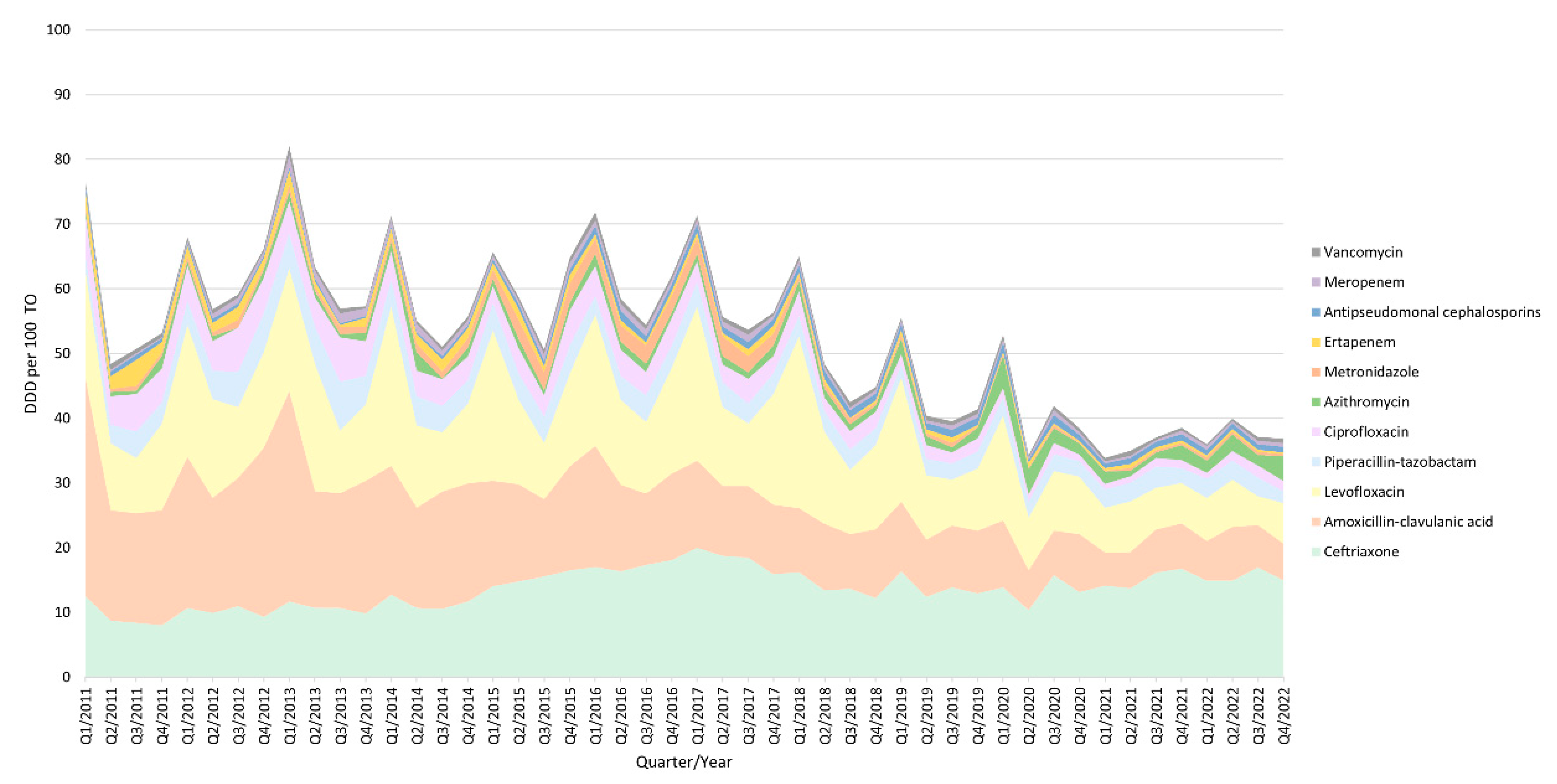
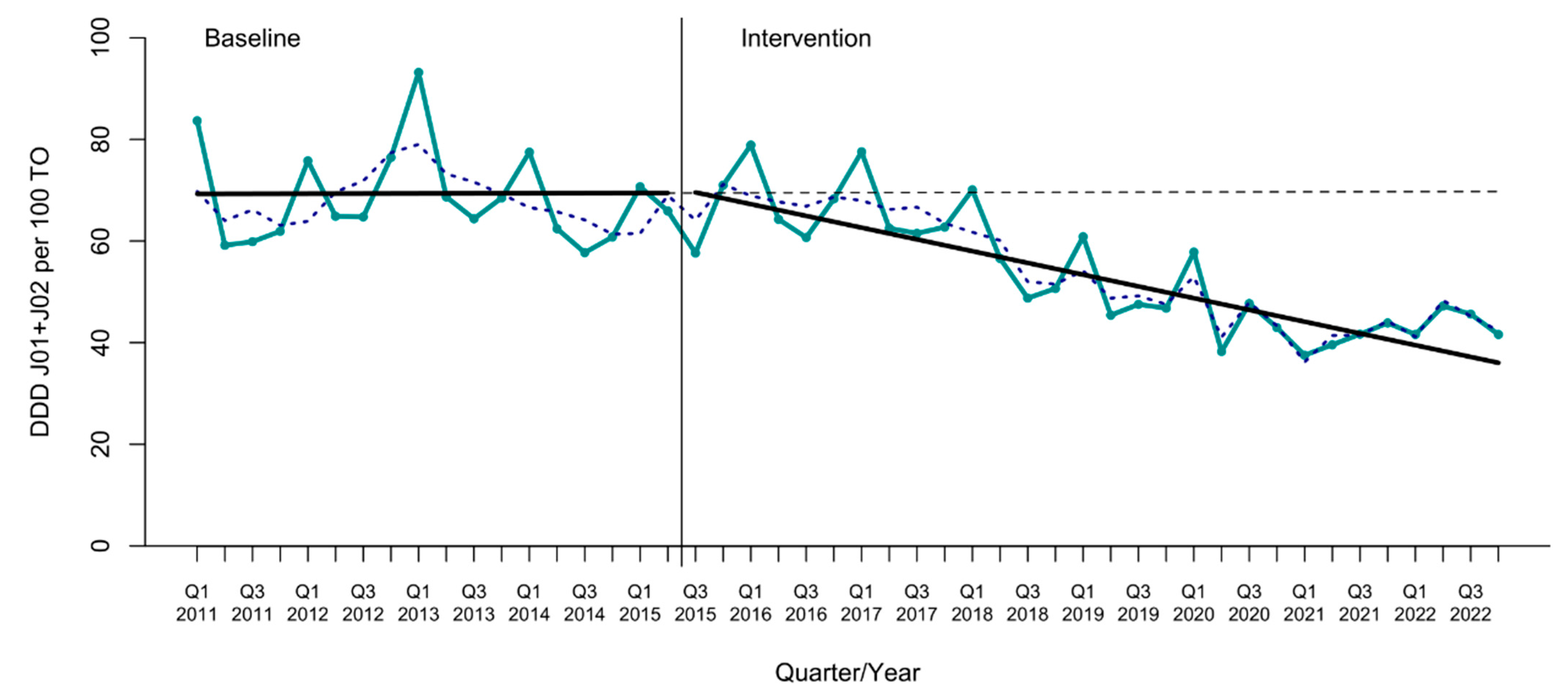
2.1. Antimicrobial Use
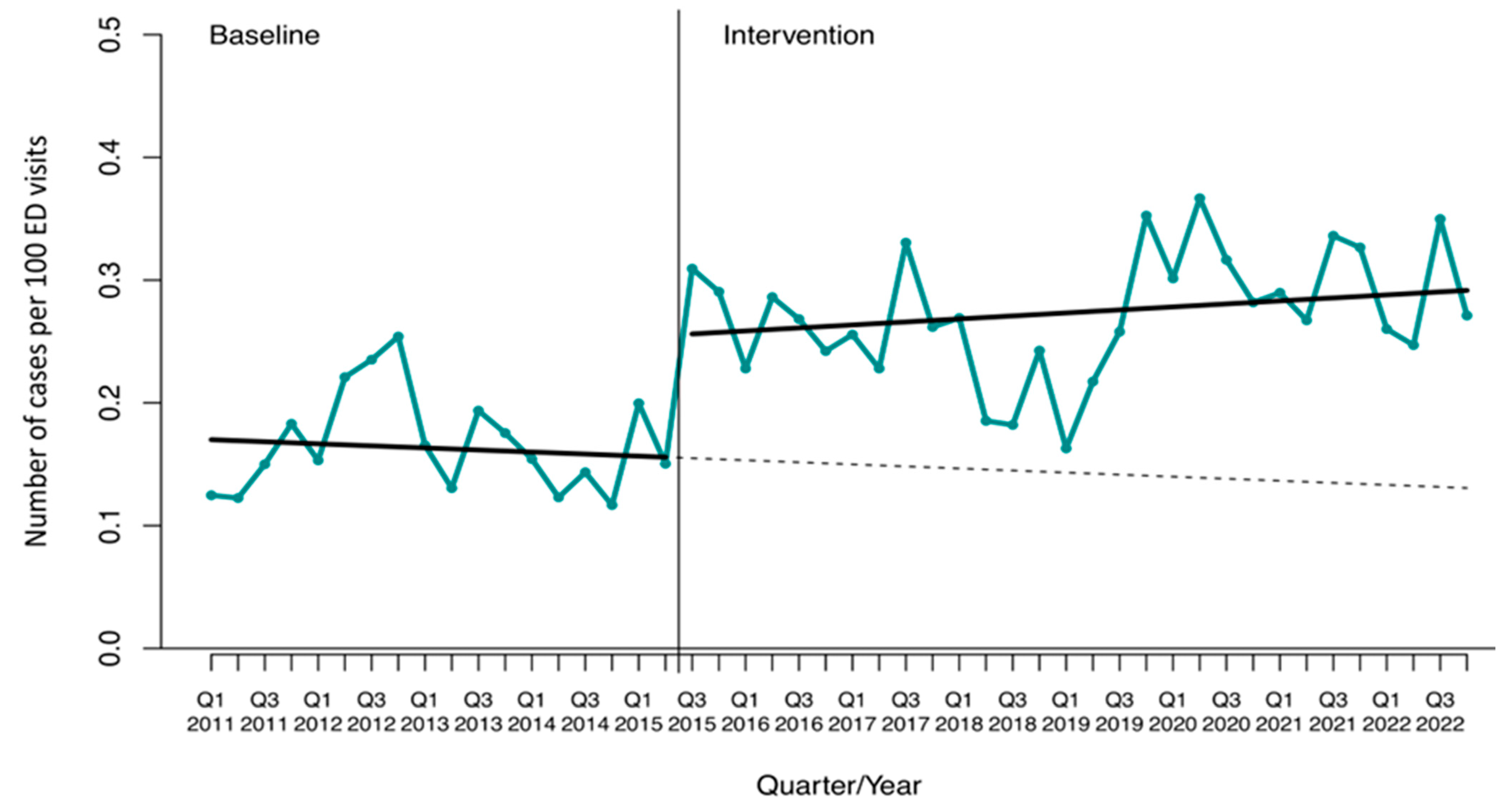
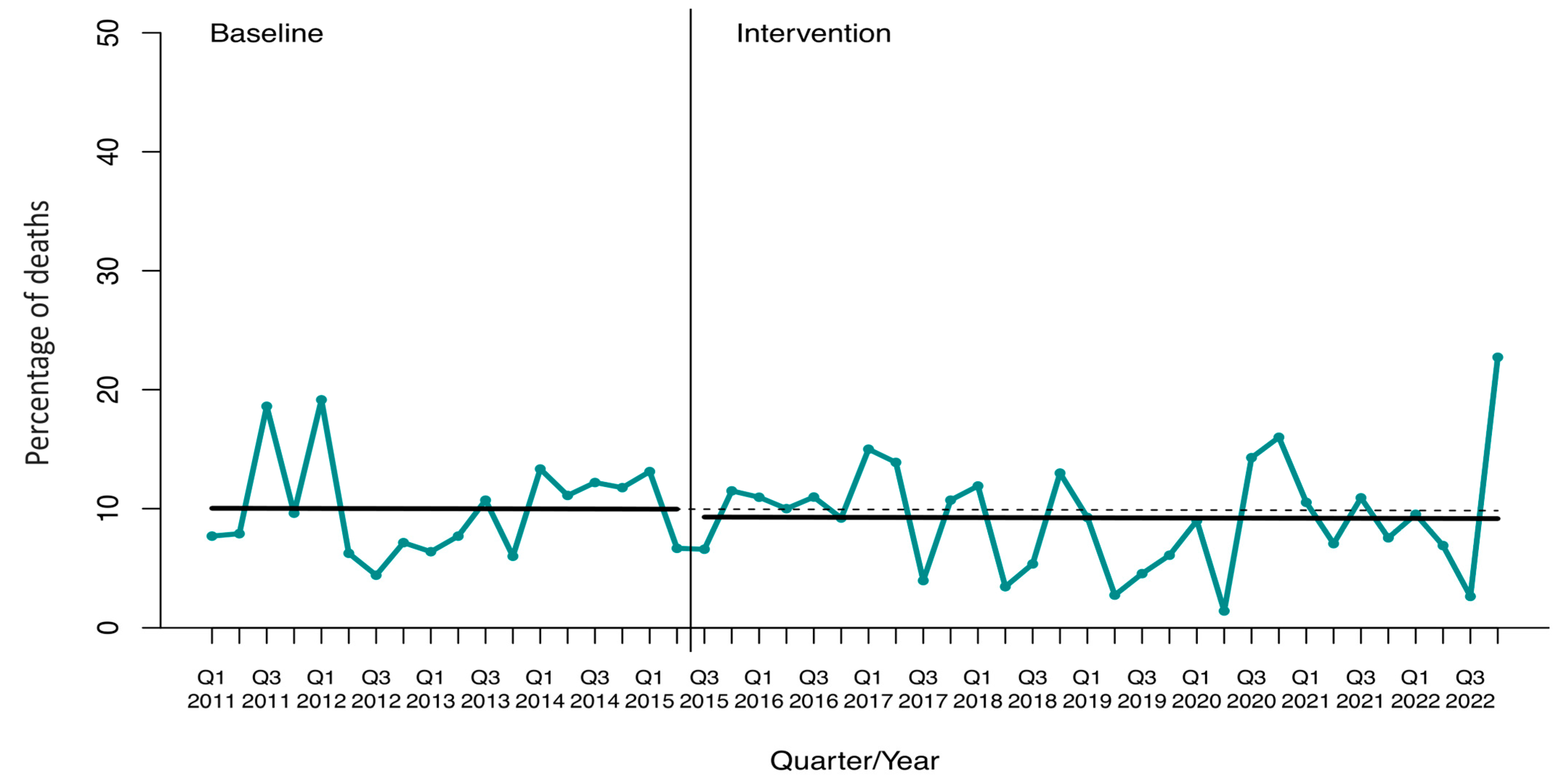
2.2. Clinical Outcomes
2.2.1. Incidence Density
2.2.2. Mortality Rate
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Intervention
4.3. Outcomes
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef] [PubMed]
- Drekonja, D.M.; Filice, G.A.; Greer, N.; Olson, A.; MacDonald, R.; Rutks, I.; Wilt, T.J. Antimicrobial stewardship in outpatient settings: A systematic review. Infect. Control Hosp. Epidemiol. 2015, 36, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.H.; Nygaard Jensen, J.; Bjerrum, L.; Siersma, V.; Winther Bang, C.; Brostrøm Kousgaard, M.; Holm, A. Effectiveness of a tailored intervention to reduce antibiotics for urinary tract infections in nursing home residents: A cluster, randomised controlled trial. Lancet Infect. Dis. 2021, 21, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Pulia, M.; Redwood, R.; May, L. Antimicrobial stewardship in the emergency department. Emerg. Med. Clin. N. Am. 2018, 36, 853–872. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.K.; Elshaboury, R.H.; Gandhi, R.G.; Hayes, B.D.; Yun, B.J.; Koehl, J.L. Assessment and Optimization of the Empiric Treatment of Urinary Tract Infections in an Academic Emergency Department Observation Unit. J. Emerg. Med. 2020, 58, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Cercenado, E.; Rodríguez-Baño, J.; Alfonso, J.L.; Calbo, E.; Escosa, L.; Fernández-Polo, A.; García-Rodríguez, J.; Garnacho, J.; Gil-Navarro, M.V.; Grau, S.; et al. Antimicrobial stewardship in hospitals: Expert recommendation guidance document for activities in specific populations, syndromes and other aspects (PROA-2) from SEIMC, SEFH, SEMPSPGS, SEMICYUC and SEIP. Enfermedades Infecc. Microbiol. Clin. 2022, 41, 238–242. [Google Scholar] [CrossRef]
- Trinh, T.D.; Klinker, K.P. Antimicrobial stewardship in the emergency department. Infect. Dis. Ther. 2015, 4, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Duran, C.; Davido, B.; Bouchand, F.; Deconinck, L.; Matt, M.; Sénard, O.; Guyot, C.; Levasseur, A.-S.; Attal, J.; et al. Impact of an antimicrobial stewardship programme to optimize antimicrobial use for outpatients at an emergency department. J. Hosp. Infect. 2017, 97, 288–293. [Google Scholar] [CrossRef] [PubMed]
- GLASS Guide for National Surveillance Systems for Monitoring Antimicrobial Consumption in Hospitals; World Health Organization: Geneva, Switzerland, 2020.
- Centers for Disease Control and Prevention (CDC); National Healthcare Safety Network (NHSN). Antimicrobial Use and Resistance (AUR) Module; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2021.
- May, L.; Martín-Quirós, A.; Oever, J.T.; Hoogerwerf, J.; Schoffelen, T.; Schouten, J. Antimicrobial stewardship in the emergency department: Characteristics and evidence for effectiveness of interventions. Clin. Microbiol. Infect. 2021, 27, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.J.; Hicks, L.A.; Roberts, R.M.; Hunkler, R.J.; Taylor, T.H. Trends and seasonal variation in outpatient antibiotic prescription rates in the United States, 2006 to 2010. Antimicrob. Agents Chemother. 2014, 58, 2763–2766. [Google Scholar] [CrossRef] [PubMed]
- Borde, J.P.; Kern, W.V.; Hug, M.; Steib-Bauert, M.; de With, K.; Busch, H.J.; Kaier, K. Implementation of an intensified antibiotic stewardship programme targeting third-generation cephalosporin and fluoroquinolone use in an emergency medicine department. Emerg. Med. J. 2015, 32, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Savoldi, A.; Foschi, F.; Kreth, F.; Gladstone, B.P.; Carrara, E.; Eisenbeis, S.; Buhl, M.; Marasca, G.; Bovo, C.; Malek, N.P.; et al. Impact of implementing a non-restrictive antibiotic stewardship program in an emergency department: A four-year quasi-experimental prospective study. Sci. Rep. 2020, 10, 8194. [Google Scholar] [CrossRef] [PubMed]
- Moehring, R.W.; Dodds Ashley, E.S.; Ren, X.; Lokhnygina, Y.; Baker, A.W.; Jones, T.M.; Lewis, S.S.; Sexton, D.J.; Anderson, D.J.; Centers for Disease Control and Prevention Epicenters Program. Denominator Matters in Estimating Antimicrobial Use: A Comparison of Days Present and Patient Days. Infect. Control Hosp. Epidemiol. 2018, 39, 612–615. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Ramos, J.; Santolaya Perrín, M.R.; González Del Castillo, J.; Candel, F.J.; Quirós, A.M.; López-Contreras González, J.; Jiménez, A.J.; Grande, A.S.-L. Design of a panel of indicators for antibiotic stewardship programs in the Emergency Department. Farm. Hosp. 2023, 48, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Cash, M.C.; Hile, G.; Johnson, J.; Stone, T.; Smith, J.; Ohl, C.; Luther, V.; Beardsley, J. Sustained impact of an antibiotic stewardship initiative targeting asymptomatic bacteriuria and pyuria in the emergency department. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e148. [Google Scholar] [CrossRef] [PubMed]
- Shishido, A.; Otake, S.; Kimura, M.; Tsuzuki, S.; Fukuda, A.; Ishida, A.; Kasai, M.; Kusama, Y. Effects of a nudge-based antimicrobial stewardship program in a pediatric primary emergency medical center. Eur. J. Pediatr. 2021, 180, 1933–1940. [Google Scholar] [CrossRef] [PubMed]
- Clemenceau, M.; Ahmed-Elie, S.; Vilfaillot, A.; Chocron, R.; Compain, F.; Lebeaux, D.; Grohs, P. Appropriateness of empirical antibiotic prescription for bloodstream infections in an emergency department from 2006 to 2018: Impact of the spread of ESBL-producing Enterobacterales. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Phungoen, P.; Apiratwarakul, K.; Lerdprawat, N.; Ienghong, K.; Sumritrin, S.; Boonsawat, W.; Sawanyawisuth, K. Clinical factors predictive of Gram-negative bloodstream infection at the Emergency Department. Germs 2022, 12, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Schoffelen, T.; Schouten, J.; Hoogerwerf, J.; Martín Quirós, A.; May, L.; Ten Oever, J.; Hulscher, M.E. Quality indicators for appropriate antimicrobial therapy in the emergency department: A pragmatic Delphi procedure. Clin. Microbiol. Infect. 2021, 27, 210–214. [Google Scholar] [CrossRef]
- Molina, J.; Peñalva, G.; Gil-Navarro, M.V.; Praena, J.; Lepe, J.A.; Pérez-Moreno, M.A.; Ferrándiz, C.; Aldabó, T.; Aguilar, M.; Olbrich, P.; et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections: A Quasi-Experimental Study of Interrupted Time-Series Analysis. Clin. Infect. Dis. 2017, 65, 1992–1999. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.; Noguer, M.; Lepe, J.A.; Pérez-Moreno, M.A.; Aguilar-Guisado, M.; Lasso de la Vega, R.; Peñalva, G.; Crespo-Rivas, J.C.; Gil-Navarro, M.V.; Salvador, J.; et al. Clinical impact of an educational antimicrobial stewardship program associated with infectious diseases consultation targeting patients with cancer: Results of a 9-year quasi-experimental study with an interrupted time-series analysis. J. Infect. 2019, 79, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Guisado-Gil, A.B.; Aguilar-Guisado, M.; Peñalva, G.; Lepe, J.A.; Espigado, I.; Rodríguez-Arbolí, E.; González-Campos, J.; Rodríguez-Torres, N.; Montero-Cuadrado, M.I.; Falantes-González, J.F.; et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Management of Patients with Hematological Diseases. Antibiotics 2021, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Casado, A.; Gimeno, A.; Aguilar-Guisado, M.; García, M.; Rodríguez, J.F.; Rivas, P.A.; Bueno, C.; Lepe, J.A.; Cisneros, J.M.; Molina, J. Safety of early oral ambulatory treatment of adult patients with bloodstream infections discharged from the emergency department. Antimicrob. Agents Chemother. 2023, 67, e00780-23. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO) Collaborating Center for Drug Statistics Methodology. ATC/DDD Index 2023. 2023. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 1 June 2023).
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 34th Edition. Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 21 March 2024).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 14.0. 2023. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 21 March 2024).
- Mattner, F.; Bange, F.C.; Meyer, E.; Seifert, H.; Wichelhaus, T.A.; Chaberny, I.F. Preventing the spread of multidrug-resistant gram-negative pathogens: Recommendations of an expert panel of the German Society for Hygiene and Microbiology. Dtsch. Arztebl. Int. 2012, 109, 39–45. [Google Scholar] [PubMed]
- Penfold, R.B.; Zhang, F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad. Pediatr. 2013, 13 (Suppl. 6), S38–S44. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Regression Intercept | Pre-Intervention Trend | Change in Level a | Change in Trend b | Absolute Effect | Relative Effect c (%) |
|---|---|---|---|---|---|---|
| Total J01 + J02 | 69.28 (62.80 to 75.75) | 0.01 (−0.55 to 0.57) | 1.28 (−4.99 to 7.55) | −1.17 (−1.92 to −0.41) | −31.81 (−54.48 to −9.14) | −45.6 (−64.5 to −26.7) |
| Ceftriaxone | 8.99 (5.83 to 12.17) | 0.28 (0.02 to 0.55) | 1.07 (−1.58 to 3.71) | −0.27 (−0.63 to 0.09) | −7.79 (−18.64 to 3.05) | −34.5 (−67.6 to −1.4) |
| Amoxicillin-clavulanic acid | 24.22 (22.52 to 25.92) | −0.40 (−0.56 to −0.24) | −2.36 (−4.58 to −0.14) | 0.05 (−0.15 to 0.26) | −0.05 (−6.17 to 6.06) | −1.1 (−120.5 to 118.3) |
| Levofloxacin | 12.99 (10.71 to 15.26) | 0.19 (0.01 to 0.36) | 0.62 (−0.06 to 1.30) | −0.55 (−0.80 to −0.31) | −15.4 (−22.7 to −8.2) | −70.1 (−83.8 to −56.4) |
| Piperacillin-tazobactam | 3.71 (2.47 to 4.95) | 0.06 (−0.05 to 0.17) | −0.64 (−1.94 to 0.66) | −0.15 (−0.29 to 0.001) | −4.52 (−8.92 to −0.12) | −67.9 (−93.9 to −41.9) |
| Ciprofloxacin | 6.22 (5.35 to 7.12) | −0.13 (−0.22 to −0.06) | 0.43 (−0.55 to 1.41) | 0.02 (−0.08 to 0.13) | 1.01 (−1.91 to 3.93) | 155.2 (−655.8 to 686.8) |
| Azithromycin | 0.66 (0.17 to 1.14) | 0.03 (−0.01 to 0.08) | 0.26 (−0.37 to 0.89) | −0.03 (−0.09 to 0.02) | 0.16 (−2.87 to 3.19) | 7.1 (−75.9 to 90.1) |
| Metronidazole | 0.22 (−0.84 to 1.28) | 0.11 (0.03 to 0.18) | 0.26 (−0.23 to 0.75) | −0.18 (−0.29 to −0.08) | −5.22 (−8.45 to −1.99) | −98.9 (−116.9 to −80.8) |
| Ertapenem | 2.16 (1.93 to 2.39) | −0.06 (−0.08 to −0.04) | 0.08 (−0.26 to 0.41) | 0.02 (−0.009 to 0.04) | 0.14 (−0.47 to 0.68) | 14.3 (−19.7 to 47.7) |
| Antipseudomonal cephalosporins | 0.53 (0.35 to 0.71) | 0.004 (−0.01 to 0.02) | 0.46 (0.36 to 0.56) | −0.006 (−0.02 to 0.01) | 0.27 (−0.31 to 0.85) | 36.9 (−68.9 to 142.9) |
| Meropenem | 0.54 (0.08 to 1.01) | 0.02 (−0.02 to 0.06) | 0.17 (−0.26 to 0.60) | −0.06 (−0.11 to −0.006) | −1.16 (−2.71 to 0.40) | −80.4 (−115.0 to −45.7) |
| Vancomycin | 0.74 (0.58 to 0.90) | −0.01 (−0.02 to 0.004) | 0.28 (0.07 to 0.49) | −0.004 (−0.02 to 0.01) | 0.20 (−0.37 to 0.78) | 83.0 (−341.2 to 507.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guisado-Gil, A.B.; Mejías-Trueba, M.; Peñalva, G.; Aguilar-Guisado, M.; Molina, J.; Gimeno, A.; Álvarez-Marín, R.; Praena, J.; Bueno, C.; Lepe, J.A.; et al. Antimicrobial Stewardship in the Emergency Department Observation Unit: Definition of a New Indicator and Evaluation of Antimicrobial Use and Clinical Outcomes. Antibiotics 2024, 13, 356. https://doi.org/10.3390/antibiotics13040356
Guisado-Gil AB, Mejías-Trueba M, Peñalva G, Aguilar-Guisado M, Molina J, Gimeno A, Álvarez-Marín R, Praena J, Bueno C, Lepe JA, et al. Antimicrobial Stewardship in the Emergency Department Observation Unit: Definition of a New Indicator and Evaluation of Antimicrobial Use and Clinical Outcomes. Antibiotics. 2024; 13(4):356. https://doi.org/10.3390/antibiotics13040356
Chicago/Turabian StyleGuisado-Gil, Ana Belén, Marta Mejías-Trueba, Germán Peñalva, Manuela Aguilar-Guisado, Jose Molina, Adelina Gimeno, Rocío Álvarez-Marín, Julia Praena, Claudio Bueno, José Antonio Lepe, and et al. 2024. "Antimicrobial Stewardship in the Emergency Department Observation Unit: Definition of a New Indicator and Evaluation of Antimicrobial Use and Clinical Outcomes" Antibiotics 13, no. 4: 356. https://doi.org/10.3390/antibiotics13040356
APA StyleGuisado-Gil, A. B., Mejías-Trueba, M., Peñalva, G., Aguilar-Guisado, M., Molina, J., Gimeno, A., Álvarez-Marín, R., Praena, J., Bueno, C., Lepe, J. A., Gil-Navarro, M. V., & Cisneros, J. M. (2024). Antimicrobial Stewardship in the Emergency Department Observation Unit: Definition of a New Indicator and Evaluation of Antimicrobial Use and Clinical Outcomes. Antibiotics, 13(4), 356. https://doi.org/10.3390/antibiotics13040356